Abstract
Objective:
To validate the Rowland Universal Dementia Assessment Scale for use in Brazil (RUDAS-BR).
Methods:
We first completed an English-Brazilian Portuguese translation and back-translation of the RUDAS. A total of 135 subjects over 60 years of age were included: 65 cognitively healthy and 70 with Alzheimer’s disease (AD) according to the DSM-IV and Neurological and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria. All participants completed an interview and were screened for depression. The receiver operating characteristic curves of the RUDAS were compared with those of the Mini Mental State Examination (MMSE) regarding the sensitivity and specificity of cutoffs, taking education into consideration.
Results:
The areas under the curve were similar for the RUDAS-BR (0.87 [95%CI 0.82-0.93]) and the MMSE (0.84 [95%CI 0.7-0.90]). RUDAS-BR scores < 23 indicated dementia, with sensitivity of 81.5% and specificity of 76.1%. MMSE < 24 indicated dementia, with sensitivity of 72.3% and specificity of 78.9%. The cutoff score was influenced by years of education on the MMSE, but not on the RUDAS-BR.
Conclusions:
The RUDAS-BR is as accurate as the MMSE in screening for dementia. RUDAS-BR scores were not influenced by education. The RUDAS-BR may improve the cognitive assessment of older persons who are illiterate or of lower educational attainment.
Dementia; Alzheimer’s disease; education; psychiatric; tests/interviews; psychometric; cognitive neuroscience; diagnosis and classification
Introduction
Dementia represents a significant problem in older adults, impacting personal, family, and social welfare by increasing costs to the healthcare system and family economy.11. Wimo A, Jönsson L, Bond J, Prince M, Winblad B; Alzheimer Disease International. The worldwide economic impact of dementia 2010. Alzheimers Dement. 2013;9:1-11. However, diagnosing dementia and cognitive disorders requires a complex workup including neuropsychological assessment for the purpose of screening and assessing the severity of limitations present in specific domains.22. McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH, et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:263-9.
Low literacy and educational attainment are important risk factors for dementia,33. Caamaño-Isorna F, Corral M, Montes-Martínez A, Takkouche B. Education and dementia: a meta-analytic study. Neuroepidemiology. 2006;26:226-32.,44. Farfe JM, Nitrini R, Suemoto CK, Grinberg LT, Ferretti RE, Leite RE, et al. Very low levels of education and cognitive reserve: a clinicopathologic study. Neurology. 2013;81:650-7. whereas higher education may be protective by contributing to cognitive reserve throughout the lifespan.55. EClipSE Collaborative Members, Brayne C, Ince PG, Keage HA, McKeith IG, Matthews FE, et al. Education, the brain and dementia: neuroprotection or compensation? Brain. 2010;133:2210-16.,66. Liu Y, Julkunen V, Paajanen T, Westman E, Wahlund LO, Aitken A, et al. Education increases reserve against Alzheimer’s disease--evidence from structural MRI analysis. Neuroradiology. 2012;54:929-38. Lower education impacts performance on a number of neuropsychological tests, particularly when test items tap into domains that are sensitive to specific knowledge and abilities acquired in school.77. Ardila A, Bertolucci PH, Braga LW, Castro-Caldas A, Judd T, Kosmidis MH, et al. Illiteracy: the neuropsychology of cognition without reading. Arch Clin Neuropsychol. 2010;25:689-712.,88. Pawlowski J, Remor E, Parente MADMP, Salles JF, Fonseca RP, Bandeira DR. The influence of reading and writing habits associated with education on the neuropsychological performance of Brazilian adults. Read Writ. 2012;25:2275-89.
This issue directly impacts diagnostic accuracy for dementia and cognitive disorders in the Brazilian older adult population. Several publications have dealt with the issue by trying to establish distinct cutoff scores for higher and lower education levels, mainly with the Mini Mental State Examination (MMSE).99. Laks J, Baptista EM, Contino AL, de Paula EO, Engelhardt E. Mini-Mental State Examination norms in a community-dwelling sample of elderly with low schooling in Brazil. Cad Saude Publica. 2007;23:315-9.,1010. Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. [The Mini-Mental State Examination in a general population: impact of educational status]. Arq Neuropsiquiatr. 1994;52:1-7. The MMSE is the most commonly used instrument for cognitive screening; however, its validity is not fully clear when used among patients with low education.1010. Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. [The Mini-Mental State Examination in a general population: impact of educational status]. Arq Neuropsiquiatr. 1994;52:1-7.
11. Laks J, Batista EM, Guilherme ER, Contino AL, Faria ME, Figueira I, et al. [Mini-mental state examination in community-dwelling elderly: preliminary data from Santo Antônio de Pádua, Rio de Janeiro, Brazil]. Arq NeuroPsiquiatr. 2003;61:782-5.
