Abstracts
OBJECTIVE:
The study aimed to understand how care for the aged has been accomplished at Family Health Units according to health professionals.
METHODS:
Qualitative study, using social phenomenological analysis according to Alfred Schutz.
RESULTS:
Seven professionals with a higher education degree were interviewed with the help of a guiding question. Based on the analysis, the following was evidenced: care based on health programs, to the detriment of care integrality and the expanded clinic, and view of integral care needs and perspectives.
CONCLUSION:
This study reveals the need to improve elderly care. The professionals recognize the population aging and indicate the need for training. The education of health workers education is the starting point for change. In addition, managers and the State need to organize a care network that includes the elderly, with services offered according to the demand.
Aged; Family Health; Comprehensive Health Care
Tal estudo buscou compreender como vem sendo realizado o cuidado ao idoso em Unidade de Saúde da Família segundo a visão dos profissionais de saúde.
MÉTODOS:
Estudo qualitativo, com a análise fenomenológica social de Alfred Schutz.
RESULTADOS:
Foram entrevistados sete profissionais de nível superior por meio de questão norteadora. A análise possibilitou evidenciar: cuidados pautados em programas de saúde, com prejuízo da integralidade do cuidado e da clínica ampliada, e visão das necessidades e perspectivas do cuidado integral.
CONCLUSÃO:
O estudo revela a necessidade de avançarmos no cuidado ao idoso. Os profissionais reconhecem o envelhecimento da população e apontam a necessidade de capacitação para o cuidado. A educação dos trabalhadores se dá como ponto de partida para a mudança. Também é preciso que os gestores e o Estado organizem uma rede de cuidado que inclua a pessoa idosa, com ofertas de serviços de acordo com a demanda apresentada.
Idoso; Saúde da família; Assistência integral à saúde
OBJETIVO:
Estudio que trata comprender cómo se está llevando a cabo el cuidado de ancianos en la Unidad de Salud de la Familia, según la opinión de los profesionales de salud.
MÉTODOS:
Estudio cualitativo con análisis social fenomenológica de Alfred Schutz.
RESULTADOS:
Entrevistamos a 07 profesionales de primer nivel a través de pregunta de investigación. El análisis evidenció: el cuidado guiado por los programas de salud, en detrimento de la atención integral y la clínica ampliada, y la visión de las necesidades y perspectivas de la atención integral.
CONCLUSIÓN:
El estudio pone de manifiesto la necesidad de avanzar en el cuidado de ancianos. Los profesionales reconocen el envejecimiento y la necesidad de mudanza. La educación de los trabajadores se da como punto de partida para el cambio. También es necesario que los administradores y el Estado organicen una red de atención que incluya a las personas mayores, con ofertas de servicios de acuerdo a la demanda presentada.
Anciano; Salud de La Familia; Atención Integral de Salud
INTRODUCTION
According to research, Brazil is going through a demographic transition phase, accompanied by significant changes in the age pyramid. Since 1940, a reduction in mortality rates is observed, mainly among younger people. The childhood mortality rate, which corresponded to 135 deaths for every thousand live birth in 1995, had dropped to 20 in 2010, a decrease by approximately 85%. In addition, in the last 15 years, the life expectancy increased from 50 to 73 years, resulting in a larger number of elderly people in the Brazilian population. Consequently, in the next 40 years, the elderly population will grow from less than 20 million to 65 million in 205011. Banco Mundial. Envelhecendo em um Brasil mais velho: implicações do envelhecimento populacional para o crescimento econômico, a redução da pobreza, as finanças públicas e a prestação de serviços. Washington: Banco Mundial; 2011..
According to data by the Brazilian Institute for Geography and Statistics (IBGE), through the 2009 National Household Research (PNAD), in 1999, the elderly population (people over 60 years of age) represented 9.1% of the Brazilian population. In 2009, this population had increased to 11.3% of all Brazilians. The PNAD also shows that 22.6% of people over 60 years of age indicated no illnesses. Almost half of the interviewed population, however, suffered from more than one chronic condition (48.9%)22. Instituto Brasileiro de Geografia e Estatistica. Indicadores sociodemográficos e de saúde no Brasil. Rio de Janeiro (RJ): Instituto Brasileiro de Geografia e Estatística; 2009..
All of these changes found through epidemiology show us important aspects that prove this age change in Brazil and underline the importance of constructing and putting in practice policies to welcome the needs that emerge over the years.
According to a report by the World Bank (2011), spending on health will considerably rise as a result of the increased proportion of elderly people and the increased frequency at which this population uses health services. Besides the factors already mentioned, the demand by elder elderly people will also increase in the next 30 years, accompanied by a growing number of weakened people, despite efforts to prevent illnesses and advanced treatments. As a consequence of population aging, the Health area will face challenges like the prevention and delay of illnesses and impairments, the health maintenance, independence and mobility of the elderly. The expansion and strengthening of the Family Health Program are considered as a care strategy for these elderly, provided that the focus and efforts towards this purpose are present11. Banco Mundial. Envelhecendo em um Brasil mais velho: implicações do envelhecimento populacional para o crescimento econômico, a redução da pobreza, as finanças públicas e a prestação de serviços. Washington: Banco Mundial; 2011..
