Abstract
Metabolic complications continue to play a major role in the management of HIV infection. Dyslipidemia associated with HIV infection and with the use of combined antiretroviral therapy includes elevations in triglycerides, reduced high-density cholesterol, and variable increases in low-density and total cholesterol. The association between dyslipidemia and specific antiretroviral agents has been underscored. Multiple pathogenic mechanisms by which HIV and antiretroviral agents lead to dyslipidemia have been hypothesized, but they are still controversial. The potential clinical and pathological consequences of HIV-associated hyperlipidemia are not completely known, but several studies reported an increased risk of coronary artery disease in HIV-positive individuals receiving combined antiretroviral therapy. HIV-infected persons who have hyperlipidemia should be managed similarly to those without HIV infection in accordance with the National Cholesterol Education Program. Life style changes are the primary target. Statins and fibrates and/or modification in antiretroviral therapy are possible approaches to this problem.
HIV/AIDS; dyslipidemia; combined antiretroviral therapy; nutrition; Public Health
ORIGINAL ARTICLE
Dyslipidemia in HIV-infected individuals
Eduardo SprinzI; Rosmeri Kuhmmer LazzarettiII; Regina KuhmmerIII; Jorge Pinto RibeiroIV
IInternal Medicine Division, Hospital de Clínicas de Porto Alegre
IIDepartment of Medicine, School of Medicine, Universidade Federal do Rio Grande do Sul; Porto Alegre, RS, Brazil
IIIDepartment of Medicine, School of Medicine, Universidade Federal do Rio Grande do Sul; Porto Alegre, RS, Brazil
IVDepartment of Medicine, School of Medicine, Universidade Federal do Rio Grande do Sul; Porto Alegre, RS, Brazil
Correspondence to Correspondence to: Eduardo Sprinz, MD, PhD Serviço de Infectologia Hospital de Clínicas de Porto Alegre Rua Ramiro Barcellos, 2350/700 90035-003, Porto Alegre, RS, Brazil Phone: +55 51 21018152; +55 51 33302961; +55 51 99573333 Fax: +55 51 33309700 E-mail: esprinz@hcpa.ufrgs.br; eduardo.sprinz@hotmail.com
ABSTRACT
Metabolic complications continue to play a major role in the management of HIV infection. Dyslipidemia associated with HIV infection and with the use of combined antiretroviral therapy includes elevations in triglycerides, reduced high-density cholesterol, and variable increases in low-density and total cholesterol. The association between dyslipidemia and specific antiretroviral agents has been underscored. Multiple pathogenic mechanisms by which HIV and antiretroviral agents lead to dyslipidemia have been hypothesized, but they are still controversial. The potential clinical and pathological consequences of HIV-associated hyperlipidemia are not completely known, but several studies reported an increased risk of coronary artery disease in HIV-positive individuals receiving combined antiretroviral therapy. HIV-infected persons who have hyperlipidemia should be managed similarly to those without HIV infection in accordance with the National Cholesterol Education Program. Life style changes are the primary target. Statins and fibrates and/or modification in antiretroviral therapy are possible approaches to this problem.
Keywords: HIV/AIDS; dyslipidemia; combined antiretroviral therapy; nutrition, Public Health.
INTRODUCTION
Combined antiretroviral therapy (cART) significantly modified the prognosis of individuals infected by the Human Immunodeficiency Virus-1 (HIV), with marked improvement in morbidity and mortality rates worldwide.1-4 Nevertheless, several clinical aspects have been developed along with the longer longevity of HIV individuals, most of them related to other chronic conditions or to the antiretroviral treatment (ART).5,6 Metabolic abnormalities such as insulin resistance and disturbances in glucose homeostasis, modified adiposity physiology with lipids alterations might result in clinical complications including glucose intolerance or diabetes mellitus; altered body fat distribution, with lipoatrophy (loss of subcutaneous fat mostly in the face and periphery) or/and lipohypertrophy (localized fat gain most often central and visceral adiposity).7,8
Some of these perturbations can be associated with ART. Protease inhibitors (PI) show direct effect on human adipose and specific effects on insulin resistance which may contribute to the overall adipose imbalance and development of lipodystrophy, and metabolic syndrome in HIV-positive individuals.7-9 In addition, nucleoside reverse transcriptase inhibitors (NRTIs) may induce mitochondrial dysfunction, which could result in effects on adipose tissue, lactic acidosis, myopathy, peripheral neuropathy, hepatic steatosis and pancreatitis as well.8,10,11 Although less involved, nonnucleoside reverse transcriptase inhibitors (NNRTIs), mainly efavirenz, might be associated with metabolic disorders, including dyslipidemia.7, 12
Those changes in metabolism and mitochondrial toxicity could eventually be associated with a greater chance of cardiovascular events and death.13-15 Although some association has already been elucidated, the relationship between antiretroviral drugs, metabolic syndrome, dyslipidemia, and cardiovascular events is still far from being fully clarified. The purpose of this review is to discuss the development of dyslipidemia and lypodistrophy, its relation to cardiovascular events, and its best management in individuals with HIV infection.
