Abstract
This study aims to check the association between overweight and obesity and sociodemographic, behavioral and clinical factors in menopausal women. A cross-sectional study of a sample of 253 menopausal women who answered questions about socioeconomic and demographic factors, health in general, eating habits and behaviors. Body-mass index (BMI) was used to assess participant nutritional status. The Menopause Rating Scale (MRS) was used to assess quality of life. To assess sexual performance we used SQ-F (Sexual Quotient, Female Version). We used bivariate analysis and hierarchical multiple regression to identify the factors associated with being overweight during menopause. Using BMI we found that 30.8% of the sample was overweight and 35.2% obese, totaling 66% overweight women in the sample. In the multiple analysis, not owning a home, the severity of symptoms using MRS, use of continuous use medication and having been on any type of diet were associated with being overweight or obese. Nutritional intervention for weight control and changing behaviors could produce considerable benefits in terms of the health and quality of life of menopausal women.
Obesity; Menopause; Women’s health
Resumo
O objetivo deste estudo é verificar a associação entre sobrepeso e obesidade e fatores sociodemográficos, comportamentais e clínicos em mulheres climatéricas. Estudo transversal, com amostra de 253 mulheres climatéricas, que responderam questões sobre fatores socioeconômicos e demográficos, saúde geral, hábitos alimentares e comportamentais. Para a avaliação do estado nutricional, foi utilizado índice de massa corpórea (IMC). Para avaliação da qualidade de vida foi utilizado a Menopause Rating Scale (MRS). Empregou-se o Quociente Sexual (QS-F)-Versão Feminina para a avaliação do desempenho sexual. Utilizou-se análise bivariada e regressão múltipla hierarquizada para identificar fatores associados ao sobrepeso e à obesidade no climatério. Pela análise do IMC, 30,8% apresentaram sobrepeso e 35,2%, obesidade, totalizando 66% de excesso de peso. Na análise múltipla, não possuir casa própria, gravidade de sintomas pela avaliação do MRS, uso de medicamento de forma contínua e ter feito algum tipo de dieta apresentaram associação com sobrepeso e obesidade. Intervenção nutricional, visando ao controle de peso e mudanças de hábitos de vida, poderá resultar em benefícios consideráveis relativos à saúde e qualidade de vida das mulheres climatéricas.
Obesidade; Climatério; Saúde da mulher
Introduction
Obesity is recognized as a multi-factor metabolic change of epidemic proportions. Its prevalence has been increasing at alarming rates in almost all countries, becoming a serious public health problem. 64.9% of the women in Brazil are overweight or obese. The problem is even greater in women between the ages of 55 and 6411. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de orçamentos familiares 2008-2009. Antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. Rio de Janeiro; 2010. [citado 2011 jun 4]. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009_encaa/pof_20082009_encaa.pdf
http://www.ibge.gov.br/home/estatistica/...
, and in women with fewer years of schooling22. Linhares RS, Horta BL, Gigante DP, Dias-da-Costa JS, Olinto MTA. Distribuição de obesidade geral e abdominal em adultos de uma cidade no Sul do Brasil. Cad Saude Publica 2012; 28(3):438-447..
Multiple factors are mentioned as the main causes of obesity in women, including changes inherent to the aging process itself, as well as changes in lifestyle such as a less active lifestyle and increased consumption of energy dense food33. Almeida JPM, Carnide C, Branquinho M, Geraldes F, Águas F. Impacto da terapia hormonal sobre o peso corpóreo. Rev Bras Ginecol Obstet 2011; 33(10):310-314.. Researchers have found that the obesity epidemic is caused by changes in the economic, social and physical environments4.
Brazil is seeing a rapid ageing of its population, and life expectancy among women is longer than it is for men. Because of this, more women will experience the changes associated with menopause55. Tannure MC, Alves M, Sena RR, Chianca TCM. Perfil epidemiológico da população idosa de Belo Horizonte, MG, Brasil. Rev. bras. enferm. 2010; 63(5):817-822., which is why this period deserves greater attention from the public health system.
The World Health Organization defines menopause as a natural phase in a woman’s life that corresponds to the transition between the reproductive and non-reproductive periods, to a decrease in the production of steroid hormones66. Mundial de la Salud (OMS). Investigaciones sobre la menopausa en los anos noventa: informe de un grupo cientifico de la OMS. Ginebra: OMS; 1996. (OMS, Serie de informes técnicos, nº 866).. This period starts at around age 40 and lasts until age 60-65. Menopause is a milestone in this phase, normally happening at around 49 years of age, diagnosed once a woman has not experienced a menstrual period for twelve consecutive months66. Mundial de la Salud (OMS). Investigaciones sobre la menopausa en los anos noventa: informe de un grupo cientifico de la OMS. Ginebra: OMS; 1996. (OMS, Serie de informes técnicos, nº 866)..
