Abstracts
PURPOSE: To verify how the impact of dysphonia in teachers is characterized according to the protocols V-RQOL (Voice-Related Quality of Life), VHI (Voice Handicap Index) and VAPP (Voice Activity and Participation Profile), and to analyze the correspondence of information obtained by these instruments. METHODS: Fourty six teachers with voice complaints that sought for speech-language pathology intervention and were diagnosed with behavioral dysphonia answered randomly the V-RQOL, VHI and VAPP questionnaires. RESULTS: Dysphonic teachers presented worse quality of life than the general dysphonic population on the V-RQOL. The VHI showed no significant handicap. On the VAPP, teachers had lower scores in the effects in social communication. The physical (VHI) and physical functioning (V-RQOL) domains were similar to each other. The VAPP provides information about aspects not contemplated by the other protocols; self-perception of the severity of dysphonia was correlated with all domains of the three protocols. The items with greatest impact on the V-RQOL were from the physical functioning domain, and, on the VHI, from the physical domain. On the VAPP, the two questions with greater occurrence were related to the effect of voice over emotion. Hence, for this population, it is suggested the use of the VAPP questionnaire, because it comprises aspects that the others don't; in addition, the V-RQOL should also be used, because it has fewer questions and more impact (total and emotional scores) than the VHI. CONCLUSION: The protocols do not show the same information for dysphonic teachers. The physical functioning (V-RQOL) and physical (VHI) domains provide similar results, however social-emotional domain of the V-RQOL exhibited more evidently the impact of the voice disorder in dysphonic teachers than the VHI. The VAPP present information not contemplated by the other protocols.
Voice; Quality of life; Dysphonia; Protocols; Faculty; Questionnaires
OBJETIVO: Verificar como o impacto da disfonia em professores é caracterizado pelos protocolos QVV (Qualidade de Vida em Voz), IDV (Índice de Desvantagem Vocal) e PPAV (Perfil de Participação e Atividades Vocais), e analisar a correspondência das informações obtidas por esses instrumentos. MÉTODOS: Quarenta e seis professores com queixa vocal que procuraram atendimento fonoaudiológico e foram diagnosticados com disfonia de base comportamental responderam aos questionários QVV, IDV e PPAV, em ordem aleatória. RESULTADOS: Professores disfônicos apresentaram pior qualidade de vida no QVV em relação à população de disfônicos. O IDV não apresentou devantagem vocal expressiva. No PPAV, os professores disfônicos apresentaram menor escore em efeitos na comunicação social. Os domínios orgânico (IDV) e físico (QVV) foram considerados iguais. O PPAV apresenta aspectos não contemplados nos demais protocolos; a auto-percepção do grau da disfonia apresentou correlação com todos os domínios dos três protocolos. No QVV, as questões com maior impacto pertencem ao físico e no IDV, ao orgânico. Já no PPAV, as duas questões de maior ocorrência relacionam-se ao efeito da voz na emoção. Assim, para esta população, sugere-se a aplicação do PPAV, por contemplar aspectos não contemplados nos demais, e do QVV, pelo reduzido número de questões e por apresentar maior impacto (escores total, emocional) em relação ao IDV. CONCLUSÃO: QVV, IDV e PPAV não apresentam as mesmas informações em professores disfônicos. Os domínios físico (QVV) e orgânico (IDV) oferecem resultados semelhantes, contudo, o sócio-emocional do QVV evidenciou mais o impacto da alteração vocal em professores disfônicos que o IDV. O PPAV apresenta informações não contempladas nos demais protocolos.
Voz; Qualidade de vida; Disfonia; Protocolos; Docentes; Questionários
ORIGINAL ARTICLE
IGraduate Program (Lato sensu) in Voice, Centro de Estudos da Voz - CEV - São Paulo (SP), Brasil
IIGraduate Program (Masters degree) in Human Communication Disorders, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brasil
IIICentro de Estudos da Voz - CEV - São Paulo (SP), Brasil; Graduate Program in Human Communication Disorders of the Department of Speech-Language Pathology and Audiology, São Paulo Federal University - Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil.
Correspondence address
ABSTRACT
PURPOSE: To verify how the impact of dysphonia in teachers is characterized according to the protocols V-RQOL (Voice-Related Quality of Life), VHI (Voice Handicap Index) and VAPP (Voice Activity and Participation Profile), and to analyze the correspondence of information obtained by these instruments.
