Abstract
OBJECTIVE: To investigate the relationship between religiosity and drug use among Brazilian university students. METHODS: This manuscript is part of the "First Nationwide Survey on the Use of Alcohol, Tobacco and Other Drugs among College Students in the 27 Brazilian State Capitals". In this study, 12,595 university students were divided into two groups according to their attendance at religious services: frequent attenders (FR; 39.1%) and non-frequent attenders (NFR; 60.8%). Subsequently, we analyzed their responses to a structured, anonymous questionnaire on drug use and other behaviors. Individual multivariate logistic regression models tested the association between religiosity and drug use (alcohol, tobacco, marijuana and at least one illicit drug). RESULTS: Drug use over the last 30 days was higher among NFR students even after controlling for demographic variables. NFR students were more likely to use alcohol OR = 2.52; 95% CI: 2.08-3.06, tobacco (2.83; 2.09-3.83), marijuana (2.09; 1.39-3.11) and at least one illicit drug (1.42; 1.12-1.79) compared to FR students. CONCLUSION: Religiosity was found to be a strongly protective factor against drug use among Brazilian university students. However, more studies are needed to identify the mechanisms by which religiosity exerts this protective influence.
Religion and Medicine; Street Drugs; Cross-Sectional Study; Students; Brazil
ORIGINAL ARTICLE
Religion as a protective factor against drug use among brazilian university students: a national survey
Fernanda Carolina GomesI; Arthur Guerra de AndradeI,II,III; Rafael IzbickiIV; Alexander Moreira-AlmeidaV; Lúcio Garcia de OliveiraI,II
IInterdisciplinary Group for Studies on Alcohol and Drugs (GREA), Department and Institute of Psychiatry, Universidade de São Paulo, Brazil
IIDepartment and Institute of Psychiatry, Universidade de São Paulo, Brazil
IIIDepartment of Psychiatry, Faculdade de Medicina do ABC, Brazil
IVInstitute of Mathematics and Statistics, Universidade de São Paulo, Brazil
VResearch Center in Spirituality and Health (NUPES), Universidade Federal de Juiz de Fora, Brazil
Corresponding author Corresponding author: Lúcio Garcia de Oliveira Department and Institute of Psychiatry, Faculdade de Medicina, Universidade de São Paulo (FMUSP), Department and Institute of Psychiatry, GREA R. Dr. Ovídio Pires de Campos, 785 05403-903, São Paulo, SP, Brazil Phone: + 55 11 3069-7892; Fax: + 55 11 3069-7893 E-mail: lucgoliver@gmail.com
ABSTRACT
OBJECTIVE: To investigate the relationship between religiosity and drug use among Brazilian university students.
METHODS: This manuscript is part of the "First Nationwide Survey on the Use of Alcohol, Tobacco and Other Drugs among College Students in the 27 Brazilian State Capitals". In this study, 12,595 university students were divided into two groups according to their attendance at religious services: frequent attenders (FR; 39.1%) and non-frequent attenders (NFR; 60.8%). Subsequently, we analyzed their responses to a structured, anonymous questionnaire on drug use and other behaviors. Individual multivariate logistic regression models tested the association between religiosity and drug use (alcohol, tobacco, marijuana and at least one illicit drug).
RESULTS: Drug use over the last 30 days was higher among NFR students even after controlling for demographic variables. NFR students were more likely to use alcohol OR = 2.52; 95% CI: 2.08-3.06, tobacco (2.83; 2.09-3.83), marijuana (2.09; 1.39-3.11) and at least one illicit drug (1.42; 1.12-1.79) compared to FR students.
CONCLUSION: Religiosity was found to be a strongly protective factor against drug use among Brazilian university students. However, more studies are needed to identify the mechanisms by which religiosity exerts this protective influence.
Descriptors: Religion and Medicine; Street Drugs; Cross-Sectional Study; Students; Brazil.
