Abstract
This study analyzed the spatial and temporal distribution of cases of visceral leishmaniasis in the State of Maranhão in the period from 2000 to 2009. Based on the number of reported cases, thematic maps were prepared to show the evolution of the geographical distribution of the disease in the state. The MCMC method was used for estimating the parameters of the Bayesian model for space-time identification of risk areas. From 2000 to 2009 there were 5389 reported cases of visceral leishmaniasis, distributed in all 18 Regional Health Units in the state, with the highest indices in the cities of Caxias, Imperatriz, Presidente Dutra and Chapadinha. The Regional Health Units with the highest relative risks per biennium were: Caxias and Barra do Corda (2000-2001), Imperatriz and President Dutra (2002-2003), Imperatriz and Caxias (2004-2005), Presidente Dutra and Codó (2006-2007) and Imperatriz and Caxias (2008-2009). There was considerable geographic expansion of visceral leishmaniasis in Maranhão, thus highlighting the need to adopt more effective measures for prevention and control of the disease in the state.
Visceral leishmaniasis; Space-time analysis; Bayesian model
Resumo
Este estudo analisou a distribuição espaço-temporal dos casos de leishmaniose visceral (LV) no estado do Maranhão, no período de 2000 a 2009. A partir do número de casos notificados, foram elaborados mapas temáticos para demonstrar a evolução da distribuição geográfica da doença no estado. Utilizou-se o método MCMC para estimação dos parâmetros do modelo bayesiano espaço-temporal para a identificação das áreas de risco. De 2000 a 2009, foram notificados 5.389 casos de leishmaniose visceral, distribuídos em todas as 18 Unidades Regionais de Saúde do estado, com as maiores incidências em: Caxias, Imperatriz, Presidente Dutra e Chapadinha. As Unidades Regionais de Saúde com maiores riscos relativos por biênio foram: Caxias e Barra do Corda (2000-2001), Imperatriz e Presidente Dutra (2002-2003), Imperatriz e Caxias (2004-2005), Presidente Dutra e Codó (2006-2007), e Imperatriz e Caxias (2008-2009). Houve uma considerável expansão geográfica da LV no Maranhão, sendo necessária a adoção de medidas mais eficazes de prevenção e controle da doença no estado.
Leishmaniose visceral; Análise espaço-temporal; Modelo bayesiano
Introduction
Visceral Leishmaniasis is a serious public health problem that is widely prevalent in the world. It is currently amongst the seven endemics considered to be a priority in relation to health actions in the world. It is on the list of neglected tropical diseases that should be eradicated by 2015 according to the World Health Organization (WHO)11. Michalsky EM, França-Silva JC, Barata RA, Silva FOL, Loureiro AMF, Fortes-Dias CL, Dias ES. Phlebotominae distribution in Janaúba, an area of transmission for visceral leishmaniasis in Brazil. Mem Inst Oswaldo Cruz 2009; 104(1):56-61.,22. World Health Organization (WHO). Leishmaniasis: Magnitude of the problem 2010. [2010 set 14]. Disponível em: http://www.who.int/leishmaniasis/burden/magnitude/burden_magnitude/en/index.html
http://www.who.int/leishmaniasis/burden/...
.
Brazil accounts for 90% of the LV cases in Latin America and it is considered the country with the third highest rates of the disease in the world33. Bern C, Maguire JH, Alvar J. Complexities of Assessing the Disease Burden Attributable to Leishmaniasis. PLoS Negl Trop Dis 2008; 2(10):3010-3313.. In Brazil, between 1999 and 2008, more than one third of districts registered autochthonous cases and in these districts the disease has not been considered a priority. Also between 1980 and 2008 70 thousand cases of LV were registered in the country which resulted in the deaths of more than 3,800 people44. Werneck GL. Expansão geográfica da leishmaniose visceral no Brasil.Cad Saude Publica 2010; 26(4):644-645,55. Barreto ML, Teixeira MG, Bastos FI, Ximenes RAA, Barata RB, Rodrigues LC. Sucessos e fracassos no controle de doenças infecciosa no Brasil: o contexto social e ambiental, políticas, intervenções e necessidades de pesquisa. The Lancet 2011; (3):47-60..
