Abstract
We report a case of a 67 year-old-male patient admitted to the intensive care unit in the post-coronary bypass surgery period who presented cardiogenic shock, acute renal failure and three episodes of sepsis, the latter with pulmonary distress at the 30th post-operative day. The patient expired within five days in spite of treatment with vancomycin, imipenem, colistimethate and amphotericin B. At autopsy severe adenovirus pneumonia was found. Viral pulmonary infections following cardiovascular surgery are uncommon. We highlight the importance of etiological diagnosis to a correct treatment approach.
adenovirus infections; human; intensive care units; bronchiolitis; viral; thoracic surgery
CASE REPORT
Fatal adenoviral necrotizing bronchiolitis case in a post-cardiac surgery intensive care unit
Jussara Bianchi CastelliI; Rinaldo F SicilianoII; Ricardo D VieiraIII; Vera D AielloIV; Tânia MV StrabelliV
IMD, PhD; Pathologist: Laboratory of Pathology, Instituto do Coração (InCor), Medical School, Universidade de São Paulo (USP), Brazil
IIMD, Infectologist, Infection Control Unit, InCor, Medical School, USP, Brazil
IIIMD, Cardiologist, Department of Atherosclerosis, InCor, Medical School, USP, Brazil
IVMD, PhD, Pathologist, Laboratory of Pathology, InCor, Medical School, USP, Brazil
VMD, PhD, Infectologist, Infection Control Unit, InCor Medical School, USP, Brazil
Correspondence to Correspondence to: Jussara Bianchi Castelli Laboratório de Anatomia Patológica Instituto do Coração (InCor) - HCFMUSP Av. Dr Enéas Carvalho de Aguiar, 44 São Paulo - SP - Brasil CEP 05403-000 jussara.castelli@incor.usp.br
ABSTRACT
We report a case of a 67 year-old-male patient admitted to the intensive care unit in the post-coronary bypass surgery period who presented cardiogenic shock, acute renal failure and three episodes of sepsis, the latter with pulmonary distress at the 30th post-operative day. The patient expired within five days in spite of treatment with vancomycin, imipenem, colistimethate and amphotericin B. At autopsy severe adenovirus pneumonia was found. Viral pulmonary infections following cardiovascular surgery are uncommon. We highlight the importance of etiological diagnosis to a correct treatment approach.
Keywords: adenovirus infections, human; intensive care units; bronchiolitis, viral; thoracic surgery.
INTRODUCTION
Severe respiratory infections by adenovirus occur in greater frequency in immunosuppressed children and adults as in the context of organ transplant or cancer.1,2 Viral pulmonary infections associated with mechanical ventilation are not frequent and are mainly reported in children and deeply immunossupressed patients. We report a case of fatal necrotizing bronchiolitis by adenovirus in a patient with severe heart disease admitted to the intensive care unit (ICU) in early post-operative cardiac surgery period.
CASE REPORT
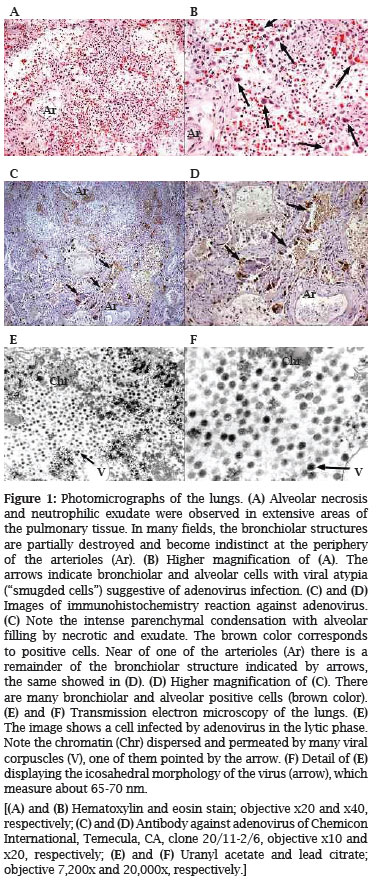
A 67 year-old-male patient, hypertensive and submitted to myocardial revascularization (MR) 17 years before, was presenting recent-onset unstable angina. The echocardiogram showed diffuse ventricular hipocinesia and severe mitral insufficiency, and a new MR and plastic mitral valve replacement due to stenosis was indicated. In the 10th post-surgery day the patient developed cardiogenic shock and acute renal failure, requiring dialysis and prolonged use of dobutamine. During this period he presented two consecutive episodes of severe sepsis: urosepsis at the 15th post-operative day caused by Klebsiella pneumoniae, treated with cefepime for 10 days, followed by a bacterial pneumonia presumably associated with mechanical ventilation treated with vancomycin plus imipenem at the 21th post-operative day. The patient had a partial clinical improvement and at the 30th post-operative day he presented new episode of sepsis with shock requiring noradrenaline, fever and progressive worsening of hypoxemia. The laboratory revealed: hemoglobin 11.2 g/dL, leukocytes 18,100 cells/mL (22% bands, 72% segmented neutrophils and 3% lymphocytes), 102,000 platelets/mm3 and negative urine and blood cultures. In spite of treatment with vancomycin, imipenem, colistimethate and amphotericin B, the patient died within five days. At autopsy there were morphological evidences of cardiogenic shock with multiple organ failure. The lungs showed diffuse alveolar damage and bilateral diffuse injuries of necrotizing bronchiolitis, with airways destruction and presence of numerous smudged cells suggestive of adenoviral infection, confirmed by immunohistochemistry and electron microscopy (Figure 1).
