Abstract
Cutaneous leiomyosarcoma is a rare neoplasia, and its periorbital presentation is rather uncommon. We present a case of a male patient who was surgically treated, with the reconstruction performed with a frontal myocutaneous flap. The patient has been followed up for one year with adequate oncologic control and good aesthetic outcome.
Keywords:
Leiomiossarcoma; Leiomyosarcoma; Sarcoma; Skin neoplasms; Surgical flaps
INTRODUCTION
Leiomyosarcomas represent approximately 7% of all soft tissue sarcomas, being more common on the abdomen and retroperitoneum. Cutaneous leiomyosarcoma (CLMS) is a rare neoplasia and is responsible for less than 3% of the superficial sarcomas.11 Enzinger FM, Weiss SW. Leiomyosarcoma. In: Soft tissue tumors. 4th ed. St Louis, Missouri: Mosby; 2001. p.491-508. CLMS can appear on any part of the body, with predilection for the lower limbs (50 to 75%), and rarely affects the face (1 to 5%).22 Fields JP, Helwig EB. Leiomyosarcoma of the skin and subcutaneous tissue. Cancer. 1981;47:156-69. Most literature data indicate a male (3:1) and Caucasian predilection, appearing more frequently in the fifth and sixth decades of life.22 Fields JP, Helwig EB. Leiomyosarcoma of the skin and subcutaneous tissue. Cancer. 1981;47:156-69.,33 Deneve JL, Messina JL, Bui MM, Marzban SS, Letson GD, Cheong D, et al. Cutaneous leiomyosarcoma: treatment and outcomes with a standardized margin of resection. Cancer Control. 2013;20:307-12. CLMS is subdivided into dermal and subcutaneous. The former appears to originate in the piloerector smooth muscle, is locally aggressive (potential of recurrence of 30 to 50%), with little tendency to metastasize. The latter seems to arise from the muscle layeer of the vessels, has more chances of recurrence (50 to 70%) and metastasis.44 Guillén DR, Cockerell CJ. Cutaneous and subcutaneous sarcomas. Clin Dermatol. 2001;19:262-8.,55 Bernstein SC, Roenigk RK. Leiomyosarcoma of the Skin - treatment of 34 cases. Dermatol Surg. 1996;22:631-5. Enzinger considers to be CLMS only those tumors originated in the piloerector muscles, which are rarer than the subcutaneous type, that comes from the small vessels. This author further classifies as vascular leiomyosarcoma those arising from medium and large caliber vessels.11 Enzinger FM, Weiss SW. Leiomyosarcoma. In: Soft tissue tumors. 4th ed. St Louis, Missouri: Mosby; 2001. p.491-508.
CLMS presents clinically as a solitary nodule. The dermal variant is found adhered to the epidermis, covered by erythematous or brownish skin, tending to be smaller and present slower growth compared to the subcutaneous subtype, that is usually mobile and covered by normal skin. There can be pain on palpation, as well as pruritus, paresthesias and bleeding.11 Enzinger FM, Weiss SW. Leiomyosarcoma. In: Soft tissue tumors. 4th ed. St Louis, Missouri: Mosby; 2001. p.491-508.,55 Bernstein SC, Roenigk RK. Leiomyosarcoma of the Skin - treatment of 34 cases. Dermatol Surg. 1996;22:631-5.,66 Fleury LFF Jr, Sanches JA Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81:207-21. Histologically, it is a smooth muscle cell tumor, with proliferation of spindle cells with a bulky, elongated cigar-shaped nucleus, besides pleomorphism and mitoses. The well differentiated areas of the tumor show a higher concentration of spindle cells, whereas the less well differentiated show giant, atypical cells with bizarre nuclei.22 Fields JP, Helwig EB. Leiomyosarcoma of the skin and subcutaneous tissue. Cancer. 1981;47:156-69.,55 Bernstein SC, Roenigk RK. Leiomyosarcoma of the Skin - treatment of 34 cases. Dermatol Surg. 1996;22:631-5.,66 Fleury LFF Jr, Sanches JA Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81:207-21. The main immunohistochemistry markers are smooth muscle actin desmin and vimentin.22 Fields JP, Helwig EB. Leiomyosarcoma of the skin and subcutaneous tissue. Cancer. 1981;47:156-69.,66 Fleury LFF Jr, Sanches JA Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81:207-21.