Amongst all of the Federal states in Brazil, Maranhão has recorded the highest number of cases of LV. From 1999 to 2005 this state was the leader in the number of confirmed cases of the disease in Brazil. By 2009, 9,972 cases were registered with the majority being registered in the districts that make up the island of São Luís: São Luís, São José de Ribamar, Paço do Lumiar e Raposa66. Caldas AJM, Costa JM, Silva AA, Vinhas V, Barral A. A risk factors associated with asymptomatic infection by Leishmania chagasi in Northeast Brazil. Trans R Soc Trop Med Hyg 2002; 96(1):21-28.,77. Nascimento MDSB, Sousa EC, Silva LM, Leal PC, Cantanhede KL, Bezerra GFB, Viana GMC. Prevalence of infection by Leishmania chagasi using ELISA (rK39 and CRUDE) and Montenegro Skin Test in a endemic leishmaniasi área of Maranhão, Brasil. Cad Saude Publica 2005; 21(6):1801-1807..
Although there has been some recognition of the magnitude of the problem in Maranhão no studies have been done over the last decade covering the scale of the problem and the number of new cases. It also should be remembered that many studies66. Caldas AJM, Costa JM, Silva AA, Vinhas V, Barral A. A risk factors associated with asymptomatic infection by Leishmania chagasi in Northeast Brazil. Trans R Soc Trop Med Hyg 2002; 96(1):21-28.
7. Nascimento MDSB, Sousa EC, Silva LM, Leal PC, Cantanhede KL, Bezerra GFB, Viana GMC. Prevalence of infection by Leishmania chagasi using ELISA (rK39 and CRUDE) and Montenegro Skin Test in a endemic leishmaniasi área of Maranhão, Brasil. Cad Saude Publica 2005; 21(6):1801-1807.-88. Mendes WS, Trovão JR, Silva AAM, Silva AR, Costa JMC. Expansão da leishmaniose visceral americana em São Luis, Maranhão, Brasil. Rev Soc Bras Med Trop 2002; 35(3):227-231. were done with a view to understanding LV’s epidemiology in the districts that make up the island of São Luís (São Luís, São José de Ribamar, Paço do Lumiar e Raposa), however we do not have any data regarding the progression of the disease in the state of Maranhão. Therefore we believe that a good grasp of the nature of the problem or the risk hot spots within the regions is essential for designating adequate resources to combat the disease and for taking appropriate health care actions.
Different Bayesian saptio-temporal models have been used to get a better understanding of the dynamics involved in the transmission of LV. This type of modeling allows for the obtaining of stable estimates of the spacial variations of the relative risks or the disease incidents99. Spiegelhalter DJ, Best NG, Carlin BP. Bayesian measures of model complexity and fit. J. R. Statist Soc B 2002; 64(4):583-639.
10. Barcellos C, Ramalho W. Situação atual do geoprocessamento e da análise de dados espaciais em saúde no Brasil. Informática Pública 2002; 4(2):221-230.-1111. Chiesa AM, Westphal MF, Kashiwagi NM. Geoprocessamento e a promoção da saúde: desigualdades sociais e ambientais em São Paulo. Rev Saude Publica 2002; 36:559-567.. However when the number of cases and the population at risk in an area over a specified period of time are low, it becomes difficult to obtain risk estimates that are near to reality. But it may be more beneficial to use information from surrounding areas to estimate the relative risks.
The use of these models in the area of epidemiology have been present in a number of studies. Vieira et al.1212. Vieira CP, Oliveira AM, Rodas LAC, Dibo MR, Guirado MM, Chiaravalloti Neto F. Temporal, spatial and spatiotemporal analysis of the occurrence of visceral leishmaniasis in humans in the City of Birigui, State of São Paulo, from 1999 to 2012. Rev Soc Bras Med Trop 47(3):350-358.described the spatial-temporal behavior of LVH in Birigui (SP). Other studies used the same model for other endemic diseases, such as that of Souza et al.1313. Sousa WV, Barcellos CC, Brito AM, Carvalho MS, Cruz OGC, Albuquerque MFM, Alves KR, Lapa TM. Aplicação de modelo bayseano empírico na análise espacial da ocorrência de hanseníase. Rev Saude Publica2001; 35(5):474-480.. They analyzed the spatial distribution of leprosy in the city of Recife. This was also done by Nobre et al.1414. Nobre AA, Schmidt AM, Lopes HS. Spatio-temporal models for mapping the incidence of malaria in Pará. Envirometrics 2005; 16(3):291-304.. They analyzed the number of malaria cases in Pará between 1996 and 1998.
In this present study the aim is to analyze spatial-temporal distribution of LV cases in Maranhão between 2000 and 2009.
Methods
This is an ecological study looking back at the history of LV cases that were registered according to the residents in the state of Maranhão between 2000 to 2009.
The state of Maranhão, that has as its capital São Luís, is located in the western region in the north east of Brazil. It covers an area of 331.933,3 km22. World Health Organization (WHO). Leishmaniasis: Magnitude of the problem 2010. [2010 set 14]. Disponível em: http://www.who.int/leishmaniasis/burden/magnitude/burden_magnitude/en/index.html
http://www.who.int/leishmaniasis/burden/...
