Abstracts
INTRODUCTION: Fibromyalgia affects 8% of the population over the age of 40 years, and 75% of the patients with fibromyalgia have poor sleep quality. OBJECTIVE: To assess the effects of hydrotherapy on the physical function and sleep quality of patients with fibromyalgia. METHODS: Patients were under clinical care at the UNASP Outpatient Clinic. This study assessed 60 female patients with fibromyalgia aged between 30 and 65 years. Out of the 60 patients assessed, 20 were excluded and 10 left the study because they could not comply with the time schedule. All patients completed the following questionnaires: Fibromyalgia Impact Questionnaire (FIQ); Pittsburgh Sleep Quality Index, and Epworth Sleepiness Scale. Training sessions were performed twice a week for two months, each session lasting 60 minutes. RESULTS: Patients' mean age was 45 years, 66% were active workers, and 34% had quit work. Right after the hydrotherapy program, the patients improved the following aspects assessed by use of the FIQ: physical function, work absenteeism, ability to do job, pain intensity, fatigue, morning tiredness, stiffness (P < 0.0001), anxiety (P = 0,0013), and depression (P < 0.0001). Sleep quality (P < 0.0001) and daytime sleepiness (P = 0.0003) also improved. CONCLUSION: Hydrotherapy improves sleep quality, physical function, professional status, psychological disorders and physical symptoms in patients with fibromyalgia.
sleep; fibromyalgia; hydrotherapy; quality of life
INTRODUÇÃO: A síndrome da fibromialgia acomete 8% da população com mais de 40 anos de idade. Dos pacientes com fibromialgia, 75% queixam-se de má qualidade do sono. OBJETIVO: Avaliar os efeitos da hidrocinesioterapia sobre a capacidade funcional e a qualidade de sono em pacientes com fibromialgia. MÉTODOS: As pacientes foram atendidas na policlínica da UNASP. Foram avaliadas 60 pacientes portadoras de fibromialgia na faixa etária entre 30 e 65 anos. Das pacientes avaliadas, 20 foram excluídas e 10 desistiram devido à impossibilidade de apresentar-se no horário do programa de exercícios. Todas as pacientes responderam aos seguintes questionários: Questionário sobre o Impacto daFibromialgia (QIF), Índice da Qualidade do Sono de Pittsburgh e Escala de Sonolência de Epworth. As sessões foram realizadas duas vezes por semana, com duração de 60 minutos cada, por um período de dois meses. RESULTADOS: A média da idade das pacientes foi de 45 anos; 66% eram trabalhadoras ativas e 34% estavam afastadas do trabalho. Verificouse que imediatamente após participarem do programa da hidrocinesioterapia, as pacientes apresentaram melhora nos seguintes aspectos avaliados por meio do QIF: capacidade funcional, absenteísmo ao trabalho, capacidade de serviço, intensidade da dor, fadiga, cansaço matinal, rigidez (P < 0,0001), ansiedade (P = 0,0013) e depressão (P < 0,0001). Houve também melhora da qualidade do sono (P < 0,0001) e no grau de sonolência diurna (P = 0,0003). CONCLUSÃO: A hidrocinesioterapia promove melhora de qualidade do sono, capacidade funcional, situação profissional, distúrbio psicológicos e sintomas físicos da síndrome em pacientes com fibromialgia.
fibromialgia; sono; hidroterapia; qualidade de vida
ORIGINAL ARTICLE
IPhysical therapist; Member of the Research Group on Hydrotherapy in Chronic Diseases, Universidade Adventista de São Paulo - UNASP
IIMaster's degree; Professor of the Physical Therapy and Administration Courses, UNASP
IIIPhD candidate, Universidade Federal de São Paulo - Unifesp; Professor of the Physical Therapy Course, Universidade Federal do Pampa - Unipampa
IVPhD candidate, Unifesp; Professor of the Physical Therapy Course, UNASP
Correspondence to
ABSTRACT
INTRODUCTION: Fibromyalgia affects 8% of the population over the age of 40 years, and 75% of the patients with fibromyalgia have poor sleep quality.
OBJECTIVE: To assess the effects of hydrotherapy on the physical function and sleep quality of patients with fibromyalgia.
METHODS: Patients were under clinical care at the UNASP Outpatient Clinic. This study assessed 60 female patients with fibromyalgia aged between 30 and 65 years. Out of the 60 patients assessed, 20 were excluded and 10 left the study because they could not comply with the time schedule. All patients completed the following questionnaires: Fibromyalgia Impact Questionnaire (FIQ); Pittsburgh Sleep Quality Index, and Epworth Sleepiness Scale. Training sessions were performed twice a week for two months, each session lasting 60 minutes.