Overall body changes & lipodystrophy syndrome in HIV infection
These alterations taken together, named "lipodystrophy syndrome associated with HIV", were first described in 1998 and included dyslipidemia, lipoatrophy, accumulation of centripetal intra-abdominal fat, and metabolic syndrome.7 The prevalence of the syndrome varies from 11% to 83% in the different studies already conducted.16,17
Body changes are associated both with accumulation (lipohypertrophy) and/or with loss (lipoatrophy) in body fat. In the case of lipohypertrophy, it is possible to find increased abdominal circumference (omental, retroperitoneal, and mesenteric), increased breast size, and accumulation of fat in dorsocervical region (buffalo hump).7,15
On the other hand, lipoatrophy, which is more related to nucleoside reverse transcriptase inhibitors (mainly thymidinic analogues, zidovudine - ZDV and stavudine - d4T), includes loss of subcutaneous fat in the gluteal region, arms and legs, along with vascular prominence in upper and lower limbs, decreased temporal and periorbital fat pad, and the appearance of nasolabial double fold.18,19
These body habitus modifications are usually associated with alterations in plasma lipids and presence of metabolic syndrome. There may be an increase in total cholesterol and low-density lipoprotein (LDL-c) fraction, and triglycerides, which are clearly associated with pro-atherogenic profile.20,21
Pathophysiology of dyslipidemia with and without cART
Lipids alterations, with increased triglycerides, due in part to decreased clearance of very low-density lipoprotein (VLDL-c) and the reduction of high-density lipoprotein (HDL-c) in circulation, were reported even before the use of antiretroviral drugs.22 Direct lipid changes related to HIV disease and/or inflammatory factors could partially explain these alterations, which could be exemplified by the fact that low CD4+ T-cell count might be considered a major atherosclerosis risk factor in HIV-infected individuals.22,23
Generally speaking, PIs are associated with dyslipidemia, which is highest with ritonavir and boosted .9,14,24 Several theories have been proposed to explain the contribution of PIs in dyslipidemia, although none of them explains all aspects. Carr et al. 7 proposed a theory based on the finding of molecular structural homology between the catalytic site of HIV protease and two human proteins involved in lipid metabolism, the protein binding of retinoic acid cytoplasmic type I (CRABP-1 -Cellular Retinoic Acid Binding Protein 1) and protein related to the receptor for low-density lipoprotein (LDL-R). Therefore, most PIs would inhibit steps of lipid metabolism, probably depending on the gene expression of the involved receptor. PI connected to CRABP-1 would decrease the activation of the receptor of 9-cis retinoic acid and dimerization with the receptor activated by the peroxisome proliferator γ (PPARγ - Peroxisome Proliferator Activated Receptor-gamma), which has a key role in the differentiation of adipocytes and apoptosis of these cells, and further improves the peripheral sensitivity to insulin. Such changes would lead to the release of lipids into the circulation and hyperlipidemia.
Another proposed mechanism is the inhibition of the activity of the plasmatic lipoproteic lipase by PI, which binds to the LDL-R. The difficulty in capturing the chylomicron and the hepatic clearance of triglycerides by complex endothelial lipoprotein lipase-LRP, in turn, would mean a lower uptake by the liver and triglycerides by cleavage of the fatty acids in glycerol. However, this hypothesis has yet to be confirmed.25
In the same way factors that could increase the activity of the protein link to the sterol regulatory element 1 (SREBP-1 -Sterol Regulatory Element Binding Protein 1) might lead to increased lipogenesis and increased production of VLDL-c. Experiments done in animals with ritonavir showed marked increase of VLDL-c in the presence of a diet rich in fat, and a significant increase in the levels of liver apoliprotein B (Apo B).26 Therefore, the increase in triglycerides caused by ritonavir could be related to the enhancement in the production of hepatic lipoprotein, by inhibiting the proteasome-mediated degradation of Apo B and SREBP-1 in the liver.27
Similarly, genetic predisposition may explain, in part, the variability between patients in relation to the effects of PIs on the metabolism of lipids. Most individuals when exposed to ritonavir may have significant increases in plasma levels of triglycerides, while in others this elevation does not occur.28,29 However, the genes involved in these phenomena are not yet known.
Generally, PIs (except atazanavir) seem to inhibit the function of GLUT-4 in the transport of glucose, which reduces the uptake of glucose mediated by insulin in skeletal muscles and in adipocytes, which can lead to changes in lipid metabolism.9,30,31
PI can also induce insulin resistance by the inhibition of translocation of SREBP-1c, directly or indirectly via PPARγ receiver.32 SREBP-1 regulates the growth and synthesis of glucose, differentiation and maturation of adipocytes and increased glucose through the adipocytes. The process of adipocyte differentiation may increase the synthesis and secretion of adiponectin, a cytokine that sensitizes insulin action.33 Since PPARγ is preferentially expressed in peripheral adipocytes, it is expected that the inhibition of protein carrier of retinoic acid by the PIs could result in apoptosis and damaged differentiation of adipocytes contributing to the development of changes in the fat distribution and insulin resistance.34
Furthermore, the class of NRTIs can also be associated with the development of dyslipidemia and insulin resistance and their consequences, as already explained. The NRTIs (mainly the thymidine analogues, d4T and ZDV) reduce the synthesis of mitochondrial DNA by inhibiting DNA polymerase gamma.35 As a result there is a depletion of mitochondrial DNA, enzyme deficiency, oxidative phosphorylation and induction of subcutaneous adipocytes apoptosis.10,11,36
Atherosclerotic disease in HIV infection and AIDS
Many studies have demonstrated an association between cART and increased risk in coronary events when compared to the general population, which may be related to dyslipidemia and to the duration of cART exposure.13,14,37,38 The largest study of cardiovascular epidemiology in HIV-infected individuals on cART is the Data Collection on Adverse Effects of Anti-Retroviral Drugs (D:A:D), a multicohort study. D:A:D has shown an increased relative risk of acute myocardial infarction of 1.26 (26% more) per year of exposure to cART in the first four to six years, and the recent use (up to 6 months) of abacavir, didanosine, lopinavir or indinavir were independently associated with increased risk.13,14,38 It is important to consider that traditional risks, such as tobacco smoking, dyslipidemia, diabetes and hypertension, were also increased in these studies. In order to estimate the 10-year cardiovascular risk in relation to the time of cART exposure, the Framingham score was evaluated in D:A:D participants.40 With the caveat that Framingham scores could under evaluate the coronary risk in HIV-infected individuals, this study showed that the chance for first cardiovascular event increased with time of exposure to ART (relative risk per year of exposure: 1.26, 95%, CI: 1.15 to 1.38).
