Abstracts
PURPOSE: to compare the previous and posterior education-learning knowledge of the 3rd year students of speech-language and hearing pathology's students about the topic Health Management. METHOD: the subjects were asked to answer a protocol before and after one year Health Management taught to be obtained the information about the learning and the relation with health-disease process, own daily lives management and what they consider a management guiding principle in the Seepch-language and hearing profession. Data were analyzed with the application of qualitative methodology Árvore de Associação de Ideias. RESULTS: the results were organized in three categories (1) Health-disease process, (2) Recovery health, (3) Speech-language and hearing pathology: therapy as a cure. In the first category it was observed that students changed the ideia of the conceptualization of health as opposed to the disease to a factor inherent in the quality of life. In the second category self-medication and the search for private care were found. And the third category they indicated the need of speech-language and hearing therapists work holistically to improve the individual's quality of life. CONCLUSION: the undergraduate training in speech-language and hearing pathology elicited partial understanding of health-disease process as a primary guideline and the challenge will be to initiate new instabilities production and provide full conditions for this knowledge capillarity in the disciplines of speech-language and hearing sciences.
Speech, Language and Hearing Sciences; Health Management; Public Health
OBJETIVO: comparar o conhecimento, prévio e posterior ao ensino-aprendizagem sobre o tema Gestão em Saúde, dos estudantes do 3º ano do curso de Fonoaudiologia. MÉTODO: os indivíduos foram solicitados a responder um protocolo antes e um ano depois de ministrado o módulo de Gestão em Saúde para serem obtidas informações sobre a forma como ocorreu o aprendizado com relação ao processo saúde-doença, administração deste conteúdo em seu cotidiano e o que consideraram como princípio norteador de gestão na profissão do fonoaudiólogo. Os dados foram analisados com a aplicação da metodologia qualitativa Árvore de Associação de Ideias. RESULTADOS: os resultados foram organizados em três categorias (1) Processo saúde-doença, (2) Recuperação da saúde, (3) Fonoaudiologia: terapia como meio de cura. Na primeira categoria se observou que os alunos passaram da conceituação da saúde como contraposição à doença para fator inerente à qualidade de vida. Na segunda constatou-se a prevalência da automedicação e busca por atendimentos privativos. Na terceira categoria indicaram a necessidade do fonoaudiólogo atuar de forma integral para melhoria da qualidade de vida do individuo. CONCLUSÃO: a formação dos alunos de graduação em Fonoaudiologia suscitou compreensão parcial do processo saúde-doença como diretriz primordial e o desafio será instaurar a produção de novas instabilidades e proporcionar as condições integrais para a capilaridade desse conhecimento junto às disciplinas específicas das ciências fonoaudiológicas.
Fonoaudiologia; Gestão em Saúde; Saúde Coletiva
ORIGINAL ARTICLES
Health management: the undergraduates' learning and academic education
Aline Megumi ArakawaI; Érica Ibelli SittaII; Magali de Lourdes CaldanaIII; Maria Aparecida Miranda de Paula MachadoIV
ISLP; PhD student, Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru Dental School/ USP, Bauru, São Paulo, Brazil
IISLP; Master by Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru Dental School/ USP, Bauru, São Paulo, Brazil
IIISLP; Associated professor of Department Speech Language and Hearing Sciences, Bauru Dental School/ USP, Bauru, São Paulo, Brazil
IVSLP; PHD Professor of Department Speech Language and Hearing Sciences, Bauru Dental School/ USP, Bauru, São Paulo, Brazil
Mailing address
ABSTRACT
PURPOSE: to compare the previous and posterior education-learning knowledge of the 3rd year students of speech-language and hearing pathology's students about the topic Health Management.
METHOD: the subjects were asked to answer a protocol before and after one year Health Management taught to be obtained the information about the learning and the relation with health-disease process, own daily lives management and what they consider a management guiding principle in the Seepch-language and hearing profession. Data were analyzed with the application of qualitative methodology Árvore de Associação de Ideias.
RESULTS: the results were organized in three categories (1) Health-disease process, (2) Recovery health, (3) Speech-language and hearing pathology: therapy as a cure. In the first category it was observed that students changed the ideia of the conceptualization of health as opposed to the disease to a factor inherent in the quality of life. In the second category self-medication and the search for private care were found. And the third category they indicated the need of speech-language and hearing therapists work holistically to improve the individual's quality of life.