METHODS: Fourty six teachers with voice complaints that sought for speech-language pathology intervention and were diagnosed with behavioral dysphonia answered randomly the V-RQOL, VHI and VAPP questionnaires.
RESULTS: Dysphonic teachers presented worse quality of life than the general dysphonic population on the V-RQOL. The VHI showed no significant handicap. On the VAPP, teachers had lower scores in the effects in social communication. The physical (VHI) and physical functioning (V-RQOL) domains were similar to each other. The VAPP provides information about aspects not contemplated by the other protocols; self-perception of the severity of dysphonia was correlated with all domains of the three protocols. The items with greatest impact on the V-RQOL were from the physical functioning domain, and, on the VHI, from the physical domain. On the VAPP, the two questions with greater occurrence were related to the effect of voice over emotion. Hence, for this population, it is suggested the use of the VAPP questionnaire, because it comprises aspects that the others don't; in addition, the V-RQOL should also be used, because it has fewer questions and more impact (total and emotional scores) than the VHI.
CONCLUSION: The protocols do not show the same information for dysphonic teachers. The physical functioning (V-RQOL) and physical (VHI) domains provide similar results, however social-emotional domain of the V-RQOL exhibited more evidently the impact of the voice disorder in dysphonic teachers than the VHI. The VAPP present information not contemplated by the other protocols.
Keywords: Voice; Quality of life; Dysphonia; Protocols; Faculty; Questionnaires
INTRODUCTION
The opinion of the patient about his/her well-being should always be taken into consideration when trying to comprehend the real impact of a disease. Instruments that assess quality of life allow the measurement of the individual's perception about effect of an illness on their personal, social and professional relations(1,2).
The perceptual and acoustic analysis surely play an essential role in the voice evaluation, however they are not sufficient to acquire the functional, social and emotional consequences of a vocal deviation(3). The impact of a voice deviation on the quality of life of an individual presents a complex relationship that is not necessarily direct to the degree of voice deviation, because it depends on several factors, including the professional use(4).
The assessment of quality of life as a method of treatment outcome evaluation for patients with voice deviation has grew bigger in the clinical settings(5). Self-assessment instruments have been utilized for either differentiating or groups patients, for estimating individual results, for evaluating the efficacy of treatment, as well as for helping the clinician to prioritize problems during the intervention process(6,7).
Several quality of life questionnaires were developed to assess the impact of specific illnesses. Among these questionnaires there are some that are related to voice, some of which have already been validated to Brazilian Portuguese, such as the Voice-Related Quality of Life - VRQOL(8,9) (Appendix 1); Voice Handicap Index - VHI(10,11), (Appendix 2) and Voice Activity and Participation Profile - VAPP(12,13), (Appendix 3). These three tools have had their validity, reliability and responsiveness demonstrated and can be used for evaluating individuals with vocal problems(14). However, none of them are profession-specific but condition-specific.
Teacher's voice has been one of the Speech-language Pathology focuses, especially because of the evidences that among the professional voice users they are probably the ones that present with the highest prevalence of vocal disorders due to the intense voice use under unfavorable work conditions. A recent historical review summarized the Speech-language Pathology contribution and pointed out the need of intervention studies(15).
Recently, a national epidemiological revision was carried out and indicated that teachers have higher occurrence of vocal symptoms when compared to the general population; great part of the teachers reported having voice problems at some point in their lives(16).
Therefore, it is important to map the impact of a dysphonia in the lives of these professionals in order to understand better the patient's perspective about his/her voice problem. Since there is not a specific self-assessment questionnaire for teachers, it is important to comprehend the information provided by the three instruments validated to the Brazilian Portuguese (V-RQOL, VHI and VAPP), to analyze whether they are interchangeable, whether there is one of them that characterizes better the effect of a voice disorder on this population, and in addition to check the relationship among them.
The purpose of the present study is to check how the impact of a dysphonia on teachers' lives is characterized by the V-RQOL, VHI and VAPP and to analyze the relationship among the information they provide.
METHODS
The project of this research was approved by the Ethics Committee of Centro de Estudos da Voz (CEV) under the 0214/06 protocol number. All the participants signed the Consent Form. Data collection took place from July 10th 2007 to June 16th 2008
The population consisted of 46 teachers (38 female, eight male) with a mean age of 34 years (20-65 years), both from public and private schools that sought for help due to voice problem in a private institution in Sao Paulo City (SINPRO-SP). The inclusion criteria were: presenting with voice complaint, otolaryngological diagnosis of behavioral based dysphonia (glottic chink and/or benign mass lesion) and indication for voice treatment; no previous voice therapy or at the most two therapy sessions.
