Abstract
Chikungunya is an arthropod-borne virus transmitted by Aedes mosquito bites. A viral mutation has allowed Aedes albopictus to become the preferred vector extending the geographic spread of the condition. The virus causes an acute febrile illness occasionally followed by a chronic rheumatic condition causing severe impairment. The diagnosis is usually confirmed with serology. No specific treatment is currently available. This article reviews the condition with emphasis on his dissemination in the Americas.
Keywords
Chikungunya; Alphavirus; Epidemics
Chikungunya virus has disseminated widely and autochthonous cases have already been reported in the Americas. Although the disease tends to be self-limited, a crippling chronic condition with severe joint compromise can affect patients for weeks to months. Health practitioners need to be acquainted with the manifestations, diagnostic methods and treatment options for this formerly “exotic” condition.
Agent
The Chikungunya virus (CHIKV) is an arthropod-borne virus that belongs to the family Togaviridae, genus Alphavirus. Its genome is composed by a single stranded positive polarity RNA molecule. The genome codifies four non-structural proteins (NS P 1-4) and three structural proteins (C, E1 and C2). The virus gets destroyed by desiccation and by temperatures above 58 °C.11 A.H. Khan, K. Morita, C. Parquet Md Mdel, F. Hasebe, E.G. Mathenge, A. Igarashi. Complete nucleotide sequence of chikungunya virus and evidence for an internal polyadenylation site. J Gen Virol. 2002; 83:3075p The alphavirus genus includes about 29 species, seven of these viruses can causes joint disorders in humans including CHIKV, O’nyong-nyong (Central Africa), Ross River and Barmah Forest (Australia and the Pacific), Semliki Forest (Africa), Sindbis (Africa, Asia, Australia and Europe), and Mayaro (South America and the French Guyana).22 F. Simon, H. Savini, P. Parola. Chikungunya: a paradigm of emergence and globalization of vector-borne diseases. Med Clin North Am. 2008; 92:1323p
There are three lineages of CHIKV with distinctive genotypic and antigenic characteristics. The virus isolated during the 2004–2006 epidemics in the Indian Ocean belongs to a distinct set within the largest phylogenetic group East/Central/South African (ECSA). However the Asian lineage is the one currently ravaging the Americas. The other group is the West African lineage.33 A.M. Powers, A.C. Brault, R.B. Tesh, S.C. Weaver. Re-emergence of Chikungunya and O’nyong-nyong viruses: evidence for distinct geographical lineages and distant evolutionary relationships. J Gen Virol. 2000; 81:471p
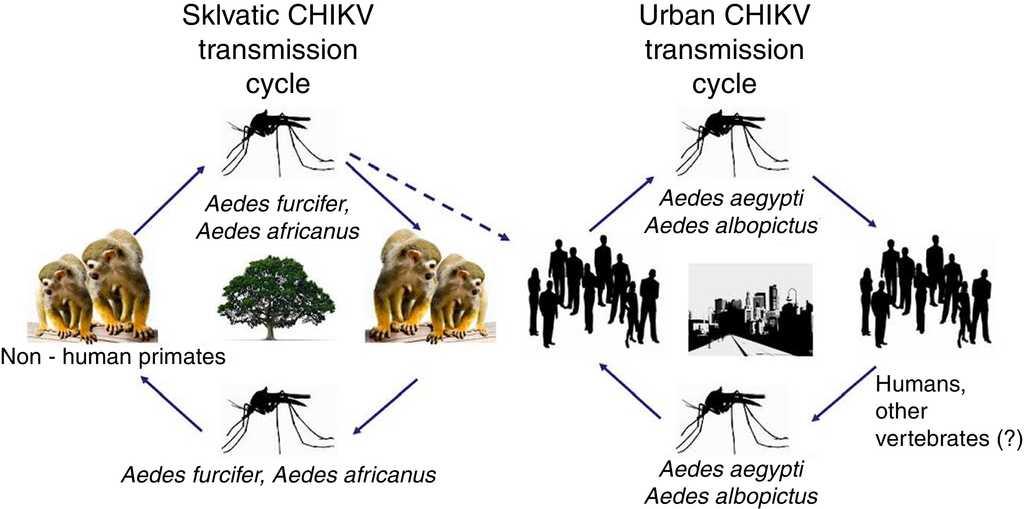
CHIKV persists in nature using two cycles: a sylvatic cycle affecting primates and mosquitoes and an urban cycle affecting humans and mosquitoes (Fig. 1).
- -
Early replication of RNA into mRNA and translation of early regulatory proteins
- -
Late replication of the RNA into mRNA and translation of late structural proteins
- -
Assembly of structural proteins and single stranded positive RNA, and virion maturation.44 J.H. Strauss, E.G. Strauss. The alphaviruses: gene expression, replication, and evolution. Microbiol Rev. 1994; 58:491p
Vector
Although there is an ample range of Aedes species that transmit the disease in Africa55 M. Diallo, J. Thonnon, M. Traore-Lamizana, D. Fontenille. Vectors of Chikungunya virus in Senegal: current data and transmission cycles. Am J Trop Med Hyg. 1999; 60:281p; in Asia and in the Indian Ocean the main vectors of CHIKV are Aedes aegypti and Aedes albopictus. A. albopictus has a wider geographical distribution, and can survive in both rural and urban environments. Mosquito eggs are quite resistant to dry seasons. A. albopictus also has a relatively long life, lasting 4–8 weeks and has a flying range of 400–600 m.66 C. Chevillon, L. Briant, F. Renaud, C. Devaux. The Chikungunya threat: an ecological and evolutionary perspective. Trends Microbiol. 2008; 16:80p All these capabilities have allowed A. albopictus to become an important vector not only of CHIKV, but also of dengue and other arbovirosis. A comparison between A. aegypti and A. albopictus is presented in Table 1.
In Brazil, an extensive DDT campaign eradicated A. aegypti from the country in the 1940–50s, however the vector was reintroduced in 1970 and become widespread again. Since 1986 it has been considered endemic in several major Brazilian cities. A. albopictus invaded Brazil in the 1980s and a recent survey has detected it in at least 59% of the Brazilian municipalities and in 24 of the 27 federal units77 R.G. Carvalho, R. Lourenço-de-Oliveira, I.A. Braga. Updating the geographical distribution and frequency of Aedes albopictus in Brazil with remarks regarding its range in the Americas. Mem Inst Oswaldo Cruz. 2014; 109:787p 88 F.A. Monteiro, R. Schama, A.J. Martins, A. Gloria-Soria, J.E. Brown, J.R. Powell. Genetic diversity of Brazilian Aedes aegypti: patterns following an eradication program. PLoS Negl Trop Dis. 2014; 8:e3167pA. aegypti affects predominantly tropical areas of Brazil (North, North-East and Central regions) and is more widespread, whereas A. albopictus is more common in the cooler Southern areas of the country. Both vectors combined put 99% of the population of Brazil at risk of acquiring CHIKV.99 M.R. Nunes, N.R. Faria, J.M. de Vasconcelos. Emergence and potential for spread of chikungunya virus in Brazil. BMC Med. 2015; 13:102p Fig. 2 shows the geographic distribution of Chikungunya virus in the Americas.