As from the change in the Brazilian Constitution in 1988, health is considered a right of all and a duty of the State, which represents an advance for Brazilian public health. The approval of the Organic Health Laws in 1990 (Law 8.080/1990 and Law 8.142/1990) gave rise to the so-called Unified Health System (SUS), which is based on the principles of universality, integrality and equity. The integrality established by the SUS goes far beyond a guideline, and represents a transformation of the traditional health model existing in Brazil. When considering health and integrality, we refer to the multidisciplinarity of care, of the individual as a whole, of the service relations among different care levels, of the relationship in teamwork33. Viegas SMF, Penna CMM. A construção da integralidade no trabalho cotidiano da equipe saúde da família. Esc Anna Nery. 2013 jan-mar; 17(1):133-41..
Years later, on October 1st 2003, Law 10.741 was issued to establish the Statute of the Elderly. Its creation represented a gain to guarantee the rights of the elderly. The Statute approaches the rights of the elderly as citizens, with an integral range, including the different facets that interfere in the quality of life of this group. Despite this legal guarantee, many bottlenecks remain for its compliance, and even lack of knowledge in the population.
This whole change in the life expectancy of the Brazilian population and, hence, the growth of the elderly population is due to the improvement of sanitation conditions in Brazil and the health technologies these policies have made available. In political terms, it is observed that Brazil has attempted to advance in response to the population changes it has gone through. The creation of the SUS and, years later, of the Statute of the Elderly, shows the concern with guaranteeing the rights of the elderly, as well as the established principles.
In 2006, according to decree 399/GM, issued on February 22nd 2006, the Health Pact is launched, to be reconsidered each year in accordance with the SUS and the population's health needs. It comprises three dimensions: the Pact for Life, the Pact in Defense of the SUS and the Management Pact44. Portaria nº 399/ GM de 22 de fevereiro de 2006. Divulga o Pacto pela Saúde 2006 - Consolidação do SUS e aprova as Diretrizes Operacionais do Referido Pacto. Diário Oficial da República Federativa do, Brasília (DF), 23 fev 2006. Seção 1: 43. .
The Pact for Life consists of health commitments in accordance with the country's situation and health priorities, defined by the federal, state and municipal governments. Its care guidelines include elderly health, proposed to implement the National Elderly Health Policy. As regards the operational directives, within the elderly health area, the Pact for Life indicates some care strategies, like the Health Booklet of the Elderly, Primary Care and Health Manual for the Elderly, Continuing Distance Education Program for primary care professionals, Welcoming, Pharmaceutical Care, Distinguished Hospitalization Care and Home Care44. Portaria nº 399/ GM de 22 de fevereiro de 2006. Divulga o Pacto pela Saúde 2006 - Consolidação do SUS e aprova as Diretrizes Operacionais do Referido Pacto. Diário Oficial da República Federativa do, Brasília (DF), 23 fev 2006. Seção 1: 43. .
In the same year as the Pact for Life was created, decree 2.528 is approved on October 19th 2006, which establishes the National Health Policy for the Elderly, aimed at "... recovering, maintaining and promoting the autonomy and independence of elderly individuals, focusing collective and individual health measures towards this end, in line with the principles and guidelines of the Unified Health System". This once again shows the search to guarantee integral care to the elderly.
To achieve its objective, the guideline for elderly care is the promotion of active and healthy aging; integral elderly health care, with an expanded perspective on biopsychosocial issues in bonding relations, interaction with health professionals and care delivery at the different levels in accordance with the identified need; intersectorial actions aiming for care integrality; resource provision to guarantee the quality of health care; encouragement of participation in social control; training and education of health professionals in elderly health care; dissemination and information about the National Elderly Health Policy for health professionals, managers and users in the SUS; promotion of national and international cooperation in elderly healthcare experiences; and, finally, support for study and research development55. Portaria nº 2.528, de 19 de outubro de 2006. Política Nacional de Saúde da Pessoa Idosa. Diário Oficial da República Federativa do Brasil, Brasília (DF), 20 out 2006. Seção 1:142..
Thus, with a view to the proper functioning of the National Elderly Health Policy, federal, state and municipal managers are responsible for providing the means to achieve the goals of this policy. To put in practice the established guidelines and develop health actions, articulation with other sectors is needed, such as education, social security, social services, work and employment, urban development, transportation, justice and human rights, sports and leisure and science and technology44. Portaria nº 399/ GM de 22 de fevereiro de 2006. Divulga o Pacto pela Saúde 2006 - Consolidação do SUS e aprova as Diretrizes Operacionais do Referido Pacto. Diário Oficial da República Federativa do, Brasília (DF), 23 fev 2006. Seção 1: 43. .
Primary Health Care works in accordance with SUS principles, aiming for health promotion, disease prevention and treatment and the reduction of damage or suffering that can compromise people's quality of life. Family Health represents the main strategy, as it enhances bonding between professionals and users in accordance with territorial limits. It is focused on the family and the community, within a collective, multiprofessional model, with a view to an integral comprehension of the individual, family and collective dimensions. Hence, the professionals working at Family Health Units are responsible for monitoring the elderly population within their coverage area, as a framework for integral and equanimous health care66. Costa GD, Cotta RMM, Ferreira MLSM, Reis JR, Franceschini SCC. Saúde da família: desafios no processo de reorientação do modelo assistencial. REBEN. 2009 jan-fev; 62(1):113-8..
