ABSTRACT
The increasing rates of nosocomial infection associated with coagulase-negative staphylococci (CoNS) were the rationale for this study, aiming to categorize oxacillin-resistant CoNS species recovered from blood culture specimens of inpatients at the UNESP Hospital das Clínicas in Botucatu, Brazil, over a 20-year period, and determine their sensitivity to other antimicrobial agents. The mecA gene was detected in 222 (74%) CoNS samples, and the four types of staphylococcal chromosomal cassette mec (SCCmec) were characterized in 19.4%, 3.6%, 54.5%, and 14.4% of specimens, respectively, for types I, II, III, and IV. Minimal inhibitory concentration (MIC) values to inhibit 50% (MIC50) and 90% (MIC90) of specimens were, respectively, 2 and >256 µL/mL for oxacillin, 1.5 and 2 µL/mL for vancomycin, 0.25 and 0.5 µL/mL for linezolid, 0.094 and 0.19 µL/mL for daptomycin, 0.19 and 0.5 µL/mL for quinupristin/dalfopristin, and 0.125 and 0.38 µL/mL for tigecycline. Resistance to oxacillin and tigecycline and intermediate resistance to quinupristin/dalfopristin were observed. Eight (2.7%) of all 300 CoNS specimens studied showed reduced susceptibility to vancomycin. Results from this study show high resistance rates of CoNS to antimicrobial agents, reflecting the necessity of using these drugs judiciously and controlling nosocomial dissemination of these pathogens.
Keywords:
CoNS; MIC; Quinupristin/dalfopristin; SCCmec; Vancomycin; Tigecycline; Staphylococcus
Introduction
Coagulase-negative staphylococci (CoNS), members of the staphylococci group, are characterized as Gram-positive cocci, presented as single cells or with irregular disposition, and are immobile, non-spore forming, catalase-positive, mostly facultative anaerobes, and lack the enzyme coagulase.11 Garrity GM, Labeda DP, Oren A. Judicial Commission of the International Committee on Systematics of Prokaryotes * XIIth International (IUMS) Congress of Bacteriology and Applied Microbiology: minutes of the meetings, 3, 4 and 6 August 2008, Istanbul, Turkey. Int J Syst Evol Microbiol. 2011;61:2775-80. CoNS are part of the human microbiota, considered opportunistic pathogens, causing infections mostly in premature babies, and immunocompromised and prosthetic patients.22 Rocchetti TT, Martins KB, Martins PYF, et al. Detection of the mecA gene and identification of Staphylococcus directly from blood culture bottles by multiplex polymerase chain reaction. Brazilian J Infect Dis. 2018;22:99-105.
The rise of antimicrobial resistance in recent years has had a great impact on hospital infections caused by CoNS. Oxacillin is a semisynthetic penicillin used in the susceptibility test for the detection of methicillin resistance and treatment of staphylococcal infections. However, rates from 66% to 95% of oxacillin resistance have been observed in CoNS clinical isolates.22 Rocchetti TT, Martins KB, Martins PYF, et al. Detection of the mecA gene and identification of Staphylococcus directly from blood culture bottles by multiplex polymerase chain reaction. Brazilian J Infect Dis. 2018;22:99-105. Oxacillin resistance is often mediated by the mecA gene, which encodes a supplemental penicillin-binding protein (PBP2a) with low-affinity to semisynthetic penicillins.33 Archer GL, Niemeyer DM. Origin and evolution of DNA associated with resistance to methicillin in staphylococci. Trends Microbiol. 1994;2:343-7. The mecA gene is located on a mobile genetic element known as the Staphylococcal Cassette Chromosome mec (SCCmec) which contains the mec complex, composed of the mecA gene and its regulator genes mecI and mecRI, the ccr complex, responsible for integration and excision of the SCCmec, and J region, which is not essential for the SCCmec formation, but may carry non-β-lactam resistance genes.44 Ito T, Katayama Y, Asada K, Mori N, Tsutsumimoto K. Structural comparison of three types of staphylococcal cassette chromosome mec integrated in the chromosome in methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. 2001;45:1323-36. To date, 13 SCCmec types have been described, based on the combination of ccr gene complex types and mec gene complex classes. The subtypes were defined by J region polymorphisms in the same combination of mec and ccr complexes.55 Wu Z, Li F, Liu D, Xue H, Zhao X. Novel type XII staphylococcal cassette chromosome mec harboring a new cassette chromosome recombinase, CcrC2. Antimicrob Agents Chemother. 2015;59:7597-601.
The emergence of oxacillin resistant isolates has led to the ultimate use of alternative antimicrobials for treatment of CoNS infections, such as the glycopeptide vancomycin. In the meantime, descriptions of reduced susceptibility and resistance to vancomycin have been reported in recent decades.66 Palazzo ICV, Araujo MLC, Darinia LC. First report of vancomycin-resistant staphylococci isolated from healthy carriers in Brazil. J Clin Microbiol. 2005;43:179-85. Reduced susceptibility to vancomycin may be related to metabolic modifications such as acceleration in peptidoglycan synthesis, resulting in cell wall thickening. In this process, vancomycin is not able to inhibit the peptidoglycan synthesis, since it is depleted due to the higher availability of D-alanyl-D-alanine sites.77 Appelbaum PC. The emergence of vancomycin-intermediate and vancomycin-resistant Staphylococcus aureus; 2006. p. 256.
Given the upsurge in hospital infections caused by CoNS, this study aimed to characterize the oxacillin resistant strains and determine the antimicrobial susceptibility of a 20-year collection of blood culture CoNS isolates from Botucatu Hospital das Clínicas inpatients.
Material and methods
Strains
Three-hundred CoNS strains were isolated from blood cultures from inpatients of the Botucatu Hospital das Clínicas - Paulista State University (UNESP). The isolates were collected from 1990 to 2009 and kept in the Culture Collection Laboratory of the Microbiology and Immunology Department of the Botucatu Biosciences Institute - UNESP. The selection criteria considered a mean prevalence of events of 35%, with a margin of error of 5%, and a 95% confidence interval.
The strains were isolated according to Koneman et al.88 Koneman EW, Allen SD, Janda WM, Schreckenberger PC. W C W. Color Atlas and Textbook of Diagnostic Microbiology. 5th ed. Philadelphia: Lippincott; 1997. Blood-agar isolates were subjected to Gram stain for observation of colony morphology and the catalase test was performed for confirmation of the genus Staphylococcus. Staphylococcal strains were submitted to the coagulase test for differentiation of the coagulase-negative and coagulase-positive groups. Coagulase-negative isolates were subjected to biochemical tests for the phenotypic identification of species. The genotypic identification was performed using primers drawn over conserved sequences adjacent to 16S and 23S genes, by ITS-PCR (internal transcribed spacer-polymerase chain reaction), described by Couto et al.99 Couto I, Pereira S, Miragaia M, Santos Sanches I, De Lencastre H. Identification of clinical staphylococcal isolates from humans by internal transcribed spacer PCR. J Clin Microbiol. 2001;39:3099-103. Amplification efficiency was monitored by electrophoresis in 3% metaphor agarose and stained with SYBR Safe. The following lineages of international reference were used: S. auricularis ATCC 33753, S. capitis subsp. capitis ATCC 27843, S. capitis subsp. urealyticus ATCC 49325, S. caprae ATCC 35538, S. cohnii ATCC 49330, S. cohnii subsp. cohnii ATCC 29974, S. epidermidis ATCC 12228, S. epidermidis ATCC 35983, S. hemolyticus ATCC 29970, S. hominis ATCC 27844, S. hominis subsp. novobiosepticus ATCC 700237, S. lentus ATCC 700403, S. lugdunensis ATCC 700328, S. saprophyticus ATCC 15305, S. schleiferi subsp. schleiferi ATCC 43808, S. sciuri subsp. sciuri ATCC 29062, S. simulans ATCC 27851, S. xylosus ATCC 29979, and S. warneri ATCC 10209.
