ABSTRACT:
Objectives:
To retrospectively describe severe cases of hospitalized patients and deaths related to the COVID-19 epidemic in the state of São Paulo, starting from the date of the first record, with symptoms onset on 02/10/2020 up to 05/20/2021.
Methods:
This is a descriptive study carried out using the Influenza Epidemiological Surveillance System (Sistema de Vigilância Epidemiológica da Gripe - SIVEP-Gripe) database. The rates of incidence, mortality, and accumulated incidence in the period were calculated, stratified by age group and Regional Health Department (RHD). In addition, severe cases were geocoded to analyze their spread across the state; and the Effective R, which determines the spread potential of a virus within a population, was calculated.
Results:
There was a significant increase in severe cases and deaths recorded in the period of one year, with incidence and mortality rates being heterogeneous within the state. The most critical periods regarding the incidence of severe cases occurred between May and July 2020 and between March and April 2021. The RHD in São José do Rio Preto, Expanded São Paulo, and Araçatuba concentrated the highest incidence and mortality rates. Severe cases and deaths were more frequent in men and in the population over 60 years, while the main risk conditions related to deaths were heart disease (59%) and diabetes (42,8%).
Conclusions:
These results not only provide a detailed profile for more efficient control action plan, but will also allow the historical understanding of the COVID-19 evolution within the state of São Paulo.
Keywords:
SARS-CoV-2; Epidemics; Health strategies; Epidemiologic surveillance services
RESUMO:
Objetivo:
Descrever, de forma retrospectiva, os casos graves de pacientes hospitalizados e os óbitos relacionados à epidemia de COVID-19 no estado de São Paulo, desde a data do primeiro registro, com início de sintomas em 10 de fevereiro de 2020 até registros disponíveis em 20 de maio de 2021.
Métodos:
Trata-se de um estudo descritivo realizado por meio da base de dados do Sistema de Vigilância Epidemiológica da Gripe. Foram calculadas as taxas de incidência, mortalidade e incidência acumulada no período, estratificadas por faixa etária e agrupadas de acordo com cada Departamento Regional de Saúde. Os casos graves foram geocodificados para a análise de seu espalhamento pelo estado e foi calculado o R efetivo, que estima o potencial de propagação de um vírus em uma população.
Resultados:
Houve aumento significativo dos casos graves e óbitos registrados no período de um ano, e as taxas de incidência e mortalidade foram heterogêneas no estado. Os períodos mais críticos em relação à incidência de casos graves ocorreram entre maio e julho de 2020 e entre março e abril de 2021. Os Departamentos Regionais de Saúde de São José do Rio Preto, Grande São Paulo e Araçatuba concentraram as maiores taxas de incidência e mortalidade. Os casos graves e óbitos foram mais frequentes nos homens e na população acima de 60 anos, e as principais condições de risco relacionadas aos óbitos foram cardiopatia (59%) e diabetes (42,8%).
Conclusões:
Espera-se que esses resultados ofereçam embasamento e possam contribuir para uma ação de controle mais eficiente da COVID-19, além de permitir o entendimento histórico de sua evolução no estado.
Palavras-chave:
SARS-CoV-2; Epidemias; Estratégias de saúde; Vigilância epidemiológica
INTRODUCTION
On January 31st, 2020, the World Health Organization declared infection by the new coronavirus (SARS-CoV-2) a global emergency and named the disease COVID-1911. World Health Organization. Novel coronavirus (COVID-19) situation. Genebra: World Health Organization; 2020.. The clinical manifestation is similar to that of other respiratory viruses, with symptoms such as fever, usually dry cough, tiredness and, although in 80% of cases the symptoms are mild22. Strabelli TMV, Uip DE. COVID-19 e o coração. Arq Bras Cardiol 2020; 114 (4): 598-600. https://doi.org/10.36660/abc.20200209
https://doi.org/https://doi.org/10.36660...
, the more severe cases (5%) present symptoms such as dyspnea, pulmonary bleeding, severe lymphopenia, and renal failure. Several studies have shown that respiratory transmission represents the dominant route for the spread of the virus33. Zhang Z, Xue T, Jin X. Effects of meteorological conditions and air pollution on COVID-19 transmission: Evidence from 219 Chinese cities. Sci Total Environ 2020; 741: 140244. https://doi.org/10.1016/j.scitotenv.2020.140244
https://doi.org/https://doi.org/10.1016/...
, mainly through human-to-human diffusion44. Bontempi E, Vergalli S, Squazzoni F. Understanding COVID-19 diffusion requires an interdisciplinary, multi-dimensional approach. Environ Res 2020; 188: 109814. https://doi.org/10.1016/j.envres.2020
https://doi.org/https://doi.org/10.1016/...
. In particular, recent studies have also shown that, in addition to droplets generated by infected people, SARS-CoV-2 can also be transmitted by submicron aerosols55. Prather KA, Wang CC, Schooley RT. Reducing transmission of SARS-CoV-2. Science 2020; 368 (6498): 1422-4. https://doi.org/10.1126/science.abc6197
https://doi.org/https://doi.org/10.1126/...
in specific conditions, such as indoor environments. Due to their small size, aerosols can penetrate deeper into the lungs and, as a consequence, aggravate the disease66. Buonanno P, Galletta S, Puca M. Estimating the severity of COVID-19: evidence from the Italian epicenter. PLoS One 2020; 15 (10): e0239569. https://doi.org/10.1371/journal.pone.0239569
https://doi.org/https://doi.org/10.1371/...
.
The virus was first identified and reported in the city of Wuhan, China, in December 201977. Du Z, Xu X, Wu Y, Wang L, Cowling BJ, Meyers LA. The serial interval of COVID-19 from publicly reported confirmed cases. medRxiv 2020: 2020.02.19.20025452. https://doi.org/10.1101/2020.02.19.20025452
https://doi.org/https://doi.org/10.1101/...