Integrality emerges as a strategy the sanitary movement has adopted to achieve the desired changes in Brazilian health. In summary, it represents a desirable characteristic of the health system and its practices. Achieving integrality means finding intersubjective practices, with interpersonal relations among the subjects, developing dialogic practices. The dialogue furthers the understanding of the presented context, identifying the needs and developing skills to recognize each situation between the subject and the health professional. Hence, claiming for integrality means promoting health actions in tune with the singular context of each relation77. Mattos RA. A integralidade na prática (ou sobre a prática da integralidade). Cad Saúde Pública. 2004 set-out; 20(5):1411-6..
In view of the above, the current stage should be verified, considering how professionals are promoting the population's health and whether they are familiar with the importance of this whole change in care. As a result of the inversion of the care model, with health promotion and care integrality as the main foci of care, it is important to verify how professionals deliver care to this population, including the assessment of advances and setbacks in this process. Hence, we aimed to understand how elderly care is delivered at a Family Health Unit according to the health professionals.
METHOD
Study Design
The qualitative method was chosen to develop this study, in the methodological framework of Alfred Schutz' social phenomenology. Phenomenology studies the phenomena, what appears to our awareness, what is given, with a view to understanding it88. Wagner HTR. Sobre fenomenologia e relações sociais: Alfred Schütz. Petrópolis (RJ): Vozes; 2012..
According to Schutz, the social world is very difficult to measure. To analyze the world through the social sciences, one needs to use the comprehensive method, by means of an investigation of its multiple types. Thus, Schutz' phenomenology is aimed at understanding the interviewee's subjectivity with regard to aspects of our awareness that can be described. Hence, each person has a situation proper to him/herself and not to the other person99. Capalbo C. Metodologia das ciências sociais: a fenomenologia de Alfred Schutz. Londrina (PR): UEL; 1998..
According to Schütz, man is a social being, lives in a world shared with his peers, with things and with himself. In this relation, man gradually constitutes his "biographic I", which will motivate him to act88. Wagner HTR. Sobre fenomenologia e relações sociais: Alfred Schütz. Petrópolis (RJ): Vozes; 2012..
Place of study
The research was undertaken in Botucatu-SP and more specifically involved the professionals from the Family Health Unit Jd. Aeroporto. The author developed activities at the selected unit in the Multiprofessional Residency Program in Family Health, affiliated with the Botucatu Medical School - Unesp. Two teams are active at the unit, covering an area of 8104 registered persons, 304 of them aged 65 years or older, according to data from the Botucatu Municipal Information System - CPDQ in January 20131010. Botucatu. Sistema de Informação do Município de Botucatu. Botucatu: CPDQ; 2013.. The service consists of two physicians, two nurses, one dentist, one dentistry assistant, six auxiliary nurses, nine health agents and three Family Health Residents. These residents were two nurses and one psychologist. One of the residents was the researcher and was therefore, for ethical reasons, excluded from the data collection.
Subjects
The research subjects were the higher-education professionals from two teams active at the Family Health Unit Jd. Aeroporto, who accepted the invitation to participate in the research and answered the following guiding question: How do you deliver care to elderly people at this health service? Tell me about it.
All professionals who accepted to participate, in compliance with ethical research criteria, signed the Informed Consent Form. Thus, seven interviews were held. None of the professionals refused to participate.
Ethical Procedures
The project was submitted to and received approval from the Research Ethics Committee at Botucatu Medical School - Unesp, under protocol 4118-2012. First, authorization for the study was obtained from the Primary Care Coordination at the Botucatu Municipal Health Secretary/SP. To preserve the subjects' anonymity, the interviews were randomly collected and numbered in the order in which they were held. They were identified using the letter I for interview, followed by a numeral.
Data collection
The researcher collected the data through interviews, registered through a recording and then transcribed for analysis.
Analysis
In phenomenological research, the researcher does not know the meaning of the subjects' experiences a priori. Based on the unknown, (s)he chooses a direction and elaborates the research problem. The analysis makes it possible to reach its meanings, about the subject's perceptions of what (s)he was questioned about99. Capalbo C. Metodologia das ciências sociais: a fenomenologia de Alfred Schutz. Londrina (PR): UEL; 1998..
Phenomenological analysis presupposes a methodological trajectory that starts with ideographic analysis: the subject's descriptions are subject to attentive and individual reading to find and, at the same time, identify the units of meaning, when the researcher grants them meaning. After identifying the meanings the interviewees have shown, nomothetic analysis is applied to all testimonies, followed by their grouping per theme, including the description and interpretation of the statement, so as to reach its invariant, its common elements and, thus, its essence. The researcher understands the subjects' actions by moving from the individual to something general, which emerges from the convergences and divergences found in the individual statements99. Capalbo C. Metodologia das ciências sociais: a fenomenologia de Alfred Schutz. Londrina (PR): UEL; 1998..
Hence, the intent was to depart from the subjects' statements and, through comprehensive analysis, reach their action in care delivery to elderly people in primary care.
RESULTS
Characteristics of the Subjects
Seven higher education professionals participated in the study, including physicians, nurses and a psychologist. As regards the professionals' age range, the mean age was 32.42 years, with a minimum age of 25 and a maximum of 47 years. Concerning experience in the area, two subjects possess between zero and two years, two between three and four and three five or more years of experience. When asked about their professional education to work in Family Health, six out of seven higher education professionals have finished or are taking a specialization program in Family Health.