Chikungunya in the Americas. In red: countries with endemic transmission with more than 1000 cases reported. In orange: Countries with endemic transmission with more than 1000 cases reported. In blue: Countries or States with imported cases only. Without color: Countries or States with no transmission reported.
In the United States, A. aegypti has been established for more than 300 years and since 1985 the Southeast of the United States has been invaded by A. albopictus, with a range extending from South Florida to Illinois.1010 J.P. Harper, S.L. Paulson. Reproductive isolation between Florida strains of Aedes aegypti and Aedes albopictus. J Am Mosq Control Assoc. 1994; 10:88p
The adaptation of CHIKV to A. albopictus is a relatively recent event. During the outbreak in the Indian Ocean in 2005–2006 the virus has acquired a mutation at residue 226 of the membrane fusion glycoprotein-1, which allows it to infest A. albopictus. This mutation is likely the cause of the wide spread of the disease.1111 I. Schuffenecker, I. Iteman, A. Michault. Genome microevolution of chikungunya viruses causing the Indian Ocean outbreak. PLoS Med. 2006; 3:e263p
Pathogenesis
CHIKV is transmitted predominantly by female mosquito bites. Alternatively the disease can be transmitted vertically from mother to fetus or theoretically by blood transfusion (although no cases have been reported so far).
After the inoculation, the virus invades endothelial cells and subcutaneous fibroblasts and replicates in a limited fashion. Circulating blood cells may be refractory to invasion. New viruses are transported to local lymph nodes where they further replicate. A significant viremia which can reach up to 108 copies/mL then ensues.1212 M. Sourisseau, C. Schilte, N. Casartelli. Characterization of reemerging chikungunya virus. PLoS Pathog. 2007; 3:e89p In the initial phases there is a massive infection of monocyte-derived macrophages which act as “Trojan horses” and transport the virus into target organs including muscle, joints, the liver and the brain.1313 Z. Her, B. Malleret, M. Chan. Active infection of human blood monocytes by Chikungunya virus triggers an innate immune response. J Immunol. 2010; 184:5903p
The innate immune response is activated by the virus via pattern recognition receptors. This triggers the production of type I interferon and activates interferon-stimulated genes which encode more than 300 proteins, with crucial roles in the host defense. In vitro studies have shown that CHIKV can be highly suppressed when interferon α/β is added to cells prior to infection.1414 O. Schwartz, M.L. Albert. Biology and pathogenesis of chikungunya virus. Nat Rev Microbiol. 2010; 8:491p
Flow cytometry showing CD8+ T lymphocyte response in the early stages of the disease and a CD4+ T lymphocyte-mediated response in the later stages, as well as production of several pro-inflammatory cytokines are evidence of a subsequent adaptive immunity reaction.1515 N. Wauquier, P. Becquart, D. Nkoghe, C. Padilla, A. Ndjoyi-Mbiguino, E.M. Leroy. The acute phase of Chikungunya virus infection in humans is associated with strong innate immunity and T CD8 cell activation. J Infect Dis. 2011; 204:115p There is heterogeneity in the cytokines expressed, reflecting the time of the illness in which they are measured and the different genetic backgrounds of the individuals affected. The persistence of a local reservoir of infected monocytes in the joints may potentially explain chronic arthritis in a subset of patients. Patients with chronic joint disease may have high levels of interleukin 6 and granulocyte macrophage colony-stimulating factor, but not of tumor necrosis factor (TNF) or IL-1b (a pattern seen in other inflammatory arthritides). Chronically affected patients also have normal levels of hepatocyte growth factor and eotaxin, as compared with recovered patients, suggesting an inability of the former subjects to maintain an immune mechanism associated with clinical recovery.1616 A. Chow, Z. Her, E.K. Ong. Persistent arthralgia induced by Chikungunya virus infection is associated with interleukin-6 and granulocyte macrophage colony-stimulating factor. J Infect Dis. 2011; 203:149p
Clinical manifestations
The incubation period for CHIKV virus ranges between 1 and 12 days. The disease usually presents abruptly with high fever, rash, back aches and myalgia. The febrile episode lasts 3–4 days. Occasionally there is a second febrile course lasting shortly. Arthralgia and arthritis are extremely common and usually polyarticular and distal, with as many as ten joints involved. Both, small and large joints can be affected. Symmetric inflammation is common, but unilateral compromise is possible. The pain is intense and crippling, preventing patients from sleeping and ambulating properly. Articular symptoms subside within 1 to 3 weeks. Other manifestation include headache; photophobia; sore throat; abdominal pain, diarrhea and vomiting; and cervical or generalized lymphadenopathy.1717 A. Mohan, D.H. Kiran, I.C. Manohar, D.P. Kumar. Epidemiology, clinical manifestations, and diagnosis of Chikungunya fever: lessons learned from the re-emerging epidemic. Indian J Dermatol. 2010; 55:54p
A morbilliform rash mostly non-pruritic, initially appearing in the upper limbs is the most common cutaneous manifestation. The rash may evolve into a vesiculobullous and rarely a purpuric exanthema, particularly in children. Hyperpigmentation in the centrofacial area and intertriginous ulcers can also be seen.1818 D. Bandyopadhyay, S.K. Ghosh. Mucocutaneous features of Chikungunya fever: a study from an outbreak in West Bengal, India. Int J Dermatol. 2008; 47:1148p
Traditionally CHIKV infection was not associated with neurologic involvement, however cases of encephalitis, meningitis, acute flaccid paralysis and sensorineural hearing loss have been described in the recent outbreaks. Among neurologic symptoms, the most prevalent seem to be abnormal mental status, headache, focal deficits and seizures.1919 Rampal, M. Sharda, H. Meena. Neurological complications in Chikungunya fever. J Assoc Physicians India. 2007; 55:765p
Photophobia, retro-orbital pain and conjunctival effusion or conjunctivitis are quite common in the acute phase of the illness. Anterior uveitis is the most common serious ocular presentation and can be associated with corneal precipitates and hypopyon. Less commonly, posterior uveitis, retinitis, choroiditis and optic neuritis have been described.2020 P. Mahendradas, K. Avadhani, R. Shetty. Chikungunya and the eye: a review. J Ophthalmic Inflamm Infect. 2013; 3:35p
Hemorrhagic manifestations are rare; however gingivorrhagia, epistaxis, hematemesis and melena have been described in old case series.2121 J.K. Sarkar, S.N. Chatterjee, S.K. Chakravarti, A.C. Mitra. Chikungunya virus infection with haemorrhagic manifestations. Indian J Med Res. 1965; 53:921p Abnormal bleeding, milder than the one seen in dengue fever, has a predilection for children.