Hypoestrogenism resulting from menopause is mentioned as the main cause of obesity, vasomotor, urogenital and psychological symptoms, as well as for poorer sexual performance and the high profile or morbimortality in women after the age of 50, when associated with environmental, psychosocial and cultural factors77. Sutton-Tyrrell K, Zhao X, Santoro N, Lasley B, Sowers M, Johnston J, Mackey R, Matthews K: Reproductive hormones and obesity: 9 years of observation from the study of women’s health across the nation. Am J Epidemiol 2010; 171(11):1203-1213.. Recent information has associated mortality risks to the age at onset of menopause. Women who enter menopause earlier have a higher mortality rate, especially from cardiovascular causes88. Wu X, Cai H, Kallianpur A, Gao YT, Yang G, Chow WH, Li HL, Zheng W, Shu XO. Age at menarche and natural menopause and number of reproductive years in association with mortality: results from a median followup of 11.2 years among 31,955 naturally menopausal Chinese women. PLoS One 2014; 9(8):e103673.,99. Mondul AM, Rodriguez C, Jacobs EJ, Calle EE. Age at natural menopause and cause-specific mortality. Am J Epidemiol 2005; 162(11):1089-1097..
This being the case, although data on morbidity is scarce, data on mortality of women during menopause justifies research to provide subsidies to promote health and disease prevention1010. Theodoro H, Rodrigues AD, Mendes KG, Liane RH, Paniz VM, Olinto MT. Reproductive characteristics and obesity in middle-aged women seen at an outpatient clinic in southern Brazil. Menopause 2012; 19(9):1022-1028.. Given the importance of this theme and its impact on women’s health, the goal of this study was to look for an association between overweight and obesity and sociodemographic, behavioral and clinical factors in menopausal women.
Methods
This is a descriptive, cross-sectional study of menopausal women aged 40 to 60, all of them participants in an annual health education event about breast cancer held between August and October 2013 at a Family Health Strategy Unit (ESF) in Montes Claros, Minas Gerais, Brazil.
This choice is the result of access, as the city lacks a specific location to provide services to menopausal women. Women aged 40 to 60 for whom anthropometric measurements could be made were considered eligible. Pregnant women, those with psychiatric diseases, or who were unable to answer the questionnaire or unavailable for the interview for any reason (e.g. no time, disease, illiteracy, explicit refusal) were excluded. The authors trained all of the interviewers ahead of time and oversaw data collection. Nutritional status, assessed via BMI, was considered the outcome variable of the study. Nutritional status was classified as underweight (BMI < 18.5); eutrophic (BMI = 18.5 - 24.9), overweight (BMI = 25 - 29.9) and obese (BMI ≥ 30) kg/m21111. Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica (ABESO). Diretrizes Brasileiras de Obesidade (2009/2010). Itapevi; 2009. [citado 2013 jul 25]. Disponível em: http://www.abeso.org.br/pdf/diretrizes_brasileiras_obesidade_2009_2010_1.pdf .
http://www.abeso.org.br/pdf/diretrizes_b...
. BMI was calculated based on measured height and weight. To assess body weight, women were weighed in light garments without their shoes, standing erect with both feet together and their arms relaxed alongside their bodies. A portable Geratherm® Body Fat Scale was used, with capacity for up to 150 kg, minimum and accurate to 50 g.