After the result of the autopsy, suspected cases of viral infection were retrospectively investigated among healthcare professionals of the ICU, family members of the patients and among other patients admitted for hospitalization in the same month. No cases of respiratory, conjunctival or gastroenteric viral infection were observed.
DISCUSSION
Adenovirus is responsible for about 5% of respiratory infections in children younger than five years and may have endemic or epidemic behavior. This virus usually causes a self-limited infection of the upper respiratory tract, conjunctivitis and gastroenteritis. Acute bronchiolitis and pneumonia are usually community-acquired and occur in patients with abnormal immunological status.
The occurrence of hospital pneumonia in ICU caused by viruses has been reported as associated with mechanical ventilation. There is no agreed definition of nosocomial viral respiratory infection and the frequencies found in different studies is quite variable (3-60%).3,4 Influenza and respiratory syncytial virus are most often found viruses. Hospital outbreaks of respiratory infections caused by adenovirus are mainly reported in pediatric units and the associated mortality was quite high, ranging from 11 to 91 %.2,5,6 Although it can occasionally occur in immunocompetent hosts, severe pulmonary adenovirus infections occurs predominantly in patients with cellular immune impairment of allogenic stem cell transplantation, solid organ transplantation, and HIV infection.1 The patient presented here had no clear immunosuppressive condition before hospitalization. However, at the time of diagnosis of severe adenovirus infection, the patient was critically ill and presented immunological deficiency. Besides the fact that the patient was in early postoperative period of cardiac surgery which could lead to Th1 impairment secondary to cardiopulmonary bypass, other factors strongly contribute to immune impairment such as advanced age and severe nosocomial septic events. Sepsis induces changes in both innate and adaptive immunity that presumably lead to increased susceptibility to secondary infections, multiorgan failure, and death.
Viral respiratory infections are uncommon causes of pulmonary infiltrates in immunocompetent individuals during post-operative period and clinically they can be difficult to differentiate from bacterial pneumonia. Absence of clinical response to antibiotic treatment, pneumonia that occurs in winter months and the knowledge of outbreaks of respiratory viral infection in the community or hospital can make the diagnosis of viral pneumonia more presumptive. In addition, the extrapulmonary flu-like symptoms can be overlooked in the sedated patient for invasive ventilation. The etiological diagnosis can be demonstrated through cytological and immunocytochemical analysis of the broncoalveolar lavage as well as with molecular biology techniques and cell culture. Unusual microorganisms should be investigated mainly if poor response to therapy is observed.
Horizontal transmission in hospital settings are well documented by molecular epidemiology. Adenovirus could be transmitted from the index case through the hands of healthcare workers or via contaminated equipment or environment. Considering that the incubation period of the adenovirus is less than 10 days, the contamination of the patient herein presented by the virus originated in the ICU. There were no suspected cases of viral infection among health professionals, family members of patients or among other patients hospitalized that month. However, this study was retrospective and no tests to detect virus could be conducted among the other patients with nosocomial pneumonia in that unit.
In conclusion, we present a case of hospital acquired pneumonia caused by adenovirus in a critically ill patient acutely immunosuppressed during the post-cardiac surgery period. We stress the possibility of adenovirus infection in nosocomial pneumonia in critically ill patients.
Submitted on: 11/23/2010
Approved on: 12/23/2010
We declare no conflict of interest.
- 1. Hakim FA, Tleyjeh IM. Severe adenovirus pneumonia in immunocompetent adults: a case report and review of the literature. Eur J Clin Microbiol Infect Dis. 2008; 27(2):153-8.
- 2. Faden H, Wynn RJ, Campagna L, Ryan RM. Outbreak of adenovirus type 30 in a neonatal intensive care unit. J Pediatr. 2005; 146(4):523-7.
- 3. Garbino J, Gerbase MW, Wunderli W et al Respiratory viruses and severe lower respiratory tract complications in hospitalized patients. Chest 2004; 125(3):1033-9.
- 4. Silva AR, Park M, Costa SF et al Respiratory virus infections in Intensive Care Unit (ICU) patients in São Paulo, Brazil.. In: 12th International Congress on Infectious Diseases, 2006, Lisboa. Int J Infect Dis. 2006. p. 188-188.
- 5. Hatherill M, Levin M, Lawrenson et al Evolution of an adenovirus outbreak in a multidisciplinary childrens hospital. J Paediatr Child Health 2004; 40(8):449-54.
- 6. Wesley AG, Pather M, Tait D. Nosocomial adenovirus infection in a paediatric respiratory unit. J Hosp Infect 1993; 25(3):183-90.
Correspondence to:
Publication Dates
-
Publication in this collection
06 June 2011 -
Date of issue
June 2011
History
-
Received
23 Nov 2010 -
Accepted
23 Dec 2010