RESULTS: Patients' mean age was 45 years, 66% were active workers, and 34% had quit work. Right after the hydrotherapy program, the patients improved the following aspects assessed by use of the FIQ: physical function, work absenteeism, ability to do job, pain intensity, fatigue, morning tiredness, stiffness (P < 0.0001), anxiety (P = 0,0013), and depression (P < 0.0001). Sleep quality (P < 0.0001) and daytime sleepiness (P = 0.0003) also improved. Conclusion: Hydrotherapy improves sleep quality, physical function, professional status, psychological disorders and physical symptoms in patients with fibromyalgia.
Keywords: sleep, fibromyalgia, hydrotherapy, quality of life.
INTRODUCTION
Fibromyalgia syndrome (FMS) is one of the most frequent rheumatologic diseases, characterized by diffuse and chronic musculoskeletal pain, with tender points in muscles or in myotendinous junctions. There are 18 tender points situated all over the body.1-3
Its etiology is still unknown, and its pathophysiology has not been totally understood. However, the following alterations have been evidenced: changes in the metabolism and oxygenation of muscle fibers; an unbalance between pain perception and the mechanisms of afferent pathways; and a reduction in the serotonin and endorphin levels.4 The pathophysiology of FMS is multicausal, and several experiments have demonstrated that uncoordinated mechanisms of nociception and pain inhibition result from sensory distortion.5
According to Weidebach,6 FMS was not well defined before the 1970s, when the first findings were published, those that determined a more deep research on the disease. Contrary to what was thought, it is not an inflammatory disease, generates no joint impairment, and causes no deformity. However, considering its chronic character, FMS has a negative impact on the patients' quality of life.
In 1990, the American College of Rheumatology (ACR) defined the following criteria for the classification and diagnosis of FMS: 1) frequent complaints of widespread pain for at least three months; and 2) presence of diffuse pain, on digital palpation, in at least 11 of the 18 standard tender points. Considering that both laboratory and imaging tests of inflammatory activity are normal, the diagnosis of FMS is primarily clinical.6,7
Ribeiro and Proietti8 have reported that in addition to pain and painful digital palpation of the tender points, patients also have nonrefreshed sleep, fatigue, morning stiffness, reduced physical functioning, anxiety, and depression, which reduce the patients' ability to perform daily domestic chores. All such symptoms make the social and professional life of patients with FMS difficult.
Approximately 75% of patients with FMS complain of poor sleep quality, which is attributed to an electroencephalic disorder, the absence of the last stage of sleep, called rapid eye movement (REM) sleep.9According to Dinges et al.,10 daytime sleepiness is one of the most frequent alterations of patients with FMS. Ferro et al.11 have shown the relationship between poor quality of sleep and higher predisposition to other diseases. Affleck et al.12 have shown the relationship between pain and sleep in patients with FMS, and have concluded that one of the major complaints is sleep deprivation related to widespread pain. Martinez et al.13 have shown the relationship between the number of tender points and loss of physical function, and that patients with FMS are at a disadvantage as compared to healthy individuals.
Hydrotherapy, usually performed in warm water (32ºC-33ºC), is strongly indicated for the treatment of FMS. During immersion, sensory stimuli compete with painful stimuli, interrupting the pain pathway.14 The effects of hydrotherapy are related to pain relief, a reduction in spasms, muscle relaxation, an increase in the range of motion, an increase in blood circulation, muscle strengthening, an increase in muscle resistance, and improvement in self-esteem.15
The present study aimed at assessing the improvement provided by hydrotherapy to patients with FMS regarding the following aspects: pain; sleep irregularities; muscle fatigue; depression; anxiety; and their reduced ability to perform daily activities.
METHODS
This is a self-controlled prospective study assessing 60 female patients clinically diagnosed with FMS according toACR criteria (frequent complaints of widespread pain for at least three months and diffuse pain, on digital palpation, in at least 11 of the 18 standard tender points). Of the 60 female patients assessed, 20 did not meet the inclusion criteria and 10 left the study because they could not abide by the time schedule. Thus, this study included 30 female patients aged 35-65 years, who had cognitive capacity to understand the purposes of the study and to sign the written informed consent, regardless of marital status, race, religion, and socioeconomic aspects. The following patients were excluded from the study: those already practicing bodybuilding and other physical activities at the gym before beginning the hydrotherapy program; and those who had any dermatologic disease, any cardiorespiratory change incompatible with the practice of aerobic exercises, and any severe comorbidity.