A high percentage of pregnant women could be affected by CHIKV (close to 50% in a cohort in the Reunion Island). Symptoms at presentation do not differ from the general population, except for the presence of epistaxis or gingivorrhagia which were seen in 9% of pregnant females. Pregnant women may require hospitalization to rule out other conditions but the outcome of their pregnancies seem to be unaffected: the number of cesarean sections, third trimester bleeding, preterm births, still births, newborns with low weight or newborns with congenital malformations was no different when compared with uninfected women.2222 X. Fritel, O. Rollot, P. Gerardin. Chikungunya virus infection during pregnancy, Reunion, France, 2006. Emerg Infect Dis. 2010; 16:418p
Transplacental transmission is unlikely. Transmission from mother to fetus occurs exclusively at the time of delivery in the setting of intrapartum maternal viremia.2323 D. Ramful, S. Sampériz, X. Fritel. Antibody kinetics in infants exposed to Chikungunya virus infection during pregnancy reveals absence of congenital infection. J Infect Dis. 2014; 209:1726p Affected neonates develop pain, prostration, fever and thrombocytopenia within few days after birth. Some of them may have encephalopathy and intracranial bleeding with prolonged sequela.2424 P. Gérardin, G. Barau, A. Michault. Multidisciplinary prospective study of mother-to-child chikungunya virus infections on the island of La Réunion. PLoS Med. 2008; 5:e60p
In the majority of patients, symptoms abate after 1–3 weeks; however some patients evolve into a chronic condition. Chronic manifestations may include monoarthritis, undifferentiated polyarthritis, joint involvement simulating rheumatoid arthritis (including fulfillment of American Academy of Rheumatology criteria, positive rheumatoid factor and characteristic erosions in the X-ray), tenosynovitis/enthesopathy, seronegative spondyloarthritis and/or back pain.2525 A. Chopra, V. Anuradha, V. Lagoo-Joshi, V. Kunjir, S. Salvi, M. Saluja. Chikungunya virus aches and pains: an emerging challenge. Arthritis Rheum. 2008; 58:2921p 2626 F. Simon, E. Javelle, M. Oliver, I. Leparc-Goffart, C. Marimoutou. Chikungunya virus infection. Curr Infect Dis Rep. 2011; 13:218p The most prominent joint swelling occurs in the ankles and feet.2727 G. Borgherini, P. Poubeau, A. Jossaume. Persistent arthralgia associated with chikungunya virus: a study of 88 adult patients on reunion island. Clin Infect Dis. 2008; 47:469p The intensity of the pain is less severe, but still significant. Extra musculoskeletal manifestations such as rash, alopecia, pruritus, ocular manifestations and Raynaud's phenomenon may also occur.2828 S.D. Thiberville, V. Boisson, J. Gaudart, F. Simon, A. Flahault, X. de Lamballerie. Chikungunya fever: a clinical and virological investigation of outpatients on Reunion Island, South-West Indian Ocean. PLoS Negl Trop Dis. 2013; 7:e2004p The chronic illness takes a toll on the well being of patients who score low in quality-of-life indices. They may be unable to return to work because of difficulties walking and handling objects.2828 S.D. Thiberville, V. Boisson, J. Gaudart, F. Simon, A. Flahault, X. de Lamballerie. Chikungunya fever: a clinical and virological investigation of outpatients on Reunion Island, South-West Indian Ocean. PLoS Negl Trop Dis. 2013; 7:e2004p 2929 C. Schilte, F. Staikowsky, T. Couderc. Chikungunya virus-associated long-term arthralgia: a 36-month prospective longitudinal study. PLoS Negl Trop Dis. 2013; 7:e2137p 3030 P. Gérardin, A. Fianu, A. Michault. Predictors of Chikungunya rheumatism: a prognostic survey ancillary to the TELECHIK cohort study. Arthritis Res Ther. 2013; 15:R9p There is evidence that patients remain symptomatic 18–36 months and even longer after becoming infected.2727 G. Borgherini, P. Poubeau, A. Jossaume. Persistent arthralgia associated with chikungunya virus: a study of 88 adult patients on reunion island. Clin Infect Dis. 2008; 47:469p 2929 C. Schilte, F. Staikowsky, T. Couderc. Chikungunya virus-associated long-term arthralgia: a 36-month prospective longitudinal study. PLoS Negl Trop Dis. 2013; 7:e2137p
Patients with more prominent acute symptoms have higher risk to evolve into the chronic stage: high fevers and chills, severe malaise, notable polyarthralgia and generalized myalgia and rash may be predictors of poor outcome.2525 A. Chopra, V. Anuradha, V. Lagoo-Joshi, V. Kunjir, S. Salvi, M. Saluja. Chikungunya virus aches and pains: an emerging challenge. Arthritis Rheum. 2008; 58:2921p Other risk factors for relapsing or persistent CHIKV infection include age older than 45, higher titers of CHIKV antibodies and elevated viral load.2424 P. Gérardin, G. Barau, A. Michault. Multidisciplinary prospective study of mother-to-child chikungunya virus infections on the island of La Réunion. PLoS Med. 2008; 5:e60p 2929 C. Schilte, F. Staikowsky, T. Couderc. Chikungunya virus-associated long-term arthralgia: a 36-month prospective longitudinal study. PLoS Negl Trop Dis. 2013; 7:e2137p Also individuals with prior joint disease are at risk: exacerbation of psoriatic and seronegative arthritides in the setting of CHIKV infection have been described.2525 A. Chopra, V. Anuradha, V. Lagoo-Joshi, V. Kunjir, S. Salvi, M. Saluja. Chikungunya virus aches and pains: an emerging challenge. Arthritis Rheum. 2008; 58:2921p
It is likely that persistence of viral replication in synovial fluid is the cause of chronic manifestations as determined by detection of viral RNA and antigen in the fluid, and by persistent serum elevation of IgM antibodies.3131 J.J. Hoarau, M.C. Jaffar Bandjee, P. Krejbich Trotot. Persistent chronic inflammation and infection by Chikungunya arthritogenic alphavirus in spite of a robust host immune response. J Immunol. 2010; 184:5914p
Although CHIKV disease has been considered self-limited, serious complications have been described as above, in addition lethality can also occur, particularly among the young, the elderly, and the immunocompromised. In Ahmedabad, India during an outbreak in 2006, all cause mortality was increased during the months of August–November, which coincided with the peak of the epidemic.3232 D. Mavalankar, P. Shastri, T. Bandyopadhyay, J. Parmar, K.V. Ramani. Increased mortality rate associated with chikungunya epidemic, Ahmedabad, India. Emerg Infect Dis. 2008; 14:412p
In the other end of the spectrum, seropositive patients without clinical manifestations have also been identified.