, and it spread around the world in a short period of time. On April 26th, a few months after the epidemic began in China, around 3 million confirmed cases and 206,000 deaths had already been registered worldwide by COVID-1988. Souza WM, Buss LF, da Silva Candido D, Carrera JP, Zarebski AE, Faria NR. Epidemiological and clinical characteristics of the COVID-19 epidemic in Brazil. Nat Hum Behav 2020; 4 (8): 856-65. https://doi.org/10.1038/s41562-020-0928-4
https://doi.org/https://doi.org/10.1038/...
. Genomic sequencing and phylogenetic analysis indicated that it is a beta-coronavirus, of the same subgenus of the severe acute respiratory failure syndrome (SARS) that caused an epidemic in China in 2003 and of the Middle East respiratory syndrome (MERS), responsible for the same condition. in the Middle East in 201222. Strabelli TMV, Uip DE. COVID-19 e o coração. Arq Bras Cardiol 2020; 114 (4): 598-600. https://doi.org/10.36660/abc.20200209
https://doi.org/https://doi.org/10.36660...
. These last two viruses likely originated from bats and then infected other mammalian hosts - a civet (Paradoxurus hermaphroditus) for SARS-CoV and a dromedary (Camelus dromedarius) for MERS-CoV - before reaching humans. The dynamics of SARS-CoV-2 are currently unknown, but there is speculation that it is also of animal origin11. World Health Organization. Novel coronavirus (COVID-19) situation. Genebra: World Health Organization; 2020..
On February 26th, 2020, the Ministry of Health in Brazil confirmed the first case of COVID-19 in Latin America: a 61-year-old Brazilian man who traveled to Lombardy, northern Italy, where a significant outbreak was occurring9. He lived in the city of São Paulo and, since then, the state has become a major epicenter of the disease in Brazil. The aim of this study was to describe and evaluate the epidemiological aspects of severe cases of hospitalized patients and deaths from COVID-19 in the state of São Paulo, from the registration of the first case in February 2020 until May 20th, 2021, in order to provide a comprehensive update on key issues, which include: spatiotemporal evolution in municipalities, age group, gender, characteristics of deaths, and related comorbidities. It is hoped, therefore, that this material will serve as a baseline to address the challenges related to the COVID-19 pandemic and become a reference for future analysis and epidemics.
METHODS
For this descriptive and retrospective study in the state of São Paulo, only severe cases of hospitalized patients and deaths from SARS confirmed for COVID-19 were considered. By definition, SARS is considered to be a flu syndrome when an individual with flu-like illness presents dyspnea/respiratory discomfort, or persistent pressure or pain in the chest, or O2 saturation of less than 95% in room air, or a bluish color (cyanosis) of the lips or face1010. Brasil. Dados da COVID-19 [Internet]. 2021 [acessado em 3 maio 2021]. Disponível em: Disponível em: https://covid.saude.gov.br/
https://covid.saude.gov.br/...
. Data were obtained from the Influenza Epidemiological Surveillance System (Sistema de Vigilância Epidemiológica da Gripe - SIVEP-Gripe), which is the official system of the Ministry of Health of Brazil1010. Brasil. Dados da COVID-19 [Internet]. 2021 [acessado em 3 maio 2021]. Disponível em: Disponível em: https://covid.saude.gov.br/
https://covid.saude.gov.br/...
, for cases with onset of symptoms between February 10th, 2020 and May 20th, 2021. The geocoding of residence addresses of hospitalized patients in severe cases was performed using the HERE API application of the QGis software, version 3.10, and with the Hqgis complement, version 0.4.4. The coordinates of the cases and the radius of influence of 5 km were used to estimate the Kernel density in the state of São Paulo, through the splanc package of the R software (R Core Team, 2021). According to Article 1 of Resolution No. 510, of April 7th, 2016, this study does not require approval by the Ethics Committee.
As unit of analysis in space, the 645 municipalities of São Paulo and the 17 regions of the Regional Health Departments (RHD) of the State Department of Health were used. The estimated population obtained from the State Data Analysis System Foundation (SEADE) for 2020 was used to calculate the mortality rate (deaths/100,000 inhabitants). For regional mortality rates, deaths were considered by municipality of residence. Percentage, mean, median, and mode distributions were calculated according to the characteristics of the variables of interest, whether categorical or continuous. To calculate age-adjusted mortality rates, the world standard population proposed by Segi1111. Segi M, Fujisaku S. Cancer mortality for selected sites in 24 countries (1950-1957). Miyagi: Tohoku University School of Medicine; 1960. p. 130-45. and modified by Doll et al.1212. World Health Organization. Cancer incidence in five continents. A technical report. Genebra: World Health Organization ; 1966. was used. On the other hand, lethality considered the number of deaths by COVID-19 in the numerator and the number of cases of SARS COVID-19 in the denominator (multiplied by 100). For the construction of time series graphics (by RHD and by age group) and calculation of the effective R, the last two epidemiological weeks were disregarded, given the large number of cases characterized as “under investigation”, which in turn interfere on the trend shown in the graphic. Thus, only records comprised in the period between February 10th, 2020 and May 1st, 2021 were considered. The effective number of reproduction R or effective R was calculated using the EpiEstim package of the R software (R Core Team, 2021). This value allows us to estimate the potential for the spread of a virus in a population under certain conditions, acting as a proxy for the spread of the virus.