12. Brucki SM, Nitrini R, Caramelli P, Bertolucci PH, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq NeuroPsiquiatr. 2003;61:777-81.-1313. Nielsen TR, Vogel A, Gade A, Waldemar G. Cognitive testing in non-demented Turkish immigrants – comparison of the RUDAS and the MMSE. Scand J Psychol. 2012;53:455-60.
The Rowland Universal Dementia Assessment Scale (RUDAS) was developed in Australia as an easily administered test for detecting dementia across different cultures that can be quickly conducted by primary health care clinicians.1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31. The RUDAS is short, consisting of six items that assess multiple cognitive domains (including attention, language, memory and visuospatial abilities). RUDAS scores range from zero to 30 points, and the test can be administered in less than 10 minutes.1515. Naqvi RM, Haider S, Tomlinson G, Alibhai S. Cognitive assessments in multicultural populations using the Rowland Universal Dementia Assessment Scale: a systematic review and meta-analysis. CMAJ. 2015;187:E169-75.
In the initial study, the authors found that the RUDAS can be directly translated into other languages, without the need to change the structure or format of any item.1313. Nielsen TR, Vogel A, Gade A, Waldemar G. Cognitive testing in non-demented Turkish immigrants – comparison of the RUDAS and the MMSE. Scand J Psychol. 2012;53:455-60. The RUDAS has already been translated and utilized in different countries.1616. Iype T, Ajitha BK, Antony P, Ajeeth NB, Job S, Shaji KS. Usefulness of the Rowland universal dementia assessment scale in South India. J Neurol Neurosurg Psychiatry. 2006;77:513-4.
17. Rowland JT, Basic D, Storey JE, Conforti DA. The Rowland universal dementia assessment scale (RUDAS) and the Folstein MMSE in a multicultural cohort of elderly persons. Int Psychogeriatr. 2006;18:111-20.
18. Limpawattana P, Tiamkao S, Sawanyawisuth K, Thinkhamrop B. Can Rowland universal dementia assessment scale (RUDAS) replace mini-mental state examination (MMSE) for dementia screening in a Thai geriatric outpatient setting? Am J Alzheimers Dis Other Demen. 2012;27:254-9.-1919. Nielsen TR, Andersen BB, Gottrup H, Lützhøft JH, Høgh P, Waldemar G. Validation of the Rowland universal dementia assessment scale for multicultural screening in Danish memory clinics. Dement Geriatr Cogn Disord. 2013;36:354-62. It is a useful cognitive evaluation tool for patients with suspected cognitive impairment and may be particularly preferable in patients from culturally and linguistically diverse populations, and among people with low or no education.1313. Nielsen TR, Vogel A, Gade A, Waldemar G. Cognitive testing in non-demented Turkish immigrants – comparison of the RUDAS and the MMSE. Scand J Psychol. 2012;53:455-60.,1515. Naqvi RM, Haider S, Tomlinson G, Alibhai S. Cognitive assessments in multicultural populations using the Rowland Universal Dementia Assessment Scale: a systematic review and meta-analysis. CMAJ. 2015;187:E169-75.
The cutoff score for RUDAS in different countries is similar. The optimal cutoff score in Australia,1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31. Denmark1919. Nielsen TR, Andersen BB, Gottrup H, Lützhøft JH, Høgh P, Waldemar G. Validation of the Rowland universal dementia assessment scale for multicultural screening in Danish memory clinics. Dement Geriatr Cogn Disord. 2013;36:354-62. and Malaysia2020. Shaaban J, Aziz AA, Abdullah Z, Ab Razak A. Validation of the Malay version of Rowland universal dementia assessment scale (MRUDAS) among elderly attending primary care clinic. Int Med J. 2013;20:555-8. was 23 points. In the Thai and Arabic versions, the optimal cutoff scores were found to be 24 and 22, respectively.1818. Limpawattana P, Tiamkao S, Sawanyawisuth K, Thinkhamrop B. Can Rowland universal dementia assessment scale (RUDAS) replace mini-mental state examination (MMSE) for dementia screening in a Thai geriatric outpatient setting? Am J Alzheimers Dis Other Demen. 2012;27:254-9.,2121. Chaaya M, Phung TK, El Asmar K, Atweh S, Ghusn H, Khoury RM, et al. Validation of the Arabic Rowland universal dementia assessment scale (A-RUDAS) in elderly with mild and moderate dementia. Aging Ment Health. 2016;20:880-7. In Denmark, Nielsen et al.1919. Nielsen TR, Andersen BB, Gottrup H, Lützhøft JH, Høgh P, Waldemar G. Validation of the Rowland universal dementia assessment scale for multicultural screening in Danish memory clinics. Dement Geriatr Cogn Disord. 2013;36:354-62. evaluated the diagnostic accuracy of the RUDAS in a multicultural sample from a memory clinic and determined an optimal cutoff score of 24 points.