There is only one major study that found no difference in cardiovascular disease in HIV-infected individuals on cART.39 Although controversial, this was a retrospective analysis of 36,766 HIV-infected individuals on cART, between 1993 and 2001, with respect to overall mortality, mortality for specific cardiovascular and cerebrovascular events, and rates of hospitalization. Hospital admissions for cardiovascular and brain diseases and the fatality rate decreased (1.7% to 0.9%, 21.3% to 5.0% from 1995 to 2001, respectively). However, the study sites were known to not offer good cardiovascular care, which could lead to a selection bias in the study. Also, it has been noticed that the prescription of lipid reducing agents gradually increased over the time.
In the Study of Strategies for Addressing the Anti-Retroviral Therapy (SMART), individuals were randomized to continue cART or to temporarily interrupt their treatment when the CD4 cell count was higher than 350 cells/mm3 and for restarting when it had fallen to less than 250 cells/mm3.41 This study was stopped prematurely by the high incidence of adverse outcomes including fatal and non-fatal cardiovascular events in the group with cART interruption. Given the general impression that cART is associated with increased risk of cardiovascular disease, it would be expected to see a reduction of these events. However, the relative risk of these complications was 1.5 times greater in the group of patients discontinuing cART compared to the group that remained on therapy. This reinforces the hypothesis in which HIV itself is considered an independent risk factor for cardiovascular disease.
Incidence of dyslipidemia in HIV infection and AIDS
Before cART, the main metabolic alteration was related to wasting, with protein-energy malnutrition, characterized by depletion of lean mass and fat. Unfavorable changes in lipid profile, with reduction in the levels of HDL-c and mild elevation in the levels of triglycerides, also occurred in advanced disease because of changes in inflammatory cytokines, phenomenon also found in other chronic inflammatory disorders not caused by HIV.22
Unfortunately, as already mentioned, cART can be associated with the development of dyslipidemia. The abnormalities in lipid profile generally occur after the beginning of ART, frequently between the third and sixth month, but its emergence may be early in regimens containing PIs.9,42,43 The prevalence of dyslipidemia in HIV-infected individuals on cART varies from 30% to 80% depending on drug combination and diagnostic definition criteria, and the most common include hypertriglyceridemia (40% to 80%), and hypercholesterolemia (10% to 50%).16,24,44
Changes in lifestyle and dyslipidemia in HIV infection and AIDS
Scientific evidence about the effectiveness of diet indicates that a limited energy intake from simple sugars and fats, the replacement of saturated fat and trans unsaturated fat by the increased consumption of fruits, vegetables, whole cereals, and nuts confer significant benefits for the health of general population. Epidemiological surveys have shown the synergistic effect of changes in lifestyle, such as "healthy" diet that provide a "shield" against the development of several non-transmissible chronic diseases, including cardiovascular disease, hypertension, diabetes mellitus, obesity and dyslipidemia in the non-HIV population.46,47 Although epidemiological surveys have not yet been conducted among HIV-infected induviduals, most studies support changes in lifestyle as a major goal to be addressed.48-55 Also, as expected, better results were achieved in individuals with adherence to diet modifications.
Our group assessed the impact of physical conditioning and diet on low levels of lipids in HIV-infected individuals with dyslipidemia and lipodystrophy. Although of short duration and dealing primarily with aerobic exercise and therapeutic intervention, there was no consistent changes in plasma lipids.49 Fitch et al., evaluated whether changes in lifestyle could have beneficial effect on cardiovascular risk factors in patients on HAART and manifestations of the metabolic syndrome. After six months, despite improvement in the physical condition, diet habit and abdominal circumference in the group that changed the way of life, there was no significant improvement in plasma lipids compared to the control group.50
The amount of fiber, alcohol and fat in diet may play an important role in dyslipidemia associated with HIV.50-55 Some components of diet, such as saturated, monounsaturated and polyunsaturated fat, fiber and alcohol, were directly linked to insulin resistance and hypercholesterolemia, whereas diet rich in fiber was inversely associated.51,52 Also, high amounts of alcohol were linked to high levels of LDL. These associations were independent of age, sex, distribution of body fat and time of exposure to PIs.
Barrios et al. prospectively evaluated the effectiveness of a low-fat diet in the reduction of cholesterol and triglycerides in 230 HIV-infected individuals. Those with good adherence to diet had a reduction of 11% and 10% in the levels of cholesterol and in 12% and 23% in the levels of triglycerides after 3 and 6 months, respectively. Adherence to diet was also associated with significant weight loss. The impact on the abovementioned metabolic parameters was more noticeable among individuals on PIs and after 6 months (cholesterol decreased 13% and 22% and triglycerides 15% and 49% at 6 and 6 months, respectively).54
The management of HIV-infected individuals with dyslipidemia needs to be validated, specified and individualized. Currently, the recommendations of the Adult AIDS Clinical Trials Group (ACTG), based on the NCEP, must be followed for the prevention and management of dyslipidemia associated with cART. These guidelines are primarily directed towards a healthy way of life, with physical activity and a balanced diet,24 but this approach is empiric as there is no sufficient clinical evidence to support it.