In this study, the hydrotherapy program was conducted in an indoor warm pool (32ºC) at the hydrotherapy sector of the Policlínica do Centro Universitário Adventista de São Paulo (UNASP). Data were collected only after approval by the institutional Ethics Committee.
All patients were assessed before and immediately after the intervention by the same observer, by using a form with demographic and clinical data. To assess the patients' quality of life, the Fibromyalgia Impact Questionnaire (FIQ) was used. It is an instrument to specifically assess the quality of life of patients with FMS, comprising 19 questions related to physical function, professional status, general well-being, psychological disorders (such as anxiety and depression), and physical symptoms (such as pain, sleep, fatigue, and stiffness), and organized into 10 items. The higher score, the greater the impact of FMS on the patient's quality of life. Burckhardt et al.16 have concluded that the FIQ is valid to be used in clinical and research situations.
To assess sleep quality, the Pittsburgh Sleep Quality Index (PSQI), whose reliability and validity had been previously established, was used. That questionnaire comprises 19 items, grouped into seven components, and each of the seven components has a maximum possible score of 3. Those components are as follows: 1) subjective sleep quality; 2) sleep latency; 3) sleep duration; 4) habitual sleep efficiency; 5) sleep disturbance; 6) use of sleeping medication; and 7) daytime dysfunction. The scores of the seven components are added together to obtain the global score of the PSQI, which ranges from 0 to 21. Scores of 0-4 indicate good sleep quality; of 5-10, poor quality; and over 10, sleep disorder.17
The Epworth Sleepiness Scale (ESS) was applied to assess and quantify daytime sleepiness during eight daily activities. The score obtained from the answers ranges from 0 to 24, 10 being the cutoff point for normality.18
The intervention protocol was applied twice a week, and comprised 15 group sessions of 60 minutes each, spent entirely in the water, respecting individual limits and each patient's progress. Arterial blood pressure was measured before every hydrotherapy session. Every therapeutic session comprised four phases: 1) warm-up obtained with straight line walking along the pool extension, in forward, backward and lateral stepping (for 5 minutes); 2) muscle stretching for upper and lower limbs and back (for 15 minutes - all stretching positions were held for 20 seconds and performed consecutively twice); 3) free active exercises for upper and lower limbs, initially non-weight bearing exercises, progressing to exercises with floatation devices and aquatic weights ranging from 0.5 kg-1 kg (for 30 minutes - trainings were performed as three sets of 12 repetitions); and 4) relaxation with active stretching for upper and lower limbs and posterior and anterior back muscles, associated with respiratory exercises, promoting progressive relaxation (for 10 minutes).
Statistical analysis
Data are expressed as means and standard deviations. Kolmogorov-Smirnov test was used to analyze data normality. Student t test was used to analyze pre- and post-intervention data. The statistical significance level adopted was P < 0.05. The sample size was calculated based on the outcome variable sleep quality, by use of the equation: expected effect/standard deviation (E/S). In this study, the expected effect was chosen as a 4-point decrease between pre- and post-intervention (minimal important clinical difference), and the standard deviation of the sample considered was the variability in the PSQI score. Thus, for an α = 0.05 and a statistical power of β = 0.8, 27 patients were necessary for sample power. All patients, even those participating in only one exercise session, were assessed by use of the intention-to-treat method.
RESULTS
This study included 30 female patients with FMS aged 35 to 65 years (mean age, 50.8 ± 12.5 years). Of those patients, 34.14% were professionally active, and 24.39% were on a leave of absence due to medical reasons. The mean number of tender points was 14.8 ± 3.1. Table 1 shows their other characteristics.
Regarding the impact of FMS on the patients' lives, they initially showed altered physical function, high work absenteeism rate, reduced ability to do job, severe pain, fatigue, morning tiredness, stiffness, and depression.
Immediately after the hydrotherapy program, those domains significantly improved (P < 0.0001). Anxiety significantly improved (P = 0.0013), but general well-being did not significantly improve (P = 0.05) (Table 2).