Introduction
According to the latest World Drug Report from the United Nations Office on Drugs and Crime (UNODC), between 149 and 272 million people report that they have used some type of illicit drug every year. Almost 200,000 people die from drug use worldwide, affecting not only the drug users but also family members, friends, co-workers and communities.1
Drug use (including the use of illicit drugs, alcohol and tobacco) is widespread, and this wide distribution increases the burden of disease related to drug use. According to the World Health Organization's "Global status report on alcohol and health," the harmful use of alcohol is a causal factor in 60 types of diseases and injuries, resulting in approximately 2.5 million deaths every year. These deaths make up almost 4% of all deaths worldwide.2 Tobacco is responsible for 5 million deaths annually.3
Given the individual and social costs of drug use, researchers have attempted to identify factors that are associated with drug use and factors that are protective against drug use.4 Of these, religiosity has been suggested as one of the most important protective factors against drug use, preventing individuals from using drugs even if they live in precarious environments.5,6 Therefore, health care providers and researchers are now increasingly interested in studying religion. In the last two decades, there has been a large increase in the number of studies showing an association between religious involvement and improved health outcomes. These associated outcomes have included fewer depressive symptoms, a lower risk of suicide, decreased mortality rates, and a better quality of life. One of the dimensions of religion that is most strongly associated with health outcomes is attendance at religious meetings. Other dimensions include religious affiliation, private religious practices (such as prayer or reading religious texts), religious coping, religious commitment (the influence of religious beliefs on one's decisions and lifestyle), and subjective religiosity (the importance of religion to the individual).7 Numerous studies have described the protective effects of religiosity against drug use in adolescents,8-12 but there are few findings about this relationship in university students, especially using national samples.
One of the oldest studies on this subject, which was conducted in Ireland, suggested that university students who attended religious services infrequently and university students who did not believe in God reported using more alcohol.13 Years later, another study in Australia found that students who believed that religion was unimportant in their lives reported using more alcohol, tobacco, marijuana and hallucinogens.14 Later, in a study of a nationally representative sample of university students in the United States, researchers found that the use of ecstasy was higher among students who stated that religion had little influence on their lives.15 In another study, these results were expanded to include the use of other drugs among European university students.16
It is worrisome, as noted by a review article, that most of the evidence about spirituality and addiction comes from populations from a restricted range of biocultural backgrounds. These populations mostly live in English-speaking countries; less than 2% of the research studies were performed in the developing world.17 The studies need to be expanded to include more diverse populations.
In Brazil, for instance, few studies have focused on the relationship between religious involvement and substance use. The majority of the available studies have found that religiosity is protective against substance use in samples of Brazilian adolescents,5,18-20 and a few studies have focused on this relationship among university students.21,22 In addition, studies of community-based samples have been scarce. A recent Brazilian study suggested that religiosity reduces the odds of using tobacco and that not having a religion increases the risk of alcohol misuse in a community-based sample of elderly adults 60 years and older.23 However, we are not aware of any Brazilian studies that have examined the relationship between religiosity and substance use in a nationally representative sample of university students.
In studies of university students, religiosity is generally a protective factor against drug use. For example, one of the pioneering studies on this subject in Brazil was conducted with medical students in Marilia, Sao Paulo, and it showed that religion played a protective role against the use of alcohol.21 Another Brazilian study showed that religiosity is also protective against the use of other drugs. The conclusion was that university students who report that they attend religious services have values and norms that result in protective behaviors.22
Although these studies were valuable in introducing an important issue, they were regional studies that were mainly descriptive. They did not evaluate the effect of religiosity on drug use while controlling for the confounding effects of other variables. Furthermore, they did not evaluate the relationship between religiosity and recent drug use, which can be measured as drug use in the last 30 days.
Thus, to overcome this lack of evidence, we aimed to assess the influence of religiosity on drug use and other behaviors within a representative sample of university students from private and public universities throughout Brazil.
Methods
This manuscript is part of the recently released report, "First Nationwide Survey on the Use of Alcohol, Tobacco and Other Drugs among College Students in the 27 Brazilian State Capitals."24 These data were gathered between May and December of 2009. This survey is a population-based epidemiological study coordinated by the National Secretariat for Drug Policies (SENAD) and the Interdisciplinary Group for Studies on Alcohol and Drugs (GREA).
Study design
A probabilistic, stratified sample of university students throughout Brazil was selected using unequally sized conglomerates, and the selected students were recruited to participate in the study. The five administrative regions of Brazil and the two types of higher education institutions (HEI; either public or private) were used as the strata for sampling. The HEIs and the classes of students (defined as the group of students studying a given subject) were considered conglomerates (i.e., primary sampling units). Because a single university student would be enrolled in more than one subject, multiplicity sampling was also used, enabling population elements to be included in more than one conglomerate.