DNA extraction
The Illustra kit (GE Healthcare) was used for DNA extraction. The steps included an initial digestion of staphylococcal cells with lysozyme (10 mg/mL) and proteinase K (20 mg/mL). Next, 500 µL of the extraction buffer were added to the mixture, which was centrifuged at 10,000 x g for 4 min. The supernatant was transferred to a column and centrifuged at 5,000g for 1 min. The fluid was discarded and 500 µL of extraction buffer were added to the column. After the centrifugation and discarding of the collected fluid, 500 µL of washing buffer were added to the column, which was submitted to centrifugation at 20,000g for 3 min. Next the column was transferred to a 1.5 mL tube and elution was performed using 200 µL of warmed MilliQ water at 70 °C.
The mecA gene detection
PCR was performed for the detection of the mecA gene. Reactions were performed using a protocol described by Murakami et al.1010 Murakami K, Minamide W, Wada K, Nakamura E, Teraoka H, Watanabe S. Identification of methicillin-resistant strains of staphylococci by polymerase chain reaction. J Clin Microbiol. 1991;29:2240-4. Doi: 1939577. The amplification efficiency was monitored by electrophoresis in a 2% agarose gel stained with SYBR Safe.
Determination of SCCmec
The SCCmec type was determined on mecA-positive strains. Reactions were performed using a protocol described by Oliveira et al.1111 Oliveira DC. Multiplex PCR Strategy for Rapid Identification of Structural Types and Variants of the Society. Antimicrob Agents Chemother. 2002;46:2155-61. and modified by Machado et al.1212 Machado ABMP, Reiter KC, Paiva RM, Barth AL. Distribution of staphylococcal cassette chromosome mec (SCCmec) types I, II, III and IV in coagulase-negative staphylococci from patients attending a tertiary hospital in southern Brazil. J Med Microbiol. 2007;56:1328-33.
Multiplex PCR was performed in 50 µL of reaction volume with 1X enzyme buffer, 1.25 U Taq polymerase DNA, 200 µM dNTP Mix, and the following primers: 10 pmol of RIF2 F2 (TTCGAGTTGCTGATGAAGAAGG) and CIF2 R2 (ATTTACCACAAGGACTACCAGC), 6 pmol of KDP F1 (AATCATCTGCCATTGGTGATGC) and KDP R1 (CGAATGAAGTGAAAGAAAGTGG), 5 pmol of DCS F2 (CATCCTATGATAGCTTGGTC) and DSC R1 (CTAAATCATAGCCATGACCG), 5 pmol of RIF4 F3 (GTGATTGTTCGAGATATGTGG), and RIF4 R9 (CGCTTTATCTGTATCTATCGC). For each reaction, 10 µL DNA was added. The cycle sequencing reactions were performed at 92 °C for 3 min, followed by 30 cycles of 92 °C for 1 min, 56 °C for 1 min, and 72 °C for 1 min and 30 s. The amplification efficiency was monitored by electrophoresis in a 2% agarose gel stained with SYBR Safe.
Determination of the minimal inhibitory concentration (MIC) by the E-test
The in vitro susceptibility of CoNS strains was tested for the following antimicrobials: Oxacillin, Vancomycin, Daptomycin, Linezolid, Quinupristin/Dalfopristin, and Tigecycline. The MIC of these drugs was determined by the E-test. The criteria used for the susceptibility classification were: Oxacillin <0.5 µg/mL (susceptible) for CoNS, except S. lugdunensis (susceptible ≤2 µg/mL and resistant ≥4 µg/mL); Vancomycin <4 µg/mL (susceptible), 8-16 µg/mL (intermediate resistant), and >32 µg/mL (resistant); Linezolid ≤4 µg/mL (susceptible); Daptomycin ≤1 µg/mL; Quinupristin/Dalfopristin ≤1 µg/mL (susceptible), 2 µg/mL (intermediate), and ≥4 µg/mL (resistant); Tigecycline ≤0.5 µg/mL.1313 (CLSI) Clinical and Laboratory Standards. Performance standards for antimicrobial susceptibility testing, document M100-S23. 2016.
Screening test for the detection of reduced susceptibility to vancomycin
In order to detect reduced susceptibility to vancomycin, a screening agar test prepared with Brain Heart Infusion (BHI) Agar and 4 µg/mL, 6 µg/mL, 8 µg/mL, and 16 µg/mL of vancomycin was used. The reference strain S. aureus ATCC 29213, susceptible to vancomycin, was used as a negative control, and strain E. faecalis ATCC 51299, resistant to vancomycin, as a positive control. Spots of a 2.0 McFarland inoculum were added to the Agar plate and incubated at 35 °C for 24 h, and the growing of at least one colony was considered as a positive result.
Analysis of the cell wall thickness
The CoNS strains that presented reduced susceptibility to vancomycin were submitted to the transmission electronic microscopy for cell wall thickness analysis. Strains were cultured in BHI broth and incubated at 37° C for 24 h. In a microtube, 1000 µL of a CoNS culture broth were centrifuged for one minute at 12,000 rpm. After discarding the supernatant, strains were fixed in a Karnovsky solution (2.5% glutaraldehyde in phosphate buffer 0.1 M [pH 7.3]) for four hours. Samples were removed from the fixer and washed three times for five minutes in distilled water. Next the samples were immersed in 0.5% osmium tetroxide for 40 min, before being washed three times for 10 min in distilled water. Samples were dehydrated using increasing concentrations of alcohol: two times for 10 min in 7.5% alcohol; two times for 10 min in 15% alcohol; two times for 10 min in 30% alcohol; two times for 10 min in 50% alcohol; three times for 15 min in 70% alcohol; two times for 15 min in 90% alcohol; two times for 10 min in 100% alcohol. After the dehydration the stubs were mounted and samples metalized. The analyses were performed in an electronic microscopy Tecnai Spirit Fei Company and the images were obtained at a magnification of 30000×.
Results
Identification of isolates
The identification of CoNS through the biochemical tests detected 223 (74.3%) S. epidermidis, 27 (9.0%) S. hemolyticus, 22 (7.3%) S. hominis, 14 (4.7%) S. warneri, 9 (3.0%) S. lugdunensis, and 5 (1.7%) S. capitis. Through the ITS-PCR method, 223 (74.3%) S. epidermidis, 29 (9.7%) S. hemolyticus, 23 (7.7%) S. hominis, 11 (3.7%) S. warneri, 9 (3.0%) S. lugdunensis, and 5 (1.7%) S. capitis were detected. Agreement between the identification methods was found in 98% of cases.
Table 1 presents the source of the CoNS species isolates, as well as the demographic data of the patients with bacteremia.
Origin of CoNS isolates and demographic data of patients with bacteremia at Hospital das Clínicas de Botucatu - Paulista State University between 1990 and 2009.