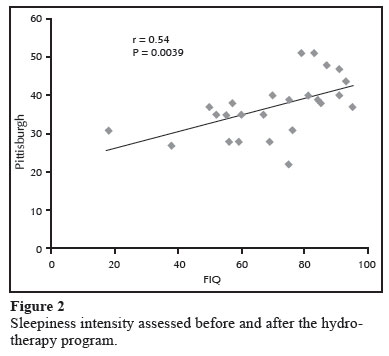
Regarding sleep, which was initially disturbed, a significant improvement was observed immediately after the hydrotherapy program (the score passed from 39.5 ± 6.29 to 33.2 ± 6.60; P < 0.0001) (Figure 1). Similarly, the sleep quality, initially altered, improved after the hydrotherapy program, with sleepiness intensity passing from 13.8 ± 7.28 to 10.1 ± 7.36; P = 0.0003 (Figure 2).
The impact of FMS did not correlated positively with sleep quality. However, the patients more affected by FMS reported worsening of their sleep quality (r = 0.54; P = 0.0039) (Figure 3).
Pain intensity correlated positively with sleepiness. However, the patients more affected by FMS reported increased sleepiness (r = 0.049; P = 0.0024) (Figure 4).
DISCUSSION
The original finding of this study was that hydrotherapy proved effective to improve the sleep quality and the physical function of patients with fibromyalgia after 15 sessions.
FMS is believed to have changes in the musculoskeletal, neuroendocrine, and central nervous systems. Because muscle pain is the major symptom of FMS, the primary cause of the syndrome was believed to be found in the musculoskeletal system. From the histological viewpoint, abnormalities in the muscular structure of patients with FMS, such as atrophic fibers and presence of elastic or reticular fibers that are not seen in the normal muscular tissue, were identified. It is worth noting the presence of functional changes, such as a reduction in highenergy phosphate concentration and in muscle oxygenation, and impaired blood flow.19 Such changes are similar to those therapy of non-physically-fit individuals with no disease. That is why those studies have not progressed.
Medicamentous therapy alone has proved not to be enough to treat the disease, and, thus, studies on alternative resources to reduce pain are required. Based on studies recommending physical therapy in the treatment of FMS, this study assessed the use of a pre-established program of water exercises to approach that syndrome.
The physiological effects of hydrotherapy originate from the combination of the physical effects of water (thermal/mechanical) and the effects of exercise.11 In fact, in the therapeutic pool, physical activities can be more easily performed due to flotation and a reduction in the gravitational force. This results in a less painful and easier practice of exercises as compared to that on the ground. Thus, in addition to muscle relaxation due to warm water, hydrotherapy provides enhancement in self-confidence and faster improvement of patients with fibromyalgia.20
The FIQ is an instrument that has been used in several clinical studies to assess physical function and the impact of fibromyalgia on patients' quality of life.21 It assesses quality of life specifically in patients with FMS, along with questions related to physical function, professional status, psychological disorders, and physical symptoms. Its Portuguese version was validated in 2006,22 and proved to be an instrument of easy understanding and applicability, valid and reliable to measure the physical function and the health status of patients with FMS, helping with its diagnosis and treatment.
This study confirms the findings about alterations in sleep quality and its improvement achieved after a hydrotherapy program. Studies have shown that nonrestorative sleep i present in 76%-90% of the patients with FMS, as compared to 10%-30% of healthy individuals.23 Poor sleep quality has been reported by 99% of the participants in the study by Theadom et al.,24 that assessed 101 patients diagnosed with FMS and evaluated by PSQI. Sleep quality was significantly predictive of pain, fatigue, and social functioning in patients with FMS.
Sleep quality is hard to define and measure, because of sleep complexity and variability among individuals. It comprises quantitative aspects, such as the number of night awakenings, sleep duration, and latency, and other aspects, such as sleep depth, tranquility, and rest sensation after sleep.25
In the present study, the instrument used to measure subjective sleep quality was the PSQI, whose Portuguese version was validated in 2008 by Bertolazi.26 It provides an index of severity and nature of the sleep disorder in the past month, being a safe, reliable, and non-invasive method, easy to apply.26 Before intervention, frequent night awakenings and few hours of actual sleep yielded a mean score of 39.5. After intervention, approximately 80% of the patients reported an improvement in their sleep quality, with a mean score reduction to 33. Such findings led us to state that hydrotherapy aids in improving sleep disorders, and, consequently, sleep quality.
