Abstracts
PURPOSE: To investigate if children with phonological disorder present different acoustic characteristics of voiceless and voiced plosives from children with typical phonological development. METHODS: Participants were 11 children with typical phonological development and five children with phonological disorder and difficulty to establish the distinctive feature [+voice] of plosives. Through words (['papa], ['baba], ['tata], ['dada], ['kaka] and ['gaga]) inserted into carrier phrases, we measured voice onset time, vowel length, burst amplitude, and occlusion length of each plosive. The acoustic parameters of voiceless and voiced plosives were compared between and within groups through statistical analysis. RESULTS: The subjects within typical phonological development presented significant results mainly in distinguishing the parameters voice onset time, vowel length, and occlusion of voiceless and voiced stops, which was different from what was observed for children with phonological disorder. The comparison between groups showed differences related to the production of voice onset time and the occlusion length of voiced plosives. Regarding the other analyzed parameters, the values were similar between groups, with no statistical differences. CONCLUSION: The marking of the voicing contrast of the group with phonological disorder is different from the group with typical phonological development, especially regarding the voice onset time and the occlusion length of the voiced segments.
Speech acoustics; Child; Speech disorders; Sound spectrography; Speech; Child language
OBJETIVO: Investigar se as crianças com desvio fonológico apresentam características acústicas distintas de sons plosivos surdos e sonoros das crianças com desenvolvimento fonológico típico. MÉTODOS:Participaram do estudo 11 crianças com desenvolvimento fonológico típico e cinco com desvio fonológico e dificuldade na aquisição do traço [+voz] das consoantes plosivas. Por meio de palavras (['papa], ['baba], ['tata], ['dada], ['kaka] e ['gaga]) inseridas em frases-veículo, mediu-se o voice onset time, a duração da vogal, a amplitude do burst e a duração da oclusão de cada plosivo. Foram comparados todos os registros acústicos de plosivos surdos e sonoros intra e intergrupo, por meio de testes estatísticos. RESULTADOS: As crianças com desenvolvimento fonológico típico apresentaram resultados significativos, principalmente, na diferenciação dos parâmetros de voice onset time, duração da vogal e oclusão de plosivos surdos e sonoros, diferentemente do observado para as crianças com desvio fonológico. A comparação entre os dois grupos mostrou diferenças quanto à produção de voice onset time e duração da oclusão dos plosivos sonoros. Com relação aos demais parâmetros analisados, os valores foram aproximados entre os grupos, sem diferença estatística. CONCLUSÃO: A marcação do contraste de sonoridade do grupo desviante mostra-se distinta em relação ao grupo de crianças com desenvolvimento fonológico típico, principalmente no que se refere ao voice onset time e à duração da oclusão dos segmentos sonoros.
Acústica da fala; Criança; Distúrbios da fala; Espectrografia do som; Fala; Linguagem infantil
ORIGINAL ARTICLE
Acoustic parameters of the voicing contrast of plosives in typical phonological development and phonological disorder
Roberta Michelon MeloI; Helena Bolli MotaII; Carolina Lisbôa MezzomoII; Brunah de Castro BrasilI; Liane LovattoIII; Leonardo ArzenoIV
IGraduate Program (Masters degree) in Human Communication Disorders, Universidade Federal de Santa Maria UFSM Santa Maria (RS), Brazil
IIUndergraduate Program in Speech-Language Pathology and Audiology, and Graduate Program in Human Communication Disorders, Universidade Federal de Santa Maria UFSM Santa Maria (RS), Brazil
IIIGraduate Program (Doctorate degree) in Phonetics, Université de Paris III Paris, France
IVGraduate Program (Masters degree) in Civil Engineering, Universidade Federal de Santa Maria UFSM Santa Maria (RS), Brazil
Correspondence address
ABSTRACT
PURPOSE: To investigate if children with phonological disorder present different acoustic characteristics of voiceless and voiced plosives from children with typical phonological development.