Detection of mecA gene and characterization of SCCmec
The mecA gene was detected in 222 (74%) of the studied samples, found in 78.5% of S. epidermidis, 75.9% of S. hemolyticus, 69.6% of S. hominis, 27.3% of S. warneri, 80% of S. capitis, and 22.2% of S. lugdunensis.
The characterization of SCCmec in mecA-positive strains was as follows: 43 (19.4%) were classified as type I, 8 (3.6%) as type II, 121 (54.5%) as type III, 32 (14.4%) as type IV, and 18 (8.1%) were not typed by this method. The correlations between the SCCmec types and methicillin-resistant CoNS species are presented in Table 2.
Determination of the minimal inhibitory concentration (MIC)
The MICs of the antimicrobials used for the treatment of CoNS infections was determined by the E-test. Oxacillin resistance was found in 206 (68.7%) CoNS strains and 25 were tigecycline resistant (8.3%). Resistance to tigecycline was detected in 4.5% of S. epidermidis, 13.8% of S. hemolyticus, 13% of S. hominis, and 11.1% of S. lugdunensis. For quinupristin/dalfopristin, one S. epidermidis isolate presented intermediate resistance with an MIC of 2 µg/mL, and one S. epidermidis and one S. hemolyticus with MICs of 3 µg/mL. The sensitivity and specificity of the oxacillin MIC by the E-test compared with the presence of mecA were, respectively, 87.4% and 82.3%.
The antimicrobial MICs for inhibition of 50% and 90% of strains (MIC50 and MIC90) were, respectively, 2 µL/mL and >256 µL/mL for oxacillin, 1.5 µL/mL and 2 µL/mL for vancomycin, 0.25 µL/mL and 0.5 µL/mL for linezolid, 0.094 µL/mL and 0.19 µL/mL for daptomycin, 0.19 µL/mL and 0.5 µL/mL for quinupristin/dalfopristin, and 0.125 µL/mL and 0.38 µL/mL for tigecycline.
With respect to CoNS species, the parameter distribution of MIC50 and MIC90 revealed high rates of oxacillin resistance in S. hemolyticus. This was the only CoNS species for which the minimal concentration to inhibit 50% of isolates was >256 µg/mL, reflecting the high resistance rate of S. hemolyticus to oxacillin (Table 3).
Determination of MIC50, MIC90, MIC range (µg/ml), and antimicrobial resistance in CoNS species.
The MIC range of each antimicrobial was compared to the SCCmec type. The isolates typed as SCCmecI presented higher tigecycline MICs and those classified as SCCmecII presented the highest oxacillin MICs. The SCCmecIV strains showed the highest MIC values for vancomycin, linezolid, daptomycin, and quinupristin/dalfopristin (Table 4).
An evaluation was performed of the oxacillin and vancomycin MICs over a period of 20 years, divided into three time periods according to the distribution of oxacillin and vancomycin MIC ranges. For oxacillin, in the first period (1990-2001), higher values of MIC were observed, but still indicating susceptibility. In the other periods (2002-2006 and 2007-2009), a decrease in the MIC values was observed, still indicating susceptibility, as well as an increase in the resistance rates. Regarding vancomycin, the same evaluation demonstrated significant differences in the three periods among strains with MICs from 0.047 µg/mL to 0.38 µg/mL and from 0.5 µg/mL to 2.0 µg/mL (Fig. 1).
Correlation between the number of CoNS and oxacillin and vancomycin MICs in the three periods: 1990-2001; 2002-2006; 2007-2009.
Determination of the reduced susceptibility to vancomycin
A growth of 214 (71.3%) strains was observed on the BHI plate with 4 µg/mL of vancomycin, 89 (29.7%) on the plate with 6 µg/mL of vancomycin, and 8 (2.6%) isolates on the 8 µg/mL vancomycin plate. None of the isolates grew in the medium with 16 µg/mL of vancomycin. There were no significant differences in MICs between strains that presented no growth on the plate complemented with vancomycin and those which grew on the 4 µg/mL vancomycin plate. Among those that showed growth on the medium with 6 µg/mL of vancomycin, the MIC range was 0.5-2 µg/mL. Among those which grew on 8 µg/mL of vancomycin, the MIC range was 0.75-24 µg/mL. The strains grown on 8 µg/mL of vancomycin were four S. epidermidis, one S. hemolyticus, two S. hominis, and one S. capitis, all resistant to oxacillin, and S. epidermidis and S. capitis being carriers of SCCmec III, S. hominis of SCCmec I, and S. hemolyticus with non-typed SCCmec.
Analysis of the cell wall thickness of strains with reduced susceptibility to vancomycin
The cell wall thickness under cell division was measured in eight strains (values are presented in nanometers, mean ± SD). The four S. epidermidis strains presented mean values of 21.66 ± 1.4, 20.12 ± 0.9, 24.24 ± 1.3, and 14.20 ± 1.3 nm. The S. hemolyticus isolate showed a cell wall thickness of 24.88 ± 1.7 nm. For the S. capitis isolate, the cell wall thickness was 19.33 ± 1.8, and for the two S. hominis isolates the values were 17.68 ± 2.1 and 24.92 ± 1.5. For comparison, the used reference strains S. epidermidis ATCC 12228 and S. hemolyticus ATCC29970 showed cell wall thicknesses of, respectively, 14.61 ± 1.2 and 14.73 ± 0.7 nm. The comparison of the studied strains against controls showed higher values, ranging from 17 nm to 24.92 nm, with the exception of one S. epidermidis isolate, which presented a lower value compared to the controls (Fig. 2).
Transmission Electronic Microscopy images of CoNS under division, for observation of cell wall thickness (in nanometers).a) S. hominis b) S. epidermidis ATCC 12228.