RESULTS
TIME AND SPACE EVOLUTION
Since the beginning of the COVID-19 epidemic in São Paulo, in February 2020 until May 20th, 2021, 366,802 cases of SARS were confirmed for COVID-19, including 106,437 deaths in the state of São Paulo (Figure 1). The highest record in the number of new confirmed SARS COVID-19 cases in a single day (3,209 cases) occurred on March 10th, 2021, by symptom onset date; while the highest number of deaths registered in 24 hours (1,389) occurred on April 6th, 2021. Accumulated incidence and mortality for the state were 858.56 and 259.10 per 100,000 inhabitants, respectively. However, over the epidemiological weeks (EW) from 2020 to EW 20, 2021, the numbers of serious cases and new deaths related to COVID-19 were heterogeneous among the different regions of the state. Figure 1B shows the six RHD with the highest incidence and mortality rates in the analyzed period. The highest cumulative incidences (per 100,000 inhabitants) were observed in the RHD of São José do Rio Preto (1,187.3) and Expanded São Paulo (954), while the highest accumulated mortality rates (per 100,000 inhabitants) were also verified in São José do Rio Preto (352.9) and in Araçatuba (301.7).
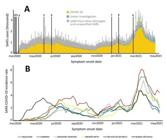
A) Temporal evolution of the number of severe cases of COVID-19 in the state of São Paulo and the main events: (1) February 26th: release of the first confirmed case of COVID-19 in Brazil; (2) March 12th: São Paulo registers community broadcasting; (3) March 12th: first confirmed death by COVID-19; (4) the government of SP state decrees quarantine; (5) June 1st: São Paulo Plan takes effect and trade is authorized in the capital; (6) July 6th: relaxation of isolation measures in some municipalities in the state; (7) January 4th: notification of first two confirmed cases of the new P1 variant in SP; (8) January 17th: start of vaccination in SP; (9) February 26th: restriction of the movement of people and new isolation measures. B) Evolution of gross incidence rates of severe acute respiratory syndrome by COVID-19 over epidemiological weeks per Regional Health Department and per 100,000 inhabitants. Symptom onset period between February 10th, 2020 and May 1st, 2021.
Regarding the spread of the disease, it is noted that the initial hotspot was the Expanded São Paulo region and, over the months, the cases progressed toward the interior of the state (Figure 2), and that the dispersion coincided with the main state highways. Currently, the Expanded São Paulo region still concentrates the absolute majority of severe cases and deaths.
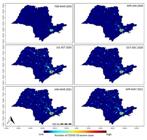
Spatial evolution of the number of cases of severe acute respiratory syndrome by COVID-19 according to place of residence, state of São Paulo. Symptom onset period between February 10th, 2020 and May 20th, 2021.
AGE RANGE AND GENDER
During the analyzed period, it was possible to observe that the numbers of hospitalizations and deaths were higher for men: 55.74% of hospitalized patients (204,440) and 56.4% of deaths (60,036) were male. The lethality among the cases of SARS COVID-19 was similar in men and women: 29.3 and 28.6%, respectively. In addition, a change in the pattern by age group can be identified from January 2021, with an increase among young people (> 20 years) and a resurgence in the longest-lived aged population (> 80 years) (Figure 3A). Considering both gender, the mean age of hospitalized patients was 58.3 years and the mean age of death was 67.1 years. Of the total number of deaths observed in the period (106,437), most occurred in male patients aged between 60 and 79 years (Figure 3B). Analyzing the time series (Figure 4), it was possible to observe two epidemic peaks of COVID-19. Throughout the entire time series, the oldest age group (> 80 years) was the most affected. It is worth noting that the number of deaths in young patients, aged between 20 and 39 years, has increased: only in the first five months of 2021 the deaths in this group almost doubled those registered in 2020 (Figure 3B).
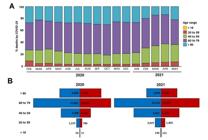
A) Deaths from severe acute respiratory syndrome by COVID-19 by age group and month of symptom onset. Symptom onset period between February 10th, 2020 and May 20th, 2021. The numbers represent the proportion of deaths in each age group. *The month of May 2021 is incomplete and there are still several cases without a completed outcome. B) Distribution of deaths by gender and age group in the state of São Paulo. 2020: period of symptom onset between February 10th, 2020 and December 31st, 2020. 2021: period of symptom onset between January 1st, 2021 and May 20th, 2021.

Time series of crude incidence (A) and mortality (B) rates of severe acute respiratory syndrome by COVID-19 by age group in the state of São Paulo. Symptom onset period between February 10th, 2020 and May 1st, 2021.
DEATHS
Among the deaths, 79,652 (74.8%) have registered one or more risk conditions, with a predominance of heart disease (59%) and diabetes (42.8%), followed by neuropathy (8.5%), obesity (12%), nephropathy (7.7%), pneumopathy (6.8%), and immunosuppression (4.5%). Of the 106,437 confirmed deaths in the state of São Paulo, 54.2% used the Intensive Care Unit (ICU) and, of these, 63.4% used invasive ventilatory support, 27.7% used noninvasive ventilatory support, and 8.9% did not use them. Until the end of 2020, the average ICU stay of patients with SARS COVID-19 who died was 14 days, but this scenario has changed in recent months. Considering only the first five months of 2021, the estimated time for a person to evolve to death after being admitted to the ICU decreased to 11 days. The absolute majority of patients who died lived in Expanded São Paulo (53,791), but the highest accumulated mortality in the period was observed in the RHD of São José do Rio Preto (352.9).
EFFECTIVE R
It was possible to observe that the effective R of COVID-19 in the state of São Paulo remained relatively stable over time (Figure 5), with values above 1 in periods of peak disease or positive variation. This estimated value over time can tell you how critical the current stage of an epidemic is.

Estimate of the effective R in the state of São Paulo for the period between April 1st, 2020 and May 1st, 2021. *CI: confidence interval.