METHODS: Participants were 11 children with typical phonological development and five children with phonological disorder and difficulty to establish the distinctive feature [+voice] of plosives. Through words (['papa], ['baba], ['tata], ['dada], ['kaka] and ['gaga]) inserted into carrier phrases, we measured voice onset time, vowel length, burst amplitude, and occlusion length of each plosive. The acoustic parameters of voiceless and voiced plosives were compared between and within groups through statistical analysis.
RESULTS: The subjects within typical phonological development presented significant results mainly in distinguishing the parameters voice onset time, vowel length, and occlusion of voiceless and voiced stops, which was different from what was observed for children with phonological disorder. The comparison between groups showed differences related to the production of voice onset time and the occlusion length of voiced plosives. Regarding the other analyzed parameters, the values were similar between groups, with no statistical differences.
CONCLUSION: The marking of the voicing contrast of the group with phonological disorder is different from the group with typical phonological development, especially regarding the voice onset time and the occlusion length of the voiced segments.
Keywords: Speech acoustics; Child; Speech disorders; Sound spectrography; Speech; Child language
INTRODUCTION
During the process of phonological acquisition, the child must learn how to deal with countless auditory, articulatory and acoustic clues, in order to acquire the contrasts between different linguistic units, phonological rules, syllabic structures, phonotactic constraints, stress of the word, among other aspects that are part of the target language(1).
Some studies point to the presence of a system with basic structures at the beginning of the phonological development, and from that limited representation, the child gradually starts to improve his phonology(2,3). While the acquisition of the sounds system did not reach all the set out standards in the language, speakers use some repair strategies, in order to adjust their difficulties in speech production(4). However, those strategies are eliminated with age progression, and the consequent maturation and sophistication of the linguistic background and of the phono-articulatory organs.
On the other hand, children who use deviant repair strategies and/or are over the age group of acquisition of a specific segment or syllabic structure are commonly found at Speech-Language Pathology practices(4,5). Those strategies present a stagnation in the course of phonological development, characterized by the lack of domain of some segments, features and/or syllabic constituents, which are part of the phonological disorder condition (PD)(6).
The plosive consonants, the class of sounds that is investigated in this study, are typically acquired in the phonological system before the third year of life; more specifically, /p/, /b/, /t/ and /d/ are acquired around the first and a half year of life, /k/ around one year and seven months, and, finally, /g/ around one year and eight months(4,7,8).
One of the repair strategies adopted during the attempt of production of these phonemes is the non-stabilization of the marked value of the feature [voice] for voiced phonemes(2). Some studies mention that the difficulty in relation to the establishment of the feature [+voice] of plosive phones is highly prevalent in the PD(9-11). Undoubtedly, homonym productions of two words with different meanings by using the devoicing strategy, such as in /kalo/ and /galo/, produced respectively as ['kalu] and ['kalu], reflect in a depletion in the subject's speech intelligibility.
Besides impairing the speech intelligibility and the listener's perception, the stabilization of the feature [+voice] in children with PD who are enrolled in phonological therapy is a mission of difficult overcoming(12). The voicing contrast of the plosive sounds involves an articulatory and acoustic refinement of the gestures that are produced in the oral cavity and also in larynx, requiring a complex temporal-spatial organization of the movements from phono-articulatory organs(13).
By establishing a relation with the presence or the absence of a subjacent knowledge of the voicing contrast to the development of the therapy in children with PD, some authors indicate that the detection of a productive knowledge with the help of acoustic analysis seems to be a facilitator factor of the rapid generalization of the phonological standards(14).
During the production of plosive segments, two important articulatory moments are observed. The first is the air flow obstruction generated by the phono-articulatory organs with the increase of the intra-oral pressure, which causes, in a second moment, the sudden liberation of that occlusion. According to the acoustic point of view, in the first moment, the spectrogram shows the production of a silence, followed by a brief transient noise known as burst(9).