CONCLUSION: the undergraduate training in speech-language and hearing pathology elicited partial understanding of health-disease process as a primary guideline and the challenge will be to initiate new instabilities production and provide full conditions for this knowledge capillarity in the disciplines of speech-language and hearing sciences.
Keywords: Speech, Language and Hearing Sciences; Health Management; Public Health
INTRODUCTION
Since the Unified National Health System (NHS) creation efforts were made by the three spheres of government, the population and the health professionals to properly implement and respect their principles1. The process of change in the Brazilian undergraduate health professions education has been based on the Law of Guidelines and Bases of Education, which seeks to qualify the students and contribute to the improvement of care provided to the NHS users. The National Curriculum Guidelines seek a more generalist, humanist, critical and reflective training, enabling health professionals to act according to ethical and scientific principles in their clinical-therapeutic and preventive practice.
In the undergraduate courses we observed the importance of establishing and implementing contents related to the public health theoretical-conceptual model, which in turn, is characterized as a field of knowledge and health practices as a social phenomenon, and also as public significance, supporting the NHS guidelines and principles2,3. The general skills and abilities to work with health care, communication, leadership, administration and management, continuing education, present in the undergraduate health care's Curriculum Guidelines, are closely linked, and even dependent on the understanding of the conditions and general elements of health services management. Thus, the theme taught in the classroom, will give opportunity to graduates, to strengthen the reorientation processes of the health care model4 as well as the daily practices in services on the "organization of the health work process based on the NHS guidelines"5.
In this context, the same authors emphasized the role of health-disease process, which was modified during the development of beliefs and values socially constructed. Admitted as part of reality, differentiated approaches are promoted since organic instance to the challenges of a "non-reductionist approach that restored the meaning of the individual in his singularity and subjectivity in relation to the others and with the world." The social ways of life production define the health challenges commonly related to the social groups formation and transformation, and thus must be fully understood in order to advance in the knowledge of more complex problems6.
This process suffers direct influences of health services offered to the population, and significant changes were made by many socialist and capitalist countries, as about its organization, exploring more intensely scientific and technological aspects offered for health systems services management7. Defying the student to operate in setting priorities as well as goals and strategies, acting in the service configuration and transformation of professional practices, evaluate, especially their efficiency, effectiveness and investment effectiveness, as well as substantial research articulated to the health services and population needs, are some functions of teaching management practices.
Conceptions about democracy, empowerment and community, are values considered fundamental in the public services quality since the individual growth is a prerequisite for the empowerment community and social changes8 and thus allowing the individual autonomy in their choices and competence in disseminating information in the health field9. These concepts rely on constant experience to be assumed and improved during the academic training, trespassing, in contrast, the specificities of the several health disciplines.
The research Swedish showed that health quality is related to the satisfaction of the user's needs and the efficient use of health resources. In addition the ability of the citizens to realize the changes that are materialized in quotidian where are the opportunities for collective learning10. In this context that involves the health-disease process, human and ethics values, social groups transformation, setting priorities, citizen satisfaction and collective learning, the purposed of this research was to compare the previous and posterior education-learning knowledge of the 3rd year students of Speech-Language and Hearing Sciences about the topic Health Management.
METHOD
The present study, which shows a longitudinal, descriptive and qualitative character, was developed after the acceptance of FOB/USP Ethics and Research Committee under the case number 146/2010.
Participants in the first sample totaled 36 and the second 31 students who signed the consent form. Its development occurred through the application of a semi-structured protocol, previously elaborated by the researchers with indirect questions. The students responded the instrument before and one year after being taught the module Health Management (30 hours) so that the different categories could be obtained: how the health-disease learning process occurred; the administration of this content in their daily lives and what would they consider as a guiding management principle in the Speech-Language and Hearing Sciences (SLH) profession.
The obtained data were analyzed qualitatively, with the application of the "tree of ideas association methodology" (Árvore de Associação de Ideias)11, which consists in reading and extracting relational categories, constructed to allow the visualization of the idea in the discourse flow (oral and written, individual or collective) and the results were substantiated in the light of the literature.