Omega 3 and dyslipidemia in the acquired immunodeficiency syndrome
It is known that omega 3 (fish oil) is associate with a reduction in cardiovascular events in general population.56 Diet supplementation with omega 3 and exercise were compared in HIV-infected patients who had triglyceride levels greater than 200 mg/dL. After 16 weeks of follow-up, there was no significant difference in the levels of triglycerides between groups. However, LDL-c levels did significantly increase in the fish oil arm, but not in the diet and exercise arm (22% versus 18%, respectively).57
Gerber et al. randomized 100 patients with hypertriglyceridemia on cART to receive fenofibrate or fish oil for eight weeks. Of 47 subjects on fish oil, 4 (8.5%) and of 48 on fenofibrate, 8 (16.7%) achieved TG < 200 mg/dL.59 When both interventions were offered to individuals who have not responded, 22% more reached target levels of triglycerides. As observed in the other study, there was an increment of LDL-c.57,58
Another study also demonstrated the benefits of polyunsaturated fatty acids omega 3 (PUFA) in HIV-infected individuals with triglyceride levels above 300 mg/dL. In the eighth week, patients who received PUFA showed an average reduction of 25% in the levels of triglycerides compared to a 1% increase in those who received the paraffin oil (p = 0.0033). In this study, nutritional guidance was also significantly important to reduce triglycerides.59
Hypolipemiants drugs in HIV infection and AIDS
Drug therapy becomes necessary when changes in lifestyle are not effective in reducing lipid level.24 Statins are the agents of choice (to reduce total cholesterol and LDL-c) and fibrates (to reduce triglycerides levels), especially gemfibrozil, fenofibrate and bezafibrate.24,60-74 In extreme condition, the association of both classes could be tried. However, these should be avoided as they could be associated with adverse effects, potential drug interactions, adherence problems and increased treatment costs.
There are few data from clinical trials with the use of statins in HIV-infected individuals. Most statins are metabolized by the cytochrome P450, isoenzyme 3A4 (CYP3A4), which is inhibited by most PIs. This could lead to an increase in serum levels of the statin and higher chance to adverse effects. Some statins are not recommended and others are considered safe to use along with cART.24,60 Simvastatin and lovastatin, which are highly metabolized by CYP3A4, are contraindicated; atorvastatin and rosuvastatin can be used with caution; and although with the lowest potency, pravastatin and fluvastatin could be more safely used, as they are mostly not metabolized by CYP3A4 isoenzyme.24,61
Henry et al. investigated the effect of atorvastatin and gemfibrozil compared to diet and exercise in HIV-positive individuals with hypertriglyceridemia. Diet and exercise decreased the levels of total cholesterol and triglycerides in 11% and 21% respectively, while gemfibrozil in combination with atorvastatin reduced the levels of total cholesterol and triglycerides by 30% and 60% respectively.47 Similarly, Miller et al. showed that gemfibrozil and diet (low saturated fat) decreased serum levels of triglycerides in 120 mg/dL, when compared to diet (p = 0.08).63
To evaluate the effectiveness of fibrates (bezafibrato, gemfibrozil and fenofibrate) and statins (pravastatin and fluvastatin) in the management of hyperlipidemia associated with the administration of PI-based cART, Calza et al. followed 288 dislipidemic individuals submitted to diet and physical activity. At the end of at least three months, 61% of the subjects responded to diet, and 106 (39%) in whom lipid levels did not decrease, were randomized to either one hypolipemiant drug. Individuals treated with fibrates had a reduction of 41% and 23%, in the levels of triglycerides and total cholesterol, respectively, after six months of treatment, and 41% and 22% in one year (LDL-c decreased by 23% and HDL-c increased by 20%). In the statin group there was a 36% and 27% reduction of triglycerides and total cholesterol after 6 months, and 34% and 25% after one year (LDL-c reduced by 26% and HDL-c increased by 24%).60
Recently the effectiveness of switching PIs for NNRTI (nevirapine or efavirenz) or hypolipemiants (statin and fibrate) was evaluated in 138 patients during 12 months.64 At the end of follow-up, there was a reduction in the levels of triglycerides by 25% in the group with nevirapine, 9% in the group with efavirenz, 41% with pravastatin and 47% with bezafibrate, which favoured hypolipemiants. Similar results were found with respect of total cholesterol and LDL-c. This study showed that in mixed hyperlipidemia associated with cART and nonresponsive to changes in lifestyle, treatment with a statin or a fibrate was more effective than switching PIs for NNRTIs.
A Brazilian study assessed the behavior of lipid profile before and after treatment with bezafibrate in 84 subjects with persistent hypertriglyceridemia that was not controlled with diet only. There was a significant reduction in levels of triglycerides (from 640 mg/dL to 372 mg/dL, p < 0.0001) and total cholesterol (from 253 mg/dL to 228 mg/dL, p < 0.01).65
In order to evaluate the effect of new drugs for lowering lipids not entirely metabolized by CYP3A4 in HIV-positive population, Calza et al. administered 10 mg/day of rosuvastatin in 16 patients with hypertriglyceridemia that were taking lopinavir/ritonavir. After 24 weeks there was an average reduction in the levels of total cholesterol and triglycerides of 21.7% and 30.1% respectively.64 Similarly, Van der Lee et al. found a reduction in the levels of total cholesterol and LDL-C, 27.6% and 31.8%, respectively (the levels of rosuvastatin were 1.6 times higher when compared with healthy volunteers).66 In both studies the drug was considered relatively safe.