For the voicing contrast of plosive phones, some acoustic parameters were researched in order to associate its influence in the differentiation among the segments [+voice]. Some of them are: the voice onset time (VOT)(9,10,15-17), the length of the vowel adjacent to the plosive consonant(10,17,18), the burst amplitude(9,15), and the length of the occlusion that precedes the burst(18,19).
Even with the high frequency of devoicing in children with PD, especially Brazilian Portuguese (BP) speakers, there is a lack of studies about this issue. Investigations that involve the analysis of acoustic parameters that are responsible for the contrast of plosive phones [+voice], in the speech of children with and without speech alteration, intend not only to provide theoretical subsidies in relation to the production of plosive sounds of PB, but also in a clinic perspective, offer a comprehension and the applicability of those acoustic clues during all the therapeutic process. Then, it will be possible to propitiate, for therapist and patient, an objective and reliable return of the characteristics of the speech production of the individual.
This study basically aimed to investigate if children with PD present distinct characteristics regarding voiceless and voiced plosive phones, when compared to children within typical phonological development (TPD).
METHODS
This study was approved by the Research Ethics Committee of the Universidade Federal de Santa Maria (UFSM/RS), under process number 23081.008886/2009-29. The study was conducted at a school clinic linked to UFSM, and also to two public schools located in the same city.
At the school clinic, individuals with PD were selected from the screening results of subjects queued at the Speech Sector of the Service. Then, their parents or legal guardians were contacted by telephone and invited to participate in the research. At the schools, a meeting was set with parents or guardians of all the enrolled students that met the age group of this study. When it was not possible to set a meeting, the consent term, containing general information (identification of the responsible researcher, sponsoring institution, etc.), justification, objectives, procedures, possible discomforts, risks and benefits of the study, was sent to the parents through the students themselves.
Thirty seven children with TPD and 17 children with PD were evaluated. However, only 16 children met the inclusion criteria and accepted to participate in this research. Then, they were divided into two groups:
- Group of children with typical phonological development (GTPD): composed of 11 children, six male and five female, aged between 5 and 8 years (mean=7 years and 5 months; SD=9.9 months), and;
- Group of children with phonological disorder (GPD): composed by five children, all male, aged between 5 and 7 years (mean=7 years; SD=11.8 months). All children of the GPD presented difficulty in the production of voiced plosive phones, besides other repair strategies regarding other segments of the BP. Below we presented the percentages of production of plosive phones considering each individual of the group, based on the auditory-perceptive analysis carried out through the Children Phonological Assessment (CPA)(20) (Chart 1).
The following inclusion criteria were considered for the GTPD: to present complete phonetic and phonological inventories; to be aged between 4 and 8 years and 11 months; not to have previously received any type of auditory and phonological therapy; to be a native speaker of BP (dialect of Rio Grande do Sul, Brazil); and not to present history of bilingualism. It was adopted as exclusion criteria the presence of vocal, auditory or language alterations, evident deficits in neurological, cognitive, psychological and/or emotional aspects, as well as the presence of alterations in the stomatognathic system, which could interfere in the phonological system.
With the exception of the first inclusion criterion that was adopted to compose the GTPD, the other inclusion criteria were also considered for the GPD. Children from the latest group should also present a diagnosis of PD, with difficulty in the production of the feature [+voice] of plosive phonemes. All voiced plosive consonants should present up to 39% of correct production, indicating the non-acquisition of the segment, with voiceless percentage greater than or equal to 40%. All [-voice] plosives should be found in the acquired phonological system. This criterion was used based on another study(21). According to the proposal of this research, a phoneme is considered not acquired when its occurrence of correct production is equal to or less than 39%, partly acquired when the occurrence is between 40% and 79%, and acquired when its occurrence is from 80% to 100%.
For the sample selection, for both groups, it was carried out an initial interview and a phonological and auditory screening which was composed by:
- Initial interview, conducted with parents and/or guardians: consisted of identification questions, including place and date of birth, history of house (if he/she had lived in another city or state), language (if he/she used to speak another language), previous treatment (if he/she had had speech therapy), and health history (pathophysiological background).