, and it has a population estimated at around 6.184.538 inhabitants1515. Feitosa AC, Trovão JR. Atlas Escolar do Maranhão: Espaço Geo-histórico e Cultural. João Pessoa: Grafset; 2006.,1616. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo demográfico - 2010. [acessado 2011 nov 10]. Disponível em: http://www.ibge.gov.br/estadosat/perfil.php?sigla=ma
http://www.ibge.gov.br/estadosat/perfil....
. Maranhão is bordered by the following: the Atlantic ocean to the north, the state of Piauí to the east, the state of Tocantins to the south and south east and the state Pará to the west. The state has: 217 districts, 5 mesoregions, 21 microregions and 18 region health units (URS).
In this study the spatial units that were analyzed were the regional health units represented by a group of neighboring districts that had similarities in relation to their: geography, climate and socio-economic position. They all also had a political/administrative office of the state Ministry for Health in Maranhão with the task of improving health care in the state. These regional health units were: Açailândia, Bacabal, Balsas, Barra do Corda, Caxias, Chapadinha, Codó, Imperatriz, Itapecuru-Mirim, Pedreiras, Pinheiro, Presidente Dutra, Rosário, Santa Inês, São Luís, São João dos Patos, Viana and Zé Doca1515. Feitosa AC, Trovão JR. Atlas Escolar do Maranhão: Espaço Geo-histórico e Cultural. João Pessoa: Grafset; 2006.,1616. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo demográfico - 2010. [acessado 2011 nov 10]. Disponível em: http://www.ibge.gov.br/estadosat/perfil.php?sigla=ma
http://www.ibge.gov.br/estadosat/perfil....
.
The population in the state of Maranhão between 2000 and 2009 was affected by all of the cases of Visceral Leishmaniasis. The information was collected from the Information System for the Notification of Diseases (SINAN) database. This was from the Secretary of State for Health in Maranhão. We excluded all information that could possibly be used to identify participants in the study in order to respect their privacy. We also took out information which was: inconsistent, imprecise, incomplete or duplicated (i.e. two or more registers of the same case). We included cases where the individual presented symptoms of LV such as: a fever for more than two weeks, hepatoesplenomegaly, and/or a confirmed diagnosis of the disease through a bone marrow aspiration showing positive forLeishmania sp. We also considered the area for URS, suggesting autochthony for the disease.
Information from the Brazilian Institute for Geography and Statistics1616. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo demográfico - 2010. [acessado 2011 nov 10]. Disponível em: http://www.ibge.gov.br/estadosat/perfil.php?sigla=ma
http://www.ibge.gov.br/estadosat/perfil....
was used to estimate and calculate the density of the population in each period for URSs.
The number of incidents of LV was calculated based on the total amount of cases registered in each URS. We then divided the estimated density population in each URS and multiplied this number by 100,000. In this way we were able to ascertain the number of those stuck down by the disease per 100,000 inhabitants.
We used the bayesian spatial-temporal model in order to obtain relative risk estimates for LV. Y represented the variable which was the number of LV registered cases at the URSs (i-ésima) during t year. i = 1,...,18 and t = 1,..., 10 (years 2000 to 2009). Foryit we used the Poisson distribution with an average µit= eitρρitor in a logarithmic formlog(µit)= log eit+ log ρit, beingeit which was the number cases expected at the URSs i in time t andρit o the relative risk at the URSs i in time t.
The number of expected cases eitwere known quantities obtained from the population of each URS in the period between 2000 and 2009. This was calculated byρit, multiplied by the number of cases at the URSs and i by the total population in all of the URSs. This was the equation:

Using this method in this study the relative riskρit was estimated through the use of the Bayesian spatial-temporal model that was adapted by Nobre et al.88. Mendes WS, Trovão JR, Silva AAM, Silva AR, Costa JMC. Expansão da leishmaniose visceral americana em São Luis, Maranhão, Brasil. Rev Soc Bras Med Trop 2002; 35(3):227-231.. The model used assumed that log(ρit) = βt + bit , and temporal effort βt =βt – 1 +vt , for t=2, ..., 10. This model considers that the relative risk is related to the temporal effectβt, which is dependent on the effort for the previous year with a random error ofvt, and a spatial-temporal effort bit.. Apart from this, the random error vt is normally distributed with an average of zero and an unknown variant , designated byvt ~Normal(0, ), andβ1 ~Normal(0, ).