Analysis
First, the testimonies were subject to ideographic analysis, that is, the full version of each interview was analyzed individually, highlighting the most meaningful terms for the researcher, in response to the guiding question "how do you deliver care to elderly patients at this health service? Tell me about it". For all interviews, the description was followed by reduction and understanding.
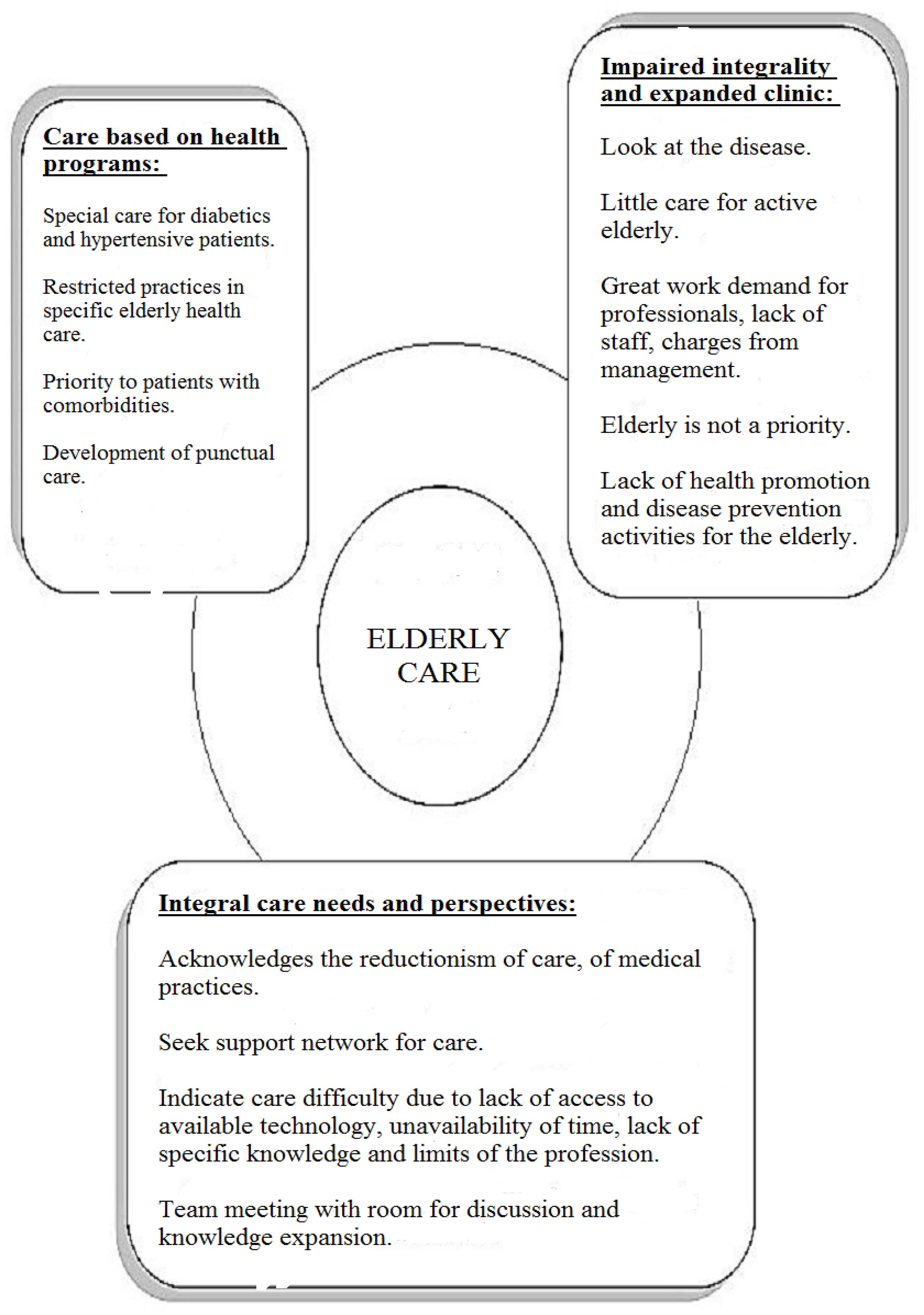
Next, the nomothetic analysis was applied, a general analysis of all testimonies in search of convergences, the common, the invariant. Based on the comprehensive reading and interpretation of the statements, three thematic categories were elaborated, as evidenced below in Figure 1:
Diagram elaborated by the authors, showing the health professionals' experiencein elderly health care at primary care level. Botucatu, São Paulo, Brazil, 2013.
The care practice of higher education professionals
CATEGORY 1: Care based on health programs
The professionals' statements revealed a frequent concern with elderly care delivery according to programs established in health policies. Nevertheless, they did not mention programs that specifically look at elderly health at any time, which respond to the needs of those over 60 years of age. Concerns with care delivery to established illnesses were shown.
(...) care especially focused on the elderly, I don't think we've got that. At least in my routine, in my work process, I don't perceive special elderly care, except when they suffer from diabetes, hypertension, or when the patient is bedridden (...) I-1
(...) we do the prostate tests. That's from 40 or 45 years onwards. So that's one kind of care, right. (...) There are the Hiperdia campaigns we do at the service, for diabetics and hypertensives, as many of them are elderly, right. I-2
As observed, the Hiperdia program, which involves the hypertensive and diabetic population, aimed at adults of any age range, is the main elderly care at the health service. The patients are included in the program after the diagnosis of these comorbidities.