In the original Australian version,1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31. the sensitivity and specificity were 89% and 98%, respectively. In Denmark,1919. Nielsen TR, Andersen BB, Gottrup H, Lützhøft JH, Høgh P, Waldemar G. Validation of the Rowland universal dementia assessment scale for multicultural screening in Danish memory clinics. Dement Geriatr Cogn Disord. 2013;36:354-62. a sensitivity of 69% and a specificity of 80% were observed, and in RUDAS-Thai2020. Shaaban J, Aziz AA, Abdullah Z, Ab Razak A. Validation of the Malay version of Rowland universal dementia assessment scale (MRUDAS) among elderly attending primary care clinic. Int Med J. 2013;20:555-8. a sensitivity and specificity of 78.7% and 60.7%, respectively, obtained. In the Arabic version,2121. Chaaya M, Phung TK, El Asmar K, Atweh S, Ghusn H, Khoury RM, et al. Validation of the Arabic Rowland universal dementia assessment scale (A-RUDAS) in elderly with mild and moderate dementia. Aging Ment Health. 2016;20:880-7. good sensitivity (83%) and specificity (85%) were also evident.
The issue of diagnosing and assessing less educated persons with dementia or other cognitive disorders has not yet been resolved in Brazil. In order to bridge this gap, we aimed to validate the RUDAS considering educational level. This study presents the Brazilian Portuguese validation of the RUDAS (RUDAS-BR).
Methods
Translation and back-translation of the Rowland Universal Dementia Assessment Scale (RUDAS)
Initially, a translation of the original English version of the RUDAS into Brazilian Portuguese was performed by an independent translator who was fluent in both English and Brazilian Portuguese. The translator had no prior knowledge of neuropsychology or cognitive instruments. The back translation was performed by a bilingual psychiatrist with knowledge of cognitive instruments. The objective was to check for any conceptual errors in translation. The experimental version of the RUDAS-BR was tested for comprehensibility with four subjects, two healthy older adults (one with ≤ 4 years of education, the other with ≥ 8 years of education) and two patients diagnosed with Alzheimer disease (AD; one with ≤ 4 years of education, the other with ≥ 8 years of education). Based on this pilot study, it was determined that the translated RUDAS-BR (online-only supplementary material, Appendix 1) demonstrated adequate comprehensibility and no changes to the original items of the RUDAS were necessary.
Participants
Study participants were selected according to the following inclusion criteria: a minimum age of 60, either with or without dementia. The exclusion criteria included: comorbid neurological or psychiatric disorders, as well as physical limitations or visual or hearing impairment that precluded cognitive testing. Subjects with depressive symptoms that did not fulfill the clinical criteria for a depressive disorder were not excluded. A total of 135 elderly individuals (≥ 60 years) comprised the final sample, including 65 healthy older adults and 70 older adults with AD.
The 70 AD patients were recruited from a university center and a military hospital. Clinical diagnosis of AD according to the DSM-IV2222. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). Arlington: American Psychiatric Publishing; 1994. and National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA)22. McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH, et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:263-9. was required, with a mild or moderate stage of severity according to the Clinical Dementia Rating (CDR).2323. Chaves ML, Camozzato AL, Godinho C, Kochhann R, Schuh A, de Almeida VL, et al. Validity of the clinical dementia rating scale for the detection and staging of dementia in Brazilian patients. Alzheimer Dis Assoc Disord. 2007;21:210-7. The diagnostic workup for the AD patients included complete blood cell count, platelet count, glycemia, triglycerides, total cholesterol and fractions, alkaline phosphatase, glutamic oxaloacetic transaminase and glutamic pyruvic transaminase, bilirubins, urea, creatinine, total proteins, calcium, free T4 levels, TSH, VDRL, and dosage of B12 and folates. Cranial Computed Tomography scan or magnetic resonance imaging scan with or without spectroscopy was also performed.
The control group was recruited from a research center on aging, a private hospital, and a military hospital. Control participants were determined to be cognitively normal by clinical evaluation and the MMSE, without neurological or psychiatric diseases. Neurological or psychiatric diseases were evaluated during the clinical assessment. Imaging and laboratory evaluation were required of all patients.
Procedures
This study was approved by the ethics committees of Instituto de Psiquiatria, Universidade Federal do Rio de Janeiro, and Hospital Naval Marcílio Dias, and all participants provided written informed consent before any procedure took place.
All participants completed a session ofapproximately 90 minutes, which included a structured interview to collect demographic, physical, and mental health data,as well as screening for depression (Geriatric Depression Scale-15 [GDS-15]),2424. Almeida OP, Almeida SA. [Reliability of the Brazilian version of the ++abbreviated form of Geriatric Depression Scale (GDS) short form]. Arq Neuropsiquiatr. 1999;57:421-6. cognition (MMSE)1212. Brucki SM, Nitrini R, Caramelli P, Bertolucci PH, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq NeuroPsiquiatr. 2003;61:777-81. and the RUDAS-BR.