RESULTS
The collected data were organized into three categories and the results received detailed reading analysis and style expression condensation on the same content, and then related to literature.
Category 1. Health-Disease process (questions 1 and 2)
In the first data collection, the result is related to the health-disease process conceptualization, presented in an opposition between health and disease, focusing on traditional hegemonic models. In the second collection, they understand the health-disease process as an inherent factor of the individuals quality of life12, considering psycho emotional factors, bringing to critical discussion of the definition assigned by the World Health Organization (WHO) preconized in 1948, in which health is "a state of complete physical, mental and social well-being and not merely the absence of disease." None of the collections refer questions about the social order adopted in the NHS implementation. The compilation of data analyzed is shown in the Figure 1.
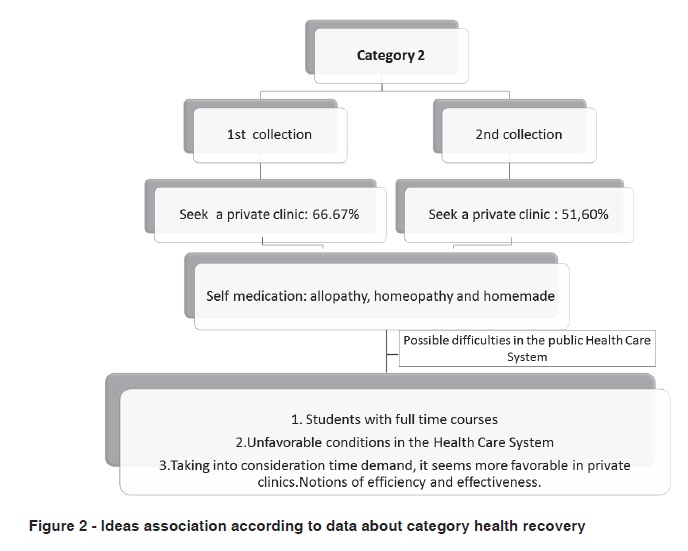
Category 2. Health recovery (questions 3 and 4)
When asked about seeking care, in case they get sick, 66.6% in the first collection and 51.6% in the second one, students opted for private clinics, in the first place, and the emergency care in the second place. On this issue it is possible to observe four relevant data:
1) when this research was conducted, the University of São Paulo granted private health insurance to students.
2) there is a Health Care Center on the campus of University tied the USP's Rectory.
3) there is little disclosure and little municipal investment in the Primary and Family Health Care Center, whereas the latter attends only 7% of the population.
4) it is embedded in the "culture" of the population to seek the Emergency Service Centers. What we are calling "culture" is the society strategy maintained and enhanced the demand for emergency health centers since there are few primary health centers(18) and family health (seven teams, divided into two strategic locations, plus a program of Community Health Agents) for a population nearly about 360,000 inhabitants, and reduced and/or poorly quantity distributed health professionals.
Regarding to the self-medication procedure in the first collection almost 50% of the responses were positive, considering homeopathic, homemade and pharmacological allopathic medication. In the second collection, the same percentage was found, using the same drugs, highlighting some therapeutic actions (antipyretic, analgesic, among others).
A summary of this information using the tree of ideas association (Árvore de Associação de Ideias ) is presented in Figure 2.
Category 3. Speech-Language and Hearing Sciences: therapy as a way of healing (question 5)
Observing the data obtained during the ideas association in the first collection the participant contradicted themselves: (1) SLH Sciences diagnose and cure organic illnesses (in the area), (2) does not heal but helps in the maintenance of a better quality of life, (3) does not heal (because there is no medication). In the second collection, although there was also opposition, the answers were in the same level of consideration about the comprehensiveness principle and health promotion (beyond the prevention), highlighting issues of psycho emotional order and citing the social dimension. Figure 3 shows the discussed ideas.
DISCUSSION
According to the questions presented in Category 1, the emphasis on the health-disease biological process, reinforced during years in speech therapy course gave way to a biopsicoemocional approach.The disease is explained as an individual's internal homeostasis break attributed to the experienced stress as a factor that determinate the health changes, corroborating with authors who affirmed13 that it's the requirement of adaptation, positive or negative, called stressor. Such stressors may be external or internal, and the first can occur independently of the personal internal world, such as: change of leadership, political changes in the country, accidents and other situations that happen outside the individual's body and mind. The second is determined by the individual, such as: anxiety, shyness, depression also including beliefs, lack of assertiveness and difficulty to express feelings.