Palacios et al. evaluated the efficacy and safety of atorvastatin 10 mg for the treatment of hypercholesterolemia in 20 patients using antiretroviral therapy for at least 12 months. Atorvastatin was safe and effective with a significant reduction in the levels of total cholesterol and LDL-c after 24 weeks of follow-up.67
Ezetimibe can be as effective as fluvastatin to reduce LDL-c69 and can have additive effect on lipids when administered along with other hypolipemiant drug.69,70,75
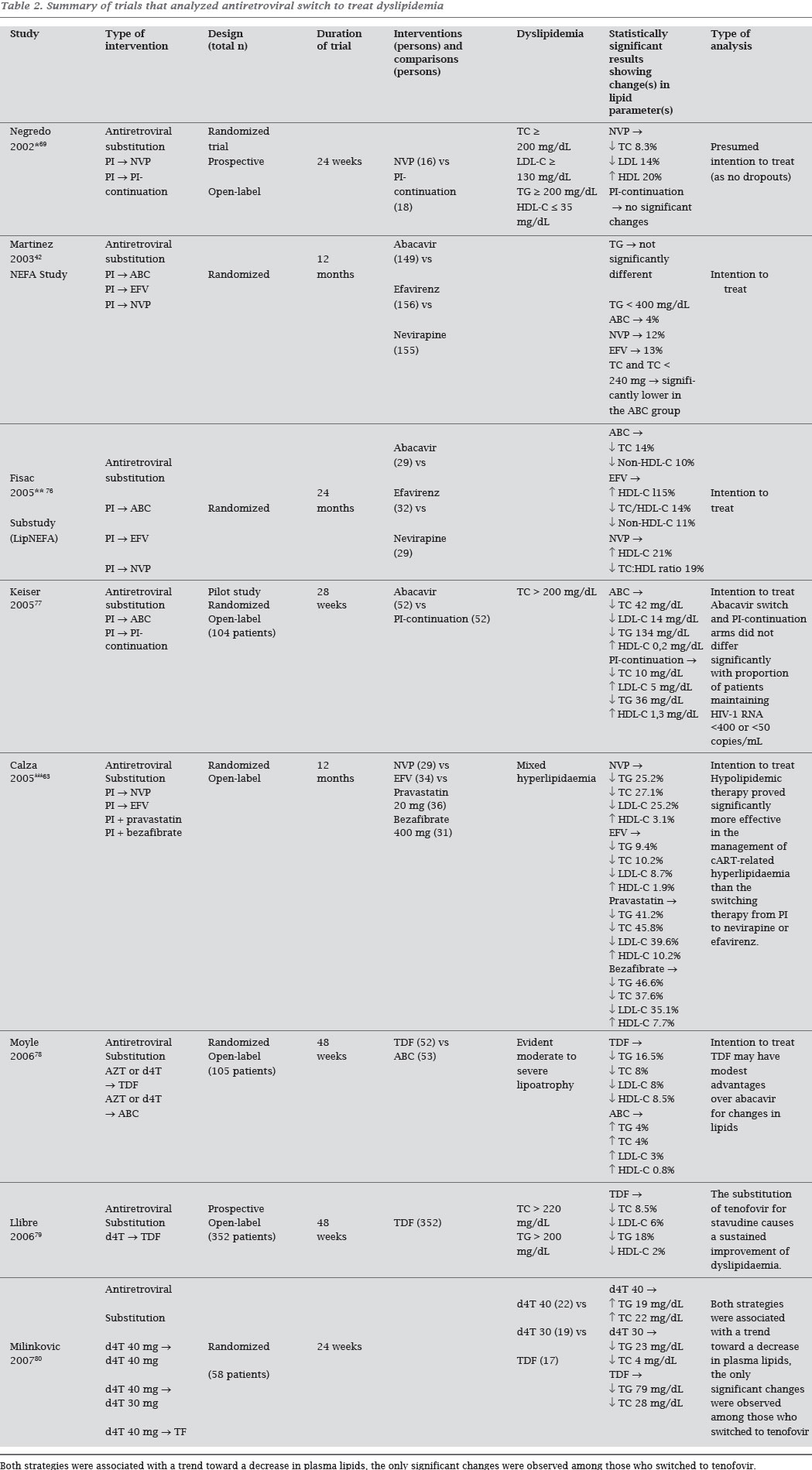
On the basis of all relevant published data, we have prepared a concise, evidence-based update of the current understanding of the clinical presentation. Tables 1 and 2 summarize results of trials conducted to treat dyslipidemia. Although less effective than hypolipemiant agents, sometimes could be easier to change ART due to problems with adherence, risk of interactions and/or increasing toxicity.76-80
Management of dyslipidemia in HIV-positive individuals
In summary, treatment guidelines for the management of dyslipidemia in these patients are the same as those recommended for the general population.24 Life style modification is the primary and first target of treatment. Drug treatment for dyslipidemia in HIV-infected persons on cART can be complex, given the possible drug interactions, toxicity, intolerance, and even impair adherence. There is strong enough evidence to support the use of fibrates to treat hypertriglyceridemia. They are relatively safe and not associated with major side effects. They also can decrease to some extend cholesterol level as well. On the other hand, hypercholesterolemia drug management is not so simple. Statins, the preferred drug class to decrease cholesterol, might be associated with side effects and drug interaction which could interfere to cART treatment. While fluvastatin and pravastatin are safe, although not very effective, simvastatin and lovastatin are contraindicated in individuals on cART which includes PI and/or ritonavir (risk of severe adverse event). The statin plasma levels are highly increased when used along with these agents. The other statins atorvastatin and rosuvastatin have better therapeutic index; they are more efficacious and could be more safely used. Conversely, the non-nucleosides efavirenz, and nevirapine can induce CYP3A4, which would decrease the statin levels. Therefore, the statin dose should be titrated in order to achieve the desirable target. Therefore, we still need to develop more friendly and safe antiretroviral drugs while a cure is not yet found to HIV infection.
Submitted on: 03/04/2010
Approved on: 03/22/2010
We declare no conflict of interest.
- 1. Palella FJ Jr, Delaney KM, Moorman AC et al Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998;338:853-60.