The other instrument used was ESS, developed in 1991 by Dr. John W. Murray to measure excessive daytime sleepiness.27 According to the author, similarly to any other questionnaire, the measuring is not subjective, although it depends on the patient's reading ability, understanding, and honest answer.28 In this study, the patients reported excessive sleepiness during daily activities before intervention, their mean ESS score being 13.88. This excessive sleepiness can be associated with frequent night awakenings, which alter the sleep/wakefulness cycle. Those alterations in the sleep pattern can result in tiredness and fatigue. After intervention, their mean ESS score was 10, showing a significant improvement. In a study with 30 individuals with FMS and using the ESS, daytime sleepiness was associated with a higher severity of FMS and more marked changes in polysomnography.29
The improvement in hypersomnolence and in sleep quality can be related to an increase in serotonin levels, resulting from the aerobic exercises performed in water at 32ºC. According to Goldenberg et al.,30 patients with FMS have a reduction in serotonin levels, which alters their sleep. However, increased serotonin levels lead to increased melatonin production, which regulates sleep and improves its quality, providing the rest sensation.
In this study, patients with FMS showed a reduction in physical function. According to Chaitow et al.,31 patients with FMS have physically unfit muscles, tendency towards muscle microtraumas, pain, and chronic fatigue. The improvement in their physical function relates to the aerobic exercises performed in water, affecting mainly the cardiovascular and musculoskeletal systems, providing the following: an increase in cardiac output;32 rightward shift of the hemoglobin curve, increased muscle capillarity, and reduced resistance to O2 diffusion from red blood cells to contractile muscle fibers;33 and remodeling of exercised muscles, with a change of type II B fibers into type II A fibers, and an increase in the number, size and enzyme concentration of mitochondria in slow-contraction muscle cells.34
One limitation of this study was not performing polysomnography, which is the gold-standard test to assess sleep quality. However, the results of this study are not invalid, considering the reliability of its method.
CONCLUSION
Hydrotherapy is well indicated to patients with fibromyalgia, improving their sleep quality, physical function, professional status, psychological disorders and physical symptoms.
Assessing the quality of life before and after the intervention showed an improvement in the patients' subjective perception of their physical and psychological conditions. Thus, interventions to improve sleep quality and physical function can contribute to improve the health and quality of life of patients with FMS.
ACKNOWLEDGEMENTS
We thank Professor Elias F. Porto for his guidance and Professor Cláudia Kumpel for her thoughtfulness and help.
REFERENCES
-
1Santos AMB, Assumpção A, Matsutani LA, Pereira CAB, Lage LV, Marques AP. Depressão e qualidade de vida em pacientes com fibromialgia. Rev Bras Reumatol 2006;10:317-24.
-
2Heymann RE, Paiva ES, Helfenstein Junior M, Pollak DF, Martinez JE, Provenza JR et al Consenso brasileiro do tratamento da fibromialgia. Rev Bras Reumatol 2010;50(1):56-66.
-
3Gimenes RO, Santos EC, Silva TJPV. Watsu no tratamento da fibromialgia. Rev Bras Reumatol 2006;46(1):75-6.
-
4Okumus M, Gokoglu F, Kocaoglu S, Ceeceli E, Yorgancioglu ZR. Muscle performance in patients with fibromyalgia. Singapore Med J 2006;47(9):752-6.
-
5Martins IRM, Polvero LO, Rocha CW, Foss MH, Junior RS. Uso de questionários para avaliar a multidimensionalidade e a qualidade de vida do fibromiálgico. Rev Bras Reumatol 2012;52(1):16-26.
-
6Weidebach WFS. Fibromialgia: evidências de um substrato neurofisiológico. Rev Associação Médica Bras 2002;48(4):291-292.
-
7Wolfe F. Fibromyalgia: the clinical syndrome. Rheum Dis Clin North Am 1989;15(1):1-19.
-
8Ribeiro LS, Proietti FA. Fibromialgia e estresse infeccioso: possíveis associações entre a síndrome de fibromialgia e infecções viróticas crônicas. Rev Bras Reumatol 2005;45(1):20-9.
-
9Wolfe F, Simons DG, Fricton J, Bennett RM, Goldenberg DL, Gerwin R et al The fibromyalgia and myofascial pain syndromes: a preliminary study of tender points and trigger points in per-sons with fibromyalgia myofascial pain syndrome and no disease. J Rheumatol 1992;19(6):944-51.
-
10Campion MR. Efeitos fisiológicos, terapêuticos e psicológicos da atividade aquática. In: Campion MR. Hidroterapia: princípios e prática São Paulo: Manole, 2000; p. 3-4.
-
11Ferro CV, Ide MR, Streit MV. Correlation between sleep disorders and subjective parameters in subjects with fibromyalgia. Fisioter Mov 2008;21(1):33-8.