All the participants read and answered the three questionnaires that were randomly presented to them at the same evaluation session without any help from the clinician.
The V-RQOL has ten items, of which six evaluate the physical functioning (PF) domain and four the social-emotional (SE) domain (Appendix 1). The items are answered on a five-point scale, where 1 means "it is not a problem" and 5 means "it is a big problem". The calculation of the score is obtained by means of an algorithm and it can vary from 0 to 100, with the latter indicating the best quality of life possible(8,9).
The VHI has 30 items that encompasses three domains: functional (F), physical (P) and emotional (E). Scores are calculated by simply adding up the gross values and can vary from 0 to 120; the higher the score, the greater is the voice handicap (Appendix 2). The items are answered on a five-point scale, where 0 means "never" and 4 means "always". Each domain can score from 0 to 40, with the latter indicating the greatest handicap(10,11).
The VAPP has 28 items that are distributed into five aspects: self-perception of the severity of the voice problem, effect on job, effect on daily communication, effect on social communication, and expression of emotions (Appendix 3). The instrument is answer on a ten-centimeter visual analogue scale with its ends varying from "normal" to "severe" for the first aspect and "never" to "always" for the others. Maximum score for each item is 10 and maximum total score is 280, which reflects the greatest negative impact(12,13).
All three questionnaires scores were calculated and pondered on 100 bases in order to make comparison possible. The statistical treatment performed was: Spearman correlation, Wilcoxon and Friedman tests. The significance level adopted was 5% (p=0.050). In addition, the following analyses were performed: mean and standard deviation of the partial and total scores; comparison among each and all domains and aspects of the three protocols; comparison of the self-perception of the severity of the voice problem with each of the domains and aspects of the three questionnaires; and finally analysis of the three most deviated items for each of the questionnaires, and for this analysis the guideline adopted was: gross score of 4 or 5 for the V-RQOL, gross score of 3 or 4 for the VHI and gross score of 6 or higher for the VAPP.
RESULTS
The results obtained by means of the V-RQOL, VHI and VAPP are presented at Tables 1 to 4.
Table 1 shows all the scores of the three questionnaires. The V-RQOL produced mean total score of 64.5, social-emotional of 75.5 and physical functioning of 56.8. The VHI produced the following mean scores: total 38.4, functional 9.4, emotional 8.2 and physical 21.6. The mean scores for the VAPP were: total 87.8, self-perception of the severity of the voice problem 4.9, effects on job 13.8, effects on daily communication 37.7, effects on social communication 7.3 and effects on expression of emotion 24.3.
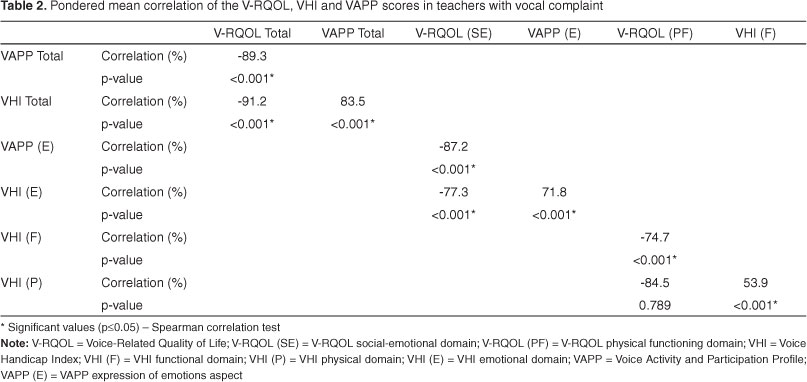
When the questionnaires are compared (Table 2), it can be observed that the total scores are different (p<0,001). The social-emotional V-RQOL domain, the VHI emotional domain and the effects on expression of emotion VAPP aspect were also different, emphasizing the fact that the instruments are complementary and irreplaceable. The V-RQOL physical functioning and the VHI functional domains as well as the VHI physical and functional domains were different too (p<0.001). On the other hand, the V-RQOL physical functioning and the VHI physical domains did not present with statistically different results (p=0.789). However, the V-RQOL physical functioning domain displayed higher scores that the VHI physical domain.
