Abstract
Cutaneous metastases from primary internal malignancies represent 0.7-9% of patients with cancer. We report a 65-year-old female patient referred for evaluation of normochromic papules on the trunk and upper limbs that had been present for three months. A skin biopsy revealed diffuse cutaneous infiltration by small round cell tumors. Immunohistochemistry was positive for AE1/AE3, CK7, estrogen receptor and mammaglobin. The final diagnosis was cutaneous metastasis of occult breast cancer, since the solid primary tumor was not identified. The location of the primary tumor can not be determined in 5-10% of cases. In these cases, 27% are identified before the patient’s death, 57% at autopsy, and the remaining 16% can not be located.
Keywords:
Breast neoplasms; Neoplasm metastasis; Skin
INTRODUCTION
Cutaneous metastasis is defined as a neoplastic lesion affecting the dermis or the subcutaneous tissue that originates from another primary tumor.11 Caldas FAA, Curtis JAG, Baldelin TAR, Zignani JM, Bauab SP. Recidivas cutâneas de tumores mamários: formas de apresentação e diagnóstico diferencial. Rev Imagem. 2006;28:197-201. Three basic patterns of metastasis mechanisms are reported: mechanical tumor stasis (anatomical proximity and lymphatic drainage), organ-specific (selective affinity of tumor cells to a specific organ), and nonselective (independent of mechanical and organ-specific factors).11 Caldas FAA, Curtis JAG, Baldelin TAR, Zignani JM, Bauab SP. Recidivas cutâneas de tumores mamários: formas de apresentação e diagnóstico diferencial. Rev Imagem. 2006;28:197-201.
Malignant neoplasms that most commonly metastasize to the skin include breast cancer, colon cancer, melanoma, lung cancer, ovary cancer, sarcomas, and cervical cancer.11 Caldas FAA, Curtis JAG, Baldelin TAR, Zignani JM, Bauab SP. Recidivas cutâneas de tumores mamários: formas de apresentação e diagnóstico diferencial. Rev Imagem. 2006;28:197-201. In most cases, cutaneous metastasis develops after the diagnosis of the primary internal malignancy and late in the course of the disease. An interval of five years from the initial diagnosis to the skin metastases is common.22 Casimiro LM, Corell JJV. Metástasis cutáneas de neoplasias internas. Med Cutan Iber Lat Am. 2009;37:117-29. 0.7-9% of patients with cancer develop skin metastasis, which is considered a rare dermatological event.22 Casimiro LM, Corell JJV. Metástasis cutáneas de neoplasias internas. Med Cutan Iber Lat Am. 2009;37:117-29.,33 Wong CYW, Helm MA, Kalb RE, Helm TN, Zeitouni NC. The presentation, pathology, and current management strategies of cutaneous metastasis. N Am J Med Sci. 2013;5:499-504. However, with the increased incidence of internal cancer, dermatologists may be the first to discover the disease.22 Casimiro LM, Corell JJV. Metástasis cutáneas de neoplasias internas. Med Cutan Iber Lat Am. 2009;37:117-29. A high index of clinical suspicion is essential for the diagnosis of cutaneous metastatic lesions.33 Wong CYW, Helm MA, Kalb RE, Helm TN, Zeitouni NC. The presentation, pathology, and current management strategies of cutaneous metastasis. N Am J Med Sci. 2013;5:499-504.
CASE
Who was referred to our institution for evaluation of asymptomatic papules and nodules on the trunk and upper limbs that had been present three months before the consultation. The patient was unable to report the initial morphology or changing pattern of the lesions. She also reported weight loss, which was not measured, and asthenia. Remarkable personal history included anemia treated with ferrous sulfate and a sectorectomy of a benign left breast lump eight years before – which was anatomopathologically confirmed. The patient was G4P3A1 and had been in menopause for 16 years. She denied alcohol abuse, smoking, or remarkable family history.