The maximum approach social achieved was the corroboration with the study14 where health and disease are two extremes of a constant dynamic performed by the individual and the environment where he/she lives, the normal-abnormal, inspiration-expiration, sleep-alert, life-death. The community conditions and determines the health and illness on the relationship between individuals and the environmental systems in which they live to interact with living and nonliving. It is through this interaction that action and reaction effects are triggered interfering in the physical and environment construction and producing (un) sustainable means to survival and preservation15,16. This dynamic is different for each individual and the difference becomes crucial according to each one's ability to deal with the aggressions one faces, called resilience17,and thus, in a subjective way, is reflected in the quality of life indicated by the students.
However, no student quoted the definition of the 8th National Health Conference, 1986, or discussed the notion of health as a social right and achievement, thus, the social and regional inequalities that act as limiting factors to the full development of a satisfactory level of health and it's organization. Although the graduate students training has been mainly directed to the health knowledge in a comprehensive, holistic way, in support to the quality of life and for some values that simultaneously instituted and are instituted by the citizenship definition ambivalence, it did not allow a relationship between individual and society, and of caring and responsible citizens.
Nowadays one of the public policies challenges has been exactly to reconcile the universalization to the citizenship term acquired in the contemporary concept, with claims for the right to preserve the differences to ensure equity.
In relation to Category 2, the excluding universality seems to keep growing, making the private sector funding mechanisms increasingly similar to the American system, "in which State action is residual"18. Currently social classes C and D have been in a scenario of struggle between the supplementary healthcare operators, due to their purchasing power increase. Data19 highlighted 1,100 active supplementary healthcare companies operators in the country, among insurers, medical cooperatives or medicine group companies and "almost all social classes A and B are already within the healthcare supplementary."
Given these explanation it can be verified that the management on the health principle is guided by notions of effectiveness (best x worst) and efficiency (investment x benefits), lined by the little time that students have in the business hours, more especially those studying full time, and by media reports that most of the times points to local public health places with long queues, independent of the procrastination that occurs within private clinics and the time for exams through the supplementary healthcare. While the comments also occur in cities where public health is well evaluated by the population, in Bauru-SP there are negative headlines every day, in the spoken or written media, for political reasons or because it states the truth about the system. Fortunately most students pointed to seek some professional help.
Concerning the self-medication procedure, there was, mainly, the disregard of nosological diagnosis and the signs and symptoms of more serious diseases that could be concealed by drugs, which are available without prescription, have strong commercial appeal, can be used for a specified time (antipyretic, for example) or are considered "without side effects." Similar results are found in a research20 that verified the use of self-medication by the future health professionals, from different courses. The authors noted that 42% of students had used drugs prescribed by doctors, and 58% used self-medication. Another study21 found the presence of self-medication in 40% of nursing students. These authors stated that the educational practices incorporation for not trivializing the use of drugs should be performed, including health students, so they can properly guide their future patients.
In some studies22 the medication has been referred as symbolic commodity and discussed from the social point of view of the physician prescribing the medication and of the individual, in which complex sets of relationships such as "hegemony, alliances, transgression, submission, power and counter power and other." The discussions concluded that health reified is embedded in a commodity consumption relationship having the need to break with this concept for a shift of health as a right. On the other hand, authors23 emphasized that, when consumed, they induces the individual to meet the need of change from a "bad" state to a "good" one, from a state of no-health, dissatisfaction, to a state of health / satisfaction, as extensively proclaimed by healthcare professionals.
Moreover, there are barriers to the medicines rational use: the lack of guidance for the users on the part of prescribers, direct advertising to the final consumer and the consumer misuse24. In this sense, self-medication and / or inappropriate prescribing may lead the individual to experience side effects, develop iatrogenic diseases and mask progressive diseases, therefore, it represents a problem to be prevented25.
Regarding the use of homemade medicines one should observe that the Ministry of Health, in the Interministerial Order 2.960/2008 introduced the National Medicinal Plants and Herbal Medicines Program, with a focus on primary care. The program, among its objectives, proposes to introduce or expand the medicinal plants supply, herbal remedies and services related to Herbal Medicine, in line with the NHS guidelines, and also to promote and recognize the popular and traditional practices of herbal and homemade medicines use26.