The sampling was carried out in two stages. In the first stage, HEIs were randomly selected from a reference list provided by the Anisio Teixeira National Educational Studies and Research Institute - INEP of the Ministry of Education in Brazil. According to this list, there were 2,252 HEIs in Brazil in 2008. Only HEIs located in the state capitals were considered for sampling. Therefore, the reference list was organized by state capital and by HEI type.
Next, HEIs were chosen with a systematic selection method based on a random starting point and using a PPeS (Probability Proportional to estimated Size; by the number of students enrolled), based on data from the reference system previously mentioned. The administration of each participating HEI was asked to provide a list of all mandatory classroom-based subjects at the undergraduate level for their institution. This list of subjects was broken down by academic year, study period and course to enable the researchers to randomly select the participating classes. Therefore, each HEI had its own reference system for the second phase of sample selection. Next, a second systematic drawing was conducted. The number of classes (drawn according to subject) was proportional to the total number of students in the HEI in a given state capital.
All of the students in a selected class were invited to participate in the study. Participation was voluntary. After accepting, the students were asked to provide informed consent. The students were responsible for filling out a research questionnaire. Personal information, such as name, address, e-mail, and the name of the university attended, was not obtained to ensure confidentiality. Once a student completed the questionnaire, which took them 50 minutes in average, he or she deposited it and the informed consent form in separate urns. More details about the methodology of this survey may be found elsewhere.24
Main outcome measures
An anonymous questionnaire with 98 close-ended questions was chosen as the research instrument. Its content was based on a World Health Organization research instrument that was adapted by Stempliuk et al.25 for use with Brazilian university students. The questionnaire provided the following information about the participating students: (a) sociodemographic data, including gender, age, marital status, ethnicity, and socioeconomic status (socioeconomic status was estimated using the Critério de Classificação Econômica Brasil (CCEB) scale,26 which was included in the body of the questionnaire and categorized students as A1, A2, B1, B2, C1, C2, D or E); (b) course description (e.g., area of study, academic year and study period); (c) academics (e.g., participation in academic activities and use of university facilities); and (d) academic performance and satisfaction with the chosen course of study.
The main outcome of interest was drug use, which was estimated over three different time periods: lifetime, last 12 months, and last 30 days. To assess the truthfulness of the responses, a fictitious drug called Relevin® was included in the questionnaire. If a participant claimed to have used it, the entire questionnaire was considered invalid and excluded from the data analysis.
To be consistent with the majority of studies that have examined the relationship between religiosity and drug use, this manuscript focused on the use of alcohol, tobacco, marijuana, and at least one illicit drug in the last 30 days.
Religious involvement was measured by the frequency with which the student claimed to go to ceremonies, services or other types of religious meetings. The students responded to the question, "Do you observe your religion?" The respondents were allowed to choose one of three possible responses: (a) No; (b) Yes, but only for special events; (c) Yes, at least once a month.
Participants
Throughout Brazil, 100 HEIs (88% of the estimated total) and 654 (70.6%) classes participated in the study. The response rate for students was 95.6%, for a total of 12,721 university students. Of these, 10 were excluded because they claimed to use Relevin®. Another 116 students were excluded from the data analysis because they did not answer questions about the frequency of their attendance at religious services. The final sample included 12,595 university students.
Groups
Of the total sample of university students, 30.6% reported that they were not attending religious services at the time of the interview, 30.2% were attending religious services occasionally (i.e., only for special events) and 39% were attending religious services at least once a month.
To be consistent with previous studies, the students that occasionally attended religious services and those who did not attend at all were grouped together in one group of non-frequent attenders (NFR; n = 7,232; 60.8%). This merging of categories was performed after the researchers ensured that there were no differences in alcohol or other drug use between the members of the two original groups. The students who attended religious services at least once a month were categorized as frequent attenders (FR; n = 5,322; 39.1%).