CoNS bacteremia evolution
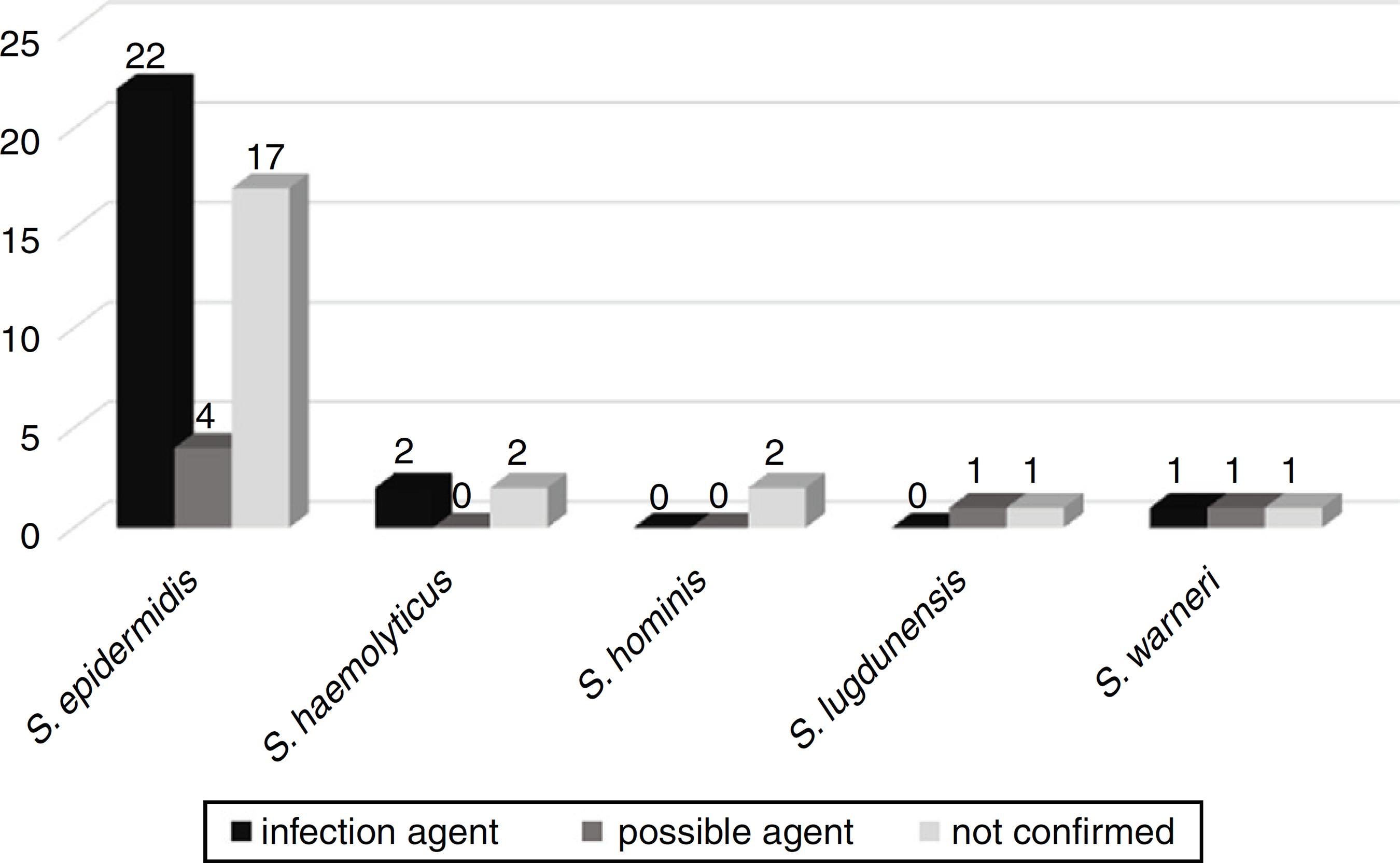
The possible evolution of bacteremia to other infections, such as sepsis, pneumonia, urinary tract infection, meningitis, peritonitis, necrotizing enterocolitis, omphalitis, and brain abscess, was followed up in 52 patients admitted to the neonatal wards. Of these, in 25 (46.3%) patients the same CoNS isolated from blood culture was confirmed to be the etiologic agent of infection. In six (11.1%), CoNS was the possible agent of infection, and in 23 (42.6%) CoNS was not related to the patient's infection (Fig. 3).
Correlation of CoNS isolated from blood cultures as possible etiological agents of infections caused in neonatal unit patients.
The mecA gene was detected in 33 (61.1%) of these CoNS, with 20 (60.6%) CoNS associated with more severe infections or possible agents of these infections.
Discussion
The CoNS are considered one of the main causes of bacteremia. The importance of these bacteria has increased in the hospital environment during recent years, mostly due to antimicrobial resistance. In the present work, 300 CoNS strains isolated from blood cultures of inpatients at the Hospital of Clinics of Botucatu, over a period of 20 years, were studied. These isolates were characterized regarding their antimicrobial susceptibility.
The mecA detection determined oxacillin resistance in 78.5% of CoNS, and the MIC50 value (2 µg/mL) was indicative of resistance to this drug, confirming the low susceptibility of these bacteria to β-lactam agents. Previous works have demonstrated that since the 1970s the CoNS isolates have presented higher oxacillin resistance rates than S. aureus.1414 John JF, Harvin AM. History and evolution of antibiotic resistance in coagulase-negative staphylococci: susceptibility profiles of new anti-staphylococcal agents. Ther Clin Risk Manag. 2007;3:1143-52.,1515 Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clin Microbiol Rev. 2014;27:870-926. The β-lactam resistance rates have been shown to range from 65% to 95% in hospitals in Brazil and in other countries.22 Rocchetti TT, Martins KB, Martins PYF, et al. Detection of the mecA gene and identification of Staphylococcus directly from blood culture bottles by multiplex polymerase chain reaction. Brazilian J Infect Dis. 2018;22:99-105.,1616 Bouchami O, Achour W, Mekni MA, Rolo J, Ben Hassen A. Antibiotic resistance and molecular characterization of clinical isolates of methicillin-resistant coagulase-negative staphylococci isolated from bacteremic patients in oncohematology. Folia Microbiol (Praha). 2011;56:122-30.,1717 Martins A, Moraes Riboli DF, Cataneli Pereira V, et al. Molecular characterization of methicillin-resistant Staphylococcus aureus isolated from a Brazilian university hospital. Braz J Infect Dis. 2014;:3-7. The highest rates of oxacillin resistance were found in S. epidermidis, followed by S. hemolyticus, S. hominis, and S. capitis. Similar results were described in previous studies, which showed oxacillin resistance in 97% of S. epidermidis between 1999 and 2001 in a neonatal intensive care unit (NICU),1818 Krediet TG, Mascini EM, Rooij E Van, Vlooswijk J, Paauw A, Gerards LJ. Molecular epidemiology of coagulase-negative staphylococci causing sepsis in a neonatal intensive care unit over an 11-year period. J Clin Microbiol. 2004;42:992-5, http://dx.doi.org/10.1128/JCM.42.3.992.
http://dx.doi.org/10.1128/JCM.42.3.992...
in 96% of S. hemolyticus isolated in Brazil,1919 Ferreira RBR, Iorio NLP, Malvar KL, et al. Coagulase-negative staphylococci : comparison of phenotypic and genotypic oxacillin susceptibility tests and evaluation of the agar screening test by using different concentrations of oxacillin. J Clin Microbiol. 2003;41:3609-14. and in 100% of S. hominis isolated in an NICU from Spain.2020 Chaves F, García-Alvarez M, Sanz F, Alba C, Otero JR. Nosocomial spread of a Staphylococcus hominis subsp. novobiosepticus strain causing sepsis in a neonatal intensive care unit. J Clin Microbiol. 2005;43:4877-9. Regarding S. capitis, discrepant results were found in the studies conducted by Caierão et al.2121 Caierão J, Musskopf M, Superti S, Roesch E, Dias CG, d’Azevedo PA. Evaluation of phenotypic methods for methicillin resistance characterization in coagulase-negative staphylococci (CNS). J Med Microbiol. 2004;53:1195-9.
Although at a lower frequency, the mecA gene was detected in S. warneri and S. lugdunensis. S. warneri has been described with rates of 33.3% of oxacillin resistance in NICUs,2222 Giusti MDe, Pacifico L, Panero A, Boccia A, Chiesa C. Phenotypic detection of nosocomial; 1999. p. 351-8. and the first description of mecA in S. lugdunensis was in the study conducted by Kawaguchi et al.2323 Kawaguchi EW, Minamide HM, Igmi H. The taxo-nomic distribution, characteristic and susceptibil-ity against antimicrobial agents of methicillin-resistant staphylococci isolated from blood. Kansenshogaku Zasshi. 1996;70:1147-53. Despite the low resistance rates,2424 Mchardy IH, Veltman J, Hindler J, Bruxvoort K, Carvalho MM, Humphries RM. Clinical and microbiological aspects of β-lactam resistance in Staphylococcus lugdunensis. J Clin Microbiol. 2017;55:585-95. determination of antimicrobial susceptibility of S. lugdunensis is important, not only due to its clinical implications, since this species is the most aggressive of the CoNS, but also for the establishment of early treatment with adequate antimicrobials and good clinical results.2525 Tee WSN, Yen Soh S, Lin R, Loo LH. Staphylococcus lugdunensis carrying the mecA gene causes catheter-associated bloodstream infection in premature neonate. J Clin Microbiol. 2003;41:519-20.