-
12Affleck G, Urrows S, Tennen H, Higgins P, Abeles M. Sequential daily relations of sleep, pain intensity, and attention to pain among women with fibromyalgia. Pain 1996;68(2-3):363-68.
-
13Martinez JE, Barauna Filho IS, Kubokawa K, Cevasco G, Pereira IS, Machado LAM. Avaliação da qualidade de vida de pacientes com fibromialgia através do "Medical Outcome Survey 36 Item Shortform Study". Rev Bras Reumatol 1999;39(6):312-6.
-
14Bates A, Hanson N. Exercícios aquáticos terapêuticos. In: Bates A, Hanson N. Síndrome da fibromialgia e exercício aquático São Paulo: Manole, 1998; p. 285-99.
-
15Soares MP. Hidroterapia no tratamento da osteoporose. Rio de Janeiro: Sprint, 1999.
-
16Burckhardt CS, Mannerkorpi K, Hedenberg L, Bjelle A. A randomized, controlled clinical trial of education and physical training for women with fibromyalgia. J Rheumatol 1994;21(4):714-20.
-
17Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28(2):193-213.
-
18Boari L, Cavalcante CM. Avaliação da escala de Epworth em pacientes com síndrome da apneia e hipopneia obstrutiva do sono. Rev Bras Otorrinolaringol 2004;70(6):752-6.
-
19Bastos CC, Oliveira EM. Síndrome da fibromialgia; tratamento em piscina aquecida. Lato & Sensu 2003;4(2):6.
-
20Salvador JP, Silva QF, Zirbes MCGM. Hidrocinesioterapia no tratamento de mulheres com fibromialgia: estudo de caso. Fisioterapia e Pesquisa 2005;11(1):27-36.
-
21Burckardt CS, Clark SR, Bennett RM. The Fibromyalgia Impact Questionnaire: Development end Validation. J Rheumatol 1991;18(5):728-33.
-
22Marques AP, Santos AMB, Assumpção A, Matsutani LA, Lage LV, Pereira CAB. Validação da Versão Brasileira do Fibromyalgia Impact Questionnaire (FIQ). Rev Bras Reumatol 2006;46(1):24-31.
-
23American Academy of Sleep Medicine. International classification of sleep disorders: Diagnostic and coding manual. 2.ed. West chester, IL: American Academy of Sleep Medicine; 2005.
-
24Theadom A, Cropley M, Humphrey KL. Exploring the role of sleep and coping in quality of life in fibromyalgia. J Psychosom Res 2007;62(2):145-51.
-
25Bixler EO, Kales A, Soldatos JD, Healey S. Prevalence of sleep disorders in the Los Angeles Metropolitan area. Am J Phsychiatry 1979;136(10):1257-62.
-
26Bertolazi AN. Tradução, adaptação cultural e validação de dois instrumentos de avaliação do sono: Escala de Sonolência de Epworthe Índice de Qualidade do Sono de Pittsburgh. Universidade Federal do Rio Grande do Sul. 2008.
-
27Johns MW. A new model for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991;14(6):540-5.
-
28Johns MW. Daytime sleepiness, snoring and obstructive sleep apnea. The Epworth Sleepiness Scale. Chest 1993;103(1):30-6.
-
29Sarzi PP, Rizzi M, Andreoli A, Panni B, Pecis M, Colombo S et al Hypersomnolence in fibromyalgia syndrome. Clin Exp Rheumatol 2002;20(1):69-72.
-
30Goldenberg DL. Fibromyalgia chronic fatigue syndrome and myofacial pain syndrome. Curr Opin Rheumatol 1991;3(2):247-58.
-
31Chaitow L. Síndrome da fibromialgia: um guia para tratamento. São Paulo: Manole, 2002.
-
32Wasserman K, Hansen JE, Sue DY, Casaburi R, Whipp BJ. Principles of exercise testing and interpretation. 3.ed. Philadelphia, PA: Lippincott Williams & Wilkins, 1999; p. 201-14.
-
33Hepple RT. Skeletal muscle: microcirculatory adaptation to metabolic demand. Med Sci Sports Exerc 2000;32(1):117-23.
-
34Starnes JW. Introduction to respiratory control in skeletal muscle. Med Sci Sports Exerc 1994;26(1):27-9.
Effect of hydrotherapy on quality of life, functional capacity and sleep quality in patients with fibromyalgia
Publication Dates
-
Publication in this collection
04 Dec 2012 -
Date of issue
Dec 2012
History
-
Received
08 Nov 2011 -
Accepted
05 Sept 2012