(...) we end up prioritizing patients in some program, there's no logic behind the work process, to organize this care in such a way that healthy individuals are considered (...) I-3
I don't think there's anything specific for elderly health. (...) the elderly is to get the flu vaccine, but we know that it's open to other publics. Hiperdia, consultations are also open to other publics and what we receive most are elderly with comorbidities. The elderly without comorbidities are somewhat excluded from our care. I-4
Hence, the elderly are only focused on in an annual activity, proposed by the municipal primary care management. During one week, punctual activities are organized at the Family Health services, focusing on the elderly.
(...) each year, there's the week of the elderly.(...) during that week, we organize actions focused on the elderly, then we attempt to do promotion, prevention activities. (...) in the routine, in daily practice, I am unable to perceive (...) any activity that considers elderly health prevention and promotion. (...) we haven't done that, right. I-1
The practices end up becoming reductionist without the holistic valuation of the elderly. Various factors can make the professionals prioritize compliance with health programs in their care, including charges to comply with targets, lack of support from management, lack of professional knowledge about care, among others. As shown, individual care delivery during consultations ends up being the main care strategy, mainly for participants in Hiperdia.
(...) patients with comorbidities, hypertension, diabetes, any other kind of illness, we deal with during the scheduled appointments (...) the elderly without any kind of comorbidity, in fact there's no active search for these elderly, right (...) I-5
(...) it's no use to change our service: ah, let's do it different then! Let's establish a project and do everything differently! Because, rightly or wrongly, we end up being charged for the care, right. I-3
(...) the service has difficulties to plan activities for the elderly without an established health problem, right. Care ends up being more focused on those cases. I-6
CATEGORY 2: Impaired integrality and expanded clinic
Delivering integral care means looking at each individual's biopsychosocial part. The expanded clinic serves not only to respond to illnesses, but also to singular health problems. Findings these practices in health services is a challenge.
We attempt to look at the most prevailing illnesses in the elderly, for an approach in that sense. I-2
(...) focused on the disease the elderly presents, right. Because an integral approach remains difficult, we always direct it towards the disease. (...) elderly people who are healthy or suffer from some change characteristic of their age, right, they end up being left aside (...) I-3
The difficulties the professionals face for an integral care practice with an expanded look are mentioned in the statements. The increased demand, lack of time, few professionals, charge to achieve targets are indicated as factors that negatively affect the quality of care. Consequently, health promotion and disease prevention activities remain in the background in elderly care.
(...) population with some kind of health demand is covered today. But, for the active elderly, but without any kind of comorbidity, we do leave to be desired in care, right (...) We are unable to fully comply with the proposal of the family health program for the elderly population, due to the spontaneous demand, the lack of employees, due to various factors. (...) the demand we get in our routine is that big, (...) that we end up without addressing some specific populations (...) there's always something that ends up confusing us a bit. Being unable to stop and think of promotion activities, organizing groups." I-1
I try not to put them on the waiting list for adults, right. Because we prioritize the child in our work, up to 18 years, and pregnant women on an open agenda. And the adults, everyone over 18 years I put on a waiting list. (...) this age range is a very critical age range. Because most of these patients don't have teeth anymore. I-7
(...) promotion actions, mainly promotion and prevention too, they hardly happen and, when they do, it is very punctually, very individually. I-3
Medicalization also continues as the main practice in elderly care. There is difficulty to offer qualified listening, develop specific group activities, recognize the population that lives in the area, so that care is for elderly who participate in health programs. Each individual is responsible for recognizing the need for health care. Without health education practices, this acknowledgement happens very restrictedly.
(...) we are kind of left at the mercy of them perceiving that they need this care (...) of a different approach and them visiting us (...) approach them in general plus the patients in the health programs, those with comorbidities (...) I-5
We focus a lot on the medication issue, right. I-3
I think there's a lot missing. We still have a very medical view that is strongly focused on the disease. We are unable to work with prevention and promotion. I-6
Despite the difficulties faced, according to the activities developed at the Family Health Service, the professionals attempt to include the elderly in non-specific activities, open to the entire population.
At our service, we have the walking group, right, but that's not just aimed at the elderly. I-2
(...) there's the walking group, right, I think that's an opportunity. I think that's also a form of care, right, but a very punctual care, I don't even know if it can be called care, because I think it's a group that is becoming increasingly independent, (...) because of our difficulty to get it organized too. (...) there's the quality of life group, which is held there in the project (...) not necessarily for elderly too. (...) for elderly who are bedridden or somehow dependent there are visits, but always for a purpose too. I-3
There are some ladies who participate in the group of women too. And in the pain group now (...) there are some elderly women who've already got some health problems. I-6
CATEGORY 3: Integral care needs and perspectives
The professionals admit difficulties to approach elderly patients. They perceive the need for a care practice that covers the different spheres of care, such as education, health promotion and disease prevention, curative care, rehabilitation and health maintenance. The educative approaches are the most negatively affected in the current context.
I think that we could really do much more for the elderly, considering not only the population who is ill, but also those without any comorbidity and who come to the service less, right. I-1
I think there's a lot missing. We still have a very medical view that is strongly focused on the disease. We are unable to work with prevention and promotion. I-6
When they need to provide some orientation in accordance with the care plan, they turn to close persons, caregivers, adopting the perspective that these will be monitored. They attempt to get to know the elderly's support network, relationship with the family, their bonds in order to comply with the prescribed care.