Table 3 shows the most deviate items of the three questionnaires. For the V-RQOL, these items belong to the physical functioning domain and for the VHI to the physical. However, for the VAPP, the two most deviated items belong to the effects on expression of emotion (45.7% and 26.1% respectively), followed by three items that had the same percentage of occurrence (21.7%) and they were related to the effects on job, on daily communication and again on expression of emotion.
Table 4 shows the comparison between the self-perception of the severity of the voice problem with each of the three questionnaire domains and aspects. All correlation were significant highlighting that the worse the vocal self-perception, the worse all and each scores of the questionnaires.
DISCUSSION
The use of quality of life questionnaires for dysphonic patients is important for the voice clinic since the impact that a voice deviation has on the life of an individual does not necessarily has a direct relationship with the degree of the dysphonia(4).
The higher number of women in the sample of this study reflects the gender profile of the population of teacher as well as the higher incidence of voice deviation in this population(17,18).
Studies from the literature show the following V-RQOL scores for dysphonic individuals: total - 71.6, emotional - 79.5 and physical functioning 74.9(8,14). By looking at our data, we observe that the teachers' scores were lower than the one for the dysphonic population; however, the social-emotional scores were similar. Teachers have worse quality of life, as far as the total and physical functioning scores are concerned, when compared to the dysphonic population. This result may be explained by the questions in this domain that reflect the main difficulties faced by the teachers, i.e. "I run out of air and need to take frequent breaths when talking", "I have trouble speaking loudly or being heard in noisy situations", "I have trouble doing my job or practicing my profession (because of my voice)", because they are professionals that have a high vocal demand and not always favorable work conditions(19).
Regarding the VHI, the dysphonic patients presented with the following mean scores: total 47.4, functional 12.6, emotional 13.1 and physical 21.7(11,14). The teachers from this study had lower total, emotional and functional scores (Table 1) when compared to the dysphonic population, except for the physical domain that showed similar scores for both population. Therefore, it can be implied that the VHI did not show clearly an expressive handicap for teachers with voice problems. On the other hand, the V-RQOL had opposite response, which reinforces the hypothesis that the questionnaires are not interchangeable.
In a study performed with dysphonic individuals, the mean VAPP scores were: total 98.8, self-perceived severity of the voice problem 5.5, effect on job 13.3, effect on daily communication 43.1, effect on social communication 12.7 and effect on expression of emotion 24.2(13,14). The data from the present study was shown to match the findings from the literature. The only aspect that presented with different values for both populations was the effect on social communication, indicating that dysphonic teachers perceive lessen social impact. A study carried out with 97 teachers of municipal schools of Bauru City showed that the total scores of individuals that reported vocal complaint were lower than the ones found in this study(20). Only the effect on social communication aspect presented analogous results. The similarity of findings in that aspect for the teacher population of both studies and the opposition for the dysphonic population(14) can be explained by the fact that teachers tend to be more communicative and extrovert due to the professional demand and so it is quite expected that they would not perceive a great social impact even with the presence of a vocal deviation.
Even though the three questionnaires analyze the reported impact of a voice problem, each of them has their own particularities making them complementary and not totally interchangeable(5,21). The V-RQOL physical functioning domain and the VHI physical domain demonstrated significant association, suggesting that their results are correspondent (Table 2). However, the V-RQOL scores were higher than the VHI for this domain, maybe that was due to the fact that the items from the V-RQOL, i.e. "I have trouble speaking loudly or being heard in noisy situations" and "I have trouble doing my job or practicing my profession (because of my voice)" express better the difficulties that teachers have when compared to the items of the VHI physical domain, i.e. "People ask, "What's wrong with your voice?", "The clarity of my voice is unpredictable" and "I try to change my voice to sound different".
Regarding the emotional impact of a dysphonia (Table 2), the social-emotional domain of the V-RQOL displayed higher values whereas the VHI emotional domain displayed lower values, emphasizing once more the fact that the instruments are not replaceable. A possible aspect that influenced this result is that the V-RQOL has items with a more social nature, such as "I avoid going out socially (because of my voice)" and "I have become less outgoing (because of my voice)". On the other hand, the three questionnaires have similar questions regarding the feeling that may be caused by a voice problem: depression, anxiety or frustration (V-RQOL), tense, upset, annoyed, embarrassed (VHI) and upset, embarrassed, low-esteem, worried and dissatisfied (VAPP). The VAPP exhibited the higher scores than the VHI that we think it is because of the similarity among some questions in the VHI, i.e. "I feel annoyed when people ask me to repeat" and "I feel embarrassed when people ask me to repeat"; "My voice makes me feel incompetent" and "My voice makes me feel handicapped".