The characterization of the SCCmec showed the presence of types I-IV in the isolates, with SCCmecIII being the most frequently detected in the studied strains, mainly in S. epidermidis, the only species that carried type IV. SCCmec type III is the largest of them all, codifies for several resistance-associated genes, and is the most commonly isolated CoNS from hospital specimens. S. epidermidis is the main colonizer of the human skin and the most commonly detected in infection sites. The selective pressure in the hospital environment leads to dissemination of SCCmec III strains, which are associated with serious infections.2626 Ito T, Katayama Y, Hiramatsu K. Cloning and nucleotide sequence determination of the entire mec DNA of pre-methicillin-resistant Staphylococcus aureus N315. Antimicrob Agents Chemother. 1999;43:1449-58. SCCmec type IV has been related with community-associated Staphylococcus spp., and was described for the first time in an S. epidermidis strain, a fact that implies its transference from S. epidermidis to S. aureus. A reduced cost transfer of SCCmec IV due to its small size would probably lead to a higher incidence of infections caused by SCCmec IV carriers.1212 Machado ABMP, Reiter KC, Paiva RM, Barth AL. Distribution of staphylococcal cassette chromosome mec (SCCmec) types I, II, III and IV in coagulase-negative staphylococci from patients attending a tertiary hospital in southern Brazil. J Med Microbiol. 2007;56:1328-33.,2727 Healy CM, Hulten KG, Palazzi DL, Campbell JR, Baker CJ. Emergence of new strains of methicillin-resistant Staphylococcus aureus in a neonatal intensive care unit. Clin Infect Dis. 2004;39:1460-6. SCCmecII presented an association with S. hemolyticus, similar to the findings of Machado et al.,1212 Machado ABMP, Reiter KC, Paiva RM, Barth AL. Distribution of staphylococcal cassette chromosome mec (SCCmec) types I, II, III and IV in coagulase-negative staphylococci from patients attending a tertiary hospital in southern Brazil. J Med Microbiol. 2007;56:1328-33. whose work only detected type II in this species.
The alternative for the treatment of oxacillin resistant staphylococci is vancomycin, a glycopeptide first used in 1958 in invasive infections. There are, however, descriptions of resistance and reduced susceptibility to this drug,66 Palazzo ICV, Araujo MLC, Darinia LC. First report of vancomycin-resistant staphylococci isolated from healthy carriers in Brazil. J Clin Microbiol. 2005;43:179-85. although unstable.2828 Mashaly GES, El-Mahdy RH. Vancomycin heteroresistance in coagulase negative Staphylococcus blood stream infections from patients of intensive care units in Mansoura University Hospitals, Egypt. Ann Clin Microbiol Antimicrob. 2017;16:3-7. The results of the current work showed that, with the exception of oxacillin, vancomycin was the drug with the highest values of MIC50 and MIC90. Despite the full susceptibility of the collection, the MIC values were the highest in the period of 20 years, and reduced susceptibility was detected in some S. epidermidis, S. hemolyticus, S. hominis, and S. capitis strains. In the studies performed by Natoli et al.,2929 Natoli S, Fontana C, Favaro M, et al. Characterization of coagulase-negative staphylococcal isolates from blood with reduced susceptibility to glycopeptides and therapeutic options. BMC Infect Dis. 2009;9:83. reduced susceptibility to vancomycin was detected with a frequency of 5.4% among CoNS isolates, in S. epidermidis and S. hemolyticus species. According to the same authors, Staphylococcus colonies grown on vancomycin agar may lead to glycopeptide heteroresistance, which can be a precursor of glycopeptide resistance, causing complicated infections and treatment failure. This should be taken into consideration in therapeutic decisions.3030 Sullivan SB, Austin ED, Stump S, et al. Reduced vancomycin susceptibility of methicillin-susceptible Staphylococcus aureus: no significant impact on mortality but increase in complicated infection. Antimicrob Agents Chemother. 2017;61, http://dx.doi.org/10.1128/AAC.00316-17.AAC.00316-17.
http://dx.doi.org/10.1128/AAC.00316-17.A...
The increase in the proportion of oxacillin resistant CoNS and decrease in their susceptibility to vancomycin emphasize the importance of studies involving other therapeutic choices. Tigecycline, a Gram-positive and negative broad spectrum semisynthetic glycylcycline, is considered a drug with excellent activity against oxacillin susceptible and resistant CoNS,1414 John JF, Harvin AM. History and evolution of antibiotic resistance in coagulase-negative staphylococci: susceptibility profiles of new anti-staphylococcal agents. Ther Clin Risk Manag. 2007;3:1143-52.,2929 Natoli S, Fontana C, Favaro M, et al. Characterization of coagulase-negative staphylococcal isolates from blood with reduced susceptibility to glycopeptides and therapeutic options. BMC Infect Dis. 2009;9:83. despite our data showing rates of 8.3% of resistance, most often in S. hemolyticus, followed by S. hominis, S. lugdunensis, and S. epidermidis. Similar MIC90 results were described for tigecycline, with no difference between oxacillin resistant and susceptible CoNS.3131 Noskin GA. Tigecycline: a new glycylcycline for treatment of serious infections. ClinInfectDis. 2005;41:S303-14 (1537-6591(Electronic)). In the studies conducted by Natoli et al.2929 Natoli S, Fontana C, Favaro M, et al. Characterization of coagulase-negative staphylococcal isolates from blood with reduced susceptibility to glycopeptides and therapeutic options. BMC Infect Dis. 2009;9:83. tigecycline demonstrated good activity against CoNS. According to those authors, tigecycline is not recommended for the treatment of bacteremia and its use should be limited in order to preserve activity against multi-resistant Gram-negative bacteria. Mutations in the ribosomal gene S10 and rpsJ and mepA genes seem to be associated with tigecycline resistance.3232 Angeles Argudin M, Roisin S, Dodémont M, Nonhoff C, Deplano A, Denisa O. Mutations at the ribosomal s10 gene in clinical strains of Staphylococcus aureus with reduced susceptibility to tigecycline. Antimicrob Agents Chemother. 2018;62:2017-9.,3333 Haim MS, Di Gregorio S, Galanternik L, et al. First description of rpsJ and mepA mutations associated with tigecycline resistance in Staphylococcus aureus isolated from a cystic fibrosis patient during antibiotic therapy. Int J Antimicrob Agents. 2017;50:739-41.
Quinupristin/dalfopristin is a streptogramin belonging to the macrolide-lincosamide-streptogramin group. The combination of quinupristin and dalfopristin is synergistic and usually bactericidal when these agents are compared singly, or compared to similar macrolide antimicrobials.3434 Manzella JP. Quinupristin-dalfopristin: a new antibiotic for severe gram-positive infections. Am Fam Physician. 2001;64:1863-6. In this work, despite presenting excellent efficacy in the majority of the studied CoNS, intermediate resistance to this drug was detected in two S. epidermidis and one S. hemolyticus. In the study conducted by Mendes et al.,3535 Mendes C, Sinto SI, Hsiung A, et al. Atividade antimicrobiana in vitro de quinupristina/dalfopristina para cocos gram-positivos isolados de cinco centros brasileiros: resultado do estudo de vigilância L-SMART. J Bras Patol Med Lab. 2002;38, http://dx.doi.org/10.1590/S1676-24442002000300005.
http://dx.doi.org/10.1590/S1676-24442002...
quinupristin/dalfopristin demonstrated excellent effectiveness for CoNS, the strains were fully susceptible, with MIC90 values of 0.38 µg/mL for the oxacillin-susceptible strains and 0.75 µg/mL for the oxacillin resistant strains. In addition, Venkatesh et al.3636 Venkatesh MP, Placencia F, Weisman LE. Coagulase-negative staphylococcal infections in the neonate and child: an update. Semin Pediatr Infect Dis. 2006;17:120-7. described good effectiveness of quinupristin/dalfopristin for oxacillin resistant and susceptible strains.