DISCUSSION
In the period considered, there was a large burden of serious cases and deaths from COVID-19 in the state of São Paulo, with the occurrence of two main epidemic peaks between May and July 2020 and March and April 2021. Cases and deaths were more frequent in men and in the population over 60 years of age in 2020, and in 2021 there is an increase in deaths in the young population (20 to 39 years of age). The main risk conditions related to death were heart disease (59%) and diabetes (42.8%). The initial hotspot was the Expanded São Paulo region and, over the months, the cases were advancing to the interior of the state in a fast and continuous way, with the increasing incidence of severe cases hospitalized in the municipalities. The RHD in São José do Rio Preto, Expanded São Paulo and Araçatuba concentrated the highest rates of incidence and mortality.
The partial adherence to social isolation observed in São Paulo can still be considered as a factor that may have contributed to the increase in cases. State government data show that, during the period of this study, the average social isolation index ranged from 39 to 59%, with greater adherence to Sundays and holidays1313. Brasil. Governo do Estado de São Paulo. Dados do isolamento social [Internet]. 2021 [acessado em 3 maio 2021]. Disponível em: Disponível em: https://www.saopaulo.sp.gov.br/coronavirus/isolamento/
https://www.saopaulo.sp.gov.br/coronavir...
. Studies show that the level of adherence to isolation depends on several factors1414. Nussbaumer-Streit B, Mayr V, Dobrescu AI, Chapman A, Persad E, Klerings I, et al. Quarantine alone or in combination with other public health measures to control COVID-19: a rapid review. Cochrane Database Syst Rev 2020; 9 (9): CD013574. https://doi.org/10.1002/14651858.CD013574.pub2
https://doi.org/https://doi.org/10.1002/...
, especially the socioeconomic and the number of residents per household1515. van Oosterhout C, Hall N, Ly H, Tyler KM. COVID-19 evolution during the pandemic - Implications of new SARS-CoV-2 variants on disease control and public health policies. Virulence. 2021; 12 (1): 507-8. https://doi.org/10.1080/21505594.2021.1877066
https://doi.org/https://doi.org/10.1080/...
,1616. Bezerra ACV, Silva CEMD, Soares FRG, Silva JAMD. Factors associated with people’s behavior in social isolation during the COVID-19 pandemic. Cien Saude Colet. 2020; 25 (suppl 1): 2411-21. https://doi.org/10.1590/1413-81232020256.1.10792020
https://doi.org/https://doi.org/10.1590/...
. The quality of housing is another important factor to be considered, as the state of São Paulo is very diverse and with very unequal living conditions; therefore, the comfort and structure of this space can make a big difference in whether or not to adhere to insulation. Research in the United Kingdom showed that people with lower income were three times less likely to practice isolation1717. Atchison CJ, Bowman L, Vrinten C, Redd R, Pristera P, Eaton JW, et al. Perceptions and behavioural responses of the general public during the COVID-19 pandemic: A cross-sectional survey of UK Adults. MedRxiv 2020: 20050039. https://doi.org/10.1101/2020.04.01.20050039
https://doi.org/https://doi.org/10.1101/...
, especially due to the type of work performed1616. Bezerra ACV, Silva CEMD, Soares FRG, Silva JAMD. Factors associated with people’s behavior in social isolation during the COVID-19 pandemic. Cien Saude Colet. 2020; 25 (suppl 1): 2411-21. https://doi.org/10.1590/1413-81232020256.1.10792020
https://doi.org/https://doi.org/10.1590/...
.
The aged population represents one of the groups most prone to severe cases and deaths from COVID-19 in the state of São Paulo. The highest lethality occurred in patients over 80 years of age (53%), similar to data from China and the United States11. World Health Organization. Novel coronavirus (COVID-19) situation. Genebra: World Health Organization; 2020.. Recently, Souza et al.88. Souza WM, Buss LF, da Silva Candido D, Carrera JP, Zarebski AE, Faria NR. Epidemiological and clinical characteristics of the COVID-19 epidemic in Brazil. Nat Hum Behav 2020; 4 (8): 856-65. https://doi.org/10.1038/s41562-020-0928-4
https://doi.org/https://doi.org/10.1038/...
analyzed the Brazilian population and found that most deaths from COVID-19 were in men and that the most frequent comorbidities were cardiovascular diseases and diabetes - similar data to those found in this study. Behavioral factors, education, especially social status, which can impair adherence to isolation measures, proved to be potentially crucial in determining susceptibility to SARS-CoV-21818. Pawlowski B, Atwal R, Dunbar RIM. Sex differences in everyday risk-taking behavior in humans. Evol Psychol 2008; 6 (1): 29-42. https://doi.org/10.1177/147470490800600104
https://doi.org/https://doi.org/10.1177/...
,1919. Raisi-Estabragh Z, McCracken C, Bethell MS, Cooper J, Cooper C, Caulfield MJ, et al. Greater risk of severe COVID-19 in Black, Asian and Minority Ethnic populations is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: study of 1326 cases from the UK Biobank. J Public Health (Oxf) 2020; 42 (3): 451-60. https://doi.org/10.1093/pubmed/fdaa095
https://doi.org/https://doi.org/10.1093/...
. This relatively unequal incidence and mortality in men can be interpreted considering many factors: the comparatively higher prevalence of comorbidities (hypertension, diabetes, cardiovascular diseases, and chronic lung diseases)2020. Sharma G, Volgman AS, Michos ED. Sex differences in mortality from COVID-19 pandemic: are men vulnerable and women protected? JACC Case Rep 2020; 2 (9): 1407-10. https://doi.org/10.1016/j.jaccas.2020.04.027
https://doi.org/https://doi.org/10.1016/...
, more risk behaviors (smoking and alcohol use), occupational exposure2121. Global Health 5050. COVID-19 sex-disaggregated data tracker. África: Global Health 5050; 2020., and gender differences in immune responses2222. Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol 2016; 16 (10): 626-38. https://doi.org/10.1038/nri.2016.90
https://doi.org/https://doi.org/10.1038/...