With the Bayesian approach is it necessary to specify the a priori distribution for the model parameters in the study. For the parameterbit, an a priori autoagressive conditional distribution was primarily used (CAR) with a variant , as proposed by Besag and Kooperberg1717. Besag J, Kooperberg C. On Conditional and intrinsic autoregressions. Biometrika 1995; 82(4):733-746., denoted bybit ~ CAR ( ), which determines the structure of the spacial correlation, given by:

Where δi is the entirety of an area considered to be neighboring thei-ésima area according to the criteria for neighbors; represents the variability in the t andwij corresponds to the weight of the neighbor from the area j and for the areai, which defines the matrix for the neighborhood1818. Bernardinelli L, Clayton D, Montomoli C. Bayesian estimates of disease maps: how important are priors? Statistics in Medicine1995; 14(21-22):2411-2431.,1919. Kelsal J, Wakefield J. Modeling spatial variation in disease risk: a geostatistical approach. Journal of the American Statistical Association 2002; 97(459):692-701.. Sometime afterwardsbit was considered for normal distribution with an average of zero and variants , in other words, without considering the spatial correlation structure.
In order to define neighboring areas in specific areas i, and its respective weight, we used the adjacency criteria that allows for the consideration of neighbors from other areas i limited to that bordered. In relation to defining the weights wijwe considered for wijbinary values, meaning wijis going to be equal to 1, if the URS i andj are adjacent and 0 if it is to the contrary1717. Besag J, Kooperberg C. On Conditional and intrinsic autoregressions. Biometrika 1995; 82(4):733-746.
18. Bernardinelli L, Clayton D, Montomoli C. Bayesian estimates of disease maps: how important are priors? Statistics in Medicine1995; 14(21-22):2411-2431.-1919. Kelsal J, Wakefield J. Modeling spatial variation in disease risk: a geostatistical approach. Journal of the American Statistical Association 2002; 97(459):692-701..
Finally for the hyper-parameters 1/, 1/ and 1/ , were considered a priori independent distribution gammas with an average and variance equal to one1414. Nobre AA, Schmidt AM, Lopes HS. Spatio-temporal models for mapping the incidence of malaria in Pará. Envirometrics 2005; 16(3):291-304.. Estimates of the parameters and hyper-parameters of interest were obtained from the Monte Carlo Method via the Markov Prison (MCMC) where the WinBugs (Win Bayesian Inference Using Gibbs Sampling) version 1.499. Spiegelhalter DJ, Best NG, Carlin BP. Bayesian measures of model complexity and fit. J. R. Statist Soc B 2002; 64(4):583-639. statistical program has been implemented.
Three prisons were used simultaneously starting from different points, with each parameter monitored after a burn-in of 5,000 iterations and these simulations were discarded. Afterwards, 10,000 distribution values a posteriori for each parameter was generated. The criteria for convergence was based on a visual inspection of charts from Markov Prison.
Maps giving risk estimates from the Bayesian model were created in theTerraView Program version 3.5 and was presented biennially.
Following ethical norms involving research of human beings, in accordance with Resolutions 196/96 and 466/12 of the National Council for Health, the study was examined and approved by the Ethics Committee on Research at the University Hospital at the Federal University of Maranhão.
Results
Between 2000 and 2009 5,389 cases of LV was registered, with the highest numbers of incidents at the URSs: Caxias (36,1/100.000 Inhab.), Imperatriz (30,8/100.000 Inhab.), Presidente Dutra (10,8/100.000 Inhab.), Codó (10,4/100.000 Inhab.) and Barra do Corda (9,8/100.000 Inhab.). The cases were registered in all of the URSs, with the reemergence of former hotspots for the disease such as at the following URSs: Caxias, Imperatriz e São Luís (6,5/100.000 hab.). There was the emergence of new hotspots for cases at the following URSs: hapadinha (5,7/100.000 hab.), Itapecuru-Mirim (5,5/100.000 hab.), Balsas (5,7/100.000 hab.), São João dos Patos (5,5/100.000 hab.), and Pedreiras (5,5/100.000 hab.). See Table 1.
Upon evaluating the number LV cases per year (Table 1) we noted that from 2007 (5,5/100.000 Inhab.) and 2009 (5,6/100.000 Inhab.) there was the lowest numbers of LV incidents and in 2000 (15,6/100.000 Inhab.) we recorded the highest numbers. On the other hand a completely different situation was seen at the URS in São Luís. 790 absolute cases were registered putting it in third place and the number of incidents was 6,5/100.000 inhabitants (in sixth position). This showed an important reduction in the main focus of the disease in the state (Table 1).