Statistical analysis
All valid questionnaires were entered into the SPSS program database. The responses were analyzed for consistency, and the database was checked. All of the estimates were weighted using sampling weights to represent the entire university student population in Brazil. Descriptive and inferential analyses were carried out using the R library survey software, 2.12.0. For numerical variables, intergroup comparisons were performed using a T-test. For categorical variables, intergroup comparisons were performed using Pearson's chi-square tests (χ2). The results were expressed as frequencies (%) with confidence intervals (95% CI). The null hypothesis was rejected at a significance level of p < .05. Subsequently, to verify the influence of religious involvement on drug use, the researchers developed individual multivariate logistic regression models for the use of alcohol, tobacco, marijuana and at least one illicit drug (marijuana included) in the last 30 days. In addition to religiosity (FR and NFR), other sociodemographic variables (gender, marital status, ethnicity, socioeconomic status (SES), and Brazilian administrative region) were included as covariates in each of the models. Non-significant variables (i.e. p > .05) were excluded from the models using backward stepwise elimination. The final models for each of the drugs are described in detail in the results section.
Ethics
This study was approved by the Research Ethics Committee of the Hospital das Clínicas, Universidade de São Paulo (CAPPesq HC-FMUSP, protocol 0378/08).
Results
Eighty-five percent of Brazilian university students reported some religious affiliation. Among these students, Catholicism was the most frequently cited religion (50.1%), followed by Evangelicalism/Protestantism (17.5%). Evangelical students were the most observant, attending religious services the most frequently (33.4%; p < .001) (Table 1).
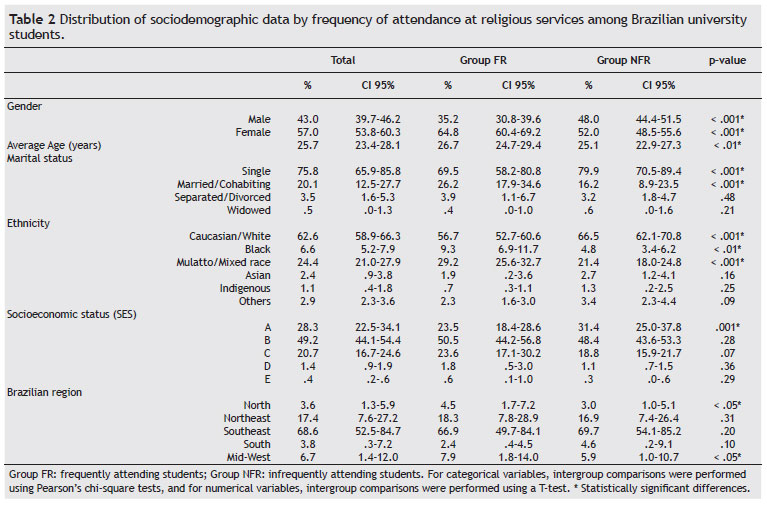
Table 2 shows the sociodemographic data that were associated with the frequency of attendance at religious services. Religious involvement was more common in slightly older (p < .01), married (p < .001), black (p < .01), mulatto (p < .001), and female students (p < .001) at institutions in the northern (p < .05) and central-western regions of Brazil (p < .05). Religious involvement was less common among white, single, and male students with high SES.
There were no differences between the FR and NFR groups in terms of the places they go besides the places where required academic activities take place. Thus, student unions, sports facilities, canteens and parks were equally frequented by the FR and NFR students. However, the FR students were more likely to frequent the library (p < .01). The NFR students were more likely to skip classes (p < .01). They generally spent that time with friends or dates (p < .01) or going to the cinema, clubs, beaches or other such places (p < .05). They also reported sleeping or resting (p < .001) or spending time in the student union when they weren't going to classes (p = .05).
Outside of the classroom, the NFR students spent more time fraternizing (p < .001), participating in physical activities (p < .001), watching television (p < .05), playing video games or computer games (p < .001), using the Internet for recreation (p < .01) or spending time on chat systems (p < .001). Conversely, a higher prevalence of students in the FR group spent their time doing volunteer work (p < .001). There were no differences between the groups in employment.
Table 3 shows that a higher percentage of the NFR students reported drinking (NFR: 8.2%; FR: 2.0%; p < .001) or using other drugs (NFR: 1.7%; FR: .2%; p < .001) when they skipped classes. Therefore, we measured the use of alcohol, tobacco, marijuana and at least one illicit drug (marijuana included) in the last 30 days.