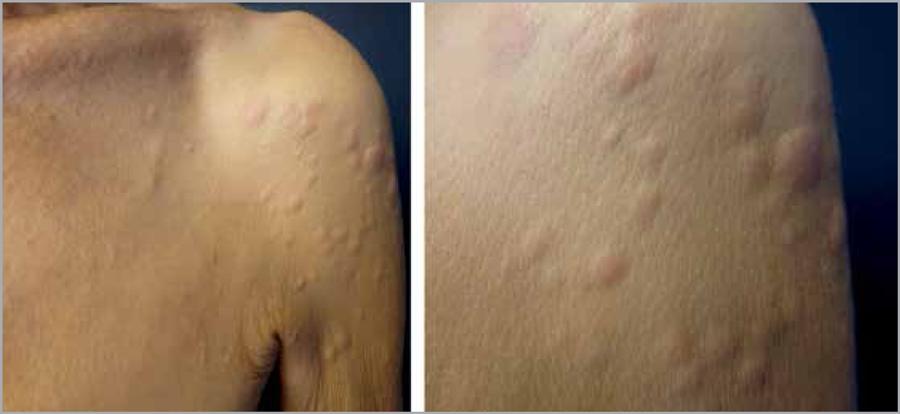
On physical examination, the patient was emaciated, pale (3+/4+), presented with normochromic rounded papules and nodules, with well-defined regular edges and fibroelastic consistency. The lesions were slightly movable, 0.3-1 cm in diameter, located on the arm root, chest and back. We also observed a linear pearl-colored scar on the left breast (Figures 1-3).
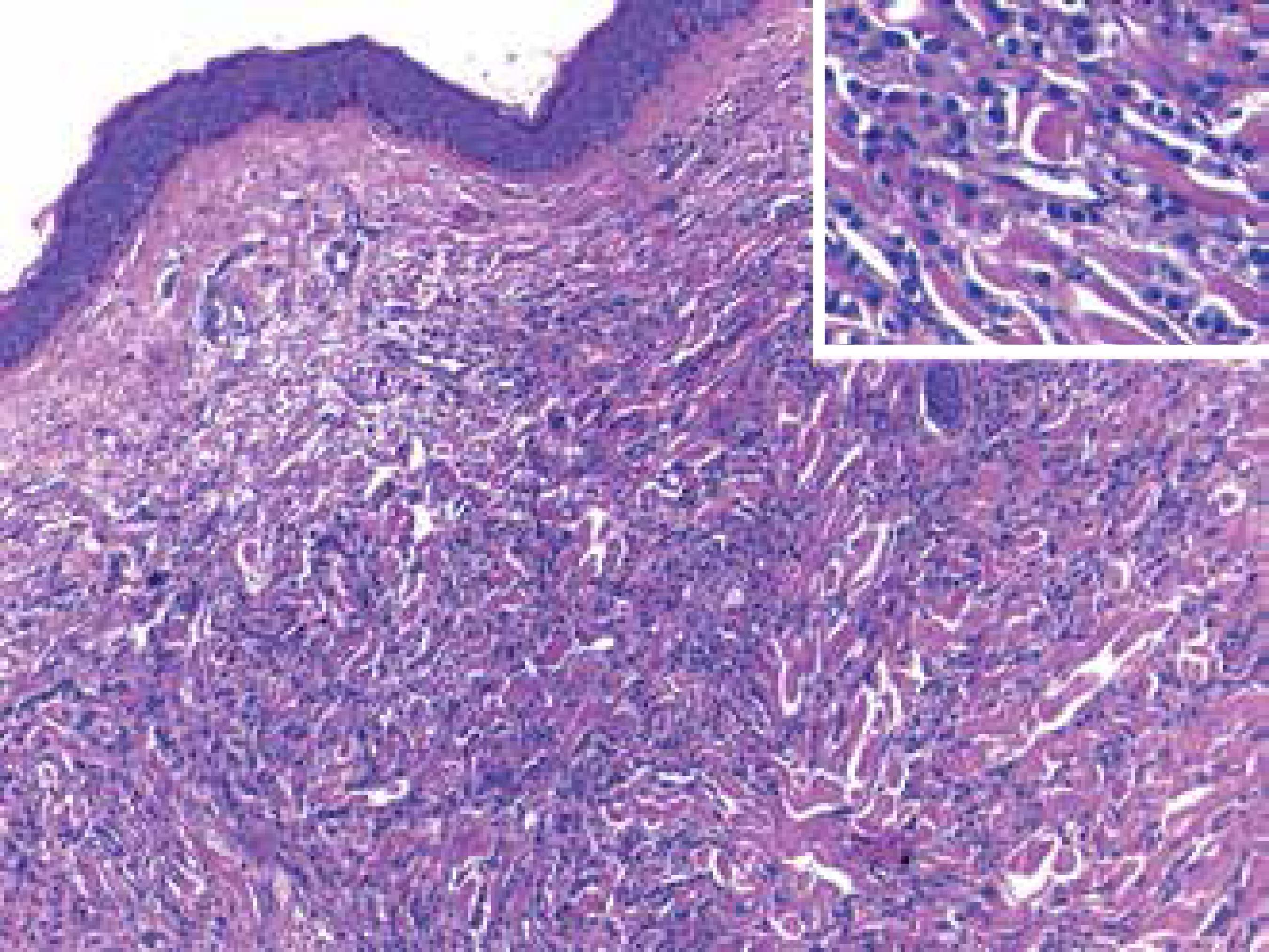
Additional tests were performed (Chart 1). Histopathology of two areas of the skin showed a diffuse round cell infiltration in the dermis and part of the hypodermis, sparing the epidermis, divulsing the collagen bundles. The lesions were isolated or linearly arranged in rows, printing an irregular pattern (Figure 4). Immunohistochemical examination showed strong and diffuse positivity for AE1/AE3, favoring the diagnosis of carcinoma, and negative results for S100 protein and leukocyte common antigen (LCA). Melanoma and hemolymphatic cancers were ruled out. Positive multigene panel showed positivity to CK7, mammaglobin, and estrogen receptor, suggesting the breast tissue as the primary site. Other markers are shown in Table 1. The patient was referred to a gynecologist who, after a clinical evaluation, opted for a biopsy of axillary lymph nodes on the left side: four lymph nodes with metastatic carcinoma.