. However, there may be other social and behavioral characteristics that favor women, as reported in previous studies2323. Johnson HD, Sholcosky D, Gabello K, Ragni R, Ogonosky N. Sex differences in public restroom handwashing behavior associated with visual behavior prompts. Percept Mot Skills 2003; 97 (3 Pt 1): 805-10. https://doi.org/10.2466/pms.2003.97.3.805
https://doi.org/https://doi.org/10.2466/...
,2424. Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Gender differences in the utilization of health care services. J Fam Pract 2000; 49 (2): 147-52. PMID: 10718692, suggesting that they are more likely to adopt hand hygiene practices2323. Johnson HD, Sholcosky D, Gabello K, Ragni R, Ogonosky N. Sex differences in public restroom handwashing behavior associated with visual behavior prompts. Percept Mot Skills 2003; 97 (3 Pt 1): 805-10. https://doi.org/10.2466/pms.2003.97.3.805
https://doi.org/https://doi.org/10.2466/...
and to seek more preventive/assistance care2424. Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Gender differences in the utilization of health care services. J Fam Pract 2000; 49 (2): 147-52. PMID: 10718692 when compared to men. Furthermore, it is necessary to highlight that mortality from COVID-19 can be determined by the intrinsic characteristics of infected individuals (age, previous diseases, lifestyle habits)2525. Feng Y, Ling Y, Bai T, Xie Y, Huang J, Li J, et al. COVID-19 with different severities: a multicenter study of clinical features. Am J Respir Crit Care Med 2020; 201 (11): 1380-8. https://doi.org/10.1164/rccm.202002-0445OC
https://doi.org/https://doi.org/10.1164/...
and also by issues related to care, such as the difficulty in accessing health services due to the overload of care and/or the lack of therapeutic resources (hospital beds, health teams, ventilators, and medications).
The distribution of the number of serious cases and deaths of COVID-19 was heterogeneous in the state, and the highest cumulative incidences were observed in the RHD of São José do Rio Preto and Expanded São Paulo, while the highest mortality rates were also observed in São José do Rio Preto and Araçatuba. It is important to emphasize that these regions represent economic centers of the state and concentrate large assistance infrastructures, which probably provide the demand in neighboring areas for health equipment with greater resoluteness. This was also evidenced by observing the incidence rates by municipality of residence, in which the formation of spatial clusters in the RHD of São José do Rio Preto and Expanded São Paulo was noted.
Multiple factors may be associated with this spatial inequality, such as the susceptibility of individuals to the virus, the prevalence of comorbidities in the population, and risk behaviors. The population characteristics related to COVID-19 are still poorly studied in the literature. Some studies, such as the one carried out by the World Health Organization11. World Health Organization. Novel coronavirus (COVID-19) situation. Genebra: World Health Organization; 2020., show a higher rate of transmission in regions with a higher population concentration. In addition, the Ministry of Health generally proposes that certain outbreaks in areas of high population density are more likely to spread and thus represent events with the potential to have a major impact on public health1010. Brasil. Dados da COVID-19 [Internet]. 2021 [acessado em 3 maio 2021]. Disponível em: Disponível em: https://covid.saude.gov.br/
https://covid.saude.gov.br/...
. Another mapping and spatial analysis study carried out in China2626. Zaslavsky R, Goulart BNGD. Migração pendular e atenção à saúde na região de fronteira. Cien Saude Colet. 2017; 22 (12): 3981-6. https://doi.org/10.1590/1413-812320172212.03522016
https://doi.org/https://doi.org/10.1590/...
showed that the distribution of COVID-19 cases was not random. The points of concentration of cases, at the beginning of the epidemic, were restricted to areas of greater economic development and population density. These factors are related to the greater number of cases, as they provide greater commuting mobility, greater number of trips, and a greater number of health establishments qualified to provide care and diagnosis2626. Zaslavsky R, Goulart BNGD. Migração pendular e atenção à saúde na região de fronteira. Cien Saude Colet. 2017; 22 (12): 3981-6. https://doi.org/10.1590/1413-812320172212.03522016
https://doi.org/https://doi.org/10.1590/...
.
It is particularly important to monitor the spread of the disease in the state of São Paulo, the most populous Brazilian state, with 44.3 million inhabitants and an intense flow of people on national and international routes. The results presented here show that the spread and interiorization of the disease in the state followed the main existing state highways. The cities of São Paulo are marked by huge socio-spatial disparities, with clear elements of peripheralization arising from the class cut that marks the national space. Mainly the medium and large municipalities (> 100,000 inhabitants) have higher demographic densities, verticalization, capillary and internalized transport networks, slums, absent or precarious water and sewage networks in part of the cities, adding elements that contribute to the spread of COVID -192727. Barrozo LV, Serafim MB, Moraes SL, Mansur G. Monitoramento espaço-temporal das áreas de alto risco de COVID-19 nos municípios do Brasil. Hygeia 2020; 43 (2): 417-25. http://doi.org/10.14393/Hygeia0054547
https://doi.org/http://doi.org/10.14393/...
.
It was noted that, from January 2021, there was a decrease in deaths among aged individuals over 80 years old and an increase in deaths in the younger population (20 to 59 years of age). The vaccination campaign aimed at aged people began in the state of São Paulo on January 17th, 2021, which may be related with the decrease in deaths in this age group, even in the short term. Studies have shown that just the first dose of the AstraZeneca vaccine, for example, already confers high protection against severe symptoms and deaths from COVID-192828. Bernal JL, Andrews N, Gower C, Robertson C, Stowe J, Tessier E, et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. BMJ 2021; 373: n1088. https://doi.org/10.1136/bmj.n1088
https://doi.org/https://doi.org/10.1136/...