Height was measured using a Carci® inelastic 0 to 150 cm tape measure set against a flat wall with no baseboard. Women were told to stand up straight with their feet together and looking straight ahead, without stretching or bending their neck. Weight and height were measured in duplicate and averaged to calculate BMI.
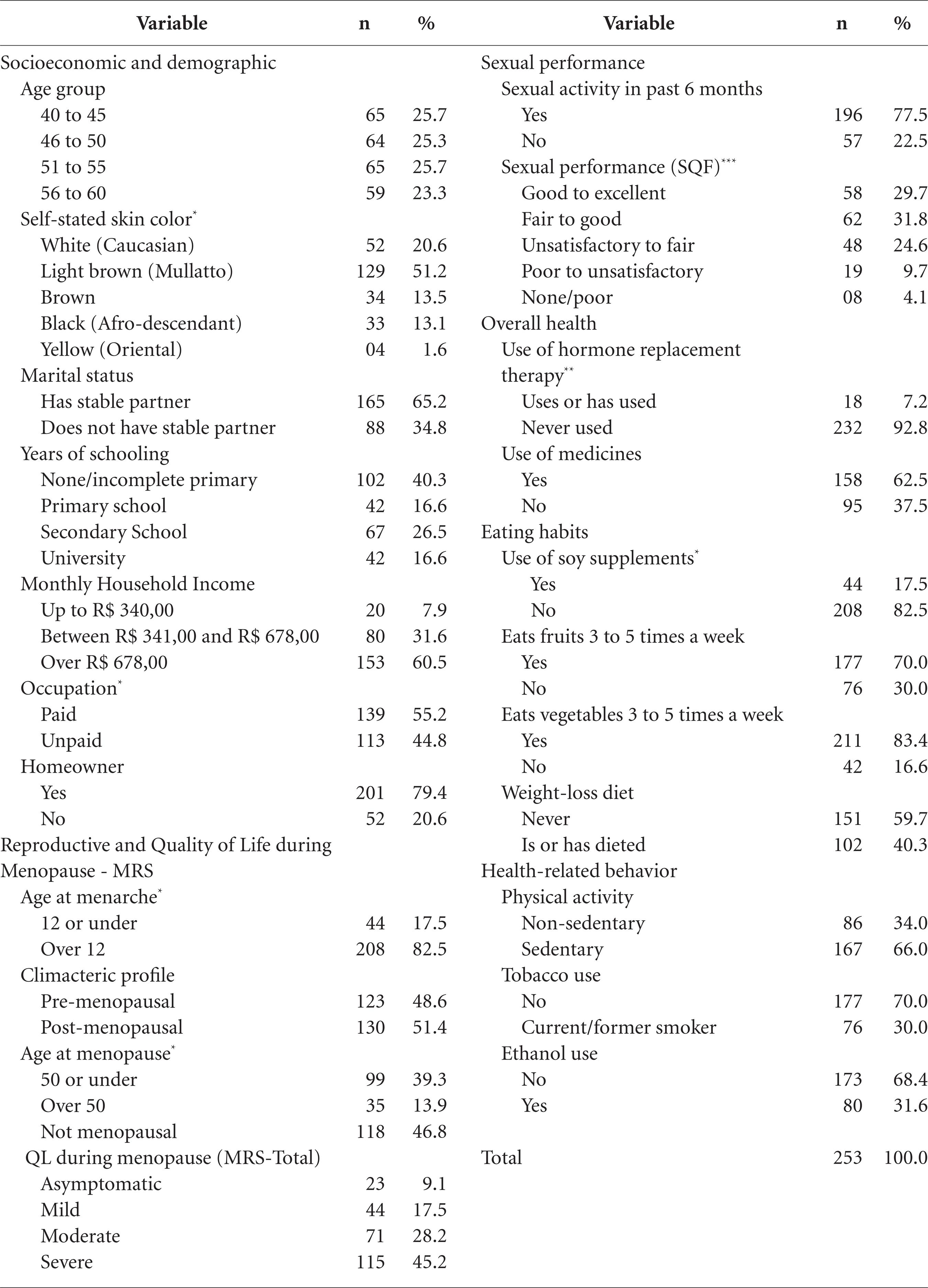
Women were interviewed and answered questions regarding six groups of independent variables: (1) socioeconomic and demographic, (2) reproductive and quality of life-MRS, (3) sexual performance, (4) overall health, (5) eating habits, and (6) health-related behavior.
Socioeconomic and demographic data included age ((40-45, 46-50, 51-55, 56-60), stated color of skin (white or non-white), marital status (stable partner, no stable partner), years of schooling (none/incomplete primary, primary, high-school, university), monthly household income (R$ 340,00 or less, R$ 341 to R$ 678,00, over R$ 678,00), occupation (paid/not paid), and home-owner (yes or no).
The reproductive variables included age at menarche (12 or less, over 12), age when entering menopause (50 or under, over 50, not yet menopausal), and the climacteric profile (pre or post menopause). Pre-menopause if regular menstrual cycles were present, and post-menopausal if the woman’s menstrual periods had been absent for a period equal to or longer than 12 consecutive months. Menopausal status was defined based on the woman’s menstrual history in the past year. Quality of life was analyzed using the Menopause Rating Scale (MRS) validated in Portuguese. This is an 11-question questionnaire dealing with symptoms, split into somato-vegetative, psychological and urogenital. This tool allowed each woman to state her opinion regarding each symptom - absent, mild, moderate, severe and very severe1212. Heinemann K, Ruebig A, Potthoff P, Schneider HP, Strelow F, Heinemann LA, Thai DM. The Menopause Rating Scale (MRS) scale: a methodological review. Health Qual Life Outcomes 2004; 2:45..
Sexual performance was assessed using the Sexual Quotient questionnaire (SQ-F) - Female Version, made up of 10 questions to be answered using a scale of 0 to 5. This tool enables analyzing the various domains of female sexual activity - desire, excitation, orgasm and their related psychophysical factors. A higher the score on SQ-F questions (except for the question regarding pain) indicates better or more satisfying sexual performance1313. Abdo CHN. Quociente sexual feminino: um questionário brasileiro para avaliar a atividade sexual da mulher. Diagn Tratamento 2009; 14(2):89-91..
The general health group of questions was made up of the following variables: present or past use of dichotomized hormone replacement therapy, and the use of other medicines split into continued use nor not. To analyze eating habits, we used as variables the use of soy supplements, eating fruits, vegetables and legumes and dieting.
Use of soy supplements was dichotomized into yes and no. In order to learn about whether the women ate fruits, vegetables and legumes, we asked two questions: how many times a day and how many times a week. The variables were dichotomized into eats fruits 3 to 5 times a week, eats fruits and legumes 3 to 5 times a week due to the small number of women who reported eating the recommended amounts in the Nutritional Guidebook for the Brazilian Population1414. Brasil. Ministério da Saúde (MS). Secretaria de Atenção à Saúde. Guia alimentar para a população brasileira: promovendo a alimentação saudável. Brasília: MS; 2008. (Série A. Normas e Manuais Técnicos).. Women were asked if they were on a weight-loss diet at the time, or had been in the past, or if they had never been on a diet.