- 2. Tuboi SH, Brinkhof MWG, Egger M et al Discordant responses to potent antiretroviral treatment in previously naive HIV-1-infected adults initiating treatment in resource-constrained countries: the antiretroviral therapy in low-income countries (ART-LINC) collaboration. J Acquir Immune Defic Syndr 2007;45:52-9.
- 3. Marins JR, Jamal LF, Chen SY et al Dramatic improvement in survival among adult Brazilian AIDS patients. AIDS 2003;17:1675-82.
- 4. Braitstein P, Brinkhof MW, Dabis F et al Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet 2006;367:817-24.
- 5. Fang CT, Chang YY, Hsu HM et al Life expectancy of patients with newly-diagnosed HIV infection in the era of highly active antiretroviral therapy. Q J Med 2007;100:97-105.
- 6. Lohse N, Hansen AB, Gerstoft J, Obel N. Improved survival in HIV-infected persons: consequences and perspectives. J Antimicrob Chemother 2007;60:461-3.
- 7. Carr A, Sâmaras K, Burton S et al A syndrome of peripheral lipodystrophy, hyperlipidemia and insulin resistance in patients receiving HIV protease inhibitors. AIDS 1998;12:51-8.
- 8. Mattevi VS, Gasparotto AS, Lazzaretti RK et al Apolipoprotein B gene polymorphisms are associated with higher cholesterol levels in HIV-infected individuals on HAART. Antiviral Therapy 2009; 14 (suppl 2): A52.
- 9. Noor MA. The role of protease inhibitors in the pathogenesis of HIV-associated insulin resistance: cellular mechanisms and clinical implications. Curr HIV/AIDS Rep. 2007;4:126-34.
- 10. Maagaard A, Kvale D. Mitochondrial toxicity in HIV-infected patients both off and on antiretroviral treatment: a continuum or distinct underlying mechanisms? J Antimicrob Chemother 2009;64:901-9. Epub 2009 Sep 9.
- 11. Côté HC. Mechanisms of antiretroviral therapy-induced mitochondrial dysfunction. Curr Opin HIV AIDS. 2007 Jul;2(4):253-60.
- 12. Carr A, Cooper DA. Adverse effects of antiretroviral therapy. Lancet 2000; 356:1423-30.
- 13. Friis-Møller N, Sabin CA, Weber R et al Cardiovascular disease risk factors in HIV patients-association with antiretroviral therapy. Results from the DAD study. AIDS 2003;17:1179-93.
- 14. D:A:D Study Group, Sabin CA, Worm SW et al Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multi-cohort collaboration. Lancet 2008; 371:1417-26.
- 15. Grinspoon S, Carr A. Cardiovascular risk and body-fat abnormalities in HIV-infected adults. N Engl J Med 2005;352:48-62.
- 16. Carr A, Samaras K, Thorisdottir A et al Diagnosis, prediction, and natural course of HIV-1 protease-inhibitor-associated lipodystrophy, hyperlipidaemia, and diabetes mellitus: a cohort study. Lancet 1999;353:2093-9.
- 17. Gervasoni C, Ridolfo AL, Trifiro G et al Redistribution of body fat in HIV-infected women undergoing combined antiretroviral therapy. AIDS 1999;13:465-71.
- 18. Safrin S, Grunfeld C. Fat Distribution and metabolic changes in patients with HIV infection. AIDS 1999;13:2493-505.
- 19. Grunfeld C, Tien P. Difficulties in understanding the metabolic complications of acquired immune deficiency syndrome. Clin Infect Dis 2003;37:43-46.
- 20. Asztalos BF, Schaefer EJ, Horvath KV et al Protease inhibitor-based HAART, HDL, and CHD-risk in HIV-infected patients. Atherosclerosis 2006;184:72-7.
- 21. Stein JH, Klein MA, Bellehumeur JL et al Use of human immunodeficiency virus-1 protease inhibitors is associated with atherogenic lipoprotein changes and endothelial dysfunction. Circulation 2001;104:257-62.
- 22. Grunfeld C, Pang M, Doerrler W et al Lipids, lipoproteins, triglyceride clearance, and cytokines in human immunodeficiency virus infection and the acquired immunodeficiency syndrome. J Clin Endocrinol Metab 1992;74:1045-52.
- 23. Zangerle R, Sarcletti M, Gallati H et al Decreased plasma concentrations of HDL cholesterol in HIV-infected individuals are associated with immune activation. J Acquir Immune Defic Syndr 1994;7:1149-56.
- 24. Dubé MP, Stein JH, Aberg JA et al Guidelines for the evaluation and management of dyslipidemia in human immunodeficiency virus (HIV)-infected adults receiving antiretroviral therapy: Recommendations of the HIV Medicine Association of the Infectious Disease Society of America and the Adult AIDS Clinical Trials Group. Clin Infect Dis 2003;37:613-27.
- 25. Mooser V, Carr A. Antiretroviral therapy-associated hyperlipidaemia in HIV disease. Curr Opin Lipidol 2001;12:313-19.
- 26. Riddle TM, Kuhel DG, Woollett LA et al HIV protease inhibitor induces fatty acid and sterol biosynthesis in liver and adipose tissues due to the accumulation of activated sterol regulatory element-binding proteins in the nucleus. J Biol Chem 2001;276:37514-9.
- 27. Liang JS, Distler O, Cooper DA et al HIV protease inhibitors protect apolipoprotein B from degradation by the proteasome: a potential mechanism for protease inhibitor-induced hyperlipidemia. Nat Med 2001;7:1327-31.
- 28. Grunfeld C, Doerrler W, Pang M et al Abnormalities of apolipoprotein E in the acquired immunodeficiency syndrome. J Clin Endocrinol Metab 1997;82:3734-40.