Surgical treatment is preferred, with margins of 1 cm or more, or Mohs micrographic surgery.33 Deneve JL, Messina JL, Bui MM, Marzban SS, Letson GD, Cheong D, et al. Cutaneous leiomyosarcoma: treatment and outcomes with a standardized margin of resection. Cancer Control. 2013;20:307-12. We report this case due to its rarity and uncommon location, as well as its surgical treatment, that proved to be satisfactory from the oncological, functional and aesthetic point of view.
CASE REPORT
Thirty-four-year-old phototype IV male was referred for evaluation of a tumor on the medial corner of the left eye tha had been present for eight months. On dermatological examination, there was a firm, erythematous nodule, measuring 2.0 x 1.5 cm, adhered to the skin, with a central crust and located on the left nasojugal groove (Figure 1). There was pain on palpation. There were no palpable lymph nodes. An incisional biopsy was performed, and the histology revealed a poorly differentiated malignancy, with a spindle cell pattern, diffusely infiltrating the dermis (Figures 2 and 3). Immunohistochemistry was positive for specific muscle actin (HHF-35), smooth muscle actin (HUC-1) and Ki-67 in 10% of the tumor cells (Figure 4). Chest radiograph and abdominal ultrasound were normal. The patient underwent surgery with lateral, medial and inferior margins of 1.5 cm and 1 cm superior margin deep down to the periosteum. The defect was reconstructed with a frontal myocutaneous flap. Histology showed clear margins, and the patient has been followed up for one year now, with no recurrence.
Firm, erythematous nodule, adhered and with central crust, measuring 2.0 x 1.5cm, located on the left nasojugal groove
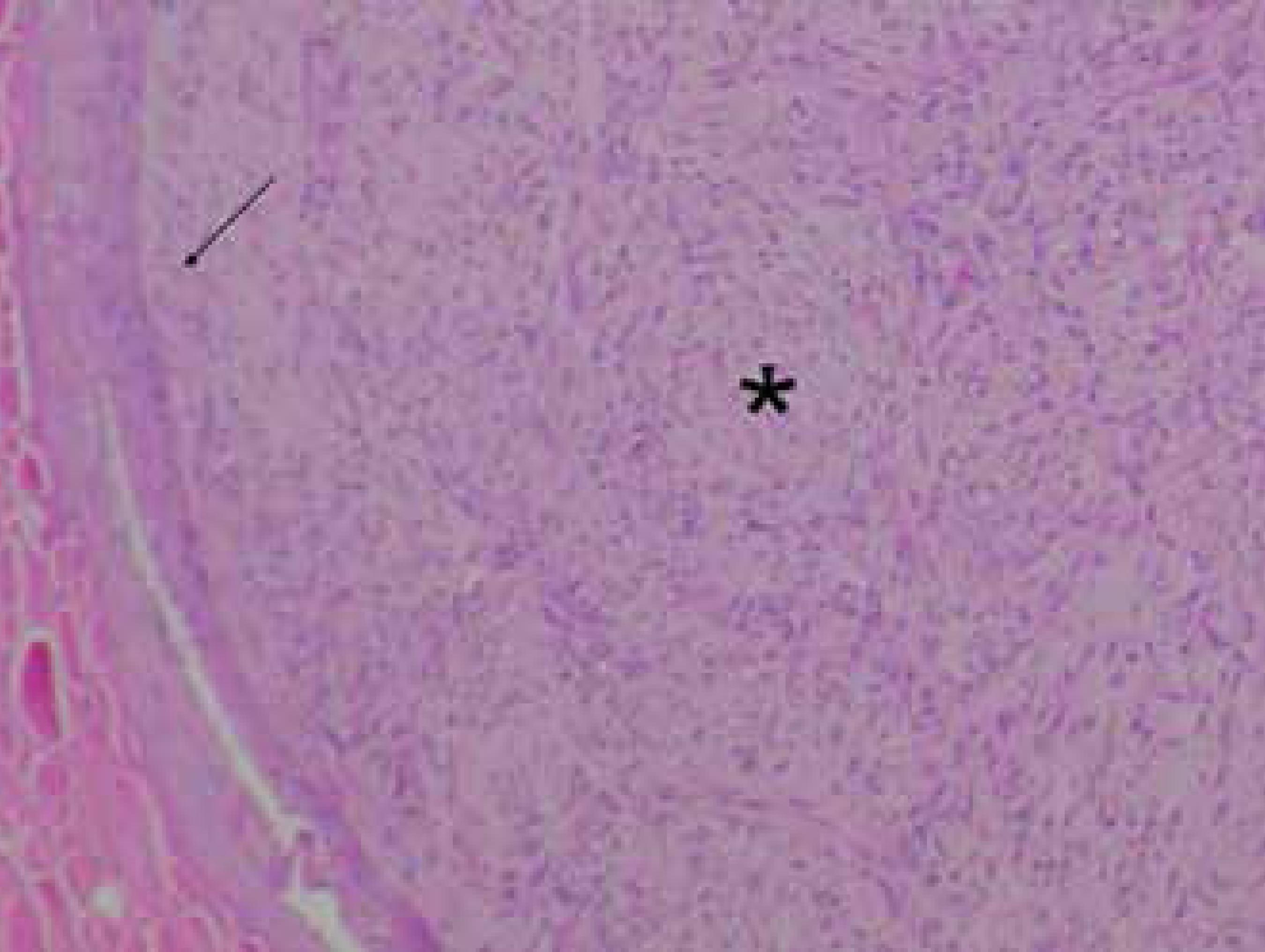
Spindle cell neoplasia (*) diffusely infiltrating the dermis and epidermis (arrow) (Hematoxylin & eosin, X200)
Detail of spindle cell with bulky, elongated, cigar-shaped nuclei (Hematoxylin & eosin, X400)
DISCUSSION