We often need to contact a closer person at their home, or a caregiver to provide the orientations. I-2
(...) I try to perceive this elderly person's relation with the people at home, if he lives with someone, right. Some elderly live alone and then there's that thing who takes care of the elderly, who's the caregiver, what bond that elderly has beyond the family, with the community, with the neighborhood, if he participates in some other activity, if he attends a group, church or his contact with the health service. I-6
The professionals' statements reveal the barriers faced in care for the elderly, whether related to access, availability, knowledge or professional limits. These barriers can be considered challenging or frustrating for the professional who delivers care.
(...) there are some people whom we know have a problem, there is medication that would offer some benefit, but these people end up not getting this benefit because they have no financial conditions to be able to purchase this medication. I-2
And for me, like, as a psychologist, it demands effort to look at other issues beyond mental health with regard to the elderly, right. I-6
Thus, they look for strategies, spaces at the service that could be used better, training the professionals for expanded care, recycling their knowledge with new contents that emerge. The team meeting is a moment of exchange among the professionals, where all participants can present their opinions, knowledge, suggestions without judgment, where they take part to exchange knowledge. The productivity of this space does not only depend on the team's availability though, but also on the excessive number of information the management provides each week to transmit to the professionals.
The team meeting is a moment we can use, right, to plan care and we still have a long road to walk, you know?! (...) And I think that should be a concern not only for the service. I think we have to start, cause an impact in the managers too. I-3
DISCUSSION
As verified in the statements, the elderly are present at the Family Health service. It can be noted that most higher education professionals have taken or are taking a specialization program in Family Health.
These professionals' perception of elderly care is technical, based on health protocols and programs. They indicate that taking care means indicating specific programs, not mentioning general elderly health programs at any time, with preventive and curative practices. Great concern with care delivery to the ill is observed, through consultations, exams and medication. Hence, the subject's integrality is considered impaired. Taking care of the ill reinforces the traditional, biomedical model that still prevails at the health services. We need a new care form, with professionals who are willing to change, to break with this care model, defending individual and collective life in the framework of each person's social rights33. Viegas SMF, Penna CMM. A construção da integralidade no trabalho cotidiano da equipe saúde da família. Esc Anna Nery. 2013 jan-mar; 17(1):133-41..
The Family Health Strategy emerges to replace a health care model, in the attempt to assume an expanded concept of health. Its objective is to enhance the reorientation of the work process, breaking with the fragmentation of care. It is through the SUS guidelines, integrality, equity, universality, regionalization, decentralization, problem-solving ability and popular participation that the strategy is structured1111. Silveira CH. Falando de modelos de assistência à saúde e do programa de Saúde da Família do Ministério da Saúde - Brasil. Rev Inter Interdisc Interthesis. 2008 jan-jul; 5(1):78-103..
The care offered by SUS professionals should include care or curative actions, and also promote health and prevent illnesses. The abilities of the FHS range from the active search in the community to home visits and clinical monitoring of diagnosed cases, including medication supplies. Nevertheless, in the search for care integrality, health education activities, welcoming of the subject, teamwork with an interdisciplinary look should be present in the FHS team's routine. This corresponds to health surveillance, which proposes an activity within a given territory, working with the local health problems and intersectoriality. The goal is to break once again with the reductionist and fragmented approach. Care should go beyond the disease and the suffering, aiming for expanded approaches1212. Alves VS. Um modelo de educação em saúde para o Programa de Saúde da Família: pela integralidade da atenção e reorientação do modelo assistencial. Interface (Botucatu). 2004-2005 set-fev; 9(16):39-52..
Then, the Hiperdia program emerges as the elderly's link with the health service professional. Diabetes and hypertension are important pathologies that deserve appropriate care to avoid severe complications. But this does not mean that being elderly means being hypertensive and/or diabetic. The professional look based on these aspects is limited, which impairs the quality of life and successful aging of the 60-year-olds not included in the program.
A study undertaken in 2010 to get to know the perception of Family Health team professionals in the Brazilian Northeast about elderly care indicates that initiatives to develop the autonomy and socialization of elderly people are emerging, but remain very fragmented and isolated. Care is more centered on treatment and recovery, mainly in the demands of elderly people originating in Hiperdia1313. Alencar MSS, Leite ALI, Memoria SVF, Sousa JMS. Percepções dos profissionais da Saúde da Família a respeito da atenção a pessoa idosa em Teresina-PI. Rev Bras Geriatr Gerontol. 2010;13(3):475-86..
In the discourse, a punctual activity is identified, in a way imposed by the coordination, for care delivery to elderly people. Each year, the professionals get organized for elderly care, through the Municipal Week of the Elderly, offering a week filled with activities for those over 60 years of age.
We could think of a devaluation of this monitored patient, who visits the health service too frequently and needs care. An integral approach is a duty of the professionals and a right of the elderly, in response to the demands the elderly present.
The individualized consultation is the main instrument used. These are even more frequent when these elderly are included in health programs, in a reduced, protocoled, imposed manner. Welcoming, qualified listening, an expanded look and integrality are left aside in professional activities with the elderly.