Interview and instruments
The interview consisted of questions regarding demographic, physical, mental health status data, health self-perception, and memory self-perception. Demographic data included age, years of education, marital status, previous occupation, and number of children. The health information component involved the participant’s history of clinical and neuropsychiatric diseases and lifestyle. The GDS-152525. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982-1983;17:37-49. is a self-report instrument with a dichotomous response format (yes/no), which is commonly used for clinical work and research. The 15-item version was used for this study. The cutoff used was 6 points.2424. Almeida OP, Almeida SA. [Reliability of the Brazilian version of the ++abbreviated form of Geriatric Depression Scale (GDS) short form]. Arq Neuropsiquiatr. 1999;57:421-6. The MMSE2626. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-98. is a brief screening test for cognitive abilities that evaluates orientation, attention, concentration, memory, calculation, language, and praxis, with scores ranging from 0 to 30.1010. Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. [The Mini-Mental State Examination in a general population: impact of educational status]. Arq Neuropsiquiatr. 1994;52:1-7. The cutoff used was 13 points for illiterate participants, 18 points for those with an elementary or middle education level (< 8 years), and 26 points for those with a high education level (> 8 years).1010. Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. [The Mini-Mental State Examination in a general population: impact of educational status]. Arq Neuropsiquiatr. 1994;52:1-7.
The RUDAS is a brief cognitive instrument consisting of six items which test memory (registration and recall), body orientation, praxis, drawing, judgment, and language, adding up to a total score of 30. Lower scores indicate poorer cognitive function.1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31. The administration and scoring guide for the original version are available online.2727. NSW Health Department, Department of Ageing, Disability and Home Care. RUDAS: Rowland Universal Dementia Assessment Scale: a multicultural cognitive assessment scale. Administration and scoring guide. 2001 [cited 2017 Mar 24]. https://www.fightdementia.org.au/sites/default/files/20110311_2011RUDASAdminScoringGuide.pdf.
https://www.fightdementia.org.au/sites/d...
Statistical analysis
Descriptive statistics were used for the demographic and clinical characteristics of the AD patients and the control group. ROC curve analysis was used to compare the accuracy of the RUDAS and the MMSE for diagnosing AD. Sensitivity, specificity, positive likelihood ratio (LR) and negative LR were calculated using Stata 14. The positive likelihood ratio was calculated as the ratio between the proportion of true positives and the proportion of false positives. The negative LR was obtained by dividing the proportion of false negatives by the proportion of true negatives. Values greater than one are desirable for the positive likelihood ratio, and values less than zero are appropriate for the negative likelihood ratio. The optimal cutoff score was determined for the RUDAS and MMSE by balancing sensitivity and specificity/according to Youden Index score. To assess the impact of education, these analyses were repeated in groups with low education (≤ 4 years of education) and high education (≥ 8 years of education). Differences in which p ≤ 0.05 were considered statistically significant. The RUDAS percentiles were calculated. Internal consistency was calculated with Cronbach’s alpha coefficient.
All statistical analysis was performed in Stata14.
Results
Details of the clinical and sociodemographic data are shown in Table 1. The AD group was significantly older than the control group, but there was no statistically significant difference in educational level. In the AD group, 10% were illiterate, whereas in the control group, 25.8% were illiterate. While most participants in the control group were widowed, the majority of participants in the AD group were married. In both groups, the majority of the participants considered their overall health as good and considered their memory as “more or less” good. In the AD group, 80% of the sample had mild AD.
The RUDAS-BR scores were as follows: the 5th percentile was 12; the 10th percentile was 14; the 25th percentile was 19; the 50th percentile was 23; the 75th percentile was 26; the 90th percentile was 28; the 95th percentile was 29; and the 99th percentile was 30. The internal consistency of the MMSE and the RUDAS were similar (0.69 and 0.54, respectively).