Cases of dengue (including the hemorrhagic presentation) and CHIKV coinfection have been described (as they share the same vector) however no coinfection with yellow fever has been reported yet.
Epidemiology
CHIKV is an enzootic virus first isolated in a febrile patient during an outbreak in the Makonde Plateau in Tanzania in 1952.3333 M.C. Robinson. An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952–53. I. Clinical features. Trans R Soc Trop Med Hyg. 1955; 49:28p Since then cases have been reported from tropical and subtropical regions of Africa, the Indian Ocean islands and South and Southeast Asia, usually following a pattern with outbreaks occurring every 7–20 years. The largest epidemic of CHIKV occurred in 2005–2006 in the Reunion Island: about 266,000 residents of this island in the Indic Ocean (34.3% of the population) were affected. Additionally as the Island is an overseas department, many cases were exported to France.2828 S.D. Thiberville, V. Boisson, J. Gaudart, F. Simon, A. Flahault, X. de Lamballerie. Chikungunya fever: a clinical and virological investigation of outpatients on Reunion Island, South-West Indian Ocean. PLoS Negl Trop Dis. 2013; 7:e2004p
In 2006 CHIKV reached continental India. The infection initially affected seven states but in the last report in 2010 had extended to 18 States and territories in the Union.3434 C. Bhagwati, M. Madhulika, K.D. Mehta, Y.S. Goswami. Profile of the chikungunya infection: a neglected vector borne disease which is prevalent in The Rajkot District. J Clin Diagn Res. 2013; 7:1008p Several other countries in South East Asia have reported cases since then and CHIKV is widespread in Malaysia, Sri Lanka and Indonesia.3535 M.M. Thiboutot, S. Kannan, O.U. Kawalekar. Chikungunya: a potentially emerging epidemic?. PLoS Negl Trop Dis. 2010; 4:e623p
In 2007 an outbreak was reported in Ravenna, Italy causing about 100 cases and at least one lethality, triggering efforts by the European Centre for Disease Prevention and Control to maintain vector control capabilities and respond effectively to the emergent outbreak.3636 G. Rezza, L. Nicoletti, R. Angelini. Infection with chikungunya virus in Italy: an outbreak in a temperate region. Lancet. 2007; 370:1840p
In December 2013 the World Health Organization reported the first local transmission of CHIKV in the Americas in the Caribbean island of Saint Martin.3737 M. Fischer, J.E. Staples. Notes from the field: chikungunya virus spreads in the Americas – Caribbean and South America, 2013–2014. MMWR Morb Mortal Wkly Rep. 2014; 63:500p Reports of the disease ravaging other countries of South and Central America have ensued since then. Although cases in returning travelers were previously identified, the CDC described autochthonous cases in Florida in 2014. A climate based mosquito population dynamics stochastic model predicts that areas with marked season variation may become epidemic foci and potential targets for strategic vector control.3838 D. Ruiz-Moreno, I.S. Vargas, K.E. Olson, L.C. Harrington. Modeling dynamic introduction of Chikungunya virus in the United States. PLoS Negl Trop Dis. 2012; 6:e1918p It has been proposed that, because individuals in the US spend far less time outdoors and typically have door and window screens, and air conditioning, the extend of a potential epidemics in the United States will be less vast than in other countries.3939 B.M. Kuehn. Chikungunya virus transmission found in the United States: US health authorities brace for wider spread. JAMA. 2014; 312:776p
The first autochthonous cases of CHIKV in Brazil were confirmed in Oiapoque, Amapa State, on September 13, 2014. An epidemiological and clinical analyses of CHIKV infection occurring in Brazil between April and September of 2014, surprisingly detected in addition to the Asian lineage, several cases of the ECSA lineage in Feira de Santana, Northeast Brazil. The cases reported had not acquired the A226V mutation, but there is concern that this genetic event may occur in the future.99 M.R. Nunes, N.R. Faria, J.M. de Vasconcelos. Emergence and potential for spread of chikungunya virus in Brazil. BMC Med. 2015; 13:102p
Like any other vector transmitted disease the propagation of CHIKV depends on characteristics of the vector, the host and the environment.