It is this context that future health professionals should take into consideration regarding the self-medication process so that the repercussion and orientation in this activity be clarified and performed in a safe way.
In the Category 3, thinking about the cure of diseases / changes / disorders related to Speech Language and Hearing Sciences, according to the questions presented, it was observed that students exercised their skills, abilities and attitudes in a critical and reflective way as suggested in and Base Law of The National Education Guidelines, especially those focused in primary health care knowledge, decision-making, leadership and administration, and management. On this approach the disorders affect the individual health, seen from two angles: first as the absence of the restricted sense of disease, that is, as quality of life, whose characteristic is adopted in health promotion, in which help be given to the subject so that he/she can find an inner balance, their empowerment through knowledge, stabilization of the aspects (psycho emotional) that surround the morbidities and therefore dispenses medical/ medication treatment or uses it as a supporting treatment. The second, in which the disease is taken as a starting point and whose treatment, medical or surgical, is performed by medical professionals, but that requires a speech, language and hearing pathologist intervention prior, during and / or after the procedure, to recovery or rehabilitation. In both models what counts is how much one suffers with the difficulty of communication that might be or that is present in the subject daily life, and the impossibility for the professionals to deal directly with the disease but which acts on the morbidity or injury implications.
Thus, these factors may signal the speech, language and hearing pathology forms of intervention on the causes and consequences of diseases considering what generates the psycho affective and social problems, which are difficult to measure by means of examination and / or improved by intake of medications. These disorders affect the professional aspects, self-confidence, happiness and safety of an indivíduo27.
At first, students indicated the use of medication as a means of providing a cure, however this statement does not appear in in the second collection, which has its focus on the aspect regarding the maintenance of health and the participation of professionals in the process of mental, physical and social healing. Authors28 advocate that aspects of speech, language and hearing should be health attributes, since they affect the competence and communicative performance in verbal and non-verbal, intra and interpersonal, and even that they do not cause physical pain, do not have signs and symptoms that can be expressed in laboratories, cannot be cured by ingestion of drugs nor lead to death, they do cause suffering. Although other areas have not been mentioned by the authors, one cannot ignore the role of the speech, language and hearing pathologist at all levels of prevention, when there is reference of certain diseases that can lead to death, as it is the case of neurological dysphagia, or in consequences of cases of advanced laryngeal cancer, as characteristics of morbidities that deserve special attention when it mentions the communication factor. Another study highlighted29 that the speech, language and hearing pathologist works in research, prevention, assessment and therapy in different areas that concern the profession, but there is need to invest in improving the quality of life through the training of professionals with the perspective of health promotion 30.
In contrast, the health care professional who has his/her training directed towards working in NHS conducts individual and collective promotion, protection and recovery of human communication, providing comprehensive care to individuals and collectivities accompanying empowerment regarding their health. It is noteworthy, therefore, that health professionals act as facilitators in the process of health education, and that the idea of integrated care in health implies a knowledge developed collectively by professionals, teachers, managers and users / patients, co-responsible for health31 production.
Thus, the construction of the current ethical and humanistic values as fairness and equality, democracy, and community empowerment, diversity and choice, and intervention or non-intervention of the state, which lead to policies of social groups transformation, to conformation of a set of priorities, the pursuit of satisfaction of citizens and the collective learning of both parties - healthcare professional and individual (or collective), were the guiding principles of the health management module on this course of Speech-Language and Hearing Sciences.
Based on the above considerations, it was possible to observe that the human being, complex and multiple, is a product and the producer of health practices, and the individuals in the care actions, are transformed into the subject of health action, according to their individual, social, economic and cultural peculiarities. Thus, individuals and groups must be empowered with knowledge in order to identify their aspirations, to satisfy their needs, favorably modifying the environment in which they live in32. In this sense, management deals with polarities. This gives us opportunities to face the challenge of questioning instances that emphasize the imbalance between autonomy and control, benefits and harms, production and reproduction, disease and health, and caregiver and one who receives care, among outras33.