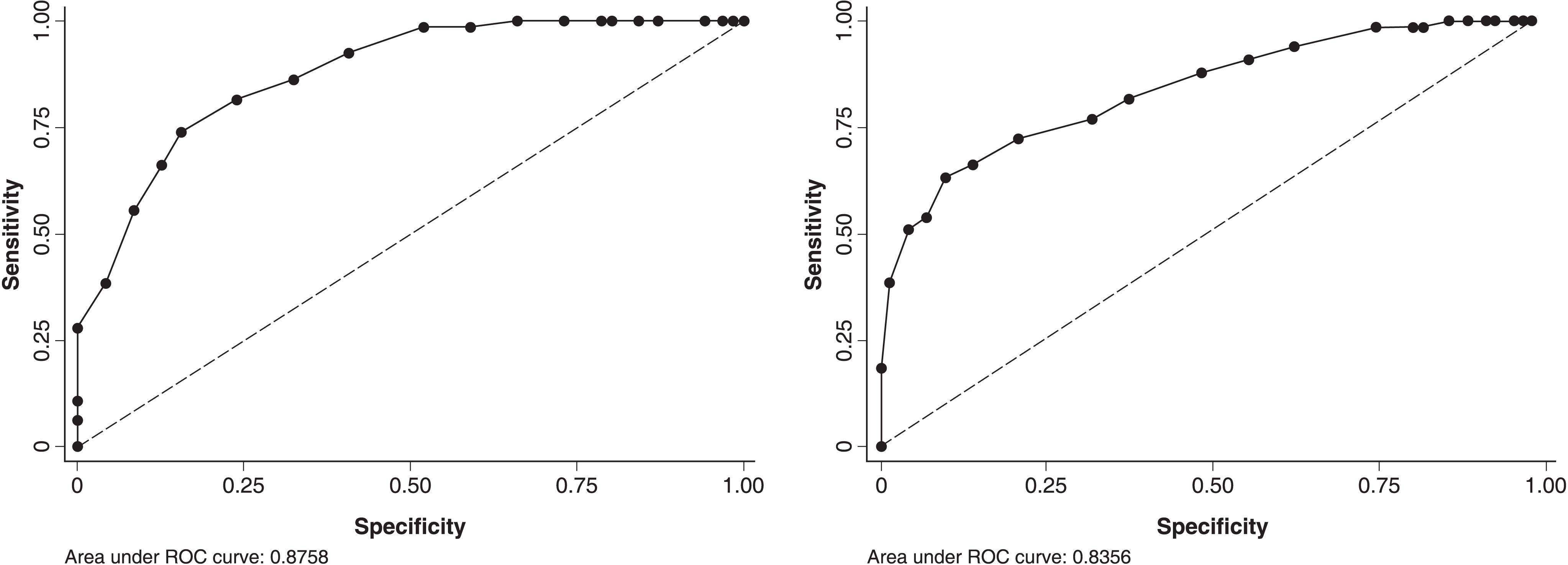
The diagnostic accuracy of the RUDAS-BR (i.e., the ability to correctly classify cognitive impairment in AD based on DSM-IV and NINCDS-ADRDA criteria) showed an area under the curve (AUC) of 0.87 (95% confidence interval [95%CI] 0.82-0.93) (Figure 1). RUDAS scores < 23 (the optimal cutoff based on the ROC curve) detected dementia with a sensitivity of 81.54% and a specificity of 76.1%, LR+ was 3.41 and LR- was 0.24 (Table 2 and Figure 1). The diagnostic accuracy of the MMSE showed an AUC of 0.84 (95%CI 0.77-0.90) (Figure 1). A MMSE score < 24 classified AD with a sensitivity of 72.3%, a specificity of 78.9%, LR+ was 3.42 and LR- was 0.35 (Table 2 and Figure 1).
Receiver operating characteristic (ROC) curve for the Rowland Universal Dementia Assessment Scale (RUDAS) and Mini Mental State Examination (MMSE).
We further analyzed the data according to the participants’ years of education, defining low education as ≤ 4 years and high education as ≥ 8 years. The accuracy of the RUDAS in the low education group (n=69) showed an AUC of 0.82 (95%CI 0.72-0.91) (Figure 2). RUDAS scores < 23 detected dementia with a sensitivity of 67.7%, a specificity of 79%, LR+ was 3.21 and LR- was 0.41. The accuracy of the MMSE in the low educational group showed an AUC of 0.75 (95%CI 0.64-0.86) (Figure 2). MMSE scores < 21 classified AD with a sensitivity of 74.19%, a specificity of 60.53%, LR+ was 1.88 and LR- was 0.43 (Table 2 and Figure 2).
Receiver operating characteristic (ROC) curve for the Rowland Universal Dementia Assessment Scale (RUDAS) and Mini Mental State Examination (MMSE) for subjects with low education.
The accuracy of the RUDAS in the high education group showed an AUC of 0.92 (95%CI 0.86-0.98) (Figure 3). RUDAS scores < 24 classified AD with a sensitivity of 91.2%, a specificity of 81.8%, LR+ was 5.0 and LR- was 0.11 (Table 2). The accuracy of the MMSE in the high education group showed an AUC of 0.97 (95%CI 0.93-1.00) (Figure 3). MMSE scores < 26 classified AD with a sensitivity of 94.12%, a specificity of 87.88%, LR+ was 7.78 and LR- was 0.07 (Table 2 and Figure 3).