- Stomatognathic system evaluation: observation of the appearance, posture, muscle tension, and mobility of the articulators (tongue, lips, cheeks, soft palate, hard palate, and teeth) and functions (breathing, sucking, chewing and swallowing).
- Language, speech and voice evaluations: they were performed based on a logical sequence of four events (figures). The child was asked to organize the pictures in sequence and tell a story. Through speech and spontaneous naming, it was observed the aspects of receptive and oral expressive language, possible phonetic, phonological and vocal quality alterations. Furthermore, for individuals in the GPD, the CPA was applied in order to obtain a more complete description of their phonetic and phonological systems. This evaluation was divided into five themed drawings that allowed obtaining a balanced speech sample by spontaneous naming, containing all the contrastive phonemes of BP, at all syllabic positions. In addition to the CPA figures, the circus figure was also used, as proposed in other study(22).
- Hearing screening: air-conduction hearing thresholds were surveyed in the frequency range from 500 Hz to 4 kHz, tested at 20 dB HL (scan mode). It was used the Interacoustics® AS208 Screening Audiometer, calibrated and respecting the care of the ambient noise.
During the course of the evaluations, when the alterations were detected, parents and/or guardians, as well as the school, were informed about the need for further evaluations and/or examinations. It was also made referrals to other professionals, as needed for each case.
For the collection of data that were submitted to acoustic analysis, it was created a list of words with the same linguistic context (disyllable and paroxitone), whereby the six plosive phonemes of BP were compared (['papa], ['baba], ['tata], ['dada], ['kaka] and ['gaga]). These words were inserted into a carrier phrase ("Speak _____ again"). Each plosive segment had two sets of three replicates arranged in a random sequence, a total of 36 sentences for each individual, and a total of 576 productions (two registers x three replicates x six plosive x 16 children = 576 productions). The carrier phrases were presented through headphones Sennheiser® HD280 PRO, and individuals were instructed to repeat the entire phrase in the habitual vocal quality. For recording the data, it was used a soundproof booth, an omnidirectional microphone (Behringer® EMC8000) placed on a pedestal at approximately 4 cm from the mouth of the individual, and an external sound card (M-AUDIO®, model FW 410) connected to a laptop computer (Windows XP SP3). Registers were made directly in the MATLAB V7.1 SP3 (Simulink Signal Processing Toolbox V6.4) in wave file and high resolution (24 bits and 96 kHz).
Then, speech registers were analyzed in the audio processing software Praat version 5.1.29 (available at www.praat.org), with sample rate of 96 kHz and 16 bits.
With the spectroscopy, it was possible to measure the VOT values, the vowel length, the burst amplitude, and the occlusion length. For extraction of the VOT in initial and medial onset, the burst and the initial vocal folds vibration were located. The VOT values (in milliseconds ms) were taken from the spectrogram as it follows:
- for the voiceless plosive phones, it was collected the measure of the length of the segment between the burst of the plosive segment and the first regular pulse of the vowel [a] of the same syllable;
- for the voiced plosive phones, it was collected the measure of the segment between the pre-voicing of the plosive segment and the register of burst. However, the VOT of plosive sounds in which the pre-voicing was considered absent were measured as the voiceless plosives.
To measure the length of the vowel (in ms) presented in the target word in initial and medial onset, it was adopted the criterion of first and last regular cycle adjacent to the plosive consonant to determine the limits of the vowel.
The burst amplitude (in decibel dB) in medial and initial onset was extracted from the central measure of the burst total length. In the presence of multiple bursts, the same procedure was performed for each burst, and then an arithmetic mean of the values was conducted.
The length of occlusion (in ms) in medial onset was measured from the end of the vowel of the stressed syllable (the vowel of the last regular cycle) until the beginning of the burst of the next plosive segment. Where the vowel was followed by a portion with spectral characteristics of noise (breathy vowel), this one was also considered within the range of occlusion.