Daptomycin, an antimicrobial studied for decades, was brought back into use in 2006, for the treatment of bacteremia and endocarditis caused by Staphylococcus.3737 Fajardo Olivares M, Hidalgo Orozco R, Rodríguez Garrido S, Rodríguez-Vidigal FF, Vera Tomé A, Robles Marcos M. Activity of vancomycin, ciprofloxacin, daptomycin, and linezolid against coagulase-negative staphylococci bacteremia. Rev Esp Quimioter. 2011;24:74-8. In the present study, daptomycin showed excellent efficacy for CoNS isolates, with low MIC50 values. Olivares et al.3737 Fajardo Olivares M, Hidalgo Orozco R, Rodríguez Garrido S, Rodríguez-Vidigal FF, Vera Tomé A, Robles Marcos M. Activity of vancomycin, ciprofloxacin, daptomycin, and linezolid against coagulase-negative staphylococci bacteremia. Rev Esp Quimioter. 2011;24:74-8. also verified the susceptibility of all CoNS to daptomycin, with low variation in the MIC values. In a work studying 1126 CoNS, conducted by Critchley et al.,3838 Critchley IA, Blosser-middleton S, Jones ME, Thornsberry C, Sahm DF, Karlowsky JA. Baseline study to determine in vitro activities of daptomycin against gram-positive pathogens isolated in the United States in 2000-2001. Antimicrob Agents Chemother. 2003;47:1689-93. daptomycin was active on a MIC range from 0.015 to 2.0 µg/mL, and the MIC90 was 0.5 µg/mL. According to those authors, the most active agents in these analyses were daptomycin and quinupristin/dalfopristin, which emphasizes the relevance of these antimicrobials in the treatment of infections caused by CoNS.
Linezolid, a synthetic oxazolidinone potentially active against several bacteria, is another drug that has demonstrated good efficacy against CoNS.3939 de Almeida LM. Caracterização molecular dos mecanismos de resistência à linezolida em estafilococos coagulase-negativos e estudo da estabilidade do fenótipo resistente. Universidade de São Paulo; 2012. Linezolid has become important for the therapeutic treatment of chronic infections by CoNS, despite the description of resistance. In Brazil, the first case of linezolid resistance was described in 2006, on a clinical isolate of MRSA4040 Gales A, Sader H, Andrade S, Lutz L, Machado A, Barth A. Emergence of linezolid-resistant Staphylococcus aureus during treatment of pulmonary infection in a patient with cystic fibrosis. Int J Antimicrob Agents. 2006;27:300-2. and, among the CoNS, in S. epidermidis, S. hominis, and S. hemolyticus.4141 Lincopan N, de Almeida LM, Elmor de Araújo MR, Mamizuka EM. Linezolid resistance in Staphylococcus epidermidis associated with a G2603T mutation in the 23S rRNA gene. Int J Antimicrob Agents. 2009;34:281-2. In the work conducted by Olivares et al.,3737 Fajardo Olivares M, Hidalgo Orozco R, Rodríguez Garrido S, Rodríguez-Vidigal FF, Vera Tomé A, Robles Marcos M. Activity of vancomycin, ciprofloxacin, daptomycin, and linezolid against coagulase-negative staphylococci bacteremia. Rev Esp Quimioter. 2011;24:74-8. despite the detection of seven linezolid resistant strains, this drug presented effective MIC values in CoNS strains. On the other hand, an outbreak of linezolid resistant S. epidermidis clones containing mutations in ribosomal proteins L3 and L4, as well as the cfr plasmid, recently identified in France, have been reported.4242 Dortet L, Glaser P, Kassis-Chikhani N, et al. Long-lasting successful dissemination of resistance to oxazolidinones in MDR Staphylococcus epidermidis clinical isolates in a tertiary care hospital in France. J Antimicrob Chemother. 2018;73:41-51.
S. hemolyticus was the species that presented the highest oxacillin MIC values, and concentrations higher than 256 µg/mL were needed to inhibit 50% of isolates. As well as for oxacillin, this species presented higher MIC values for tigecycline and most of the antimicrobials tested. Several works show high rates of resistance to the antimicrobials used for the treatment of infections caused by S. hemolyticus, especially methicillin and glycopeptides. Some authors describe a high prevalence of genes encoding resistance to β-lactam and aminoglycoside agents, as well as a significant proportion of isolates with MIC values close to the resistance breakpoint,4343 Fredheim EGA, Klingenberg C, Rohde H, et al. Biofilm formation by staphylococcus haemolyticus. J Clin Microbiol. 2009;47:1172-80.,4444 Frogatt JW, Johnston JL, Galetto DW, Archer GL. Antimicrobial resistance in nosocomial isolates of {IStaphlococcus haemolyticus}. Antimicrob Agents Chemother. 1989;33:460-6. emphasizing the importance of S. hemolyticus as a multiresistant pathogen.
The association of the MIC range with the SCCmec types demonstrated higher MICs for vancomycin, linezolid, daptomycin, and quinupristin/dalfopristin in S. epidermidis carrying SCCmecIV. The genes related to resistance to these antimicrobials are mediated by plasmids, found mostly in methicillin resistant strains with hospital origin.4545 Otto M. Staphylococcus epidermidis-the “accidental” pathogen. Nat Rev Microbiol. 2009;7:555-67. SCCmec IV is characteristic of community isolates, especially due to its size and low adaptive cost. Studies suggest that the acquisition of resistance genes has environmental non-clinical origin, given the high diversity of resistance gene carriers in the natural environment.4646 Davies JE. Origins, acquisition and dissemination of antibiotic resistance determinants. Ciba Found Symp. 1997;207:15-27, discussion 27-35.,4747 Martínez JL, Baquero F, Andersson DI. Predicting antibiotic resistance. Nat Rev Microbiol. 2007;5:958-65. Furthermore, SCCmecIV was only detected in S. epidermidis, which as the most common species in human skin is the most influenced by selective pressure. The higher MICs compared to other antimicrobials may also be related to the selective pressure, as the level of exposure to these drugs in the hospital environment would bias the selection of reduced susceptibility and resistant strains, since several mutation events, genetic recombination, and modifications in the microbial physiology are needed to generate phenotypic changes.4848 Andersson DI, Hughes D. Antibiotic resistance and its cost: is it possible to reverse resistance?. Nat Rev Microbiol. 2010;8:260-71.