The health-related behavior group of questions was comprised of the variable exercise (physical activity), assessed using the criteria established by the Brazilian Cardiology Society1515. Sociedade Brasileira de Cardiologia. Departamento de Aterosclerose da Sociedade Brasileira de Cardiologia. IV Diretriz Brasileira Sobre Dislipidemias e Prevenção da Aterosclerose. Arq Bras Cardiol 2007; 88(Supl. 1):2-19.. Women with no regular physical activity – defined as at least 30 minutes 3 times a week, regardless of the type of exercise – were considered sedentary1515. Sociedade Brasileira de Cardiologia. Departamento de Aterosclerose da Sociedade Brasileira de Cardiologia. IV Diretriz Brasileira Sobre Dislipidemias e Prevenção da Aterosclerose. Arq Bras Cardiol 2007; 88(Supl. 1):2-19..
Initially we performed descriptive analyses of all of the survey variables using frequency distributions. We then ran bivariate analyses between the outcome variable and each independent variable, using a Poisson regression model with robust variance. We estimated gross Prevalence Ratios (PR) and their respective 95% confidence intervals. The variables with a descriptive level (p-value) of less than 0.25 were selected for multiple analysis using a hierarchical Poisson regression model. Here we used the model in Figure 1, with blocks of distal (socioeconomic and demographic), intermediate (reproductive and MRS quality of life and sexual performance) and proximal (overall health, eating habits and health-related behavior) variables1616. Lins APM, Sichieri R, Coutinho WF, Ramos EG, Peixoto MVM, Fonseca VM. Alimentação saudável, escolaridade e excesso de peso entre mulheres de baixa renda. Cien Saude Colet 2013; 18(2):357-366..
The stepwise forward procedure was used for each hierarchical level, starting with the variable with the largest statistical significance selected from the bivariate analysis, and then adding the other variables one by one by decreasing order of descriptive level.
Demographic and socioeconomic characteristics was the first block to be added to the model, remaining as an adjustment factor for intermediate and proximal determinants only when those variables had a descriptive level of p<0.05. We then added intermediate variables (reproductive, quality of life-MRS and sexual performance). Only variables with p<0.05 were kept in the model after adjusting for the distal level variables. We included the proximal variables (overall health, eating habits and health-related behavior) last. Again, only variables with p<0.05 were kept in the model after adjusting for the distal level variables.
We estimated gross Prevalence Ratios (PR) and their respective 95% confidence intervals. The Deviance test was used to assess the quality of the adjustment of the multiple model. Analyses were performed using PASW® 17.0.
This study complies with Resolution 466/2012. This study was approved by the Research Ethics Committee (REC) of Universidade Estadual de Montes Claros.
Women waiting to schedule mammograms were individually approached and invited to participate in the study. After explaining the study goals, responsibilities and procedures, those wishing to participate signed a Free and Informed Consent Form (FICF).
Results
The sample was made up of women with an average age of 50.2 (SD ± 5.8 years), 86 of them (34%) classified as eutrophic, 78 (30.8%) as overweight and 89 (35.2%) as obese. A total of 167 women (66% of the sample) were overweight or obese. The average BMI was 28.1 kg⁄m2 (SD ± 5.6). Other characteristics of the study group are listed in Table 1.
Tables 2 and 3 show the results of the bivariate analyses. This study found a 0.25% association between the following variables and the outcome of overweight or obese: years of schooling (p = 0.120), occupation (p = 0.129), home-owner (p = 0.011), age at menarche (p = 0.012), QoL during menopause (p = 0.002), use of medicines (p = 0.002), use of soy supplements (p = 0.207), eating fruits (0.247) and dieting (0.000). These variables were selected for the final multiple analysis.
The results of factors associated with being overweight or obese from the hierarchical multiple regression analysis are shown in Table 4. In the more distal determination block, the variable “owns home” was associated with being overweight. The prevalence of overweight/obesity was higher among women claiming not own the home they live in (PR = 1.26)
In the intermediate block, Quality of Life during Menopause (MRS) was associated with being overweight or obese, regardless of demographic and socioeconomic characteristics. The prevalence of overweight and obesity was higher among women with mild (PR = 2.02), moderate (PR = 2.03) and severe (PR = 2.53) symptoms compared to women with no symptoms. Among the proximal variables, we found that women using medicines (PR = 1.26) and those who are dieting or have dieted (PR = 1.49) showed a higher incidence of overweight/obesity after adjusting for the variables in the hierarchically superior blocks.