Table 4 shows that over the last 30 days, the NFR students were more likely to report drinking (NFR: 80.3%; FR: 53.8%; p < .001) and using tobacco (NFR: 32.3%; FR: 13.6%; p < .001) than the FR students. Over the last 12 months, 32.6% of the NFR students reported using at least one other drug compared to 22.3% of the FR students (p < .001). The NFR students were also more likely to report marijuana use (NFR: 16.2%; FR: 6.0%; p < .001). The same findings were identified for drug use in the last 30 days. It is worth noting that 75.9% of the NFR students used at least one illicit drug in the last 30 days, while only 16.9% of the FR students reported doing so (p < .01).
Overall, religiosity remained in all of the logistic regression models for which 30-day drug use was the outcome variable. Not attending religious services was associated with drug use. Thus, as noted in Table 5, even after controlling for confounding variables, the NFR students reported alcohol use at higher rates than the FR students in the previous 30 days (OR = 2.52; p < .01). The odds ratios for tobacco, marijuana and other drugs were 2.83 (p < .001), 2.09 (p < .001), and 1.42 (p < .01), respectively.
Male students were more likely to have used alcohol (OR = 2.05; p < .001) and marijuana (OR = 1.44; p < .001) in the last 30 days compared to female students. Students between 18 and 34 years of age were more likely to have used alcohol and other drugs in the last 30 days than students younger than 18 years. Married students were less likely to have used marijuana in the last 30 days than single students (OR = .41; p < .001), and separated students were more likely than single students to have used other drugs (OR = 2.28, p < .001). The students from SES class A were more likely to have engaged in alcohol, tobacco, marijuana and other drug use in the last 30 days than the students from SES classes B and C. Finally, the students from southern Brazil were more likely to have used alcohol, tobacco and other drugs than the students from northern Brazil.
Discussion
Of the entire sample of Brazilian students, 85% reported some religious affiliation, and almost 40% of that group stated that they attend a religious activity at least monthly.
The distribution of the students' religions resembled the distribution of religions in the general Brazilian population, although there were some differences. In the most recent Brazilian census,27 92.6% of the general population claimed some religious affiliation. Only 7.4% had no religious affiliation. The percentage of university students with no religious affiliation was twice the percentage of Brazilians in the general population with no religious affiliation.27,28
As in the general Brazilian population, Catholicism, Evangelicalism and Spiritism were the most frequently reported religions among the university students,27,28 although some differences may be observed.
On the other hand, our findings are consistent with other studies of university students. Silva et al.22 found that 71% of Brazilian undergraduate students reported some religious affiliation and that 59.1% attended some religious services, similar to our findings. Moore et al.29 also found that nearly 59% of a sample of university students reported that they attend religious services at least once a month.
The differences between university students and the general population may be explained by differences in the age distribution. A multivariate analysis of recent survey data from a representative sample of the Brazilian population found that religious involvement was not associated with income and educational level but that religious involvement was more frequent among females and older people.28
The rates of 30-day drug use were higher among the NFR students, suggesting that religiosity may be a protective factor against drug use. In general, these findings are consistent with other regional Brazilian studies.21,22
It is important that we assessed the protective effect of religion with a measure of recent drug use (30-day drug use) because the other Brazilian studies measured drug use over the lifetime and in the last 12 months.21,22 The 30-day drug use measure is less vulnerable to memory bias than other drug use measures.
In addition, the protective effect of religion was observed for alcohol, tobacco, marijuana and other illicit drugs, consistent with a recent meta-analysis,30 regardless of how religiosity is defined.
However, some religions may be more protective than other religions. Our findings showed that Protestant students attended religious services more often than students from other religions, with the exception of Spiritists and Buddhists. This finding is consistent with other studies. Borini et al.21 showed that alcohol use was significantly lower among Protestant university students. Moreover, Protestants were not likely to be excessive drinkers, suggesting that more conservative religions are more protective against alcohol use. Further supporting these findings, a recent Brazilian study of adults 60 years and older showed that evangelical individuals were 51% less likely to use tobacco.23 Taken together, these findings highlight the need to investigate this issue more closely.
Although the protective role of religion is known, the mechanism by which it confers protection has not been elucidated. Some authors have suggested that religious teachings may be protective by exercising a direct influence on family structure or on an individual's personality or through instilling the values of respect and the sanctity of life.5,6,31,32
Among adolescents, the effects of religiosity on drug use may be mediated by better self-control and less tolerance for deviance.33 In addition, these effects may be mediated by higher levels of social support, especially from parents.20 In addition to religiosity, parental monitoring and parental norms also exert an influence on the behavior of adolescents, especially on substance use.12 In addition, other variables, such as gender and ethnicity, seem to modulate the relationship between religiosity and drug use,8-11 presenting an issue that warrants further study.
