Recent studies have shown that self-injurious episodes in autism are due to catatonic symptoms.11. Sajith SG, Liew SF, Tor PC. Response to electroconvulsive therapy in patients with autism spectrum disorder and intractable challenging behaviors associated with symptoms of catatonia. J ECT. 2017;33:63-7.
2. Wachtel LE, Dhossche DM. Self-injury in autism as an alternate sign of catatonia: implications for electroconvulsive therapy. Med Hypotheses. 2010;75:111-4.-33. Wachtel LE, Shorter E, Fink M. Electroconvulsive therapy for self-injurious behaviour in autism spectrum disorders: recognizing catatonia is key. Curr Opin Psychiatry. 2018;31:116-22. It has been theorized that these symptoms are caused by dysfunction of GABAergic receptors.22. Wachtel LE, Dhossche DM. Self-injury in autism as an alternate sign of catatonia: implications for electroconvulsive therapy. Med Hypotheses. 2010;75:111-4. This report describes a case in which electroconvulsive therapy (ECT) was used successfully to treat self-injury in a patient with severe autism and highlights the viability of ECT as a therapeutic option for this population.
A 17-year-old male diagnosed with severe autism spectrum disorder (ASD) – with no language development and incapable of basic self-care and social interaction – was admitted to the psychiatry ward of Hospital das Clínicas, Universidade Estadual de Campinas (UNICAMP), in January 2018 due to extreme aggression and self-injurious behavior.
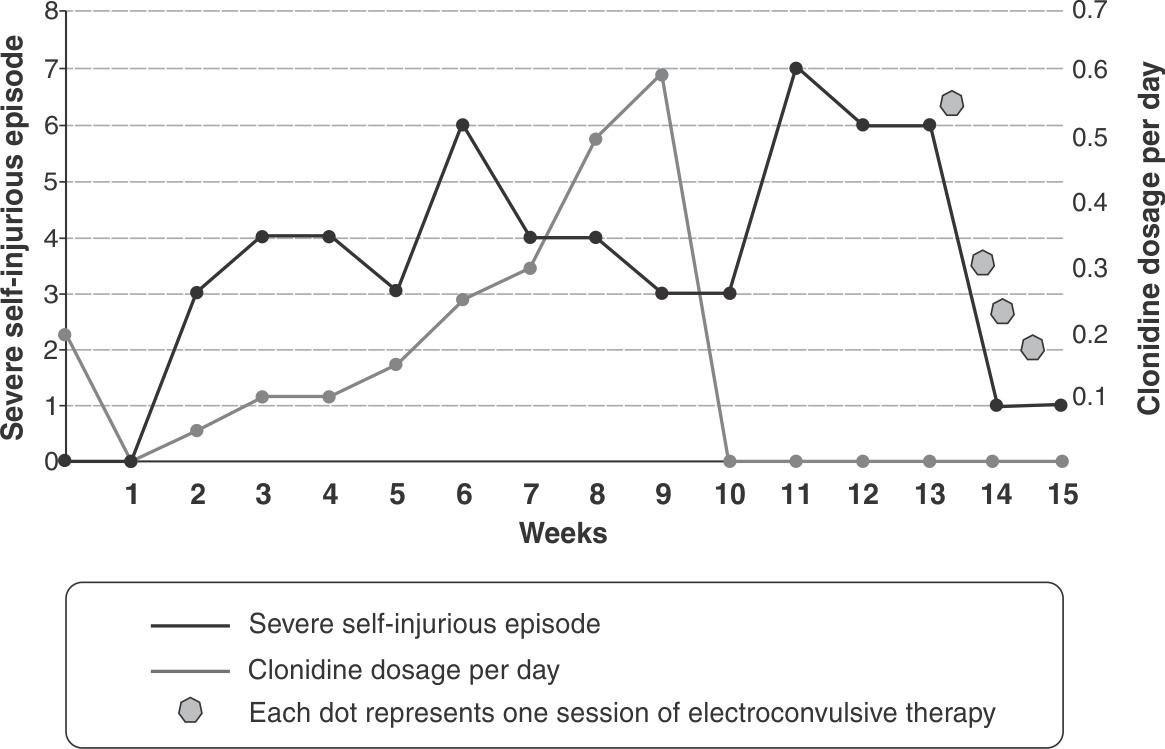
Several drug regimens had been trialed to control his symptoms; at the time of admission, his treatment included clozapine, haloperidol, and levomepromazine. The patient responded best to clonidine, with partial control of symptoms and decreased severity of self-injurious episodes. However, in late March 2018, a clonidine shortage led to sudden discontinuation of treatment, and his episodes once again became more frequent and more severe (Figure 1).