Receiver operating characteristic (ROC) curve for the Rowland Universal Dementia Assessment Scale (RUDAS) and Mini Mental State Examination (MMSE) for subjects with high education.
See online-only supplementary material, Appendix 2, for detailed reports on RUDAS and MMSE sensitivity and specificity.
Discussion
The current study presents a validated version of the RUDAS for use in Brazil, which is compared with the MMSE to describe its diagnostic accuracy for detecting dementia in older adults.
The English-Brazilian Portuguese translation and back-translation demonstrated an adequate comprehensibility, and no further changes to the original RUDAS items were needed. The optimal cutoff score suggested in original article was < 23 points,1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31. and our data is in line with that finding. Overall, data on sensitivity, specificity, and LR+ and LR- for RUDAS-BR (scores < 23) and MMSE (scores < 24) were similar. The AUCs of 0.82 for the RUDAS-BR and 0.84 for the MMSE.
It is worth noting, however, that in contrast to the MMSE, the optimal cutoff for diagnostic accuracy using the RUDAS-BR does not substantially vary due to educational level. In the current study, the RUDAS cutoff was ≤ 23 for those with a low level of education and 24 for those with a high level of education. This is in contrast with the highly disparate cutoffs suggested for the MMSE, 21 points for those with a low level of education and 26 points for those with a high level of education. The influence of education on the MMSE has been previously noted in other Brazilian studies.1010. Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. [The Mini-Mental State Examination in a general population: impact of educational status]. Arq Neuropsiquiatr. 1994;52:1-7.
11. Laks J, Batista EM, Guilherme ER, Contino AL, Faria ME, Figueira I, et al. [Mini-mental state examination in community-dwelling elderly: preliminary data from Santo Antônio de Pádua, Rio de Janeiro, Brazil]. Arq NeuroPsiquiatr. 2003;61:782-5.-1212. Brucki SM, Nitrini R, Caramelli P, Bertolucci PH, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq NeuroPsiquiatr. 2003;61:777-81.,2828. Caramelli P, Herrera E Jr, Nitrini R. O mini-exame do estado mental no diagnóstico de demência em idosos analfabetos. Arq Neuropsiquiatr. 1999;57:7-12. Previous research has also demonstrated that educational level does not influence the RUDAS.1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31.,1717. Rowland JT, Basic D, Storey JE, Conforti DA. The Rowland universal dementia assessment scale (RUDAS) and the Folstein MMSE in a multicultural cohort of elderly persons. Int Psychogeriatr. 2006;18:111-20.,1919. Nielsen TR, Andersen BB, Gottrup H, Lützhøft JH, Høgh P, Waldemar G. Validation of the Rowland universal dementia assessment scale for multicultural screening in Danish memory clinics. Dement Geriatr Cogn Disord. 2013;36:354-62.,2929. Basic D, Rowland JT, Conforti DA, Vrantsidis F, Hill K, LoGiudice D, et al. The validity of the Rowland universal dementia assessment scale (RUDAS) in a multicultural cohort of community-dwelling older persons with early dementia. Alzheimer Dis Assoc Disord. 2009;23:124-9.
Furthermore, for individuals with a low level of education, the AUC of the MMSE was 0.75 and that of the RUDAS was 0.82, which indicates that the RUDAS is more accurate than the MMSE in the low education group. The AUCs were similar for both instruments in the higher education group (0.92 and 0.97 for the RUDAS and MMSE, respectively). In the low education group, the RUDAS-BR ROC is better than that of the MMSE, although not significantly different.
To the best of our knowledge, the present study is the first to demonstrate this phenomenon in a Brazilian sample.
In the original1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31. and the Malay2020. Shaaban J, Aziz AA, Abdullah Z, Ab Razak A. Validation of the Malay version of Rowland universal dementia assessment scale (MRUDAS) among elderly attending primary care clinic. Int Med J. 2013;20:555-8. versions, the optimal RUDAS cutoff score based on the ROC curve was ≤ 23 points. In the initial study, RUDAS was not affected by gender, years of education, differential performance factors or preferred language.1414. Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31. Rowland et al.1717. Rowland JT, Basic D, Storey JE, Conforti DA. The Rowland universal dementia assessment scale (RUDAS) and the Folstein MMSE in a multicultural cohort of elderly persons. Int Psychogeriatr. 2006;18:111-20. compared the accuracy of the RUDAS and MMSE for diagnosing dementia in a multicultural cohort of elderly people, including six groups according to language background (English-speaking, Asian non-English-speaking, and non-Asian non-English-speaking), finding that RUDAS scores below 23 suggested dementia. RUDAS is at least as accurate as the MMSE, and does not appear to be influenced by language, education or gender. Nielsen et al.1313. Nielsen TR, Vogel A, Gade A, Waldemar G. Cognitive testing in non-demented Turkish immigrants – comparison of the RUDAS and the MMSE. Scand J Psychol. 2012;53:455-60. have compared RUDAS and MMSE performance among Turkish immigrants in Denmark and have found that the level of education represented a significant variable for both the RUDAS and the MMSE performance, although the impact of education was considerably more pronounced for the MMSE.