Discussion
The frequency of overweight and obesity among the study population was 66%, with an average BMI of 28.1 kg/m2 (SD = 5.6), which is close to the number reported by other authors1010. Theodoro H, Rodrigues AD, Mendes KG, Liane RH, Paniz VM, Olinto MT. Reproductive characteristics and obesity in middle-aged women seen at an outpatient clinic in southern Brazil. Menopause 2012; 19(9):1022-1028.,1717. Gallon CW, Wender MCO. Estado nutricional e qualidade de vida da mulher climatérica. Rev Bras Ginecol Obstet 2012; 34(4):175-183.,1818. Martinazzo J, Zemolin GP, Spinelli RB, Zanardo VPS, Ceni GC. Avaliação nutricional de mulheres no climatério atendidas em ambulatório de nutrição no norte do Rio Grande do Sul, Brasil. Cien Saude Colet 2013; 18(11):3349-3356.. In the city of Passo Fundo, RS a study of 298 menopausal women showed that 68.4% of them were overweight, with an average BMI of 28.3 kg/m2 (SD = 7.0)1919. Colpani V, Spritzer PM, Lodi AP, Dorigo GG, Miranda IAS, Hahn LB, Palludo LP, Pietroski RL, Oppermann K. Atividade física de mulheres no climatério: comparação entre auto-relato e pedômetro. Rev Saude Publica 2014; 48(2):258-265.. This is close to the 64% prevalence found in a group of 611 women in Caxias do Sul, with an average BMI of 27.4 kg/m22020. De Lorenzi DRS, Basso E, Fagundes PO, Saciloto B. Prevalência de sobrepeso e obesidade no climatério. Rev Bras Ginecol Obstet 2005; 27(8):479-484.. A survey of Brazilian women showed that 64.9% had some degree of excess weight, confirming the magnitude of this problem among the female population11. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de orçamentos familiares 2008-2009. Antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. Rio de Janeiro; 2010. [citado 2011 jun 4]. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009_encaa/pof_20082009_encaa.pdf
http://www.ibge.gov.br/home/estatistica/...
.
Data from Brazil (2011) shows a growing prevalence of excess weight among women, with the highest prevalence in women 45 to 54 and 55 to 64 years of age, or 55.9% and 60.9% respectively2121. Brasil. Ministério da Saúde (MS). Secretaria de Vigilância em Saúde. Vigitel Brasil 2011: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: MS; 2012.. Similar results show that obesity among women has also increased11. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de orçamentos familiares 2008-2009. Antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. Rio de Janeiro; 2010. [citado 2011 jun 4]. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009_encaa/pof_20082009_encaa.pdf
http://www.ibge.gov.br/home/estatistica/...
,2020. De Lorenzi DRS, Basso E, Fagundes PO, Saciloto B. Prevalência de sobrepeso e obesidade no climatério. Rev Bras Ginecol Obstet 2005; 27(8):479-484.,2222. Giolo De Carvalho F, de Souza Santos R, Iannetta R, Marques Miguel Suen V, Marliere Navarro A, Nonino Borges CB, Marchini JS, Iannetta O. Analysis of bone microarchitecture related to anthropometry in climateric women. Nutr Hosp 2012; 27(2):612-616.. According to the literature, in middle-aged women, overweight and obesity are relevant risk factors for the development of chronic diseases such as metabolic syndrome23.
Given this scenario, we find that aging may have be a strong influencer for developing obesity due to the decrease in hormone levels that brings with it a decrease in the amount of energy spent. By associating this change with external factors such as inappropriate eating habits and a sedentary lifestyle, middle-age women may experience an average 2 kg/year weight increase during the course of three years2424. Polotsky HN, Polotsky AJ. Metabolic implications of menopause. Sem rep med 2010; 28(5):426-434..
We reiterate the importance of these findings, as they make this population a target for public health programs seeking to prevent obesity and its associated comorbidities. The city of Montes Claros is located on the border between the Southeast and Northeast regions of Brazil. From an economic and social point of view, it is closer to the Northeast than the Southeast, being located in the semi-arid region of the state of Minas Gerais, a poor region with low rainfall and consequently limited water resources. The recent increase in the purchasing power of lower income households has influenced an imbalance between calories ingested and calories burned, resulting in excess weight. An explanation for this may be related to the recent trend to replacing traditional foods in the Brazilian diet (such as rice, beans and vegetables) with processed foods and beverages, with a higher energy density and eating patterns that can compromise the energy balance and increase the risk of obesity in this population.
According to the results of the multiple analysis, not owning a home, severe symptoms according to the MRS, continued use medicines and past dieting are associated with being overweight or obese. On the other hand, a study of 456 menopausal women in Paraná found different results, showing that the main factors related to obesity are having three or more children and not using hormone replacement therapy2525. Gravena AAF, Brischiliari SCR, Lopes TCR, Agnolo CMD, Carvalho MDB, Pelloso SM. Excess weight and abdominal obesity in postmenopausal Brazilian women: a population based study. BMC womens health 2013; 13(46):3-7..
This study found that women who do not own their own home are twice as likely to be overweight or obese than those who do. This variable may be understood as an economic indicator, and refers to a higher prevalence of excess weight and obesity, as does a study of 440 women that found that lower income was associated with excess weight2626. Rosa MI, Silva FML, Giroldi SB, Antunes GN, Wendland EM. Prevalência e fatores associados à obesidade em mulheres usuárias de serviços de pronto-atendimento do Sistema Único de Saúde no sul do Brasil. Cien Saude Colet 2011; 16(5):2559-2566.. One may infer that lower household income makes it harder to purchase a home, and may be associated with decrease knowledge of which foods are healthier and associated with balanced body weight. A survey of 758 women showed that 73.6% ate a healthy diet, a habit that increases with income1616. Lins APM, Sichieri R, Coutinho WF, Ramos EG, Peixoto MVM, Fonseca VM. Alimentação saudável, escolaridade e excesso de peso entre mulheres de baixa renda. Cien Saude Colet 2013; 18(2):357-366.. However, this matter must be further explored in new studies, as other authors did not make this same observation1717. Gallon CW, Wender MCO. Estado nutricional e qualidade de vida da mulher climatérica. Rev Bras Ginecol Obstet 2012; 34(4):175-183..