Skin: diffuse neoplastic infiltration in the dermis (hematoxylin and eosin; x200); Inset: higher magnification showing small round cell tumors
Given the clinical findings and laboratory test results, a final diagnosis of cutaneous metastasis of occult breast cancer was made since the primary solid tumor was not detected by any other examination. We reviewed the slides of the sectorectomy performed in 2005 and identified no neoplasias. The patient was then referred to an oncologist for follow-up and chemotherapy. Unfortunately, she died 10 months after the diagnosis.
DISCUSSION
The frequency of cutaneous metastases has increased due to higher cancer survival rates and better therapeutic alternatives.44 Gabriela Frías A, Sagrario Hierro O, Adriana Miranda G. Metástasis cutâneas. Dermatología Rev Mex 2006;50:60-8. The identification of both the skin cancer and the primary tumor can be difficult due to the great variability in clinical course. After a cancer treatment, metastases can be the first sign of relapse, having a significant prognostic value for substantially reducing survival rates.22 Casimiro LM, Corell JJV. Metástasis cutáneas de neoplasias internas. Med Cutan Iber Lat Am. 2009;37:117-29.
Metastases are more common in older people. A skin biopsy in patients with cancer should be considered in case of early or sudden onset, delayed healing, bleeding tendency, or vascular appearance of the lesions that do not resolve after treatment.22 Casimiro LM, Corell JJV. Metástasis cutáneas de neoplasias internas. Med Cutan Iber Lat Am. 2009;37:117-29.
About 60% of the metastatic cancers are adenocarcinomas. Malignant neoplasms that most metastasize include breast, lung, and gastrointestinal tract cancers. In patients under 50 years of age, metastasis is often linked to malignant melanoma. In pediatric patients, although infrequent, metastasis are usually caused by neuroblastomas and leukemias.55 Strohl RA. Cutaneous manifestations of malignant disease. Dermatol Nurs. 1998;10:23-5.,66 Schwartz RA. Cutaneous metastatic disease. J Am Acad Dermatol. 1995;33:161
The most common sites of metastasis (75%) are the scalp, navel, chest wall, and abdomen, and in 75% of women, they occur on the chest and abdomen. In women, the most common primary malignancy is breast cancer (69%), which tends to metastasize later to the anterior thoracic wall.33 Wong CYW, Helm MA, Kalb RE, Helm TN, Zeitouni NC. The presentation, pathology, and current management strategies of cutaneous metastasis. N Am J Med Sci. 2013;5:499-504.,77 Chiu CS, Lin CY, Kuo TT, Kuan YZ, Chen MJ, Ho HC, et al. Malignant cutaneous tumors of the scalp: a study of demographic characteristics and histologic distributions of 398 Taiwanese patients. J Am Acad Dermatol. 2007;56:448-52. Van den Hurk et al. (2011) analyzed metastases patterns in patients diagnosed with primary breast cancer and found that skin metastases often appear later than metastases in other areas.88 van den Hurk CJ, Eckel R, van de Poll-Franse LV, Coebergh JW, Nortier JW, Hölzel D, et al. Unfavourable pattern of metastases in M0 breast cancer patients during 1978-2008: a population-based analysis of the Munich Cancer Registry. Breast Cancer Res Treat. 2011;128:795-805.