The Thai validation of the RUDAS found an optimal cutoff score of ≤ 24, as well as that education affected the scores.1818. Limpawattana P, Tiamkao S, Sawanyawisuth K, Thinkhamrop B. Can Rowland universal dementia assessment scale (RUDAS) replace mini-mental state examination (MMSE) for dementia screening in a Thai geriatric outpatient setting? Am J Alzheimers Dis Other Demen. 2012;27:254-9. The Arabic version found a cutoff of 22 based on the ROC curves.2121. Chaaya M, Phung TK, El Asmar K, Atweh S, Ghusn H, Khoury RM, et al. Validation of the Arabic Rowland universal dementia assessment scale (A-RUDAS) in elderly with mild and moderate dementia. Aging Ment Health. 2016;20:880-7. Nielsen et al.1919. Nielsen TR, Andersen BB, Gottrup H, Lützhøft JH, Høgh P, Waldemar G. Validation of the Rowland universal dementia assessment scale for multicultural screening in Danish memory clinics. Dement Geriatr Cogn Disord. 2013;36:354-62. evaluated the diagnostic accuracy of the RUDAS in a multicultural sample of patients referred to Danish memory clinics and observed that the optimal cut-point based on the ROC curve was 24 points. Regression analyses revealed that the RUDAS was unaffected by factors related to immigrant status.
The RUDAS has proven to be less affected by education, cultural, and linguistic factors than the MMSE, making it a particularly valuable tool when screening for cognitive impairment in elderly multicultural patient populations.
This study has some limitations that should be acknowledged. The current sample included only participants in mild or moderate stages of dementia. The findings do not apply for evaluating individuals with severe dementia. In addition, the sample was selected from individuals attending an outpatient clinic. Therefore, replication of this RUDAS validation in a community-based sample will be important.
The data presented here suggest that the RUDAS-BR is as accurate as the MMSE for classifying AD. The RUDAS proved to be less affected by educational level than the MMSE. The use of the RUDAS-BR may improve the cognitive screening of older adults in different cultures, since it has demonstrated comprehensibility following direct translation into Brazilian Portuguese and was not influenced by education level.
Acknowledgements
The authors would like to thank the International Liaison Committee Research Editing and Consulting Program (RECP) and its consultant, Mary Beth Spitznagel, PhD, for the English edition. This study received financial support from Fundação de Apoio à Pesquisa do Estado do Rio de Janeiro (FAPERJ; edital n° 06/2013), Programa Pró-Idoso – Apoio ao Estudo de Temas Relacionados à Saúde e Cidadania de pessoas Idosas – 2013 (FAPERJ/ E-26/110.069/2013). JL is Researcher 2 from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Cientista do Nosso Estado from FAPERJ.
References
-
1Wimo A, Jönsson L, Bond J, Prince M, Winblad B; Alzheimer Disease International. The worldwide economic impact of dementia 2010. Alzheimers Dement. 2013;9:1-11.
-
2McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH, et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:263-9.
-
3Caamaño-Isorna F, Corral M, Montes-Martínez A, Takkouche B. Education and dementia: a meta-analytic study. Neuroepidemiology. 2006;26:226-32.
-
4Farfe JM, Nitrini R, Suemoto CK, Grinberg LT, Ferretti RE, Leite RE, et al. Very low levels of education and cognitive reserve: a clinicopathologic study. Neurology. 2013;81:650-7.
-
5EClipSE Collaborative Members, Brayne C, Ince PG, Keage HA, McKeith IG, Matthews FE, et al. Education, the brain and dementia: neuroprotection or compensation? Brain. 2010;133:2210-16.
-
6Liu Y, Julkunen V, Paajanen T, Westman E, Wahlund LO, Aitken A, et al. Education increases reserve against Alzheimer’s disease--evidence from structural MRI analysis. Neuroradiology. 2012;54:929-38.
-
7Ardila A, Bertolucci PH, Braga LW, Castro-Caldas A, Judd T, Kosmidis MH, et al. Illiteracy: the neuropsychology of cognition without reading. Arch Clin Neuropsychol. 2010;25:689-712.
-
8Pawlowski J, Remor E, Parente MADMP, Salles JF, Fonseca RP, Bandeira DR. The influence of reading and writing habits associated with education on the neuropsychological performance of Brazilian adults. Read Writ. 2012;25:2275-89.
-
9Laks J, Baptista EM, Contino AL, de Paula EO, Engelhardt E. Mini-Mental State Examination norms in a community-dwelling sample of elderly with low schooling in Brazil. Cad Saude Publica. 2007;23:315-9.