Metabolic and physiological modifications related to selective pressure could be observed in strains grown on 8 µg/mL vancomycin agar, as the cell wall thickening was found in most CoNS isolates due to increased peptidoglycan synthesis. This mechanism is more advantageous for CoNS than the acquisition of the van operon, which is a mediator of vancomycin resistance. The van operon is acquired by horizontal gene transfer and its expression is only stimulated in the presence of glycopeptide. This stimulus causes a very high adaptive cost in the presence of vancomycin, being disadvantageous for the CoNS in a vancomycin medium.4848 Andersson DI, Hughes D. Antibiotic resistance and its cost: is it possible to reverse resistance?. Nat Rev Microbiol. 2010;8:260-71.,4949 Livermore D. Can better prescribing turn the tide of resistance?. Nat Rev Microbiol. 2004;2:73-8. Regarding the acquisition of other resistance genes in CoNS, such as the mecA gene, the initial adaptive cost is softened by compensatory additional mutations for the resistance “costs”. Recently, punctual mutations in genes such as vraR have been shown to be associated with reduced susceptibility to vancomycin and cell wall thickening in staphylococci.5050 Baek JY, Chung DR, Ko KS, et al. Genetic alterations responsible for reduced susceptibility to vancomycin in community-associated MRSA strains of ST72. J Antimicrob Chemother. 2017;72:2454-60.
The present study showed a high rate of bacteremia caused by CoNS in neonatal and pediatric units, involving children under one year of age, the main agents being S. epidermidis, S. hemolyticus, S. hominis, S. lugdunensis, and S. warneri. S. capitis were not isolated in these units, being agents of bacteremia in adults admitted to the internal medicine ward, gastroenterology, neurology, and emergency room.
As the study involved bacteremia caused by staphylococci isolated over more than 30 years, much of the data associated with patients’ medical records could not be retrieved, so it was not possible to associate the infection outcome of all patients, which is a limitation of the current study. Data obtained from patients in neonatal units indicated the clinical importance of CoNS bacteremia, which may progress to diseases that require specialized care.
Knowledge of antimicrobial resistance is of great importance for the correct treatment of infections caused by CoNS. Furthermore, the virulence factors of these bacteria and the immunity of patients are factors that contribute to the ability of the microorganism to cause more serious infections.
The results of our study spanning 20 years showed a high frequency of antimicrobial resistance in CoNS, which reflects the excessive use of these drugs. Besides the metabolic and physiologic modifications that could lead to reduced susceptibility to antimicrobials, their condition as human commensal bacteria make them ideal transporters and an efficient reservoir of resistance genes, especially the low-cost elements, such as SCCmec.4545 Otto M. Staphylococcus epidermidis-the “accidental” pathogen. Nat Rev Microbiol. 2009;7:555-67. The antimicrobials which offered the best results should be used in such a way as to preserve their efficacy and prevent resistance.
Acknowledgments
We thank the São Paulo Research Foundation (FAPESP- Process: 2011/23742-2)) and the National Council for Scientific and Technological Development (CNPq- Process: 470649/2011-9) for the financial support.
References
-
1Garrity GM, Labeda DP, Oren A. Judicial Commission of the International Committee on Systematics of Prokaryotes * XIIth International (IUMS) Congress of Bacteriology and Applied Microbiology: minutes of the meetings, 3, 4 and 6 August 2008, Istanbul, Turkey. Int J Syst Evol Microbiol. 2011;61:2775-80.
-
2Rocchetti TT, Martins KB, Martins PYF, et al. Detection of the mecA gene and identification of Staphylococcus directly from blood culture bottles by multiplex polymerase chain reaction. Brazilian J Infect Dis. 2018;22:99-105.
-
3Archer GL, Niemeyer DM. Origin and evolution of DNA associated with resistance to methicillin in staphylococci. Trends Microbiol. 1994;2:343-7.
-
4Ito T, Katayama Y, Asada K, Mori N, Tsutsumimoto K. Structural comparison of three types of staphylococcal cassette chromosome mec integrated in the chromosome in methicillin-resistant Staphylococcus aureus Antimicrob Agents Chemother. 2001;45:1323-36.
-
5Wu Z, Li F, Liu D, Xue H, Zhao X. Novel type XII staphylococcal cassette chromosome mec harboring a new cassette chromosome recombinase, CcrC2. Antimicrob Agents Chemother. 2015;59:7597-601.
-
6Palazzo ICV, Araujo MLC, Darinia LC. First report of vancomycin-resistant staphylococci isolated from healthy carriers in Brazil. J Clin Microbiol. 2005;43:179-85.
-
7Appelbaum PC. The emergence of vancomycin-intermediate and vancomycin-resistant Staphylococcus aureus; 2006. p. 256.
-
8Koneman EW, Allen SD, Janda WM, Schreckenberger PC. W C W. Color Atlas and Textbook of Diagnostic Microbiology. 5th ed. Philadelphia: Lippincott; 1997.
-
9Couto I, Pereira S, Miragaia M, Santos Sanches I, De Lencastre H. Identification of clinical staphylococcal isolates from humans by internal transcribed spacer PCR. J Clin Microbiol. 2001;39:3099-103.
-
10Murakami K, Minamide W, Wada K, Nakamura E, Teraoka H, Watanabe S. Identification of methicillin-resistant strains of staphylococci by polymerase chain reaction. J Clin Microbiol. 1991;29:2240-4. Doi: 1939577.
-
11Oliveira DC. Multiplex PCR Strategy for Rapid Identification of Structural Types and Variants of the Society. Antimicrob Agents Chemother. 2002;46:2155-61.
-
12Machado ABMP, Reiter KC, Paiva RM, Barth AL. Distribution of staphylococcal cassette chromosome mec (SCCmec) types I, II, III and IV in coagulase-negative staphylococci from patients attending a tertiary hospital in southern Brazil. J Med Microbiol. 2007;56:1328-33.
-
13(CLSI) Clinical and Laboratory Standards. Performance standards for antimicrobial susceptibility testing, document M100-S23. 2016.
-
14John JF, Harvin AM. History and evolution of antibiotic resistance in coagulase-negative staphylococci: susceptibility profiles of new anti-staphylococcal agents. Ther Clin Risk Manag. 2007;3:1143-52.
-
15Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clin Microbiol Rev. 2014;27:870-926.
-
16Bouchami O, Achour W, Mekni MA, Rolo J, Ben Hassen A. Antibiotic resistance and molecular characterization of clinical isolates of methicillin-resistant coagulase-negative staphylococci isolated from bacteremic patients in oncohematology. Folia Microbiol (Praha). 2011;56:122-30.
-
17Martins A, Moraes Riboli DF, Cataneli Pereira V, et al. Molecular characterization of methicillin-resistant Staphylococcus aureus isolated from a Brazilian university hospital. Braz J Infect Dis. 2014;:3-7.
-
18Krediet TG, Mascini EM, Rooij E Van, Vlooswijk J, Paauw A, Gerards LJ. Molecular epidemiology of coagulase-negative staphylococci causing sepsis in a neonatal intensive care unit over an 11-year period. J Clin Microbiol. 2004;42:992-5, http://dx.doi.org/10.1128/JCM.42.3.992
» http://dx.doi.org/10.1128/JCM.42.3.992 -
19Ferreira RBR, Iorio NLP, Malvar KL, et al. Coagulase-negative staphylococci : comparison of phenotypic and genotypic oxacillin susceptibility tests and evaluation of the agar screening test by using different concentrations of oxacillin. J Clin Microbiol. 2003;41:3609-14.
-
20Chaves F, García-Alvarez M, Sanz F, Alba C, Otero JR. Nosocomial spread of a Staphylococcus hominis subsp. novobiosepticus strain causing sepsis in a neonatal intensive care unit. J Clin Microbiol. 2005;43:4877-9.