When focusing on integrality and with a view to the construction of expanded clinics, the goal is, through the biopsychosocial, to consider these elderly in their singularity, and to develop individualized care plans based on their specific needs. The professionals reveal difficulties to put these concepts in practice, for many reasons, including the organization of the service, great care demand, compliance with targets/production, among others, which negatively affect the quality of care delivery.
The expanded clinic is a tool to articulate and include different situations. This clinic recognizes that, at a given time, some focus may be predominant, without this causing the denial of other approaches though. No disciplinary approaches are downgraded, thus aiming for integral, multiprofessional care management. The expanded clinic work with an expanded understanding of the health-disease process, a shared construction of diagnoses and treatments, the transformation of work with the ability to listen, to critically deal with automated conducts, to cope with social and subjective problems, with family and community1414. Ministério da Saúde (Brasil). Secretaria de atenção à saúde. Política nacional de Humanização da atenção e Gestão do SUS. Clínica ampliada e compartilhada. Brasília (DF): Ministério da Saúde; 2009..
A study undertaken in the FHS in Natal-RN shows that Family Health is capable of promoting changes in care practices, but that the lack of adherence and institutional support represents a threat to this practice1515. Araujo MBS, Rocha PM. Trabalho em equipe: um desafio para a consolidação da Estratégia de Saúde da Família. Ciênc Saúde Coletiva. 2007;12(2):455-64..
Hence, medicalization remains strong as the main care offered. We consider that, when used appropriately, medicines offer many benefits to people, but that we need to think of new alternatives that provide long-term benefits without causing dependence. Educative activities, individually or in group, qualified listening, socio-epidemiological knowledge of the activity area are strategies to expand health practices.
The professionals expect the elderly to come to them in search of care, with self-perceived health needs. As the population's education is still focused on curative care, leaving this responsibility to the mercy of the elderly is a very trifling and deficient attitude.
The autonomy of the health service users is an individual need. Health professionals are responsible for promoting increasing levels of autonomy in the subjects' way of life. Health education and information are part of this process. Being autonomous entails a possibility for the users to reconstruct the meanings of their life and this gains actual importance in their way of life, in the satisfaction of their needs, in the broadest possible sense1616. Cecilio LCO. As necessidades de saúde como conceito estruturante na luta pela integralidade e eqüidade na atenção. In: Pinheiro R, Mattos RA. Os sentidos da integralidade na atenção e no cuidado à saúde. Rio de Janeiro (RJ): ABRASCO; 2001. p.113-26..
In view of the lack of activities for the elderly, the professionals attempt to include these into the service routine, in practices that are taking place, mainly in group activities.
Once again, the professionals' perception of the difficulties faced in elderly care is observed. They refer to the importance of self-care through education, health promotion, prevention, curative care, rehabilitation and health maintenance. They always attempt to provide orientations in view of the elderly's support network, which strengthens this care. In addition, they are familiar with the family relations and established bonds. In fact, the data reveal difficulties in the professionals' awareness of these actions.
Not just the professional practices, whether these are restricted or expanded, influence care for the elderly. The professionals often feel frustrated when they know that there are specific care possibilities for a certain elderly person, which will benefit him/her and will offer a better quality of life, but end up being confronted with social issues, like the elderly's low income for example, or the prescription of medicines the health service does not provide.
The challenge the professionals face is to consider integrality articulated with other sectors, integrality as a focus in the work process. The reorganization of Primary Health Care with the FHS has allowed for more welcoming health units, offering high-quality care with greater problem-solving ability, despite all difficulties faced1717. Fracolli LA, Zoboli ELP, Granja GF, Ermel RC. Conceito e prática da integralidade na Atenção Básica: a percepção das enfermeiras. Rev Esc Enferm USP. out 201;45(5):1135-41..
The training the health professionals mention is an effective care strategy. Knowing how to use common spaces at the service, like the team meeting, for educational purpose, would benefit all stakeholders. The change in the care model derives from the professionals' education and training for elderly care, with a view to minimizing dependence and promoting autonomy, favoring old age with quality of life. Care delivery in accordance with the Statute of the Elderly will result in safe, ethical and high-quality care1818. Martins JJ, Schier J, Erdmann, Albuquerque GL. Políticas públicas de atenção à saúde do idoso: reflexão acerca da capacitação dos profissionais da saúde para o cuidado com o idoso. Rev Bras Geriatr Gerontol. 2007;10(3):371-82..
In a study published in 2007, the need for professional training for geriatric care is observed. This care is still new in the Brazilian context, perhaps because old age remains a new demographic form. Without professionals able to deliver elderly care, no integral, expanded care will be available at the health services. For the health policies to be put in practice, these workers need knowledge, as "new knowledge provokes new practices"1818. Martins JJ, Schier J, Erdmann, Albuquerque GL. Políticas públicas de atenção à saúde do idoso: reflexão acerca da capacitação dos profissionais da saúde para o cuidado com o idoso. Rev Bras Geriatr Gerontol. 2007;10(3):371-82..
Another author affirms that, even without proper elderly care training, the professionals make efforts to offer care in accordance with the SUS. A long road remains ahead in terms of actions for healthy aging, with changes in the health model and a focus on elderly people in the FHS1212. Alves VS. Um modelo de educação em saúde para o Programa de Saúde da Família: pela integralidade da atenção e reorientação do modelo assistencial. Interface (Botucatu). 2004-2005 set-fev; 9(16):39-52..