It is noteworthy that the words that had omission or inaccurate production of some of the analyzed parameters were excluded from the sample before being statistically analyzed. At the same time, in each individual it was calculated the mean of the acoustic parameter values in all replicates of each target word.
All acoustic parameters of the voiceless and voiced plosive sounds were measured and tabulated individually by each individual and for each group separately. The acoustic parameters of these phones were compared statistically in each group using the Wilcoxon test. Thereafter, the acoustic parameters were statistically compared between groups (GTPD and GPD) by using the Mann-Whitney test. The significance level adopted was 5% (p<0.05).
These tests were chosen due to the absence of normal distribution and sample size. The Wilcoxon test is used for the analysis of related samples and the Mann-Whitney test for two independent groups. Non-parametric tests assign points to the measure of variables, so that the values of median, mean, standard deviation, variation and coefficient of variation were used to illustrate all the information for each group.
RESULTS
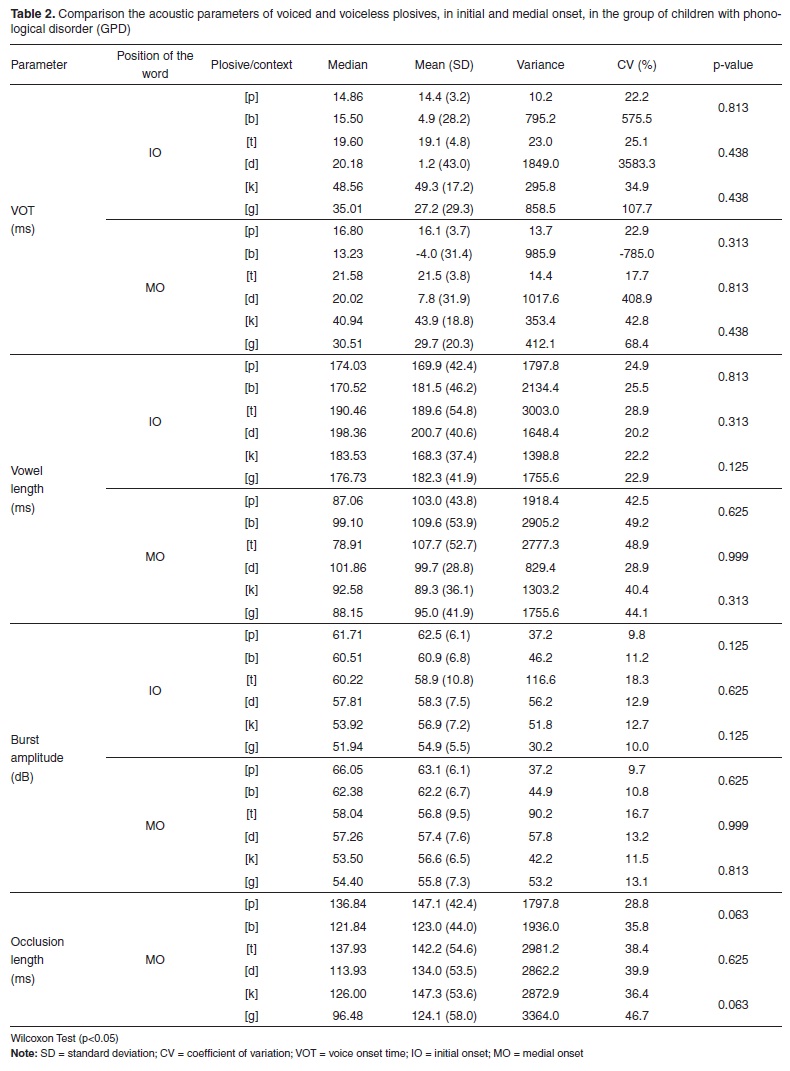
When the acoustic parameters (VOT, vowel length, burst amplitude, and occlusion length) of voiceless and voiced plosive sounds were compared in initial and medial onset in each of the analyzed groups, it was observed that the GTPD used clues of most acoustic tasks in a distinct way, according to the plosive phone [+voice] or [-voice], marking, this way, the voicing contrast. However, the same was not verified in the GPD results (Tables 1 and 2).