Among university students, the enhancement of spiritual well-being seems to be one of the intermediate factors in the relationship between religiosity and alcohol use.34 Abdel-Khalek35 reported that religious students reported higher subjective well-being, and Turner-Musa and Lipscomb36 noted that poor spiritual well-being increased the odds of smoking and alcohol use. Therefore, these studies may suggest that religiosity contributes to better quality of life among university students.37
Our results showed that the FR students were more likely to participate in normative activities, such as volunteer work or going to the library. The other students displayed more non-normative behaviors that may be risky under some circumstances. Religiosity may induce healthy and pro-social values and behaviors, protecting students from health-jeopardizing behaviors (including drug use) and improving the quality of life. However, this statement is only speculative, it was not supported by our findings. The mediators of the effect of religiosity on the health of university students are still unclear and warrant further study.
Higher socioeconomic status was actually found to be a factor for drug usage, not a protective factor. Thus, having a higher socioeconomic status increased one's odds of having engaged in drug use over the last 30 days. This relationship was also found by Silva et al.22 According to their study, the university students from higher income families were more vulnerable to alcohol and drug use in the last 12 months. On the other hand, the university students of lower socioeconomic status reported less alcohol and drug use. The same relationship was also described among Brazilian adolescents. Tavares et al.18 have suggested that there is a linear relationship between drug use and socioeconomic status, such that the prevalence ratio for drug use decreased from the upper to the lower social classes. This relationship deserves further study, especially as it relates to religiosity.
Our research has limitations, but the findings are encouraging. There continues to be an enormous unmet need for drug use prevention and treatment, particularly in developing countries. The results of our study may help to draft and update clinical practices in the field of alcohol and drug use in Brazil and to develop public policies for university students. Investigating these relationships among university students would be of great value, as they are the subgroup that uses drugs most frequently.38,39
The incorporation of spiritual aspects into university prevention and treatment programs may help reduce the rates of alcohol and drug use by students in the university setting. Moreover, it is possible that encouraging university students to improve their spiritual health may help to alleviate the potentially deadly consequences of alcohol and drug use. Finally, religiosity may be incorporated into interventions to reduce risky sexual behaviors, as the effects of religiosity on these behaviors have also been suggested.
Limitations
This study has some limitations. The cross-sectional design limited our ability to assess a causal relationship between religiosity and substance use. The data were mainly student-reported, and the students may have under- or overestimated their alcohol and drug use. Finally, psychiatric comorbidities were not evaluated, and it is important to understand how they may interfere with the relationships evaluated. The findings reported here might not be generalizable to the entire population of Brazilian students.
Conclusion
To our knowledge, our study is the first to show that religious involvement is a protective factor against drug use in a nationwide sample of Brazilian university students. This finding corroborates the studies that have been conducted in other countries and expands on the existing data from regional studies in Brazil. Perhaps religious involvement is a protective factor because it promotes meaning and the adoption of normative values and behaviors for a healthy life. However, the mechanism is still unclear. Because religious involvement has emerged as a strong and consistent protective factor against drug use, investigating the "active ingredients" that enable religious involvement to prevent drug use will be a very important task for future studies. This research has the potential to identify targets for prevention, treatment, and rehabilitation strategies. In addition, religious communities may be mobilized for public health interventions regarding substance use, as preliminary studies have shown positive outcomes for health interventions provided by faith-based organizations. Some of these initiatives have started in Brazil (e.g., the course "Drug use prevention in religious institutions and similar movements - Faith in prevention", a joint initiative of the Brazilian National Secretariat for Drug Policies [Secretaria Nacional de Políticas sobre Drogas - SENAD] and the Universidade Federal de São Paulo [UNIFESP]). Finally, another issue that deserves further investigation is the impact of therapeutic communities run by religious groups in Brazil, which are attended by thousands of patients with substance dependence. In summary, as religious involvement has consistently emerged as one of the strongest protective factors against drug use, the current challenge is to identify the mechanisms behind this relationship and to develop public health strategies that use this knowledge to decrease drug use.
Acknowledgements
We thank the National Secretariat for Drug Policies (SENAD; 19/2008) and the Research Support Foundation of the State of São Paulo (FAPESP; 08/55550-7) for their financial support, as well as the Interdisciplinary Group for Studies on Alcohol and Drugs (GREA/FMUSP).