-
10Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. [The Mini-Mental State Examination in a general population: impact of educational status]. Arq Neuropsiquiatr. 1994;52:1-7.
-
11Laks J, Batista EM, Guilherme ER, Contino AL, Faria ME, Figueira I, et al. [Mini-mental state examination in community-dwelling elderly: preliminary data from Santo Antônio de Pádua, Rio de Janeiro, Brazil]. Arq NeuroPsiquiatr. 2003;61:782-5.
-
12Brucki SM, Nitrini R, Caramelli P, Bertolucci PH, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq NeuroPsiquiatr. 2003;61:777-81.
-
13Nielsen TR, Vogel A, Gade A, Waldemar G. Cognitive testing in non-demented Turkish immigrants – comparison of the RUDAS and the MMSE. Scand J Psychol. 2012;53:455-60.
-
14Storey JE, Rowland JT, Basic D, Conforti DA, Dickson HG. The Rowland universal dementia assessment scale (RUDAS): a multicultural cognitive assessment scale. Int Psychogeriatr. 2004;16:13-31.
-
15Naqvi RM, Haider S, Tomlinson G, Alibhai S. Cognitive assessments in multicultural populations using the Rowland Universal Dementia Assessment Scale: a systematic review and meta-analysis. CMAJ. 2015;187:E169-75.
-
16Iype T, Ajitha BK, Antony P, Ajeeth NB, Job S, Shaji KS. Usefulness of the Rowland universal dementia assessment scale in South India. J Neurol Neurosurg Psychiatry. 2006;77:513-4.
-
17Rowland JT, Basic D, Storey JE, Conforti DA. The Rowland universal dementia assessment scale (RUDAS) and the Folstein MMSE in a multicultural cohort of elderly persons. Int Psychogeriatr. 2006;18:111-20.
-
18Limpawattana P, Tiamkao S, Sawanyawisuth K, Thinkhamrop B. Can Rowland universal dementia assessment scale (RUDAS) replace mini-mental state examination (MMSE) for dementia screening in a Thai geriatric outpatient setting? Am J Alzheimers Dis Other Demen. 2012;27:254-9.
-
19Nielsen TR, Andersen BB, Gottrup H, Lützhøft JH, Høgh P, Waldemar G. Validation of the Rowland universal dementia assessment scale for multicultural screening in Danish memory clinics. Dement Geriatr Cogn Disord. 2013;36:354-62.
-
20Shaaban J, Aziz AA, Abdullah Z, Ab Razak A. Validation of the Malay version of Rowland universal dementia assessment scale (MRUDAS) among elderly attending primary care clinic. Int Med J. 2013;20:555-8.
-
21Chaaya M, Phung TK, El Asmar K, Atweh S, Ghusn H, Khoury RM, et al. Validation of the Arabic Rowland universal dementia assessment scale (A-RUDAS) in elderly with mild and moderate dementia. Aging Ment Health. 2016;20:880-7.
-
22American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). Arlington: American Psychiatric Publishing; 1994.
-
23Chaves ML, Camozzato AL, Godinho C, Kochhann R, Schuh A, de Almeida VL, et al. Validity of the clinical dementia rating scale for the detection and staging of dementia in Brazilian patients. Alzheimer Dis Assoc Disord. 2007;21:210-7.
-
24Almeida OP, Almeida SA. [Reliability of the Brazilian version of the ++abbreviated form of Geriatric Depression Scale (GDS) short form]. Arq Neuropsiquiatr. 1999;57:421-6.
-
25Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982-1983;17:37-49.
-
26Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-98.
-
27NSW Health Department, Department of Ageing, Disability and Home Care. RUDAS: Rowland Universal Dementia Assessment Scale: a multicultural cognitive assessment scale. Administration and scoring guide. 2001 [cited 2017 Mar 24]. https://www.fightdementia.org.au/sites/default/files/20110311_2011RUDASAdminScoringGuide.pdf
» https://www.fightdementia.org.au/sites/default/files/20110311_2011RUDASAdminScoringGuide.pdf -
28Caramelli P, Herrera E Jr, Nitrini R. O mini-exame do estado mental no diagnóstico de demência em idosos analfabetos. Arq Neuropsiquiatr. 1999;57:7-12.
-
29Basic D, Rowland JT, Conforti DA, Vrantsidis F, Hill K, LoGiudice D, et al. The validity of the Rowland universal dementia assessment scale (RUDAS) in a multicultural cohort of community-dwelling older persons with early dementia. Alzheimer Dis Assoc Disord. 2009;23:124-9.
Publication Dates
-
Publication in this collection
15 Feb 2018 -
Date of issue
Jul-Sep 2018
History
-
Received
24 Mar 2017 -
Accepted
16 June 2017