Leiomyosarcoma is an uncommon neoplasia, with clinical features similar to other skin tumors. In our case, the initial differential diagnoses proposed were dermatofibrosarcoma protuberans, basal cell carcinoma, squamous cell carcinoma and pilomatricoma. The final diagnosis was made after histological examination with hematoxylin and eosin (HE) in paraffin and complementary immunohistochemistry, key tests for this rare tumor.
The differentiation between dermal and subcutaneous CLMS is important because they have distinct clinical and prognostic features. The dermal type occurs in men on the fifth and seventh decades of life, has better prognosis, local recurrence rates of 14-50% and low metastatic potential; the subcutaneous type occurs in both genders equally, in a more advanced age (fifth and eighth decades of life), has a poorer prognosis with local recurrence rates that range between 40-60% and the likelihood of metastasis of 20-60%.77 Winchester DS, Hocker TL, Brewer JD, Baum CL, Hochwalt PC, Arpey CJ, et al. Leiomyosarcoma of the skin: clinical, histopathologic, and prognostic factors that influence outcomes. J Am Acad Dermatol. 2014;71:919-25.
8 Bernstein SC, Roenigk RK. Leiomyosarcoma of the skin: treatment of 34 cases. Dermatol Surg. 1996;22:631-5.-99 Snowden RT, Osborn FD, Wong FS, Sebelik ME. Superficial leiomyosarcoma of the head and neck: case report and review of the literature. Ear Nose Throat J. 2001;80:449-53. According to Annest et al., the dermal type occurs predominantly on the head and neck, whereas the subcutaneous type favors the lower limbs.1010 Annest NM, Grekin SJ, Stone MS, Messingham MJ. Cutaneous leiomyosarcoma: a tumor of the head and neck. Dermatol Surg. 2007;33:628-33. However, in a more recent study, the extremities were the most commonly affected area for both dermal and subcutaneous types (52% for both).77 Winchester DS, Hocker TL, Brewer JD, Baum CL, Hochwalt PC, Arpey CJ, et al. Leiomyosarcoma of the skin: clinical, histopathologic, and prognostic factors that influence outcomes. J Am Acad Dermatol. 2014;71:919-25.