. The emergence of new variants, mainly P1 (Brazilian variant originated in Manaus) may also have some relationship with this change in pattern in recent months. The very characteristics of the etiologic agent can contribute to the spread or severity of cases, due to its ability to mutate and interact among species. According to the epidemiological bulletin of Instituto Adolfo Lutz2929. Instituto Adolfo Lutz. Monitoramento das linhagens do SARS-CoV-2 nas regiões de saúde do estado de São Paulo. Ceara: Instituto Adolfo Lutz; 2021., almost half (45.9%) of the samples tested in Expanded São Paulo between January and February 2021 are of the new P1 variant, while in other municipalities, such as Araraquara, it already represents the majority of the tested samples (59.26%) in the same period. Studies have observed that this new variant could change the COVID-19 mortality pattern among age groups, as well as change its pathogenicity and virulence profile3030. Freitas ARR, Giovanetti M, Alcantara LCJ. Variantes emergentes do SARS-CoV-2 e suas implicações na saúde coletiva. Inter Amn J Med Health. 2021; 3 (1): 4-10. https://doi.org/10.31005/iajmh.v4i.181
https://doi.org/https://doi.org/10.31005...
.
The profile of severe cases and deaths from COVID-19 described in this study is similar to that found in other countries11. World Health Organization. Novel coronavirus (COVID-19) situation. Genebra: World Health Organization; 2020.,3131. The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. Vital surveillances: the epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)-China, 2020. China CDC Weekly 2020, 2 (8): 113-22. https://doi.org/10.31005/iajmh.v4i.181
https://doi.org/https://doi.org/10.31005...
and Brazilian states88. Souza WM, Buss LF, da Silva Candido D, Carrera JP, Zarebski AE, Faria NR. Epidemiological and clinical characteristics of the COVID-19 epidemic in Brazil. Nat Hum Behav 2020; 4 (8): 856-65. https://doi.org/10.1038/s41562-020-0928-4
https://doi.org/https://doi.org/10.1038/...
,3232. Castro MC, Kim S, Barberia L, Ribeiro AF, Gurzenda S, Ribeiro KB, et al. Spatiotemporal pattern of COVID-19 spread in Brazil. Science 2021; 372 (6544): 821-6. https://doi.org/10.1126/science.abh1558
https://doi.org/https://doi.org/10.1126/...
,3333. Araújo AAC, Amaral JV, Sousa JN, Fonseca MCS, Viana CDMC, Mendes PHM, et al. COVID-19: analysis of confirmed cases in Teresina, Piaui, Brazil. Rev Prev Infecç. Saúde 2020; 6 (3): 2-8. https://doi.org/10.1590/SciELOPreprints.465
https://doi.org/https://doi.org/10.1590/...
. There were fewer records in young individuals between 0 and 19 years, similarly to the results found by Araújo et al.3333. Araújo AAC, Amaral JV, Sousa JN, Fonseca MCS, Viana CDMC, Mendes PHM, et al. COVID-19: analysis of confirmed cases in Teresina, Piaui, Brazil. Rev Prev Infecç. Saúde 2020; 6 (3): 2-8. https://doi.org/10.1590/SciELOPreprints.465
https://doi.org/https://doi.org/10.1590/...
in Teresina, Piauí, and to the Data Analysis Centers for Disease Control and Prevention (CDC)3131. The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. Vital surveillances: the epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)-China, 2020. China CDC Weekly 2020, 2 (8): 113-22. https://doi.org/10.31005/iajmh.v4i.181
https://doi.org/https://doi.org/10.31005...
in the Chinese cities of Huabei and Wuhan. In this study, it was noted that the comorbidities most associated with death were heart disease (59%) and diabetes (42.8%), corroborating the findings of Cupertino et al.3434. Cupertino MC, Cupertino GA, Gomes AP, Mayers NA, Siqueira-Batista R. COVID-19 in Brazil: epidemiological update and perspectives. Asian Pac J Trop Med 2020; 13 (5): 193-6. https://doi.org/10.4103/1995-7645.282215
https://doi.org/https://doi.org/10.4103/...
in the Brazilian territory. The speed of the spread of COVID-19 and its movement of interiorization in the state of São Paulo occurred in a similar way to that found by Castro et al.3232. Castro MC, Kim S, Barberia L, Ribeiro AF, Gurzenda S, Ribeiro KB, et al. Spatiotemporal pattern of COVID-19 spread in Brazil. Science 2021; 372 (6544): 821-6. https://doi.org/10.1126/science.abh1558
https://doi.org/https://doi.org/10.1126/...
. Regions such as the state of São Paulo, which have particular social, geographic, and economic characteristics, may reveal their own pattern of dissemination of COVID-19, which makes it interesting and necessary to continuously and rigorously monitor the epidemiological profile of cases and deaths. In this sense, there is no single solution for the entire country, but public health policies must observe regional singularities.
It is important to mention the strengths and weaknesses of this study. Regarding limitations, the main highlight is the use only of severe cases of hospitalization, which does not portray the reality of SARS-CoV-2 in the infected population as a whole, including asymptomatic ones. Still, the data presented here are consistent with the literature. The differences in mortality observed in some RHD in the two epidemic peaks may be related to the availability of beds in the ICU and not singularly to the lethality attributable to the new variants, which was not possible to measure here. Another variable that was not considered in this study was the vaccination coverage of age groups in 2021, which could bias the conclusions about deaths at different ages. Among the strengths, it is worth noting that only confirmed cases of COVID-19 were used, followed since its appearance in Brazil until today, in addition to data from SIVEP-Gripe.
The COVID-19 pandemic represents one of the most challenging and worrisome public health crises of this generation. There is a need for constant monitoring of cases and deaths, as well as the development of a multidisciplinary approach in view of the wide spectrum of systemic manifestations arising from COVID-19. Many uncertainties remain regarding the virus-host interaction and the evolution of the pandemic. Currently, therapeutic strategies to deal with the infection are of limited support, until scientific evidence materializes, and prevention aimed at reducing transmission in the community is the most concrete strategy, as vaccines are not yet available in sufficient quantity with a view to the expected effectiveness. However, we have here a temporal profile of how the virus is responding in different regional and population profiles. It is expected that the start and course of the vaccination campaign, especially in the groups prioritized so far (aged people, patients with comorbidities, and health professionals) represent the predictable impact with the decrease in severe cases and deaths in the medium term, thus modifying the current pandemic scenario.