Another economic indicator the authors found to be associated with excess weight are few years of schooling1010. Theodoro H, Rodrigues AD, Mendes KG, Liane RH, Paniz VM, Olinto MT. Reproductive characteristics and obesity in middle-aged women seen at an outpatient clinic in southern Brazil. Menopause 2012; 19(9):1022-1028.,2626. Rosa MI, Silva FML, Giroldi SB, Antunes GN, Wendland EM. Prevalência e fatores associados à obesidade em mulheres usuárias de serviços de pronto-atendimento do Sistema Único de Saúde no sul do Brasil. Cien Saude Colet 2011; 16(5):2559-2566.. Although referred to in the literature, this study did not find such association.
The chance of being overweight was found to be eight times higher among women with severe menopausal symptoms according to the MRS, than among those with no symptoms. A survey of menopausal women found that higher BMIs were associated with poorer scores on the MRS quality of life scale1717. Gallon CW, Wender MCO. Estado nutricional e qualidade de vida da mulher climatérica. Rev Bras Ginecol Obstet 2012; 34(4):175-183.. A study of 490 women in Saudi Arabia found a strong correlation between obesity and severe menopausal symptoms2727. AlQuaiz AM, Tayel SA, Habiba FA. Assessment of symptoms of menopause and their severity among Saudi women in Riyadh. Ann Saudi Med 2013; 33(1):63-67.. A study in Scotland found a relationship between vasomotor symptoms such as heat waves and obesity2828. Duffy OK, Iversen L, Hannaford PC. Factors associated with reporting classic menopausal symptoms differ. Climacteric 2013; 16(2):240-251.. On the other hand, a study of 305 women showed no correlation between BMI and the symptoms assessed by the MRS2929. Tan MN, Kartal M, Guldal D. The effect of physical activity and body mass index on menopausal symptoms in Turkish women: a cross-sectional study in primary care. BMC Womens Health 2014; 14(38):1-9..
Regarding overall health, another factor related to excess weight was the use of medicine. Women making continuous use of medicines were two and a half as likely to be obese than those who did not. A study conducted by the Ribeirão Preto menopause outpatient clinic showed high BMIs, with 62% of the women taking three or more medicines per day3030. Santos RDS, Furtado EC, Carvalho FGD, Iannetta R, Nonino CB, Marchini JS, Ribas Filho OID, Suen VMM. Climaterium, food intake and medicines. International Journal of Nutrology 2012; 5(3):134-138.. The average BMI found in a study of 200 menopausal women revealed obesity, with almost half (48.5%) claiming they use medicine for cardiovascular diseases and 23% use andi-depressants1717. Gallon CW, Wender MCO. Estado nutricional e qualidade de vida da mulher climatérica. Rev Bras Ginecol Obstet 2012; 34(4):175-183.. One explanation for this positive association is a higher prevalence of morbidities in women of a more advanced age, among them those associated with obesity such as high blood pressure, metabolic syndrome, bone and muscle diseases and depression. Furthermore, medicines symbolize a desire to change the “natural course” of most diseases, and go beyond a specific therapy, becoming a cultural characteristic.
Regarding eating habits, women who had already dieted to lose weight, or who were dieting while the study was underway, had a higher prevalence of excess weight and obesity than women who had never dieted. In this study, 40.3% of the women reported that they were or had dieted to lose weight. An analysis of the medical records of menopausal women showed that 66.7% of the participants had gone on some sort of diet and that the average MI of these women was 30.7% kg/m2, indicating they were obese1818. Martinazzo J, Zemolin GP, Spinelli RB, Zanardo VPS, Ceni GC. Avaliação nutricional de mulheres no climatério atendidas em ambulatório de nutrição no norte do Rio Grande do Sul, Brasil. Cien Saude Colet 2013; 18(11):3349-3356..
Correlating the presence of overweight or obesity and sexual performance, we found no statistical significance, as did another study3131. Kadioglu P, Yetkin DO, Sanli O, Yalin AS, Onem K, Kadioglu A. Obesity might not be a risk factor for female sexual dysfunction. BJUI 2010; 106(9):1357-1361.. On the other hand, other surveys show an association between these factors, relating this association primarily to self-perceived physical attraction3232. Castro MJA, Márquez-Veja J, Arteta-Acosta C. Disfunción sexual en mujeres climatéricas afrodescendientes del Caribe Colombiano. Iatreia 2014; 27(1):31-41.,3333. Shahhosseini Z, Gardeshi ZH, Pourasgha M, Salehi F. A review of affecting factors on sexual satisfaction in women. Mater Socio Med 2014; 26(6):378-381..