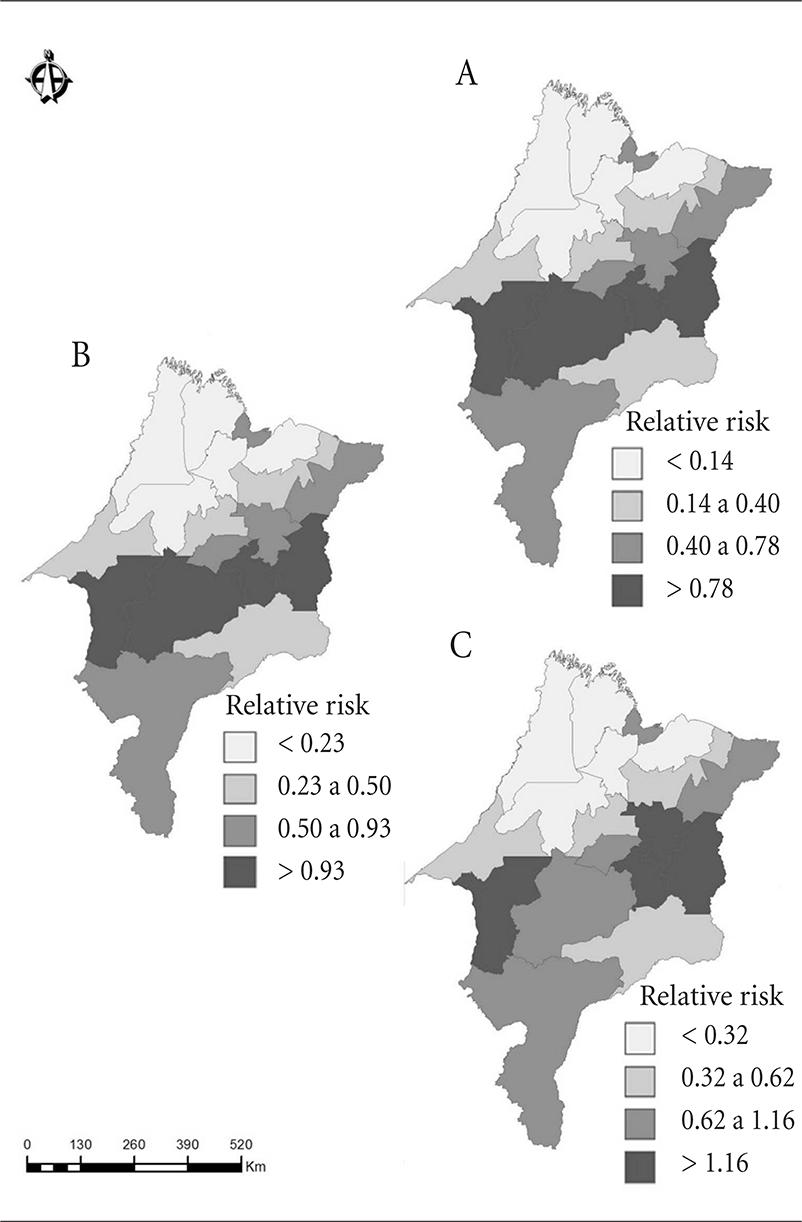
Figure 1 and Figure 2 shows the temporal biennial progression of LV at the URSs in the study. The following URSs over two years showed the highest estimated relative risks: Caxias, Barra do Corda, Imperatriz and Presidente Dutra from 2000-2001 (RR = 0,8-5,2) and 2002-2003 (RR = 0,9-4,3). The following URSs over the next two years showed the highest risks: Imperatriz, Caxias, Presidente Dutra and Codó from 2004-2005 (RR = 1,2-3,7) and 2006-2007 (RR = 1,4-3,1) to greatest risks. Also the following URSs registered the highest risk for 2008-2009: Imperatriz, Caixas, Codó and Itapecuru-Mirim with relative risks that varied between 1,9 and 2,6.
Spatial Temporal analysis of the areas of risk for Visceral Leishmaniasis (LV) for Regional Health Units (URS) in the state of Maranhão, bieannial: 2000-2001 (A), 2002-2003(B), 2004-2005(C).
Spatial Temporal analysis of the areas of risk for Visceral Leishmaniasis (LV) for Regional Health Units (URS) in the state of Maranhão, bieannial: 2006-2007 (A), 2008-2009 (B).
Discussion
This study showed that there was an accentuated geographical distribution of LV amongst the region health units in Maranhão between 2000 and 2009. Aside from the appearance of new hotspots, previous hotspot areas continued to show occurrences of the disease. This demonstrates that the existing control measures have not been sufficient to neither control LV endemic areas nor to prevent the outbreaks in areas that were then considered safe.