- 29. Shahmanesh M, Jaleel H, DeSilva Y et al Protease inhibitor related type III hyperlipoproteinaemia is common and not associated with apolipoprotein-E E2/E2 phenotype. Sex Transm Infect 2001;77:283-6
- 30. Hertel J, Struthers H, Horj CB, Hruz PW. A structural basis for the acute effects of HIV protease inhibitors on GLUT4 intrinsic activity. J Biol Chem 2004;279:55147-52.
- 31. Murata H, Hruz PW, Mueckler M. Indinavir inhibits the glucose transporter isoform Glut4 at physiologic concentrations. AIDS 2002;16:859-63.
- 32. Bastard JP, Caron M, Vidal H et al Association between altered expression of adipogenic factor SREBP1 in lipoatrophic adipose tissue from HIV-1-infected patients and abnormal adipocyte differentiation and insulin resistance. Lancet 2002;359:1026-31.
- 33. Mynarcik, DC, Combs T, McNurlan MA et al Adiponectin and leptin levels in HIV-infected subjects with insulin resistance and body fat redistribution. J Acquir Immune Defic Syndr 2002; 31: 514-20.
- 34. Tontonoz P, Hu E, Spiegelman BM. Regulation of adipocyte gene expression and differentiation bt peroxisome proliferator activated receptor c. Curr Opin Genet Dev 1995; 5: 571-76.
- 35. Brinkman K, Smeitink JA, Romijn JA, Reiss P. Mitochondrial toxicity induced by nucleoside-analogue reverse-transcriptase inhibitors is a key factor in the pathogenesis of antiretroviraltherapy-related lipodystrophy. Lancet 1999;354:1112-5.
- 36. Nolan D, Hammond E, Martin A et al, Mitochondrial DNA depletion and morphologic changes in adipocytes associated with nucleoside reverse transcriptase inhibitor therapy. AIDS 2003;17:1329-38.
- 37. The DAD Study Group. Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med 2007;356:1723-35.
- 38. Triant VA, Lee H, Hadigan C, Grinspoon SK. Increased acute myocardial infarction rates and cardiovascular risk factors among patients with human immunodeficiency virus disease. J Clin Endocrinol Metab 2007;92:2506-12.
- 39. Bozzette SA, Ake CF, Tam HK et al Cardiovascular and cerebrovascular events in patients treated for human immunodeficiency virus infection. N Engl J Med 2003;348:702-10.
- 40. Law MG, Friis-Møller N, El-Sadr WM et al The use of the Framingham equation to predict myocardial infarctions in HIV-infected patients: comparison with observed events in the DAD Study. HIV Medicine 2006;7:218-30.
- 41. El-Sadr WM, Lundgren JS, Neaton JD. CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med 2006;355:2283-96.
- 42. Martinez E, García-Viejo MA, Blanco JL et al Impact of switching from human immunodeficiency virus type 1 pro-tease inhibitors to efavirenz in successfully treated adults with lipodystrophy. Clin Infect Dis 2000;31:1266-73.
- 43. Calza L, Manfred R, Chiodo F. Dyslipidaemia associated with antiretroviral therapy in HIV-infected patients. J Antimicrob Chemother 2004;53:10-14.
- 44. Savês M, RaffiF, Capeau J et al Factors related to lipodystrophy and metabolic alterations in patients with human immunodeficiency virus infection receiving highly active antiretroviral therapy. Clin Infect Dis 2002;34:1396-1405.
- 45. Guimarães AC, Lima M, Mota E et al The cholesterol level of a selected level of a selected Brazilian salaried population: biological and socioeconomic influences. Cardiovascular Disease Prevention 1998;1:306-317.
- 46. Tang JL, Armitage JM, Lancaster T et al Systematic review of dietary intervention trials to lower blood total cholesterol in free-living subjects. BMJ 1998;316:1213-20.
- 47. Yu-Poth S, Zhao G, Etherton T et al Effects of the National Cholesterol Education Programs Step I and Step II dietary intervention programs on cardiovascular disease risk factors: a meta-analysis. Am J Clin Nutr 1999;69:632-46.
- 48. Jones SP, Doran DA, Leatt PB et al Short-term exercise training improves body composition and hyperlipidaemia in HIV-positive individuals with lipodystrophy. AIDS 2001;2049-51.
- 49. Terry L, Sprinz E, Stein R et al Exercise training in HIV-1infected individuals with dyslipidemia and lipodystrophy. Med Sci Sports Exerc 2006;38:411-7.
- 50. Fitch KV, Anderson EJ, Hubbard JL et al Effects of a lifestyle modification program in HIV-infected patients with the metabolic syndrome. AIDS 2006;20:1843-50.
- 51. Hadigan C, Jeste S, Anderson EJ et al Modifiable dietary habits and their relation to metabolic abnormalities in men and women with human immunodeficiency virus infection and fat redistribution. Clin Infect Dis 2001;33:710-7.
- 52. Batterham MJ, Brown D, Workman C. Modifying dietary fat intake can reduce serum cholesterol in HIV-associated hypercholesterolemia. AIDS 2002;17:1414-6.
- 53. Batterham MJ, Garsia R, Greenop PA. Dietary intake, serum lipids, insulin resistance and body composition in the era of highly active antiretroviral therapy Diet FRS Study. AIDS 2000;14:1839-43.
- 54. Barrios A, Blanco F, García-Benayas T et al Effect of dietary intervention on highly active antiretroviral therapy-treated dyslipidemia. AIDS 2002;16:2079-81.
- 55. Shah M, Tierney K, Adams-Huet B et al The role of diet, exercise and smoking in dyslipidaemia in HIV-infected patients with lipodystrophy. HIV Med 2005;6:291-8.
- 56. Bang HO, Dyerberg J, Sinclair HM. The composition of the Eskimo food in north western Greenland. Am J Clin Nutr 1980;33:2657-61.