-
21Caierão J, Musskopf M, Superti S, Roesch E, Dias CG, d’Azevedo PA. Evaluation of phenotypic methods for methicillin resistance characterization in coagulase-negative staphylococci (CNS). J Med Microbiol. 2004;53:1195-9.
-
22Giusti MDe, Pacifico L, Panero A, Boccia A, Chiesa C. Phenotypic detection of nosocomial; 1999. p. 351-8.
-
23Kawaguchi EW, Minamide HM, Igmi H. The taxo-nomic distribution, characteristic and susceptibil-ity against antimicrobial agents of methicillin-resistant staphylococci isolated from blood. Kansenshogaku Zasshi. 1996;70:1147-53.
-
24Mchardy IH, Veltman J, Hindler J, Bruxvoort K, Carvalho MM, Humphries RM. Clinical and microbiological aspects of β-lactam resistance in Staphylococcus lugdunensis J Clin Microbiol. 2017;55:585-95.
-
25Tee WSN, Yen Soh S, Lin R, Loo LH. Staphylococcus lugdunensis carrying the mecA gene causes catheter-associated bloodstream infection in premature neonate. J Clin Microbiol. 2003;41:519-20.
-
26Ito T, Katayama Y, Hiramatsu K. Cloning and nucleotide sequence determination of the entire mec DNA of pre-methicillin-resistant Staphylococcus aureus N315. Antimicrob Agents Chemother. 1999;43:1449-58.
-
27Healy CM, Hulten KG, Palazzi DL, Campbell JR, Baker CJ. Emergence of new strains of methicillin-resistant Staphylococcus aureus in a neonatal intensive care unit. Clin Infect Dis. 2004;39:1460-6.
-
28Mashaly GES, El-Mahdy RH. Vancomycin heteroresistance in coagulase negative Staphylococcus blood stream infections from patients of intensive care units in Mansoura University Hospitals, Egypt. Ann Clin Microbiol Antimicrob. 2017;16:3-7.
-
29Natoli S, Fontana C, Favaro M, et al. Characterization of coagulase-negative staphylococcal isolates from blood with reduced susceptibility to glycopeptides and therapeutic options. BMC Infect Dis. 2009;9:83.
-
30Sullivan SB, Austin ED, Stump S, et al. Reduced vancomycin susceptibility of methicillin-susceptible Staphylococcus aureus: no significant impact on mortality but increase in complicated infection. Antimicrob Agents Chemother. 2017;61, http://dx.doi.org/10.1128/AAC.00316-17.AAC.00316-17
» http://dx.doi.org/10.1128/AAC.00316-17.AAC.00316-17 -
31Noskin GA. Tigecycline: a new glycylcycline for treatment of serious infections. ClinInfectDis. 2005;41:S303-14 (1537-6591(Electronic)).
-
32Angeles Argudin M, Roisin S, Dodémont M, Nonhoff C, Deplano A, Denisa O. Mutations at the ribosomal s10 gene in clinical strains of Staphylococcus aureus with reduced susceptibility to tigecycline. Antimicrob Agents Chemother. 2018;62:2017-9.
-
33Haim MS, Di Gregorio S, Galanternik L, et al. First description of rpsJ and mepA mutations associated with tigecycline resistance in Staphylococcus aureus isolated from a cystic fibrosis patient during antibiotic therapy. Int J Antimicrob Agents. 2017;50:739-41.
-
34Manzella JP. Quinupristin-dalfopristin: a new antibiotic for severe gram-positive infections. Am Fam Physician. 2001;64:1863-6.
-
35Mendes C, Sinto SI, Hsiung A, et al. Atividade antimicrobiana in vitro de quinupristina/dalfopristina para cocos gram-positivos isolados de cinco centros brasileiros: resultado do estudo de vigilância L-SMART. J Bras Patol Med Lab. 2002;38, http://dx.doi.org/10.1590/S1676-24442002000300005
» http://dx.doi.org/10.1590/S1676-24442002000300005 -
36Venkatesh MP, Placencia F, Weisman LE. Coagulase-negative staphylococcal infections in the neonate and child: an update. Semin Pediatr Infect Dis. 2006;17:120-7.
-
37Fajardo Olivares M, Hidalgo Orozco R, Rodríguez Garrido S, Rodríguez-Vidigal FF, Vera Tomé A, Robles Marcos M. Activity of vancomycin, ciprofloxacin, daptomycin, and linezolid against coagulase-negative staphylococci bacteremia. Rev Esp Quimioter. 2011;24:74-8.
-
38Critchley IA, Blosser-middleton S, Jones ME, Thornsberry C, Sahm DF, Karlowsky JA. Baseline study to determine in vitro activities of daptomycin against gram-positive pathogens isolated in the United States in 2000-2001. Antimicrob Agents Chemother. 2003;47:1689-93.
-
39de Almeida LM. Caracterização molecular dos mecanismos de resistência à linezolida em estafilococos coagulase-negativos e estudo da estabilidade do fenótipo resistente. Universidade de São Paulo; 2012.
-
40Gales A, Sader H, Andrade S, Lutz L, Machado A, Barth A. Emergence of linezolid-resistant Staphylococcus aureus during treatment of pulmonary infection in a patient with cystic fibrosis. Int J Antimicrob Agents. 2006;27:300-2.
-
41Lincopan N, de Almeida LM, Elmor de Araújo MR, Mamizuka EM. Linezolid resistance in Staphylococcus epidermidis associated with a G2603T mutation in the 23S rRNA gene. Int J Antimicrob Agents. 2009;34:281-2.
-
42Dortet L, Glaser P, Kassis-Chikhani N, et al. Long-lasting successful dissemination of resistance to oxazolidinones in MDR Staphylococcus epidermidis clinical isolates in a tertiary care hospital in France. J Antimicrob Chemother. 2018;73:41-51.
-
43Fredheim EGA, Klingenberg C, Rohde H, et al. Biofilm formation by staphylococcus haemolyticus. J Clin Microbiol. 2009;47:1172-80.
-
44Frogatt JW, Johnston JL, Galetto DW, Archer GL. Antimicrobial resistance in nosocomial isolates of {IStaphlococcus haemolyticus}. Antimicrob Agents Chemother. 1989;33:460-6.
-
45Otto M. Staphylococcus epidermidis-the “accidental” pathogen. Nat Rev Microbiol. 2009;7:555-67.
-
46Davies JE. Origins, acquisition and dissemination of antibiotic resistance determinants. Ciba Found Symp. 1997;207:15-27, discussion 27-35.
-
47Martínez JL, Baquero F, Andersson DI. Predicting antibiotic resistance. Nat Rev Microbiol. 2007;5:958-65.
-
48Andersson DI, Hughes D. Antibiotic resistance and its cost: is it possible to reverse resistance?. Nat Rev Microbiol. 2010;8:260-71.
-
49Livermore D. Can better prescribing turn the tide of resistance?. Nat Rev Microbiol. 2004;2:73-8.
-
50Baek JY, Chung DR, Ko KS, et al. Genetic alterations responsible for reduced susceptibility to vancomycin in community-associated MRSA strains of ST72. J Antimicrob Chemother. 2017;72:2454-60.
Publication Dates
-
Publication in this collection
26 June 2020 -
Date of issue
Mar-Apr 2020
History
-
Received
4 Sept 2019 -
Accepted
27 Jan 2020 -
Published
19 Feb 2020