Relationship between severe self-injurious behavior, clonidine withdrawal, and electroconvulsive therapy sessions during hospitalization.
ECT was prescribed, and four sessions were done in late April. The patient started to show improvement after the first session; after the second, he was able to help the staff fold bed linens and walk around the hospital’s common area unaided without any inappropriate behavior. In the course of 2 weeks between the first ECT session and his hospital discharge, he had only two episodes of self-injurious behavior: one immediately after the first session, with no evident reason, and the second one during a visit from his mother, as soon as he realized she was about to leave. After his discharge, the patient continued to show improvement.
As in the case described herein, the first line of treatment for self-injurious symptoms of catatonia is behavioral therapy and pharmacotherapy44. Mahatmya D, Zobel A, Valdovinos MG. Treatment approaches for self-injurious behavior in individuals with autism: behavioral and pharmacological methods. J Early Intensive Behav Interv. 2008;5:106-18.; common agents include clozapine55. Teixeira E. Clozapina no tratamento da agressividade patológica grave em crianças e adolescentes com transtorno de conduta ou com autismo [dissertation]. Campinas: Universidade Estadual de Campinas; 2012. and risperidone.44. Mahatmya D, Zobel A, Valdovinos MG. Treatment approaches for self-injurious behavior in individuals with autism: behavioral and pharmacological methods. J Early Intensive Behav Interv. 2008;5:106-18. Both are supported by studies, but some patients may respond poorly, thus suggesting the need for alternative treatments.
The effects of ECT on the brain are still unclear. Hypotheses include increased GABAergic function, decreased function of dopaminergic and serotoninergic receptors as a secondary effect, normalization of the hypothalamic-pituitary-adrenal axis, and release of other, previously inhibited neuromodulators.22. Wachtel LE, Dhossche DM. Self-injury in autism as an alternate sign of catatonia: implications for electroconvulsive therapy. Med Hypotheses. 2010;75:111-4.,33. Wachtel LE, Shorter E, Fink M. Electroconvulsive therapy for self-injurious behaviour in autism spectrum disorders: recognizing catatonia is key. Curr Opin Psychiatry. 2018;31:116-22.
More studies are needed to provide additional data on the utility of ECT to treat self-injurious behavior in patients with severe ASD and provide criteria for the use of ECT for this purpose. It is important that behavioral therapies and pharmacological intervention be prioritized in such cases, given the large body of evidence proving their efficacy. Nevertheless, ECT shows promising results for patients refractory to behavioral and pharmacological treatment, and may become a first-line therapy in the near future.
References
-
1Sajith SG, Liew SF, Tor PC. Response to electroconvulsive therapy in patients with autism spectrum disorder and intractable challenging behaviors associated with symptoms of catatonia. J ECT. 2017;33:63-7.
-
2Wachtel LE, Dhossche DM. Self-injury in autism as an alternate sign of catatonia: implications for electroconvulsive therapy. Med Hypotheses. 2010;75:111-4.
-
3Wachtel LE, Shorter E, Fink M. Electroconvulsive therapy for self-injurious behaviour in autism spectrum disorders: recognizing catatonia is key. Curr Opin Psychiatry. 2018;31:116-22.
-
4Mahatmya D, Zobel A, Valdovinos MG. Treatment approaches for self-injurious behavior in individuals with autism: behavioral and pharmacological methods. J Early Intensive Behav Interv. 2008;5:106-18.
-
5Teixeira E. Clozapina no tratamento da agressividade patológica grave em crianças e adolescentes com transtorno de conduta ou com autismo [dissertation]. Campinas: Universidade Estadual de Campinas; 2012.
Publication Dates
-
Publication in this collection
17 Oct 2019 -
Date of issue
Sep-Oct 2019
History
-
Received
1 May 2019 -
Accepted
1 July 2019