Although metastasis clinical presentation is variable, it is more frequently characterized as normochromic or brownish firm nodules with sudden onset. Lesions can be painless or associated with pain and sensitivity, with fast initial growth and subsequent stabilization. They may be solitary or multiple, with inflammatory or sclerotic aspects, and may retract the skin.22 Casimiro LM, Corell JJV. Metástasis cutáneas de neoplasias internas. Med Cutan Iber Lat Am. 2009;37:117-29.,99 Bordel-Gómez MT, Used-Aznar MM. Metástasis cutáneas de adenocarcinoma de origen primario desconocido. Actas Dermosifiliogr. 2006;97:662-5. Extensive cutaneous involvement of metastatic breast cancer may mimic cellulitis or a breast-plate of armor (“en cuirasse” pattern).33 Wong CYW, Helm MA, Kalb RE, Helm TN, Zeitouni NC. The presentation, pathology, and current management strategies of cutaneous metastasis. N Am J Med Sci. 2013;5:499-504.
Differential diagnosis consists of other similar histologically lesions, benign, inflammatory, or malignant, of different prognostics.1010 Wambacher-Gasser B, Zelger B, Zelger BG, Steiner H. Clear cell dermatofibroma. Histopathology. 1997;30:64-9. Breast cancer immunohistochemistry reveals a cytokeratins pattern of CK7+/CK20-. Estrogens and progesterone receptors are markers that increase the detection sensitivity of breast cancers.77 Chiu CS, Lin CY, Kuo TT, Kuan YZ, Chen MJ, Ho HC, et al. Malignant cutaneous tumors of the scalp: a study of demographic characteristics and histologic distributions of 398 Taiwanese patients. J Am Acad Dermatol. 2007;56:448-52.
Despite the imaging techniques and immunohistochemistry, the primary tumor location cannot be determined in 5-10% of cases. In general, patients with metastatic carcinoma of unknown primary site have a worse prognosis. In these patients, the primary tumor is only identified in 27% of cases before death; 57%, at autopsy; and for the remaining 16%, primary tumor can not be identified.88 van den Hurk CJ, Eckel R, van de Poll-Franse LV, Coebergh JW, Nortier JW, Hölzel D, et al. Unfavourable pattern of metastases in M0 breast cancer patients during 1978-2008: a population-based analysis of the Munich Cancer Registry. Breast Cancer Res Treat. 2011;128:795-805.
-
*
Work performed at Department of Dermatology at Hospital e Maternidade Celso Pierro - Pontifícia Universidade Católica de Campinas (HMCP-PUCCampinas) – Campinas (SP), Brazil.
-
Financial Support: None
References
-
1Caldas FAA, Curtis JAG, Baldelin TAR, Zignani JM, Bauab SP. Recidivas cutâneas de tumores mamários: formas de apresentação e diagnóstico diferencial. Rev Imagem. 2006;28:197-201.
-
2Casimiro LM, Corell JJV. Metástasis cutáneas de neoplasias internas. Med Cutan Iber Lat Am. 2009;37:117-29.
-
3Wong CYW, Helm MA, Kalb RE, Helm TN, Zeitouni NC. The presentation, pathology, and current management strategies of cutaneous metastasis. N Am J Med Sci. 2013;5:499-504.
-
4Gabriela Frías A, Sagrario Hierro O, Adriana Miranda G. Metástasis cutâneas. Dermatología Rev Mex 2006;50:60-8.
-
5Strohl RA. Cutaneous manifestations of malignant disease. Dermatol Nurs. 1998;10:23-5.
-
6Schwartz RA. Cutaneous metastatic disease. J Am Acad Dermatol. 1995;33:161
-
7Chiu CS, Lin CY, Kuo TT, Kuan YZ, Chen MJ, Ho HC, et al. Malignant cutaneous tumors of the scalp: a study of demographic characteristics and histologic distributions of 398 Taiwanese patients. J Am Acad Dermatol. 2007;56:448-52.
-
8van den Hurk CJ, Eckel R, van de Poll-Franse LV, Coebergh JW, Nortier JW, Hölzel D, et al. Unfavourable pattern of metastases in M0 breast cancer patients during 1978-2008: a population-based analysis of the Munich Cancer Registry. Breast Cancer Res Treat. 2011;128:795-805.
-
9Bordel-Gómez MT, Used-Aznar MM. Metástasis cutáneas de adenocarcinoma de origen primario desconocido. Actas Dermosifiliogr. 2006;97:662-5.
-
10Wambacher-Gasser B, Zelger B, Zelger BG, Steiner H. Clear cell dermatofibroma. Histopathology. 1997;30:64-9.
Publication Dates
-
Publication in this collection
Sep-Oct 2016
History
-
Received
17 Mar 2015 -
Accepted
27 May 2015