For the V-RQOL, the items with the highest occurrence belong to the physical functioning domain and are related to the respiratory coordination, voice loudness and work (Table 3). For the VHI, these questions belonged to the physical domain that relates to the vocal quality and effort to phonate. For the VAPP, the first two items with the highest occurrence were from the effect on expression of emotion aspect, followed by three questions with the same occurrence and they were related to effect on job, emotion and daily communication: "Are you worried about your voice problem?", "Do you feel dissatisfied because of your voice problem?", "In the last six months, has your voice problem affected your decisions for your future career?", "Do you feel upset about your voice problem?" and "Does your voice problem affect your communication in noisy environments?". Such items may reflect the emotional impact of the dysphonia, the concern with their job and difficulty with voice projection. Perhaps, these results came out because the VAPP does not have a functional domain, and therefore have items that the other instruments do not have, such as the effect on job and on daily communication. It is important to highlight that certain items are alike: "I have trouble speaking loudly or being heard in noisy situations" from V-RQOL, and "Does your voice problem affect your communication in noisy environments?", both questions are related to the need of speaking loud in noisy environments that sometimes may be unfavorable working conditions that these professionals face(15); another example is "I run out of air and need to take frequent breaths when talking" from the V-RQOL and "I feel as though I have to strain to produce voice" and "I use a great deal of effort to speak" from the VHI that indicate a difficulty in balancing the respiratory and phonatory systems, which can be physiologically addressed during the rehabilitation process, with for instance the Vocal Function Exercises - VFE(22). The VHI has two items that demonstrate the variability of the vocal quality throughout the day that is not investigated by the other questionnaires: "The sound of my voice varies throughout the day" and "My voice is worse in the evening". Questions related to expression of emotion and with changing job in the future also had high occurrence: "I have trouble doing my job or practicing my profession (because of my voice)" from the V-RQOL and "Are you worried about your voice problem?", "Do you feel upset about your voice problem?" and "In the last 6 months, has your voice problem affected your decisions for your future career?" from VAPP. These findings were also confirmed by other studies carried out with teachers(16,17).
The results showed that the worse the self-perceived severity of the voice problem, the worse were all the scores for the three questionnaires (Table 4). It is worth mentioning that the V-RQOL scores are negative due to the value inversion, since the higher scores indicate better quality of life, whereas is the opposite for the VHI and the VAPP.
When comparing the V-RQOL and the VHI, the V-RQOL would be more suitable for assessing dysphonic teachers, given that it not only is the shorter and less time demanding tool, but it also displayed the highest total and social-emotional scores. Moreover, the VHI physical domain was considered equal to the V-RQOL physical functioning domain. When dysphonic teachers are compared to the general population, they present worse quality of life exhibited by the total and physical functioning domain of the V-RQOL, whereas the VHI provided similar results for both population.
The VAPP contemplate aspects that the other two questionnaires do not and are important for professional voice users, since it assess the emotional impact as well as the effect on job, daily and social communication and the perceived severity of the voice problem. Therefore, we can suggest the administration of both the VAPP and the V-RQOL, the first for being comprehensive and investigate aspects that the others do not, and the latter for having the physical functioning domain that the VAPP does not have.
Last of all, it is important to consider the profile of the population that is going to be addressed. Studies with diverse populations and different type of dysphonias contribute to mapping the behavior of the instruments for the groups studied.
CONCLUSION
The three questionnaires used for this research do not provide the same information and showed to be complementary. The V-RQOL physical functioning domain and the VHI physical domain provide similar results, while the V-RQOL emotional domain exhibited more evidently the impact of a vocal deviation in dysphonic teachers. The VAPP supply information that the others don't contemplate. Therefore, the selection of the instrument should consider the specificity of the purpose.
REFERENCES
- 1. Benninger MS, Sataloff RT. The evaluation of outcomes and quality of life in individuals with voice disorders. J Singing. 1999;56(2):39-43.
- 2. World Health Organization. WHOQOL Measuring quality of life [Internet]. 1997 [cited 2011 Jun 14]. [place unknown]: WHO; 1997. (Programme on Mental Health). Available from: http://www.who.int/mental_health/media/68.pdf
- 3. Hogikyan ND, Wodchis WP, Spak C, Kileny PR. Longitudinal effects of botulinum toxin injections on voice-related quality of life (V-RQOL) for patients with adductory spasmodic dysphonia. J Voice. 2001;15(4):576-86.