Finally, the evidence presented in this study may be useful in formulating grounded hypotheses for the development of strategic public policies and, therefore, in the application of more assertive control actions in the most vulnerable regions and age groups. The panorama shown here will certainly favor not only the control bodies in the current situation, but will also contribute to the realization of a quick response to this and future pandemics, in addition to allowing the understanding and historical record of its spread.
ACKNOWLEDGMENTS
To the technicians of the Division of Respiratory Transmission Diseases/CVE/CCD/SES-SP for their collaboration and support throughout the work process; institutions linked to the State Department of Health (Coordination of Disease Control, Center for Epidemiological Surveillance, Instituto Adolfo Lutz, Epidemiological Surveillance Groups) and Municipal Health Secretariats, notably in the areas of surveillance, immunization, assistance, and laboratory.
REFERÊNCIAS
-
1World Health Organization. Novel coronavirus (COVID-19) situation. Genebra: World Health Organization; 2020.
-
2Strabelli TMV, Uip DE. COVID-19 e o coração. Arq Bras Cardiol 2020; 114 (4): 598-600. https://doi.org/10.36660/abc.20200209
» https://doi.org/https://doi.org/10.36660/abc.20200209 -
3Zhang Z, Xue T, Jin X. Effects of meteorological conditions and air pollution on COVID-19 transmission: Evidence from 219 Chinese cities. Sci Total Environ 2020; 741: 140244. https://doi.org/10.1016/j.scitotenv.2020.140244
» https://doi.org/https://doi.org/10.1016/j.scitotenv.2020.140244 -
4Bontempi E, Vergalli S, Squazzoni F. Understanding COVID-19 diffusion requires an interdisciplinary, multi-dimensional approach. Environ Res 2020; 188: 109814. https://doi.org/10.1016/j.envres.2020
» https://doi.org/https://doi.org/10.1016/j.envres.2020 -
5Prather KA, Wang CC, Schooley RT. Reducing transmission of SARS-CoV-2. Science 2020; 368 (6498): 1422-4. https://doi.org/10.1126/science.abc6197
» https://doi.org/https://doi.org/10.1126/science.abc6197 -
6Buonanno P, Galletta S, Puca M. Estimating the severity of COVID-19: evidence from the Italian epicenter. PLoS One 2020; 15 (10): e0239569. https://doi.org/10.1371/journal.pone.0239569
» https://doi.org/https://doi.org/10.1371/journal.pone.0239569 -
7Du Z, Xu X, Wu Y, Wang L, Cowling BJ, Meyers LA. The serial interval of COVID-19 from publicly reported confirmed cases. medRxiv 2020: 2020.02.19.20025452. https://doi.org/10.1101/2020.02.19.20025452
» https://doi.org/https://doi.org/10.1101/2020.02.19.20025452 -
8Souza WM, Buss LF, da Silva Candido D, Carrera JP, Zarebski AE, Faria NR. Epidemiological and clinical characteristics of the COVID-19 epidemic in Brazil. Nat Hum Behav 2020; 4 (8): 856-65. https://doi.org/10.1038/s41562-020-0928-4
» https://doi.org/https://doi.org/10.1038/s41562-020-0928-4 -
9Rodriguez-Morales AJ, Gallego V, Escalera-Antezana JP, Méndez CA, Zambrano LI, Franco-Paredes C, Cimerman S. COVID-19 in Latin America: The implications of the first confirmed case in Brazil. Travel Med Infect Dis 2020; 35: 101613. https://doi.org/10.1016/j.tmaid.2020.101613
» https://doi.org/https://doi.org/10.1016/j.tmaid.2020.101613 -
10Brasil. Dados da COVID-19 [Internet]. 2021 [acessado em 3 maio 2021]. Disponível em: Disponível em: https://covid.saude.gov.br/
» https://covid.saude.gov.br/ -
11Segi M, Fujisaku S. Cancer mortality for selected sites in 24 countries (1950-1957). Miyagi: Tohoku University School of Medicine; 1960. p. 130-45.
-
12World Health Organization. Cancer incidence in five continents. A technical report. Genebra: World Health Organization ; 1966.