Thanks to commercial exchange, A. albopictus has expanded to new geographic areas including more recently the Southeast of the United States and the Caribbean region.4040 C.G. Moore, C.J. Mitchell. Aedes albopictus in the United States: ten-year presence and public health implications. Emerg Infect Dis. 1997; 3:329p As mentioned previously, the A226V mutation has increased the fitness of CHIKV and its ability to replicate in A. albopictus.4141 K.A. Tsetsarkin, D.L. Vanlandingham, C.E. McGee, S. Higgs. A single mutation in Chikungunya virus affects vector specificity and epidemic potential. PLoS Pathog. 2007; 3:e201p
The climatic changes in Europe (and in the rest of the world) have favored the propagation of A. albopictus and in some cases the autochthonous transmission of CHIKV, such in Northern Italy in 2007 (but also cases of dengue in the south of France and in Croatia).3232 D. Mavalankar, P. Shastri, T. Bandyopadhyay, J. Parmar, K.V. Ramani. Increased mortality rate associated with chikungunya epidemic, Ahmedabad, India. Emerg Infect Dis. 2008; 14:412p
Historically CHIKV infection was considered a self-limited and non-lethal disease, however 254 deaths in Reunion were attributed directly or indirectly to CHIKV, thus changing the perspective about the infection and emphasizing the role of the condition of the host in the prognosis of the disease.3232 D. Mavalankar, P. Shastri, T. Bandyopadhyay, J. Parmar, K.V. Ramani. Increased mortality rate associated with chikungunya epidemic, Ahmedabad, India. Emerg Infect Dis. 2008; 14:412p
Diagnosis
The laboratory diagnosis of CHIKV depends on the quality, volume and timing of the sample obtained during the course of the disease.4242 M. Dash, I. Mohanty, S. Padhi. Laboratory diagnosis of chikungunya virus: do we really need it?. Indian J Med Sci. 2011; 65:83p CHIKV infection can be diagnosed and confirmed by direct detection of the virus, viral RNA recognition or identification of serum specific antibodies.4343 A.M. Powers. Chikungunya. Clin Lab Med. 2010; 30:209p
An acute phase serum sample obtained within 7 days of disease onset would likely have a high degree of viremia. This sample will be the best diagnostic option for virus isolation or nucleic acid detection.4444 M. Panning, K. Grywna, M. van Esbroeck, P. Emmerich, C. Drosten. Chikungunya fever in travelers returning to Europe from the Indian Ocean region, 2008. Emerg Infect Dis. 2006; 14:416p Both techniques are highly sensitive and specific, and results can be obtained within hours (for nucleic acid detection) or in 2 days (virus isolation).4545 B. Pastorino, M. Bessaud, M. Grandadam, S. Murri, H.J. Tolou, C.N. Peyrefitte. Development of a TaqMan RT-PCR assay without RNA extraction step for the detection and quantification of African Chikungunya viruses. J Virol Methods. 2005; 124:65p PCR techniques have the advantage of being faster and provide a prompt indication of the viral load in clinical samples and in the supernatant of cultures4242 M. Dash, I. Mohanty, S. Padhi. Laboratory diagnosis of chikungunya virus: do we really need it?. Indian J Med Sci. 2011; 65:83p 4343 A.M. Powers. Chikungunya. Clin Lab Med. 2010; 30:209p 4646 F. Burt, W. Chen, S. Mahalingam. Chikungunya virus and arthritic disease. Lancet Infect Dis. 2014; 14:789p whereas viral isolation by means of cellular culture are slower and require a biosafety level 3 laboratory to reduce the risk of viral transmission. CHIKV isolation can be accomplished by intracerebral inoculation in mice less than a year old4646 F. Burt, W. Chen, S. Mahalingam. Chikungunya virus and arthritic disease. Lancet Infect Dis. 2014; 14:789p or by inoculation in mosquitoes. In vitro cellular culture methods require mosquito cells (C6/36) or other mammal cells including BHK-21, Vero and HeLa. The cytopathic effect the virus causes in these cell lines has a sensitivity comparable to in vivo methods.4747 M.N. Pyndiah, V. Pursem, G. Meetoo. Chikungunya virus isolation using simplified cell culture technique in Mauritius. Med Trop (Mars). 2012; 72:
Most commonly the diagnosis of CHIKV is based on the detection of anti-CHIKV IgM o IgG in acute and convalescent samples. The diagnosis is confirmed by a four-fold rising titer between the aforementioned samples or by demonstration of specific IgM antibodies.4242 M. Dash, I. Mohanty, S. Padhi. Laboratory diagnosis of chikungunya virus: do we really need it?. Indian J Med Sci. 2011; 65:83p 4343 A.M. Powers. Chikungunya. Clin Lab Med. 2010; 30:209p Specific IgM antibodies are readily detected by enzyme linked immunosorbent assay (ELISA) 7 days post infection, thus making this test the preferred indicator of recent infection. Many patients may present too early in the course of the disease and the test may need to be repeated. Immunochromatography may be better for detection of IgG during the convalescent period. IgG antibodies usually persists for years whereas IgM antibodies decline to undetectable levels by 3 or 4 months, although in subjects with chronic symptoms these antibodies may persist for up to 24 months.4646 F. Burt, W. Chen, S. Mahalingam. Chikungunya virus and arthritic disease. Lancet Infect Dis. 2014; 14:789p
Treatment
Currently there is no specific therapy approved for CHIKV disease. The only therapeutic option is symptomatic relief. Hydration and electrolyte balance should be optimized. Paracetamol 1 g three to four times a day in adults; or 50–60 mg per kg body weight per day in divided doses in children; is the treatment of choice for fever, headache and/or pain according to the World Health Organization.4848 World Health Organization. Guidelines on clinical management of Chikungunya fever. Available here: http://www.wpro.who.int/mvp/topics/ntd/Clinical_Mgnt_Chikungunya_WHO_SEARO.pdf [accessed 10.12.15].
http://www.wpro.who.int/mvp/topics/ntd/C...
Other non-steroidal analgesics are also usually recommended for pain control; however aspirin should be avoided to prevent further platelet dysfunction. In crippling cases corticosteroid use has been advocated, although there is not enough scientific information to support their use.4949 W. Taubitz, J.P. Cramer, A. Kapaun. Chikungunya fever in travelers: clinical presentation and course. Clin Infect Dis. 2007; 45:e1p French investigators who have experienced the devastating outbreak in the Reunion Island advocate use of tumor necrosis alpha inhibitors for chronic cases that fulfill the criteria for rheumatoid arthritis or seronegative spondyloarthropathy, but no supportive evidence exists beyond expert advice.
Ribavirin is a purine nucleoside analog currently used in the treatment of hepatitis C. A small study that enrolled 10 patients using ribavirin 200 mg orally twice a day for 7 days showed improvement in arthralgia and returned capacity to ambulate. Unfortunately the study used non-blinded comparators and it was too small to reveal meaningful results.5050 R. Ravichandran, M. Manian. Ribavirin therapy for Chikungunya arthritis. J Infect Dev Ctries. 2008; 2:140p In theory combined use of ribavirin and type I interferon alpha may show a synergistic effect.