Thus, the students emphasized that the Speech-Language and Hearing Sciences participates in a cycle that seeks to provide improved quality of life of the individual, considering an interdisciplinary work of NHS principles: comprehensiveness as an essential fact in the development of the therapeutic process of a patient or community. Study34 confirms the need for full implementation of the health care services from the organization of services to the professional training at undergraduate level. And in the case of professional training, agents such as: teachers, school leaders, students, education managers and managers of NHS must be present.
CONCLUSION
Given the found data it can be concluded that the graduate students training in SLH Sciences prompted the partial understanding of the health-disease process as a primary guideline for exploring the territories of unique powers in the social practices field (health). However, it enhanced the learning progress regarding comprehensiveness process, when adopted in its praxis, theoretical positions focused on the quality of life and health promotion, simultaneously investing on disease prevention, in a broad and interdisciplinary sense. Thus, the challenge will be to establish the production of new instabilities and provide integral conditions for the capillarity of this knowledge with the specific Speech-Language and Hearing Sciences disciplines. Procedures can be adopted focusing on restructuring the methodology of teaching and learning by observing the contributions and limitations of the activities performed and the topics covered with students frequent dialogues in order to verify their suggestions, criticism and the thought directed to a better assimilation of the content offered.
REFERENCES
- 1. Ceccim RB, Armani TB, Rocha CF. O que dizem a legislação e o controle social em saúde sobre a formação de recursos humanos e o papel dos gestores públicos, no Brasil. Cien Saude Colet. 2002;7(2):373-83.
- 2. Carvalho SR. Saúde coletiva e promoção da saúde: sujeito e mudança. São Paulo: Hucitec, 2005.
- 3. Barroso MGT. Saúde coletiva e promoção da saúde: sujeito e mudança. Cad Saude Publica. 2007;23(1): 244-6.
- 4. Koifman L, Gomes LN. A Graduação em saúde coletiva: um debate ou uma realidade? Rev Bras Educ Méd. 2008;32(4):4178.
- 5. Carvalho SR, Cunha GT. A gestão da atenção na saúde: elementos para se pensar a mudança da organização na saúde. In: Campos GW, Minayo MC, Akerman M, Drumond Jr M, Carvalho YM. Tratado de Saúde Coletiva, São Paulo; Rio de Janeiro: Hucitec; Fiocruz, 2007.
- 6. Barata RB. Epidemiologia e ciências sociais. In: Barata RB e Briceño-Leon R. Doenças endêmicas: abordagens sociais, culturais e comportamentais. Rio de Janeiro:Fiocruz, 2000.
- 7. Paim JS. Epidemiologia e planejamento: a recomposição das práticas epidemiológicas na gestão do SUS. Cienc Saude Coletiva. 2003;8(2):557-67.
- 8. Kasmel A, Tanggaard P. Evaluation of changes in individual community-related empowerment in community health promotion interventions in Estonia. Int J Environ Res Public Health. 2011;8(6):1772-91.
- 9. Brites LS, Souza APR, Lessa AH. Fonoaudiólogo e agente comunitário de saúde: uma experiência educativa. Rev Soc Bras Fonoaudiol. 2008;13(3):258-66.
- 10. Øvretveit J. Health Service Quality: an introduction to quality methods for health services. 3. ed. London:Blackwell Science, 1995.
- 11. Spink JM, Lima H. Rigor e visibilidade: a explicitação dos passos da interpretação. In: Spink MJ. Práticas discursivas e produção de sentidos no cotidiano aproximações teóricas e metodológicas. São Paulo:Cortez, 1999.
- 12. Penteado RZ, Servilha EAM. Fonoaudiologia em saúde pública/coletiva: compreendendo prevenção e o paradigma da promoção da saúde. Distúrb Comun. 2004;16(1):107-16.
- 13. Furtado ES, Falcone EMO, Clark C. Avaliação do estresse e das habilidades sociais na experiência acadêmica de estudantes de medicina de uma universidade do Rio de Janeiro. Interação Psicol. 2003;7(2):43-51.
- 14. Souza SPS, Lima RAG. Chronic condition and normality: towards the movement that broadens the power of acting and being happy. Rev. Latinoam. Enferm. 2007;15(1):156-64.