-
13Brasil. Governo do Estado de São Paulo. Dados do isolamento social [Internet]. 2021 [acessado em 3 maio 2021]. Disponível em: Disponível em: https://www.saopaulo.sp.gov.br/coronavirus/isolamento/
» https://www.saopaulo.sp.gov.br/coronavirus/isolamento/ -
14Nussbaumer-Streit B, Mayr V, Dobrescu AI, Chapman A, Persad E, Klerings I, et al. Quarantine alone or in combination with other public health measures to control COVID-19: a rapid review. Cochrane Database Syst Rev 2020; 9 (9): CD013574. https://doi.org/10.1002/14651858.CD013574.pub2
» https://doi.org/https://doi.org/10.1002/14651858.CD013574.pub2 -
15van Oosterhout C, Hall N, Ly H, Tyler KM. COVID-19 evolution during the pandemic - Implications of new SARS-CoV-2 variants on disease control and public health policies. Virulence. 2021; 12 (1): 507-8. https://doi.org/10.1080/21505594.2021.1877066
» https://doi.org/https://doi.org/10.1080/21505594.2021.1877066 -
16Bezerra ACV, Silva CEMD, Soares FRG, Silva JAMD. Factors associated with people’s behavior in social isolation during the COVID-19 pandemic. Cien Saude Colet. 2020; 25 (suppl 1): 2411-21. https://doi.org/10.1590/1413-81232020256.1.10792020
» https://doi.org/https://doi.org/10.1590/1413-81232020256.1.10792020 -
17Atchison CJ, Bowman L, Vrinten C, Redd R, Pristera P, Eaton JW, et al. Perceptions and behavioural responses of the general public during the COVID-19 pandemic: A cross-sectional survey of UK Adults. MedRxiv 2020: 20050039. https://doi.org/10.1101/2020.04.01.20050039
» https://doi.org/https://doi.org/10.1101/2020.04.01.20050039 -
18Pawlowski B, Atwal R, Dunbar RIM. Sex differences in everyday risk-taking behavior in humans. Evol Psychol 2008; 6 (1): 29-42. https://doi.org/10.1177/147470490800600104
» https://doi.org/https://doi.org/10.1177/147470490800600104 -
19Raisi-Estabragh Z, McCracken C, Bethell MS, Cooper J, Cooper C, Caulfield MJ, et al. Greater risk of severe COVID-19 in Black, Asian and Minority Ethnic populations is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: study of 1326 cases from the UK Biobank. J Public Health (Oxf) 2020; 42 (3): 451-60. https://doi.org/10.1093/pubmed/fdaa095
» https://doi.org/https://doi.org/10.1093/pubmed/fdaa095 -
20Sharma G, Volgman AS, Michos ED. Sex differences in mortality from COVID-19 pandemic: are men vulnerable and women protected? JACC Case Rep 2020; 2 (9): 1407-10. https://doi.org/10.1016/j.jaccas.2020.04.027
» https://doi.org/https://doi.org/10.1016/j.jaccas.2020.04.027 -
21Global Health 5050. COVID-19 sex-disaggregated data tracker. África: Global Health 5050; 2020.
-
22Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol 2016; 16 (10): 626-38. https://doi.org/10.1038/nri.2016.90
» https://doi.org/https://doi.org/10.1038/nri.2016.90 -
23Johnson HD, Sholcosky D, Gabello K, Ragni R, Ogonosky N. Sex differences in public restroom handwashing behavior associated with visual behavior prompts. Percept Mot Skills 2003; 97 (3 Pt 1): 805-10. https://doi.org/10.2466/pms.2003.97.3.805
» https://doi.org/https://doi.org/10.2466/pms.2003.97.3.805 -
24Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Gender differences in the utilization of health care services. J Fam Pract 2000; 49 (2): 147-52. PMID: 10718692
-
25Feng Y, Ling Y, Bai T, Xie Y, Huang J, Li J, et al. COVID-19 with different severities: a multicenter study of clinical features. Am J Respir Crit Care Med 2020; 201 (11): 1380-8. https://doi.org/10.1164/rccm.202002-0445OC
» https://doi.org/https://doi.org/10.1164/rccm.202002-0445OC -
26Zaslavsky R, Goulart BNGD. Migração pendular e atenção à saúde na região de fronteira. Cien Saude Colet. 2017; 22 (12): 3981-6. https://doi.org/10.1590/1413-812320172212.03522016
» https://doi.org/https://doi.org/10.1590/1413-812320172212.03522016 -
27Barrozo LV, Serafim MB, Moraes SL, Mansur G. Monitoramento espaço-temporal das áreas de alto risco de COVID-19 nos municípios do Brasil. Hygeia 2020; 43 (2): 417-25. http://doi.org/10.14393/Hygeia0054547
» https://doi.org/http://doi.org/10.14393/Hygeia0054547 -
28Bernal JL, Andrews N, Gower C, Robertson C, Stowe J, Tessier E, et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. BMJ 2021; 373: n1088. https://doi.org/10.1136/bmj.n1088
» https://doi.org/https://doi.org/10.1136/bmj.n1088 -
29Instituto Adolfo Lutz. Monitoramento das linhagens do SARS-CoV-2 nas regiões de saúde do estado de São Paulo. Ceara: Instituto Adolfo Lutz; 2021.
-
30Freitas ARR, Giovanetti M, Alcantara LCJ. Variantes emergentes do SARS-CoV-2 e suas implicações na saúde coletiva. Inter Amn J Med Health. 2021; 3 (1): 4-10. https://doi.org/10.31005/iajmh.v4i.181
» https://doi.org/https://doi.org/10.31005/iajmh.v4i.181 -
31The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. Vital surveillances: the epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)-China, 2020. China CDC Weekly 2020, 2 (8): 113-22. https://doi.org/10.31005/iajmh.v4i.181
» https://doi.org/https://doi.org/10.31005/iajmh.v4i.181 -
32Castro MC, Kim S, Barberia L, Ribeiro AF, Gurzenda S, Ribeiro KB, et al. Spatiotemporal pattern of COVID-19 spread in Brazil. Science 2021; 372 (6544): 821-6. https://doi.org/10.1126/science.abh1558
» https://doi.org/https://doi.org/10.1126/science.abh1558 -
33Araújo AAC, Amaral JV, Sousa JN, Fonseca MCS, Viana CDMC, Mendes PHM, et al. COVID-19: analysis of confirmed cases in Teresina, Piaui, Brazil. Rev Prev Infecç. Saúde 2020; 6 (3): 2-8. https://doi.org/10.1590/SciELOPreprints.465
» https://doi.org/https://doi.org/10.1590/SciELOPreprints.465 -
34Cupertino MC, Cupertino GA, Gomes AP, Mayers NA, Siqueira-Batista R. COVID-19 in Brazil: epidemiological update and perspectives. Asian Pac J Trop Med 2020; 13 (5): 193-6. https://doi.org/10.4103/1995-7645.282215
» https://doi.org/https://doi.org/10.4103/1995-7645.282215
-
Financial support: none
Publication Dates
-
Publication in this collection
06 Sept 2021 -
Date of issue
2021
History
-
Received
31 May 2021 -
Accepted
16 June 2021 -
Preprint posted on
21 June 2021