Chloroquine can inhibit viral replication in Vero cells by disrupting internalization of CHIKV containing endosomes. An open pilot study on 10 patients who completed 20 weeks of therapy showed significant improvement in the Ritchie articular index (commonly used to evaluate joint involvement in patients with rheumatoid arthritis) and in morning stiffness,5151 S.W. Brighton. Chloroquine phosphate treatment of chronic Chikungunya arthritis. An open pilot study. S Afr Med J. 1984; 66:217p however a small clinical trial failed to show decrease in the duration of viremia. Actually patients on chloroquine in that trial complained or worsening arthralgia as compared with placebo, but the course duration was only 5 days.5252 X. De Lamballerie, V. Boisson, J.C. Reynier. On chikungunya acute infection and chloroquine treatment. Vector Borne Zoonotic Dis. 2008; 8:837p
Anterior and posterior uveitis caused by CHIKV have been treated with topical steroids and cycloplegics, and systemic steroids and acyclovir respectively. The role of acyclovir in this clinical situation is disputed.2020 P. Mahendradas, K. Avadhani, R. Shetty. Chikungunya and the eye: a review. J Ophthalmic Inflamm Infect. 2013; 3:35p
There are a number of drugs which may potentially have effect against CHIKV but they have not been used in clinical trials.2626 F. Simon, E. Javelle, M. Oliver, I. Leparc-Goffart, C. Marimoutou. Chikungunya virus infection. Curr Infect Dis Rep. 2011; 13:218p 5353 P. Kaur, J.J. Chu. Chikungunya virus: an update on antiviral development and challenges. Drug Discov Today. 2013; 18:969p They are summarized in Table 2. Among them siRNA, 21-23 nucleotide small interfering RNA that is homologous in sequence to E2 and ns1 genes of Chikungunya, seem to be highly promising.5454 D. Parashar, M.S. Paingankar, S. Kumar. Administration of E2 and NS1 siRNAs inhibit chikungunya virus replication in vitro and protects mice infected with the virus. PLoS Negl Trop Dis. 2013; 7:e2405p
Human polyvalent immunoglobulins obtained from convalescent patients with CHIKV infection have been purified and used in mouse models and exhibit a high neutralizing activity, preventing viremia.5555 T. Couderc, N. Khandoudi, M. Grandadam. Prophylaxis and therapy for Chikungunya virus infection. J Infect Dis. 2009; 200:516p The use of hyperimmune serum has been successfully explored in other viral diseases, but no human trials have been attempted for CHIKV disease yet. Monoclonal antibodies have also been isolated and used as prophylactic agents in mice lacking type I IFN receptors. These antibodies have shown complete protection against lethality in the murine model.5656 P. Pal, K.A. Dowd, J.D. Brien. Development of a highly protective combination monoclonal antibody therapy against Chikungunya virus. PLoS Pathog. 2013; 9:e1003312p
A case series has reported treatment for 21 patients with chronic CHIKV infection who satisfied the American College of Rheumatology criteria for rheumatoid arthritis (including a positive rheumatoid factor). All patients were treated with disease modifying antirheumatic drugs including methotrexate and TNF blockers, in addition to corticosteroids. Overall the clinical response seems to have been poor.5757 E. Bouquillard, B. Combe. A report of 21 cases of rheumatoid arthritis following Chikungunya fever. A mean follow-up of two years. Joint Bone Spine. 2009; 76:654p
Prevention
The best method to prevent CHIKV is avoidance of mosquito bites. This may be accomplished by use of repellents (preferably containing DEET), wearing of long-sleeved shirts and long pants and use of screens, bed nets and air conditioning.5858 Centers for Disease Control and Prevention. Chikungunya virus – prevention. Available here: http://www.cdc.gov/chikungunya/prevention/.
http://www.cdc.gov/chikungunya/preventio...
Reduction of peridomiciliary water puddles and containers may prevent mosquito proliferation.
Travelers to endemic areas need to be educated about their risks, precautions and symptom recognition.
There is potential of transmission of CHIKV via blood transfusion, although cases have not been reported yet. Sanitary authorities may need to undertake mass screening if the risk is high.5959 A. Farrugia, T.R. Kreil. Reflections on the emergence of chikungunya virus in the United States: time to revisit a successful paradigm for the safety of blood-derived therapies. Transfusion. 2015; 55:224p
The OX513A strain of A. aegypti is composed by radiation sterilized male insects. A study of the release of these agents in a suburb of Juazeiro, Bahia, Brazil demonstrated a reduction of 95% of the local A. aegypti population in one year. The Sterile Insect Technique (SIT) is a genetic control system that seems promising as a mean of vector control.6060 D.O. Carvalho, A.R. McKemey, L. Garziera. Suppression of a field population of Aedes aegypti in Brazil by sustained release of transgenic male mosquitoes. PLoS Negl Trop Dis. 2015; 9:e0003864p Its use, among public controversy, has been imitated in Key West, the most southern region of the United States.
There is no vaccine currently available to prevent CHIKV infection. An ideal vaccine, should be of low cost, highly stable (as it will be predominantly administered in developing countries), administered in a single injection and able to stimulate rapid protection.
There are many vaccine candidates that have been tested in mouse models, one of the most intriguing ones is a non-adjuvanted, inactivated whole virus CHIKV vaccine applied by dermal application using a delivery system called Foroderm. Foroderm consists of elongated microparticles to which the whole virus is attached. Topical application in mice is followed by circulation of the particles into the lymphatic system (verified by fluorescence). A single application protected mice against viremia and disease following a virus challenge.6161 P.A. Rudd, A.P. Raphael, M. Yamada. Effective cutaneous vaccination using an inactivated chikungunya virus vaccine delivered by Foroderm. Vaccine. 2015; 33:5172p
In the last 2 years two vaccines have been tested in Phase 1 trials in humans: a live recombinant measles-virus-based chikungunya vaccine and a virus-like particle chikungunya virus vaccine (VRC-CHKVLP059-00-VP). Both of them were immunogenic, safe and well tolerated.6262 K. Ramsauer, M. Schwameis, C. Firbas. Immunogenicity, safety, and tolerability of a recombinant measles-virus-based chikungunya vaccine: a randomised, double-blind, placebo-controlled, active-comparator, first-in-man trial. Lancet Infect Dis. 2015; 15:519p 6363 L.J. Chang, K.A. Dowd, F.H. Mendoza. Safety and tolerability of chikungunya virus-like particle vaccine in healthy adults: a phase 1 dose-escalation trial. Lancet. 2014; 384:2046p More advanced phase II/III trials are hampered by the sporadic nature of the infection, which makes planning and approval of clinical trials quiet challenging.
A single vaccine has been tested in phase II trials. This was a serially passaged, plaque-purified live Chikungunya vaccine produced by the United States Army Medical Research Institute for Infectious Diseases (USAMRIID). The vaccine was injected subcutaneously and compared in a double-blinded randomized study with placebo. Ninety eight percent of recipients developed neutralizing antibodies (which persisted in 50% of cases for more than a year). The vaccine was safe and the only difference with placebo was more frequent arthalgia.6464 R. Edelman, C.O. Tacket, S.S. Wasserman, S.A. Bodison, J.G. Perry, J.A. Mangiafico. Phase II safety and immunogenicity study of live chikungunya virus vaccine TSI-GSD-218. Am J Trop Med Hyg. 2000; 62:681p Despite the promising results further clinical development was aborted in 2000 due to the lack of commercial interest.
Conflicts of interest
The authors declare no conflicts of interest.