- 57. Wohl DA, Tien HC, Busby M et al Randomized study of the safety and efficacy of fish oil (omega-3 fatty acid) supplementation with dietary and exercise counseling for the treatment of antiretroviral therapy-associated hypertriglyceridemia. Clin Infect Dis 2005;41:1498-504.
- 58. Gerber JG, Kitch DW, Fichtenbaum CJ et al Fish oil and fenofibrate for the treatment of hypertriglyceridemia in HIV-infected subjects on antiretroviral therapy: results of ACTG A5186. J Acquir Immune Defic Syndr 2008;47:459-66.
- 59. De Truchis P, Kirstetter M, Perier A et al Reduction in triglyceride level with N-3 polyunsaturated fatty acids in HIV-infected patients taking potent antiretroviral therapy: a randomized prospective study. J Acquir Immune Defic Syndr 2007; 44:278-85.
- 60. Calza L, Manfredi R, Chiodo F. Statins and fibrates for the treatment of hyperlipidaemia in HIV-infected patients receiving HAART. AIDS 2003;17:851-9.
- 61. Martínez E, Leyes P, Ros E. Effectiveness of lipid-lowering therapy in HIV patients. Curr Opin HIV AIDS 2008;3:240-6.
- 62. Henry K, Melroe H, Huebesch J et al Atorvastatin and gemfibrozil for protease-inhibitor-related lipid abnormalities. Lancet 1998;352:1031-2.
- 63. Miller J, Brown D, Amin J et al A randomized, double-blind study of gemfibrozil for the treatment of protease inhibitor- associated hypertriglyceridemia. AIDS 2002;16:2195-200.
- 64. Calza L, Manfredi R, Colangeli V et al Substitution of nevi-rapine or efavirenz for protease inhibitor versus lipid-lowering therapy for the management of dyslipidaemia. AIDS 2005;19:1051-8.
- 65. Hajjar LA, Carleraro D, Yu PC et al Cardiovascular manifestations in patients infected with the human immunodeficiency virus. Arq Bras Cardiol 2005;85:363-77.
- 66. Van der Lee M, Sabkatsing R, Schippers E et al Pharmacokinetics and pharmacodynamics of combined use of lopinavir/ritonavir and rosuvastatin in HIV-infected patients. Antivir Ther. 2007;12:1127-32.
- 67. Palacios R, Santos J, González M et al Efficacy and Safety of Atorvastatin in the Treatment of Hypercholesterolemia Associated With Antiretroviral Therapy. J Acquir Immune Defic Syndr 2002;30:536-7.
- 68. Coll B, Aragonés G, Parra S et al. Ezetimibe effectively decreases LDL-cholesterol in HIV-infected patients. AIDS 2006;20:1675-7.
- 69. Negredo E, Ribalta J, Paredes R et al. Reversal of atherogenic lipoprotein profile in HIV-1 infected patients with lipodystrophy after replacing protease inhibitors by nevirapine. AIDS 2002; 16: 1383-89.
- 70. Bennett MT, Johns KW, Bondy GP. Ezetimibe is effective when added to maximally tolerated lipid lowering therapy in patients with HIV. Lipids Health Dis 2007;6:15.
- 71. Calza L, Manfredi R, Chiodo F. Use of fibrates in the management of hyperlipidaemia in HIV-infected patients receiving HAART. Infection 2002;30: 26-31.
- 72. Miller J, Brown D, Amin J et al. A randomised, double-blind study of gemfibrozil for the treatment of protease inhibitorassociated hypertriglyceridaemia. AIDS 2002;16:2195-00.
- 73. Badiou S, De Boever CM, Dupuy A et al. Fenofibrate improves the atherogenic lipid profile and enhances LDL resistance to oxidation in HIV-positive adults. Atherosclerosis 2004;172 273-9.
- 74. Mallon PWG, Miller J, Kovacic JC, Kent-Hughes J, Norris R, Samaras K, Feneley MP, Cooper DA, Carr A. Effect of pravastatin on body composition and markers of cardiovascular disease in HIV-infected Men a randomized, placebo-controlled study. AIDS 2006;20:1003-10.
- 75. Negredo E, Moltó J, Puig J et al. Ezetimibe, a promising lipid-lowering agent for the treatment of dyslipidaemia in HIV-infected patients with poor response to statins. AIDS 2006;20:2159-64.
- 76. Fisac C, Fumero E, Crespo M et al. Metabolic benefits 24 months after replacing a protease inhibitor with abacavir, efavirenz or nevirapine. AIDS 2005;19:91725.
- 77 Keiser PH, Sension MG, DeJesus E et al. Substituting abacavir for hyperlipidemia-associated protease inhibitors in HAART regimens improves fasting lipid profiles, maintains virologic suppression, and simplifies treatment. BMC Infect Dis 2005;5:2.
- 78. Moyle GJ, Sabin CA, Cartledge J et al. A randomized comparative trial of tenofovir DF or abacavir as replacement for a thymidine analogue in persons with lipoatrophy. AIDS. 2006;20:2043-50.
- 79. Llibre JM, Domingo P, Palacios R et al. Sustained improvement of dyslipidaemia in HAART treated patients replacing stavudine with tenofovir. AIDS 2006;20:1407-14.
- 80. Milinkovic A, Martinez E, López S et al. The impact of reducing stavudine dose versus switching to tenofovir on plasma lipids, body composition and mitochondrial function in HIV-infected patients. Antivir Ther 2007;12:407-15.
Correspondence to:
Publication Dates
-
Publication in this collection
14 Feb 2011 -
Date of issue
Dec 2010
History
-
Accepted
22 Mar 2010 -
Received
04 Mar 2010