LV is a recognized public health problem in the state of Maranhão since 198088. Mendes WS, Trovão JR, Silva AAM, Silva AR, Costa JMC. Expansão da leishmaniose visceral americana em São Luis, Maranhão, Brasil. Rev Soc Bras Med Trop 2002; 35(3):227-231.,2020. Coutinho AC, Silva EL, Caldas, AJM. Análise dos casos e óbitos por leishmaniose visceral no estado do Maranhão, no período de 2000 a 2008.Rev Pesq Saúde 2012; 13(1):11-15.. During the period of this study we observed an expansion of the disease not only in the areas with the greatest concentration of cases such as São Luís, Imperatriz e Caxias, but also in other regions. Various factors may have contributed to the spreading of this disease in the state. Among them, we can highlight the intense inter-municipal migratory flux which has also occurred at interstate level. This is the case for cities near to the Vale de Rio Doce railway line or Teresina (PI). This is also the case for cities with a large amount of deforestation.
These types of population movements facilitate the introduction of LV etiological agents in once disease free areas. It also makes endemic areas even more susceptible to the disease. Many families that have migrated from rural areas have settled on the outskirts of the cities which vary in size. They lived in densely populated areas where there is little infrastructure or basic sanitation. This was the case in São Luis (MA) in the 80s where intense migration occurred due to the beginning of big industrial projects. This sparked an epidemic66. Caldas AJM, Costa JM, Silva AA, Vinhas V, Barral A. A risk factors associated with asymptomatic infection by Leishmania chagasi in Northeast Brazil. Trans R Soc Trop Med Hyg 2002; 96(1):21-28.,77. Nascimento MDSB, Sousa EC, Silva LM, Leal PC, Cantanhede KL, Bezerra GFB, Viana GMC. Prevalence of infection by Leishmania chagasi using ELISA (rK39 and CRUDE) and Montenegro Skin Test in a endemic leishmaniasi área of Maranhão, Brasil. Cad Saude Publica 2005; 21(6):1801-1807..
However we observed rises in cases in municipalities on the continent that did not previously register the disease. There was a considerable fall in the number of LV cases in the districts on the island of São Luís in the 90s66. Caldas AJM, Costa JM, Silva AA, Vinhas V, Barral A. A risk factors associated with asymptomatic infection by Leishmania chagasi in Northeast Brazil. Trans R Soc Trop Med Hyg 2002; 96(1):21-28.,77. Nascimento MDSB, Sousa EC, Silva LM, Leal PC, Cantanhede KL, Bezerra GFB, Viana GMC. Prevalence of infection by Leishmania chagasi using ELISA (rK39 and CRUDE) and Montenegro Skin Test in a endemic leishmaniasi área of Maranhão, Brasil. Cad Saude Publica 2005; 21(6):1801-1807.,99. Spiegelhalter DJ, Best NG, Carlin BP. Bayesian measures of model complexity and fit. J. R. Statist Soc B 2002; 64(4):583-639. up to the present day. Other studies that evaluated the spatial temporal distribution of LV in various Brazilian regions, utilizing different methods, also showed a high number of cases in locations that had not registered the disease2121. Mestre GLC, Fontes CJF. A expansão da epidemia da leishmaniose visceral no estado de Mato Grosso, 1998-2005. Rev Soc Bras Med Trop 2007; 40(1):42-48.
22. Dantas-Torres F, Brandão-Filho S. Expansão geográfica da leishmaniose visceral no Estado de Pernambuco. Rev Soc Bras Med Trop 2006; 39(4):352-356.-2323. Margonari C, Freitas CR, Ribeiro RC, Moura ACM, Timbo M, Gripp AH, Pessanha JE, Dias ES. Epidemiology of visceral leishmaniasis through spatial analysis, in Belo Horizonte municipality, state of Minas Gerais, Brazil.Mem do Inst Oswaldo Cruz 2006; 101(1):31-38.. This geographical expansion of the disease could be associated with the low impact of the control measures that were used. It may also be due to the way how the disease is diagnosed and the registration system. This could also be the case in relation to the mobility of the people.
In spite of the number of new cases that remained high through the study, we noticed a reduction in the incidents and an increase in the geographical distribution of LV in Maranhão with variations among URSs. Furlan2424. Furlan MBG. Epidemia de leishmaniose visceral no município de Campo Grande-MS, 2002-2006. Epidemiol Serv Saúde 2010; 19(1):15-24. observed that the differences of the incidents among the regions maybe to do with the different contexts for each region which subsequently influenced the spread of LV.
Certainly there were other factors that must have influenced the geographical progression of LV in Maranhão. It seems that the majority of cases are associated with anthropic pressure on the environment and the disorderly occupation of areas. Another important aspect is the capacity of the sandflyLutzomyia longipalpis (Diptera: Which can be found in practically the entire state2525. Rebêlo JMM, Rocha RV, Moraes JLP, Silva CRM, Silva LF, Alves GA. The fauna of phlebotomines (Diptera, Psychodidae) in diferente phytogeographic regions of the state of Maranhão. Brazil. Rev Bras Entomol 2010; 54(3):494-500..