References
-
1A.H. Khan, K. Morita, C. Parquet Md Mdel, F. Hasebe, E.G. Mathenge, A. Igarashi. Complete nucleotide sequence of chikungunya virus and evidence for an internal polyadenylation site. J Gen Virol. 2002; 83:3075p
-
2F. Simon, H. Savini, P. Parola. Chikungunya: a paradigm of emergence and globalization of vector-borne diseases. Med Clin North Am. 2008; 92:1323p
-
3A.M. Powers, A.C. Brault, R.B. Tesh, S.C. Weaver. Re-emergence of Chikungunya and O’nyong-nyong viruses: evidence for distinct geographical lineages and distant evolutionary relationships. J Gen Virol. 2000; 81:471p
-
4J.H. Strauss, E.G. Strauss. The alphaviruses: gene expression, replication, and evolution. Microbiol Rev. 1994; 58:491p
-
5M. Diallo, J. Thonnon, M. Traore-Lamizana, D. Fontenille. Vectors of Chikungunya virus in Senegal: current data and transmission cycles. Am J Trop Med Hyg. 1999; 60:281p
-
6C. Chevillon, L. Briant, F. Renaud, C. Devaux. The Chikungunya threat: an ecological and evolutionary perspective. Trends Microbiol. 2008; 16:80p
-
7R.G. Carvalho, R. Lourenço-de-Oliveira, I.A. Braga. Updating the geographical distribution and frequency of Aedes albopictus in Brazil with remarks regarding its range in the Americas. Mem Inst Oswaldo Cruz. 2014; 109:787p
-
8F.A. Monteiro, R. Schama, A.J. Martins, A. Gloria-Soria, J.E. Brown, J.R. Powell. Genetic diversity of Brazilian Aedes aegypti: patterns following an eradication program. PLoS Negl Trop Dis. 2014; 8:e3167p
-
9M.R. Nunes, N.R. Faria, J.M. de Vasconcelos. Emergence and potential for spread of chikungunya virus in Brazil. BMC Med. 2015; 13:102p
-
10J.P. Harper, S.L. Paulson. Reproductive isolation between Florida strains of Aedes aegypti and Aedes albopictus. J Am Mosq Control Assoc. 1994; 10:88p
-
11I. Schuffenecker, I. Iteman, A. Michault. Genome microevolution of chikungunya viruses causing the Indian Ocean outbreak. PLoS Med. 2006; 3:e263p
-
12M. Sourisseau, C. Schilte, N. Casartelli. Characterization of reemerging chikungunya virus. PLoS Pathog. 2007; 3:e89p
-
13Z. Her, B. Malleret, M. Chan. Active infection of human blood monocytes by Chikungunya virus triggers an innate immune response. J Immunol. 2010; 184:5903p
-
14O. Schwartz, M.L. Albert. Biology and pathogenesis of chikungunya virus. Nat Rev Microbiol. 2010; 8:491p
-
15N. Wauquier, P. Becquart, D. Nkoghe, C. Padilla, A. Ndjoyi-Mbiguino, E.M. Leroy. The acute phase of Chikungunya virus infection in humans is associated with strong innate immunity and T CD8 cell activation. J Infect Dis. 2011; 204:115p
-
16A. Chow, Z. Her, E.K. Ong. Persistent arthralgia induced by Chikungunya virus infection is associated with interleukin-6 and granulocyte macrophage colony-stimulating factor. J Infect Dis. 2011; 203:149p
-
17A. Mohan, D.H. Kiran, I.C. Manohar, D.P. Kumar. Epidemiology, clinical manifestations, and diagnosis of Chikungunya fever: lessons learned from the re-emerging epidemic. Indian J Dermatol. 2010; 55:54p
-
18D. Bandyopadhyay, S.K. Ghosh. Mucocutaneous features of Chikungunya fever: a study from an outbreak in West Bengal, India. Int J Dermatol. 2008; 47:1148p
-
19Rampal, M. Sharda, H. Meena. Neurological complications in Chikungunya fever. J Assoc Physicians India. 2007; 55:765p
-
20P. Mahendradas, K. Avadhani, R. Shetty. Chikungunya and the eye: a review. J Ophthalmic Inflamm Infect. 2013; 3:35p
-
21J.K. Sarkar, S.N. Chatterjee, S.K. Chakravarti, A.C. Mitra. Chikungunya virus infection with haemorrhagic manifestations. Indian J Med Res. 1965; 53:921p
-
22X. Fritel, O. Rollot, P. Gerardin. Chikungunya virus infection during pregnancy, Reunion, France, 2006. Emerg Infect Dis. 2010; 16:418p
-
23D. Ramful, S. Sampériz, X. Fritel. Antibody kinetics in infants exposed to Chikungunya virus infection during pregnancy reveals absence of congenital infection. J Infect Dis. 2014; 209:1726p
-
24P. Gérardin, G. Barau, A. Michault. Multidisciplinary prospective study of mother-to-child chikungunya virus infections on the island of La Réunion. PLoS Med. 2008; 5:e60p
-
25A. Chopra, V. Anuradha, V. Lagoo-Joshi, V. Kunjir, S. Salvi, M. Saluja. Chikungunya virus aches and pains: an emerging challenge. Arthritis Rheum. 2008; 58:2921p
-
26F. Simon, E. Javelle, M. Oliver, I. Leparc-Goffart, C. Marimoutou. Chikungunya virus infection. Curr Infect Dis Rep. 2011; 13:218p
-
27G. Borgherini, P. Poubeau, A. Jossaume. Persistent arthralgia associated with chikungunya virus: a study of 88 adult patients on reunion island. Clin Infect Dis. 2008; 47:469p
-
28S.D. Thiberville, V. Boisson, J. Gaudart, F. Simon, A. Flahault, X. de Lamballerie. Chikungunya fever: a clinical and virological investigation of outpatients on Reunion Island, South-West Indian Ocean. PLoS Negl Trop Dis. 2013; 7:e2004p
-
29C. Schilte, F. Staikowsky, T. Couderc. Chikungunya virus-associated long-term arthralgia: a 36-month prospective longitudinal study. PLoS Negl Trop Dis. 2013; 7:e2137p
-
30P. Gérardin, A. Fianu, A. Michault. Predictors of Chikungunya rheumatism: a prognostic survey ancillary to the TELECHIK cohort study. Arthritis Res Ther. 2013; 15:R9p
-
31J.J. Hoarau, M.C. Jaffar Bandjee, P. Krejbich Trotot. Persistent chronic inflammation and infection by Chikungunya arthritogenic alphavirus in spite of a robust host immune response. J Immunol. 2010; 184:5914p
-
32D. Mavalankar, P. Shastri, T. Bandyopadhyay, J. Parmar, K.V. Ramani. Increased mortality rate associated with chikungunya epidemic, Ahmedabad, India. Emerg Infect Dis. 2008; 14:412p