Received on August 24, 2011; accepted on May 15, 2012

- 1. United Nations Office on Drugs and Crime - UNODC. World Drug Report: 2008. New York: United Nations; 2008.
- 2. World Health Organization (WHO).Global status report on alcohol and health. Geneva: World Health Organization; 2011.
- 3. World Health Organization (WHO). Global Status Report on Alcohol. Geneva: World Health Organization; 2004.
- 4. Terry-McElrath YM, Emery S, Szczypka G, Johnston LD. Potential exposure to anti-drug advertising and drug-related attitudes, beliefs, and behaviors among United States youth, 1995-2006. Addict Behav. 2011;36(1-2):116-24.
- 5. Van der Meer Sanchez Z, De Oliveira LG, Nappo SA. Religiosity as a protective factor against the use of drugs. Subst Use Misuse. 2008;43(10):1476-86.
- 6. Edlund MJ, Harris KM, Koenig HG, Han X, Sullivan G, Mattox R, et al. Religiosity and decreased risk of substance use disorders: is the effect mediated by social support or mental health status? Soc Psychiatry Epidemiol. 2010;45(8):827-36.
- 7. Moreira-Almeida A, Neto FL, Koenig HG. Religiousness and mental health: a review. Rev Bras Psiquiatr. 2006;28(3):242-50.
- 8. Chen CY, Dormitzer CM, Bejarano J, Anthony JC. Religiosity and the earliest stages of adolescent drug involvement in seven countries of Latin America. Am J Epidemiol. 2004;159(12):1180-8.
- 9. Piko BF, Fitzpatrick KM. Substance use, religiosity, and other protective factors among Hungarian adolescents. Addict Behav. 2004;29(6):1095-107.
- 10. Wallace JM Jr, Delva J, O'Malley PM, Bachman JG, Schulenberg JE, Johnston LD, et al. Race/ethnicity, religiosity and adolescent alcohol, cigarette and marijuana use. Soc Work Public Health. 2007;23(2-3):193-213.
- 11. Steinman KJ, Ferketich AK, Sahr T. The dose-response relationship of adolescent religious activity and substance use: variation across demographic groups. Health Educ Behav. 2008;35(1):22-43
- 12. Parsai M, Kulis S, Marsiglia FF. Parental Monitoring, Religious Involvement and Drug Use Among Latino and Non-Latino Youth in the Southwestern United States. Br J Soc Work. 2010;40(1):100-14.
- 13. Parfrey PS. The effect of religious factors on intoxicant use. Scand J Soc Med. 1976;4(3):135-40.
- 14. Engs RC. The drug-use patterns of helping-profession students in Brisbane, Australia. Drug Alcohol Depend. 1980;6(4):231-46.
- 15. Strote J, Lee JE, Wechsler H. Increasing MDMA use among college students:results of a national survey. J Adolesc Health. 2002;30(1):64-72.
- 16. Luna A, Osuna E, Zurera L, Garcia Pastor MV, Castillo del Toro L. The relationship between the perception of alcohol and drug harmfulness and alcohol consumption by university students. Med Law. 1992;11(1-2):3-10.
- 17. Cook CC. Addiction and spirituality. Addiction. 2004;99(5):539-51. Erratum in: Addiction. 2006;101(5):761.
- 18. Tavares BF, Beria JU, Lima MS. Prevalência do uso de drogas e desempenho escolar entre adolescentes. Rev Saúde Pública. 2001;35(2):150-8.
- 19. Dalgalarrondo P, Soldera MA, Corrêa Filho HR, Silva CA. Religion and drug use by adolescents. Rev Bras Psiquiatr. 2004;26(2):82-90.
- 20.Sanchez ZM, Opaleye ES, Chaves TV, Noto AR, Nappo SA. God forbids or mom disapproves? religious beliefs that prevent drug use among youth. J Adolesc Res. 2011;26(5):591-616.
- 21. Borini P, Oliveira CM, Martins MG, Guimarães RC. Padrão de uso de bebidas alcoólicas de estudantes de medicina (Marília, São Paulo): parte 1. J Brasileiro de Psiquiatria. 1994;43(2):93-103.