The elevated relative risk in the decade that the study covered in the Imperatriz e Caxias URSs, reinforce the idea detailed by Dantas-Torres and Brandão-Filho2222. Dantas-Torres F, Brandão-Filho S. Expansão geográfica da leishmaniose visceral no Estado de Pernambuco. Rev Soc Bras Med Trop 2006; 39(4):352-356. that beating the disease which is typically prevalent in rural areas can and has been achieved in urban and peri-urban medium and large cities. On the other hand, the destruction of nature for the construction of social housing and to widen roads may have contributed to the increase in the vector density in the URSs, particularly in Imperatriz. This was due to the population increases because of the soya plantation and the extraction of wood in the pre-amazon region.
Mestre e Fontes2121. Mestre GLC, Fontes CJF. A expansão da epidemia da leishmaniose visceral no estado de Mato Grosso, 1998-2005. Rev Soc Bras Med Trop 2007; 40(1):42-48.identified the wide geographical expansion of LV in Mato Grosso, affecting urban and peri-urban areas in various districts. This was also the case for the suburbs in the state where the spread of the disease went hand in hand with the disorderly occupation of urban areas and migratory flux. As was the case in Maranhão Werneck et al.2626. Werneck GL, Pereira TJCF, Farias GC, Silva FO, Chaves FC, Gouvêa MV, Costa CHN, Carvalho FAA. Avaliação da efetividade das estratégias de controle da leishmaniose visceral na cidade de Teresina, Estado do Piauí, Brasil: resultados do inquérito inicial -2004. Epidemiol Serv Saúde 2008; 17(2):87-96. blamed the lack of an effective and permanent monitoring system with human resources and the lack of sufficient finances to aid in the control of LV in urban centers.
One of the major problems found during this study was the lack of or inconsistencies in the information which resulted in variations in numbers which could not be explained. The data that was filled in was understood as the result of routine activities in health services. In spite of the work of Epidemiological Monitoring Departments in the districts, little contentment was registered.
Despite the aforementioned limitations, the results of the study allowed for a diagnosis of the geographical expansion of LV in the state of Maranhão. We were able to map the areas of risks for occurrences and incidents of the cases. We hope to have contributed to the planning of health actions and in the design of a state plan for management in this area which is more closely aligned to the epidemiological and social reality of the state.
The number of cases of LV in Maranhão is still very high and can be found throughout all of the URSs. This is specially the case in areas where the population has grown during the period of the study. However what is needed are more effective prevention and control measures to control the disease in the state.
Referências
-
1Michalsky EM, França-Silva JC, Barata RA, Silva FOL, Loureiro AMF, Fortes-Dias CL, Dias ES. Phlebotominae distribution in Janaúba, an area of transmission for visceral leishmaniasis in Brazil. Mem Inst Oswaldo Cruz 2009; 104(1):56-61.
-
2World Health Organization (WHO). Leishmaniasis: Magnitude of the problem 2010. [2010 set 14]. Disponível em: http://www.who.int/leishmaniasis/burden/magnitude/burden_magnitude/en/index.html
» http://www.who.int/leishmaniasis/burden/magnitude/burden_magnitude/en/index.html -
3Bern C, Maguire JH, Alvar J. Complexities of Assessing the Disease Burden Attributable to Leishmaniasis. PLoS Negl Trop Dis 2008; 2(10):3010-3313.
-
4Werneck GL. Expansão geográfica da leishmaniose visceral no Brasil.Cad Saude Publica 2010; 26(4):644-645
-
5Barreto ML, Teixeira MG, Bastos FI, Ximenes RAA, Barata RB, Rodrigues LC. Sucessos e fracassos no controle de doenças infecciosa no Brasil: o contexto social e ambiental, políticas, intervenções e necessidades de pesquisa. The Lancet 2011; (3):47-60.
-
6Caldas AJM, Costa JM, Silva AA, Vinhas V, Barral A. A risk factors associated with asymptomatic infection by Leishmania chagasi in Northeast Brazil. Trans R Soc Trop Med Hyg 2002; 96(1):21-28.
-
7Nascimento MDSB, Sousa EC, Silva LM, Leal PC, Cantanhede KL, Bezerra GFB, Viana GMC. Prevalence of infection by Leishmania chagasi using ELISA (rK39 and CRUDE) and Montenegro Skin Test in a endemic leishmaniasi área of Maranhão, Brasil. Cad Saude Publica 2005; 21(6):1801-1807.