-
33M.C. Robinson. An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952–53. I. Clinical features. Trans R Soc Trop Med Hyg. 1955; 49:28p
-
34C. Bhagwati, M. Madhulika, K.D. Mehta, Y.S. Goswami. Profile of the chikungunya infection: a neglected vector borne disease which is prevalent in The Rajkot District. J Clin Diagn Res. 2013; 7:1008p
-
35M.M. Thiboutot, S. Kannan, O.U. Kawalekar. Chikungunya: a potentially emerging epidemic?. PLoS Negl Trop Dis. 2010; 4:e623p
-
36G. Rezza, L. Nicoletti, R. Angelini. Infection with chikungunya virus in Italy: an outbreak in a temperate region. Lancet. 2007; 370:1840p
-
37M. Fischer, J.E. Staples. Notes from the field: chikungunya virus spreads in the Americas – Caribbean and South America, 2013–2014. MMWR Morb Mortal Wkly Rep. 2014; 63:500p
-
38D. Ruiz-Moreno, I.S. Vargas, K.E. Olson, L.C. Harrington. Modeling dynamic introduction of Chikungunya virus in the United States. PLoS Negl Trop Dis. 2012; 6:e1918p
-
39B.M. Kuehn. Chikungunya virus transmission found in the United States: US health authorities brace for wider spread. JAMA. 2014; 312:776p
-
40C.G. Moore, C.J. Mitchell. Aedes albopictus in the United States: ten-year presence and public health implications. Emerg Infect Dis. 1997; 3:329p
-
41K.A. Tsetsarkin, D.L. Vanlandingham, C.E. McGee, S. Higgs. A single mutation in Chikungunya virus affects vector specificity and epidemic potential. PLoS Pathog. 2007; 3:e201p
-
42M. Dash, I. Mohanty, S. Padhi. Laboratory diagnosis of chikungunya virus: do we really need it?. Indian J Med Sci. 2011; 65:83p
-
43A.M. Powers. Chikungunya. Clin Lab Med. 2010; 30:209p
-
44M. Panning, K. Grywna, M. van Esbroeck, P. Emmerich, C. Drosten. Chikungunya fever in travelers returning to Europe from the Indian Ocean region, 2008. Emerg Infect Dis. 2006; 14:416p
-
45B. Pastorino, M. Bessaud, M. Grandadam, S. Murri, H.J. Tolou, C.N. Peyrefitte. Development of a TaqMan RT-PCR assay without RNA extraction step for the detection and quantification of African Chikungunya viruses. J Virol Methods. 2005; 124:65p
-
46F. Burt, W. Chen, S. Mahalingam. Chikungunya virus and arthritic disease. Lancet Infect Dis. 2014; 14:789p
-
47M.N. Pyndiah, V. Pursem, G. Meetoo. Chikungunya virus isolation using simplified cell culture technique in Mauritius. Med Trop (Mars). 2012; 72:
-
48World Health Organization. Guidelines on clinical management of Chikungunya fever. Available here: http://www.wpro.who.int/mvp/topics/ntd/Clinical_Mgnt_Chikungunya_WHO_SEARO.pdf [accessed 10.12.15].
» http://www.wpro.who.int/mvp/topics/ntd/Clinical_Mgnt_Chikungunya_WHO_SEARO.pdf -
49W. Taubitz, J.P. Cramer, A. Kapaun. Chikungunya fever in travelers: clinical presentation and course. Clin Infect Dis. 2007; 45:e1p
-
50R. Ravichandran, M. Manian. Ribavirin therapy for Chikungunya arthritis. J Infect Dev Ctries. 2008; 2:140p
-
51S.W. Brighton. Chloroquine phosphate treatment of chronic Chikungunya arthritis. An open pilot study. S Afr Med J. 1984; 66:217p
-
52X. De Lamballerie, V. Boisson, J.C. Reynier. On chikungunya acute infection and chloroquine treatment. Vector Borne Zoonotic Dis. 2008; 8:837p
-
53P. Kaur, J.J. Chu. Chikungunya virus: an update on antiviral development and challenges. Drug Discov Today. 2013; 18:969p
-
54D. Parashar, M.S. Paingankar, S. Kumar. Administration of E2 and NS1 siRNAs inhibit chikungunya virus replication in vitro and protects mice infected with the virus. PLoS Negl Trop Dis. 2013; 7:e2405p
-
55T. Couderc, N. Khandoudi, M. Grandadam. Prophylaxis and therapy for Chikungunya virus infection. J Infect Dis. 2009; 200:516p
-
56P. Pal, K.A. Dowd, J.D. Brien. Development of a highly protective combination monoclonal antibody therapy against Chikungunya virus. PLoS Pathog. 2013; 9:e1003312p
-
57E. Bouquillard, B. Combe. A report of 21 cases of rheumatoid arthritis following Chikungunya fever. A mean follow-up of two years. Joint Bone Spine. 2009; 76:654p
-
58Centers for Disease Control and Prevention. Chikungunya virus – prevention. Available here: http://www.cdc.gov/chikungunya/prevention/
» http://www.cdc.gov/chikungunya/prevention/ -
59A. Farrugia, T.R. Kreil. Reflections on the emergence of chikungunya virus in the United States: time to revisit a successful paradigm for the safety of blood-derived therapies. Transfusion. 2015; 55:224p
-
60D.O. Carvalho, A.R. McKemey, L. Garziera. Suppression of a field population of Aedes aegypti in Brazil by sustained release of transgenic male mosquitoes. PLoS Negl Trop Dis. 2015; 9:e0003864p
-
61P.A. Rudd, A.P. Raphael, M. Yamada. Effective cutaneous vaccination using an inactivated chikungunya virus vaccine delivered by Foroderm. Vaccine. 2015; 33:5172p
-
62K. Ramsauer, M. Schwameis, C. Firbas. Immunogenicity, safety, and tolerability of a recombinant measles-virus-based chikungunya vaccine: a randomised, double-blind, placebo-controlled, active-comparator, first-in-man trial. Lancet Infect Dis. 2015; 15:519p
-
63L.J. Chang, K.A. Dowd, F.H. Mendoza. Safety and tolerability of chikungunya virus-like particle vaccine in healthy adults: a phase 1 dose-escalation trial. Lancet. 2014; 384:2046p
-
64R. Edelman, C.O. Tacket, S.S. Wasserman, S.A. Bodison, J.G. Perry, J.A. Mangiafico. Phase II safety and immunogenicity study of live chikungunya virus vaccine TSI-GSD-218. Am J Trop Med Hyg. 2000; 62:681p
Publication Dates
-
Publication in this collection
Jan-Feb 2016
History
-
Received
09 Sept 2015 -
Accepted
16 Oct 2015