Treatment is essentially surgical. Surgical excision with wide margins is the most used technique to treat this tumor. Despite the lack of consensus regarding the most adequate margins, studies suggest using a minimum 1cm margin.22 Fields JP, Helwig EB. Leiomyosarcoma of the skin and subcutaneous tissue. Cancer. 1981;47:156-69.,33 Deneve JL, Messina JL, Bui MM, Marzban SS, Letson GD, Cheong D, et al. Cutaneous leiomyosarcoma: treatment and outcomes with a standardized margin of resection. Cancer Control. 2013;20:307-12.,55 Bernstein SC, Roenigk RK. Leiomyosarcoma of the Skin - treatment of 34 cases. Dermatol Surg. 1996;22:631-5. Mohs micrographic surgery has shown promising results, with high rates of cure and preservation of health tissue, but more cases need to be reported so that it can be considered the standard treatment technique. Chemotherapy and radiotherapy are controversial, but adjuvant radiotherapy has been used for high grade tumors, cases with positive margins, tumors larger than 5 cm and for those with extensive subcutaneous involvement.33 Deneve JL, Messina JL, Bui MM, Marzban SS, Letson GD, Cheong D, et al. Cutaneous leiomyosarcoma: treatment and outcomes with a standardized margin of resection. Cancer Control. 2013;20:307-12.
We report the case of a dermal CLMS, in a male, phototype IV patient, occurring at an early age and on an uncommon location. Our patient’s tumor has a better prognosis due to the lower rates of recurrence and few cases of metastasis found in the literature. In a study performed by Winchester et al, 5 out of 48 dermal CLMS cases developed metastasis, with 2 out of 5 cases resulting in death.77 Winchester DS, Hocker TL, Brewer JD, Baum CL, Hochwalt PC, Arpey CJ, et al. Leiomyosarcoma of the skin: clinical, histopathologic, and prognostic factors that influence outcomes. J Am Acad Dermatol. 2014;71:919-25. We opted for a conventional surgical excision with wide margins since Mohs surgery is not available in our hospital. Adjuvant radiotherapy was not indicated because it is controversial and due to the risk of radiation induced cataracts, considering the lesion was on the periorbital area. The prognosis is favorable, considering the resection of the primary tumor showed tumor-free margins. The patient will be reviewed every six months for the first 5 years (the period with highest recurrence rates) and then annually to monitor possible recurrence and/or metastasis.1010 Annest NM, Grekin SJ, Stone MS, Messingham MJ. Cutaneous leiomyosarcoma: a tumor of the head and neck. Dermatol Surg. 2007;33:628-33.
-
*
Study conducted at Hospital Universitário Lauro Wanderley of the Universidade Federal da Paraíba (HULW-UFPB) - João Pessoa (PB), Brazil.
-
Financial Support: None
REFERENCES
-
1Enzinger FM, Weiss SW. Leiomyosarcoma. In: Soft tissue tumors. 4th ed. St Louis, Missouri: Mosby; 2001. p.491-508.
-
2Fields JP, Helwig EB. Leiomyosarcoma of the skin and subcutaneous tissue. Cancer. 1981;47:156-69.
-
3Deneve JL, Messina JL, Bui MM, Marzban SS, Letson GD, Cheong D, et al. Cutaneous leiomyosarcoma: treatment and outcomes with a standardized margin of resection. Cancer Control. 2013;20:307-12.
-
4Guillén DR, Cockerell CJ. Cutaneous and subcutaneous sarcomas. Clin Dermatol. 2001;19:262-8.
-
5Bernstein SC, Roenigk RK. Leiomyosarcoma of the Skin - treatment of 34 cases. Dermatol Surg. 1996;22:631-5.
-
6Fleury LFF Jr, Sanches JA Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81:207-21.
-
7Winchester DS, Hocker TL, Brewer JD, Baum CL, Hochwalt PC, Arpey CJ, et al. Leiomyosarcoma of the skin: clinical, histopathologic, and prognostic factors that influence outcomes. J Am Acad Dermatol. 2014;71:919-25.
-
8Bernstein SC, Roenigk RK. Leiomyosarcoma of the skin: treatment of 34 cases. Dermatol Surg. 1996;22:631-5.
-
9Snowden RT, Osborn FD, Wong FS, Sebelik ME. Superficial leiomyosarcoma of the head and neck: case report and review of the literature. Ear Nose Throat J. 2001;80:449-53.
-
10Annest NM, Grekin SJ, Stone MS, Messingham MJ. Cutaneous leiomyosarcoma: a tumor of the head and neck. Dermatol Surg. 2007;33:628-33.
Publication Dates
-
Publication in this collection
2017
History
-
Received
31 July 2015 -
Accepted
18 Apr 2016