The arrival of menopause comes with ageing, and oftentimes weight-gain. Surveys show that obesity changes women’s self-esteem, creating a negative body image and compromising their sexual satisfaction3333. Shahhosseini Z, Gardeshi ZH, Pourasgha M, Salehi F. A review of affecting factors on sexual satisfaction in women. Mater Socio Med 2014; 26(6):378-381.,3434. Câmara CNS, Corrêa HVV, Silva SCB, Da Silva CSA, Silva Junior M, Brito RS. Life Cycle Comparative Analysis of Sexual Function in Women with Normal and Overweight Body Mass Index. Creative Education 2014; 5(15):1363-1376.. Furthermore, this vision may lead women to believe that they have lost their powers of seduction. Thus menopausal and especially post-menopausal women may feel incompetent and unable of good sexual performance.
Conclusion
Although this study was developed with a non-probabilistic sample, which limits the external validity of the results, some variables have been found to be associated with excess weight, such as not owning a home, which is a reflection of an unfavorable economic situation, menopausal symptoms, continuous use of medicines and past dieting.
The frequency of excess weight found in our study is in line with the results of other studies in this country, showing that measures must be taken as this morbid condition in menopausal women is not only influenced by biological factors such as hypoestrogenism, but also by psychosocial and life-style factors.
Thus, overweight and obesity associated with menopause require increased attention and a multidisciplinary approach to women’s health to prevent morbi-mortality in this population group. The results also indicate a number of important behavioral, sociodemographic and clinical factors that should be further investigated in new studies.
Acknowledgements
Interinstitucional Master in the Universidade Estadual de Montes Claros (UNIMONTES) and Faculdades Integradas Pitágoras de Montes Claros (FIPMoc).
Referências
-
1Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de orçamentos familiares 2008-2009. Antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil Rio de Janeiro; 2010. [citado 2011 jun 4]. Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009_encaa/pof_20082009_encaa.pdf
» http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009_encaa/pof_20082009_encaa.pdf -
2Linhares RS, Horta BL, Gigante DP, Dias-da-Costa JS, Olinto MTA. Distribuição de obesidade geral e abdominal em adultos de uma cidade no Sul do Brasil. Cad Saude Publica 2012; 28(3):438-447.
-
3Almeida JPM, Carnide C, Branquinho M, Geraldes F, Águas F. Impacto da terapia hormonal sobre o peso corpóreo. Rev Bras Ginecol Obstet 2011; 33(10):310-314.
-
4Sturm R, An R. Obesity and economic environments. CA Cancer J C 2014; 64(5):337-350.
-
5Tannure MC, Alves M, Sena RR, Chianca TCM. Perfil epidemiológico da população idosa de Belo Horizonte, MG, Brasil. Rev. bras. enferm 2010; 63(5):817-822.
-
6Mundial de la Salud (OMS). Investigaciones sobre la menopausa en los anos noventa: informe de un grupo cientifico de la OMS Ginebra: OMS; 1996. (OMS, Serie de informes técnicos, nº 866).
-
7Sutton-Tyrrell K, Zhao X, Santoro N, Lasley B, Sowers M, Johnston J, Mackey R, Matthews K: Reproductive hormones and obesity: 9 years of observation from the study of women’s health across the nation. Am J Epidemiol 2010; 171(11):1203-1213.
-
8Wu X, Cai H, Kallianpur A, Gao YT, Yang G, Chow WH, Li HL, Zheng W, Shu XO. Age at menarche and natural menopause and number of reproductive years in association with mortality: results from a median followup of 11.2 years among 31,955 naturally menopausal Chinese women. PLoS One 2014; 9(8):e103673.
-
9Mondul AM, Rodriguez C, Jacobs EJ, Calle EE. Age at natural menopause and cause-specific mortality. Am J Epidemiol 2005; 162(11):1089-1097.
-
10Theodoro H, Rodrigues AD, Mendes KG, Liane RH, Paniz VM, Olinto MT. Reproductive characteristics and obesity in middle-aged women seen at an outpatient clinic in southern Brazil. Menopause 2012; 19(9):1022-1028.
-
11Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica (ABESO). Diretrizes Brasileiras de Obesidade (2009/2010). Itapevi; 2009. [citado 2013 jul 25]. Disponível em: http://www.abeso.org.br/pdf/diretrizes_brasileiras_obesidade_2009_2010_1.pdf .
» http://www.abeso.org.br/pdf/diretrizes_brasileiras_obesidade_2009_2010_1.pdf -
12Heinemann K, Ruebig A, Potthoff P, Schneider HP, Strelow F, Heinemann LA, Thai DM. The Menopause Rating Scale (MRS) scale: a methodological review. Health Qual Life Outcomes 2004; 2:45.
-
13Abdo CHN. Quociente sexual feminino: um questionário brasileiro para avaliar a atividade sexual da mulher. Diagn Tratamento 2009; 14(2):89-91.