- 4. Behlau M, Hogikyan ND, Gasparini G. Quality of life and voice: study of a Brazilian population using the voice-related quality of life measure. Folia Phoniatr Logop. 2007;59(6):286-96.
- 5. Portone CR, Hapner ER, McGregor L, Otto K, Johns MM 3rd. Correlation of the Voice Handicap Index (VHI) and the Voice-Related Quality of Life Measure (V-RQOL). J Voice. 2007;21(6):723-7.
- 6. Berlim MT, Fleck MP. "Quality of life": a brand new concept for research and practice in psychiatry. Rev Bras Psiquiatr. 2003;25(4):249-52.
- 7. Higginson IJ, Carr AJ. Measuring quality of life: Using quality of life measures in the clinical setting. BMJ. 2001;322(7297):1297-300.
- 8. Hogikyan ND, Sethuraman G. Validation of an instrument to measure voice-related quality of life (V-RQOL). J Voice. 1999;13(4):557-69.
- 9. Gasparini G, Behlau M. Quality of life: validation of the Brazilian version of the voice-related quality of life (V-RQOL) measure. J Voice. 2009;23(1):76-81.
- 10. Jacobson BH, Johson A, Grywalski C, Silbergleit AK, Jacobson GP, Benninger M, Newman CW. The Voice Handicap Index (VHI): development and validation. Am J Speech Lang Pathol 1997;6:66-70.
- 11. Santos LM, Gasparini G, Behlau M. Validação do protocolo do Índice de Desvantagem Vocal (IDV) no Brasil [monografia]. São Paulo: Centro de Estudos da Voz; 2007.
- 12. Ma EP, Yiu EM. Voice activity and participation profile: assessing the impact of voice disorders on daily activities. J Speech Lang Hear Res. 2001;44(3):511-24.
- 13. Oliveira AAR, Gasparini G, Behlau M. Validação do protocolo perfil de participação e atividades vocais (PPAV) no Brasil [monografia]. São Paulo: Centro de Estudos da Voz; 2006.
- 14. Behlau M, Oliveira G, Santos LA, Ricarte A. Validação no Brasil de protocolos de auto-avaliação do impacto de uma disfonia. Pró-Fono. 2009;21(4):326-32.
- 15. de Medeiros AM, Barreto SM, Assunção AA. Voice disorders (dysphonia) in public school female teachers working in Belo Horizonte: prevalence and associated factors. J Voice. 2008;22(6):676-87.
- 16. Behlau M, Zambon F, Guerrieri AC, Roy N, GVP. Panorama epidemiológico sobre a voz do professor no Brasil [Internet]. In: 17º Congresso Brasileiro de Fonoaudiologia e 1º Congresso Ibero-Americano de Fonoaudiologia; 2009 Out 21-24; Salvador. Disponível em: http://www.sbfa.org.br/portal/anais2009/resumos/R1511-1.pdf
- 17. Roy N, Merrill RM, Thibeault S, Gray SD, Smith EM. Voice disorders in teachers and the general population: effects on work performance, attendance, and future career choices. J Speech Lang Hear Res. 2004;47(3):542-51.
- 18. Coyle SM, Weinrich BD, Stemple JC. Shifts in relative prevalence of laryngeal pathology in a treatment-seeking population. J Voice. 2001;15(3):424-40.
- 19. Duffy OM, Hazlett DE. The impact of preventive voice care programs for training teachers: a longitudinal study. J Voice. 2004;18(1):63-70.
- 20. Martinello JG. Avaliações psicométricas de qualidade de vida e voz em professores da rede municipal de Bauru [dissertação]. São Paulo: Universidade de São Paulo, Faculdade de Odontologia de Bauru; 2009.
- 21. Franic DM, Bramlett RE, Bothe AC. Psychometric evaluation of disease specific quality of life instruments in voice disorders. J Voice. 2005;19(2):300-15.
- 22. Roy N, Gray SD, Simon M, Dove H, Corbin-Lewis K, Stemple JC. An evaluation of the effects of two treatment approaches for teachers with voice disorders: a prospective randomized clinical trial. J Speech Lang Hear Res. 2001;44(2):286-96.
Comparison of V-RQOL, VHI and VAPP scores in teachers

Publication Dates
-
Publication in this collection
28 Oct 2011 -
Date of issue
Sept 2011
History
-
Accepted
12 Aug 2010 -
Received
19 May 2010