FINAL CONSIDERATIONS
This research process permitted the achievement of the established objectives, showing how elderly care has been delivered at the primary care level. It was also revealed that advancements are still needed in care for the elderly. The professionals acknowledge the increase in this population and, at the same time, the lack of preparation for care delivery. The biological, fragmented model remains very strong, representing a challenge for public health nowadays. It is a fact that service management directly influences care for the elderly. While there are charges to achieve targets, unprepared professionals, limited numbers of professionals at the services and high demands, it will be difficult to advance towards care integrality.
The professionals indicate that elderly people are not attended as a priority in the FHS, that there are punctual actions with a view to successful aging. The FHS and the National Elderly Health Policy can be considered new policies that are being implemented. Nevertheless, we are experiencing and monitoring this increase in elderly people at the health services. Strategies and actions need to be devised to absorb this demand.
Although this study comes with limitations, as it is descriptive and limited to a restricted population, indicates the need for health professionals to gain awareness of the senile aging process and plan care strategies at their units. Education is the starting point as, without knowledge, there is no movement towards change. In addition, it serves as an alert for managers and the State to urgently organize the care network for elderly people in the community, adapting the service supply to the demand presented by today's elderly, with growing numbers, and by future elderly with varying degrees of dependence and vulnerability.
REFERÊNCIAS
-
1Banco Mundial. Envelhecendo em um Brasil mais velho: implicações do envelhecimento populacional para o crescimento econômico, a redução da pobreza, as finanças públicas e a prestação de serviços. Washington: Banco Mundial; 2011.
-
2Instituto Brasileiro de Geografia e Estatistica. Indicadores sociodemográficos e de saúde no Brasil. Rio de Janeiro (RJ): Instituto Brasileiro de Geografia e Estatística; 2009.
-
3Viegas SMF, Penna CMM. A construção da integralidade no trabalho cotidiano da equipe saúde da família. Esc Anna Nery. 2013 jan-mar; 17(1):133-41.
-
4Portaria nº 399/ GM de 22 de fevereiro de 2006. Divulga o Pacto pela Saúde 2006 - Consolidação do SUS e aprova as Diretrizes Operacionais do Referido Pacto. Diário Oficial da República Federativa do, Brasília (DF), 23 fev 2006. Seção 1: 43.
-
5Portaria nº 2.528, de 19 de outubro de 2006. Política Nacional de Saúde da Pessoa Idosa. Diário Oficial da República Federativa do Brasil, Brasília (DF), 20 out 2006. Seção 1:142.
-
6Costa GD, Cotta RMM, Ferreira MLSM, Reis JR, Franceschini SCC. Saúde da família: desafios no processo de reorientação do modelo assistencial. REBEN. 2009 jan-fev; 62(1):113-8.
-
7Mattos RA. A integralidade na prática (ou sobre a prática da integralidade). Cad Saúde Pública. 2004 set-out; 20(5):1411-6.
-
8Wagner HTR. Sobre fenomenologia e relações sociais: Alfred Schütz. Petrópolis (RJ): Vozes; 2012.
-
9Capalbo C. Metodologia das ciências sociais: a fenomenologia de Alfred Schutz. Londrina (PR): UEL; 1998.
-
10Botucatu. Sistema de Informação do Município de Botucatu. Botucatu: CPDQ; 2013.
-
11Silveira CH. Falando de modelos de assistência à saúde e do programa de Saúde da Família do Ministério da Saúde - Brasil. Rev Inter Interdisc Interthesis. 2008 jan-jul; 5(1):78-103.
-
12Alves VS. Um modelo de educação em saúde para o Programa de Saúde da Família: pela integralidade da atenção e reorientação do modelo assistencial. Interface (Botucatu). 2004-2005 set-fev; 9(16):39-52.
-
13Alencar MSS, Leite ALI, Memoria SVF, Sousa JMS. Percepções dos profissionais da Saúde da Família a respeito da atenção a pessoa idosa em Teresina-PI. Rev Bras Geriatr Gerontol. 2010;13(3):475-86.
-
14Ministério da Saúde (Brasil). Secretaria de atenção à saúde. Política nacional de Humanização da atenção e Gestão do SUS. Clínica ampliada e compartilhada. Brasília (DF): Ministério da Saúde; 2009.
-
15Araujo MBS, Rocha PM. Trabalho em equipe: um desafio para a consolidação da Estratégia de Saúde da Família. Ciênc Saúde Coletiva. 2007;12(2):455-64.
-
16Cecilio LCO. As necessidades de saúde como conceito estruturante na luta pela integralidade e eqüidade na atenção. In: Pinheiro R, Mattos RA. Os sentidos da integralidade na atenção e no cuidado à saúde. Rio de Janeiro (RJ): ABRASCO; 2001. p.113-26.
-
17Fracolli LA, Zoboli ELP, Granja GF, Ermel RC. Conceito e prática da integralidade na Atenção Básica: a percepção das enfermeiras. Rev Esc Enferm USP. out 201;45(5):1135-41.
-
18Martins JJ, Schier J, Erdmann, Albuquerque GL. Políticas públicas de atenção à saúde do idoso: reflexão acerca da capacitação dos profissionais da saúde para o cuidado com o idoso. Rev Bras Geriatr Gerontol. 2007;10(3):371-82.
Publication Dates
-
Publication in this collection
Sep-Dec 2013
History
-
Received
22 Apr 2013 -
Reviewed
30 June 2013 -
Accepted
09 Aug 2013