- 15. Cezar-Vaz MR, Soares MCF, Martins SR, Sena J, Santos LR, Rubira LT et al. Saber ambiental: instrumento interdisciplinar para a produção de saúde. Texto & Contexto Enferm. 2005;14(3):391-7.
- 16. Sant'Anna CF, Cezar-Vaz MR, Cardoso LS, Erdmann AL, Soares JFS. Determinantes sociais de saúde: características da comunidade e trabalho das enfermeiras na saúde da família. Rev Gaúch Enferm. 2010;31(1):92-9.
- 17. Libório RMC, Ungar M. Resiliência oculta: a construção social do conceito e suas implicações para práticas profissionais junto a adolescentes em situação de risco. Psicol Reflex Crít. 2010;23(3):476-84.
- 18. Faveret Filho P, Oliveira PJ. A universalização excludente: reflexões sobre as tendências do sistema de saúde. Dados Rev Ciênc Sociais. 1990;33(2):257-83.
-
19Saúde na Mídia. Ministério da Saúde. Clipping da Imprensa. Ministério da Saúde/ANS. Valor Econômico/BR: O sonho da nova classe média. Valor Financeiro. 2011:62-4. [acesso em 2013 abr 02]. Disponível em http://saude.empauta.com
- 20. Aquino DS, Barros JAC, Silva MDP. A automedicação e os acadêmicos da área de saúde. Cienc Saude Coletiva. 2010;15(5):2533-8.
- 21. Souza LAF, Silva CD, Ferraz GC, Sousa FAEF, Pereira LV. the prevalence and characterization of self-medication for obtaining pain relief among undergraduate nursing students. Rev Latino-Am. Enfermagem. 2011;19(2):245-51.
- 22. Lefèvre F. O medicamento como mercadoria simbólica. São Paulo :Cortez, 1991.
- 23. Melo CM, Oliveira DR. uso de inibidores de apetite por mulheres: um olhar a partir da perspectiva de gênero. Cienc Saude Coletiva. 2011;16(5):2523-32.
- 24. Silva IM, Catrib AMF, Matos VC, Gondim APS. Automedicação na adolescência: um desafio para a educação em saúde. Cienc Saude Coletiva. 2011;16(Supl. 1):1651-60.
- 25. Gérvas J. Prevención cuaternaria. Acta Sanitaria. 2011.
-
26Brasil. Ministério da Saúde. Portaria interministerial nº 2.960, de 9 de dezembro de 2008. Brasília, DF: Ministério da Saúde; 2008 [acesso em 2012 mar 14]. Acessem em: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2008/pri2960_09_12_2008.html
- 27. Fernandes EL, Cintra LG. Relato de experiência: a inserção da fonoaudiologia na Estratégia da Saúde da Família: relato de caso. Rev. APS. 2010;13(3):380-5.
- 28. Moreira MD, Mota HB. Os caminhos da fonoaudiologia no sistema único de saúde SUS. Rev CEFAC. 2009;11(3):516-21.
- 29. Bacha SMC, Osório AMN. Fonoaudiologia & educação: uma revisão da prática histórica. Rev CEFAC. 2004;6(2):215-21.
- 30. Lipay MS, Almeida EC. A fonoaudiologia e sua inserção na saúde pública. Rev Ciênc Méd. 2007;16(1):31-41.
- 31. Machado MFAS, Monteiro EMLM, Queiroz DT, Vieira NFC, Barroso MGT. Integralidade, formação de saúde, educação em saúde e as propostas do SUS uma revisão conceitual. Cienc Saude Coletiva. 2007;12(2):335-42.
- 32. Erdmann AL, Andrade SR, Mello ALSF, Meirelles BHS. Gestão das práticas de saúde na perspectiva do cuidado complexo. Texto Contexto Enferm. 2006; 15(3):483-91.
- 33. Cunha GT. A gestão para a clínica ampliada. São Paulo:HUCITEC, 2005.
- 34. Ceccim RB, Feuerwerker LCM. Mudança na graduação das profissões de saúde sob o eixo da integralidade. Cad Saude Publica. 2004;20(5):1400-10.
Endereço para correspondência:
Publication Dates
-
Publication in this collection
18 Sept 2013 -
Date of issue
Aug 2013
History
-
Received
13 Aug 2012 -
Accepted
26 Mar 2013