- 22. Silva LV, Malbergier A, Stempliuk V A, Andrade AG. Factors associated with drug and alcohol use among university students. Rev Saúde Pública. 2006;40(2):280-8.
- 23. Blay SL, Batista AD, Andreoli SB, Gastal FL. The relationship between religiosity and tobacco, alcohol use, and depression in an elderly community population. Am J Geriatr Psychiatry. 2008;16(11):934-43.
- 24. Andrade AG, Duarte PCAV, Oliveira LG. 1st Nationwide Survey on the Use of Alcohol, Tobacco and Other Drugs among College Students in the 27 Brazilian State Capitals. Brasília: SENAD; 2010. Available from: URL http://www.obid.senad.gov.br/portais/OBID/index.php
- 25. Stempliuk V A, Barroso LP, Andrade AG, Nicastri S, Malbergier A. Comparative study of drug use among undergraduate students at the University of São Paulo-São Paulo campus in 1996 and 2001. Rev Bras Psiquiatr. 2005;27(3):185-93.
- 26. ABEP. Critério de Classificação Econômica Brasil. Associação Brasileira de Empresas de Pesquisa; 2008 [cited 2011 Jun 20]; Available from: URL: http://www.abep.org/novo/Content.aspx?ContentID=302
-
27IBGE Instituto Brasileiro de Geografia e Estatística. 2000. [text on the internet]. [cited 2010 Aug 12]. Available from: http://pt.wikipedia.org/wiki/Religi%C3%B5es_no_Brasil
» link - 28. Moreira-Almeida A, PinskyI, Zaleski M, Laranjeira R. Religious involvement and sociodemographic factors: a Brazilian national survey. Rev Psiq Clín. 2010;37(1):12-15.
- 29. Moore EW, Berkley-Patton JY, Hawes SM. Religiosity, Alcohol Use, and Sex Behaviors Among College Student-Athletes. J Relig Health. 2011 Oct. [Epub ahead of print]
- 30. Yeung JW, Chan YC, Lee BL. Youth religiosity and substance use: a meta-analysis from 1995 to 2007. Psychol Rep. 2009;105(1):255-66.
- 31. Geppert C, Bogenschutz MP, Miller WR. Development of a bibliography on religion, spirituality and addictions. Drug Alcohol Rev. 2007;26(4):389-95.
- 32. King MB, Koenig HG. Conceptualising spirituality for medical research and health service provision. BMC Health Serv Res. 2009;13(9):1-7
- 33. Walker C, Ainette MG, Wills TA, Mendoza D. Religiosity and substance use: test of an indirect-effect model in early and middle adolescence. Psychol Addict Behav. 2007;21(1):84-96.
- 34. Johnson TJ, Sheets VL, Kristeller JL. Identifying mediators of the relationship between religiousness/spirituality and alcohol use. J Stud Alcohol Drugs. 2008;69(1):160-70.
- 35. Abdel-Khalek AM. Subjective well-being and religiosity in Egyptian college students. Psychol Rep. 2011;108(1):54-8.
- 36. Turner-Musa J, Lipscomb L. Spirituality and social support on health behaviors of african american undergraduates. Am J Health Behav. 2007;31(5):495-501.
- 37. Abdel-Khalek AM. Quality of life, subjective well-being, and religiosity in Muslim college students. Qual Life Res. 2010;19(8):1133-43.
- 38. Johnston, L.D., O'Malley, P.M., Bachman, J.G. & Schulenberg, J.E. Monitoring the Future National survey results on drug use, 1975-2008: College students and adults age 19-50. NIH Publication No. 09-7403. Bethesda, MD: National Institute on Drug Abuse; 2009.
- 39. Oliveira LG, Galduróz JCF, Wagner GA, Andrade AG. Uso de drogas pelos universitários brasileiros: contexto nacional e internacional. In: Arthur Guerra de Andrade, Paulina do Carmo Arruda Vieira Duarte, Lúcio Garcia de Oliveira. (Org.). I Levantamento Nacional sobre o uso de Álcool, Tabaco e outras Drogas entre Universitários das 27 Capitais Brasileiras. 1Ş ed. Brasília - DF:, 2010, p. 181-96.
Corresponding author:
Publication Dates
-
Publication in this collection
04 Apr 2013 -
Date of issue
Mar 2013
History
-
Received
24 Aug 2011 -
Accepted
15 May 2012