-
8Mendes WS, Trovão JR, Silva AAM, Silva AR, Costa JMC. Expansão da leishmaniose visceral americana em São Luis, Maranhão, Brasil. Rev Soc Bras Med Trop 2002; 35(3):227-231.
-
9Spiegelhalter DJ, Best NG, Carlin BP. Bayesian measures of model complexity and fit. J. R. Statist Soc B 2002; 64(4):583-639.
-
10Barcellos C, Ramalho W. Situação atual do geoprocessamento e da análise de dados espaciais em saúde no Brasil. Informática Pública 2002; 4(2):221-230.
-
11Chiesa AM, Westphal MF, Kashiwagi NM. Geoprocessamento e a promoção da saúde: desigualdades sociais e ambientais em São Paulo. Rev Saude Publica 2002; 36:559-567.
-
12Vieira CP, Oliveira AM, Rodas LAC, Dibo MR, Guirado MM, Chiaravalloti Neto F. Temporal, spatial and spatiotemporal analysis of the occurrence of visceral leishmaniasis in humans in the City of Birigui, State of São Paulo, from 1999 to 2012. Rev Soc Bras Med Trop 47(3):350-358.
-
13Sousa WV, Barcellos CC, Brito AM, Carvalho MS, Cruz OGC, Albuquerque MFM, Alves KR, Lapa TM. Aplicação de modelo bayseano empírico na análise espacial da ocorrência de hanseníase. Rev Saude Publica2001; 35(5):474-480.
-
14Nobre AA, Schmidt AM, Lopes HS. Spatio-temporal models for mapping the incidence of malaria in Pará. Envirometrics 2005; 16(3):291-304.
-
15Feitosa AC, Trovão JR. Atlas Escolar do Maranhão: Espaço Geo-histórico e Cultural João Pessoa: Grafset; 2006.
-
16Instituto Brasileiro de Geografia e Estatística (IBGE). Censo demográfico - 2010. [acessado 2011 nov 10]. Disponível em: http://www.ibge.gov.br/estadosat/perfil.php?sigla=ma
» http://www.ibge.gov.br/estadosat/perfil.php?sigla=ma -
17Besag J, Kooperberg C. On Conditional and intrinsic autoregressions. Biometrika 1995; 82(4):733-746.
-
18Bernardinelli L, Clayton D, Montomoli C. Bayesian estimates of disease maps: how important are priors? Statistics in Medicine1995; 14(21-22):2411-2431.
-
19Kelsal J, Wakefield J. Modeling spatial variation in disease risk: a geostatistical approach. Journal of the American Statistical Association 2002; 97(459):692-701.
-
20Coutinho AC, Silva EL, Caldas, AJM. Análise dos casos e óbitos por leishmaniose visceral no estado do Maranhão, no período de 2000 a 2008.Rev Pesq Saúde 2012; 13(1):11-15.
-
21Mestre GLC, Fontes CJF. A expansão da epidemia da leishmaniose visceral no estado de Mato Grosso, 1998-2005. Rev Soc Bras Med Trop 2007; 40(1):42-48.
-
22Dantas-Torres F, Brandão-Filho S. Expansão geográfica da leishmaniose visceral no Estado de Pernambuco. Rev Soc Bras Med Trop 2006; 39(4):352-356.
-
23Margonari C, Freitas CR, Ribeiro RC, Moura ACM, Timbo M, Gripp AH, Pessanha JE, Dias ES. Epidemiology of visceral leishmaniasis through spatial analysis, in Belo Horizonte municipality, state of Minas Gerais, Brazil.Mem do Inst Oswaldo Cruz 2006; 101(1):31-38.
-
24Furlan MBG. Epidemia de leishmaniose visceral no município de Campo Grande-MS, 2002-2006. Epidemiol Serv Saúde 2010; 19(1):15-24.
-
25Rebêlo JMM, Rocha RV, Moraes JLP, Silva CRM, Silva LF, Alves GA. The fauna of phlebotomines (Diptera, Psychodidae) in diferente phytogeographic regions of the state of Maranhão. Brazil. Rev Bras Entomol 2010; 54(3):494-500.
-
26Werneck GL, Pereira TJCF, Farias GC, Silva FO, Chaves FC, Gouvêa MV, Costa CHN, Carvalho FAA. Avaliação da efetividade das estratégias de controle da leishmaniose visceral na cidade de Teresina, Estado do Piauí, Brasil: resultados do inquérito inicial -2004. Epidemiol Serv Saúde 2008; 17(2):87-96.
Publication Dates
-
Publication in this collection
Dec 2015
History
-
Received
02 Mar 2015 -
Reviewed
07 Apr 2015 -
Accepted
09 Apr 2015