-
14Brasil. Ministério da Saúde (MS). Secretaria de Atenção à Saúde. Guia alimentar para a população brasileira: promovendo a alimentação saudável. Brasília: MS; 2008. (Série A. Normas e Manuais Técnicos).
-
15Sociedade Brasileira de Cardiologia. Departamento de Aterosclerose da Sociedade Brasileira de Cardiologia. IV Diretriz Brasileira Sobre Dislipidemias e Prevenção da Aterosclerose. Arq Bras Cardiol 2007; 88(Supl. 1):2-19.
-
16Lins APM, Sichieri R, Coutinho WF, Ramos EG, Peixoto MVM, Fonseca VM. Alimentação saudável, escolaridade e excesso de peso entre mulheres de baixa renda. Cien Saude Colet 2013; 18(2):357-366.
-
17Gallon CW, Wender MCO. Estado nutricional e qualidade de vida da mulher climatérica. Rev Bras Ginecol Obstet 2012; 34(4):175-183.
-
18Martinazzo J, Zemolin GP, Spinelli RB, Zanardo VPS, Ceni GC. Avaliação nutricional de mulheres no climatério atendidas em ambulatório de nutrição no norte do Rio Grande do Sul, Brasil. Cien Saude Colet 2013; 18(11):3349-3356.
-
19Colpani V, Spritzer PM, Lodi AP, Dorigo GG, Miranda IAS, Hahn LB, Palludo LP, Pietroski RL, Oppermann K. Atividade física de mulheres no climatério: comparação entre auto-relato e pedômetro. Rev Saude Publica 2014; 48(2):258-265.
-
20De Lorenzi DRS, Basso E, Fagundes PO, Saciloto B. Prevalência de sobrepeso e obesidade no climatério. Rev Bras Ginecol Obstet 2005; 27(8):479-484.
-
21Brasil. Ministério da Saúde (MS). Secretaria de Vigilância em Saúde. Vigitel Brasil 2011: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico Brasília: MS; 2012.
-
22Giolo De Carvalho F, de Souza Santos R, Iannetta R, Marques Miguel Suen V, Marliere Navarro A, Nonino Borges CB, Marchini JS, Iannetta O. Analysis of bone microarchitecture related to anthropometry in climateric women. Nutr Hosp 2012; 27(2):612-616.
-
23Maharlouei N, Bellissimo N, Ahmadi SM, Lankarani KB. Prevalence of metabolic syndrome in pre-and postmenopausal iranian women. Diabetes 2013; 16(5):561-567.
-
24Polotsky HN, Polotsky AJ. Metabolic implications of menopause. Sem rep med 2010; 28(5):426-434.
-
25Gravena AAF, Brischiliari SCR, Lopes TCR, Agnolo CMD, Carvalho MDB, Pelloso SM. Excess weight and abdominal obesity in postmenopausal Brazilian women: a population based study. BMC womens health 2013; 13(46):3-7.
-
26Rosa MI, Silva FML, Giroldi SB, Antunes GN, Wendland EM. Prevalência e fatores associados à obesidade em mulheres usuárias de serviços de pronto-atendimento do Sistema Único de Saúde no sul do Brasil. Cien Saude Colet 2011; 16(5):2559-2566.
-
27AlQuaiz AM, Tayel SA, Habiba FA. Assessment of symptoms of menopause and their severity among Saudi women in Riyadh. Ann Saudi Med 2013; 33(1):63-67.
-
28Duffy OK, Iversen L, Hannaford PC. Factors associated with reporting classic menopausal symptoms differ. Climacteric 2013; 16(2):240-251.
-
29Tan MN, Kartal M, Guldal D. The effect of physical activity and body mass index on menopausal symptoms in Turkish women: a cross-sectional study in primary care. BMC Womens Health 2014; 14(38):1-9.
-
30Santos RDS, Furtado EC, Carvalho FGD, Iannetta R, Nonino CB, Marchini JS, Ribas Filho OID, Suen VMM. Climaterium, food intake and medicines. International Journal of Nutrology 2012; 5(3):134-138.
-
31Kadioglu P, Yetkin DO, Sanli O, Yalin AS, Onem K, Kadioglu A. Obesity might not be a risk factor for female sexual dysfunction. BJUI 2010; 106(9):1357-1361.
-
32Castro MJA, Márquez-Veja J, Arteta-Acosta C. Disfunción sexual en mujeres climatéricas afrodescendientes del Caribe Colombiano. Iatreia 2014; 27(1):31-41.
-
33Shahhosseini Z, Gardeshi ZH, Pourasgha M, Salehi F. A review of affecting factors on sexual satisfaction in women. Mater Socio Med 2014; 26(6):378-381.
-
34Câmara CNS, Corrêa HVV, Silva SCB, Da Silva CSA, Silva Junior M, Brito RS. Life Cycle Comparative Analysis of Sexual Function in Women with Normal and Overweight Body Mass Index. Creative Education 2014; 5(15):1363-1376.
Publication Dates
-
Publication in this collection
Apr 2016
History
-
Received
24 Mar 2015 -
Reviewed
23 Oct 2015 -
Accepted
25 Oct 2015

 Source: Lins et al.13.
Source: Lins et al.13.