The comparisons of acoustic parameters between the two groups, for each phone and also for the two syllabic positions (initial and medial onset), it was evident that the VOT and the occlusion length of the voiced plosive segments were the only distinct registers between GTPD and GPD. These acoustic clues seem to represent the difficulty of children with PD in this study to establish the production of plosive sounds [+voice] (Tables 3 and 4).
DISCUSSION
According to the presented results, it was confirmed that children with TPD, in the age group that was investigated in this study, demonstrate that they have a domain about the contrast of the feature [±voice], once many differences were found between the acoustic clues of voiced and voiceless plosive sounds, marking the characterization of the voicing contrast of these segments, except for the last investigated register, the burst amplitude (Table 1). Other studies also report specific linguistic, acoustic and articulatory knowledge of phonological patterns of language by children with typical development, either by comparing the VOT(10,13,23-25), the length of the vowel(10,23) or other acoustic clues(14,19,24,26).
From the GTPD data, it was observed that the VOT is a determining register in the establishment of voicing contrast. The results agree with another study that presented that the length of VOT showed higher values for the voiced segments, which mostly showed a pre-voicing anterior to the burst, distinguishing it from the voiceless ones(10).
The length of the vowel that is adjacent to the plosive consonant also showed to be a distinct acoustic parameter between voiceless and voiced plosive sounds. When preceded or followed by a voiced segment, the vowel tends to be longer than when in the context of voiceless plosive sounds, which coincides with other studies(9,10,17,18).
In relation to burst amplitude, few significant results were found. However, from the median and mean values (Table 1), it is possible to observe that the voiced plosive sounds were slightly more intense in the release of the occlusion than the voiceless ones, unlike the findings of other studies(18,19).
Also in the GTPD, the length of occlusion of the articulators for the production of plosive consonants in medial onset was higher in voiceless plosive sounds, corroborating the findings of other studies(18,19).
On the other hand, in relation to the results for the GPD, unlike what was observed for the GTPD, children with phonological alterations and difficulty in stabilizing the feature [+voice], no significant difference was observed in the sound differentiation through the investigated acoustic clues (Table 2). It was evident, then, the difficulty of these children in manipulating some acoustic characteristics that are involved in the production of voiced phonemes. Other authors mention(15) that this difficulty may be related to physiological immaturity or these elements are not equally perceptible.
By comparing the acoustic registers of children with TPD and PD, it was noticed that the greatest obstacle to adequate production of voiced plosive segments in children with TPD seems to be related to the production of VOT and length of occlusion of the segments [+voice] (Tables 3 and 4). This is justified once these parameters showed to be differentiated from GTPD, with statistical significance. The values of VOT and length of occlusion of voiceless segments, length of the vowel and burst amplitude, these registers are similar between the two groups, with no difference between them.
The production of pre-voicing, i.e., the production of negative VOT was the most difficult problem of TPD to be observed in this study. To produce a suitable VOT, and thus keep the distinctive language relations, the child must learn to produce the required glottic and supraglottic gestures and coordinate them in a precise time interval(13).
For BP, the vibration of the vocal folds that is prior to burst is crucial acoustic register for the distinction of negative and positive VOT, as well as in other languages such as Dutch(27). It is believed that the same articulatory complexity and importance are involved in maintaining the length of the occlusion.
Regarding the vowel length in the GPD, even though not showing any distinction to voicing with significant results, it showed values close to the values of the GTPD. Thus, it seems that vowel length reflects the first tests or trials of children with PD in stabilizing the tone contrast of their language.
In another study(28), it was also referred the influence of the acoustic pattern of the length of the vowel in the acquisition of segments in general. The author stated that the acquisition of this length happens before the acquisition of consonants and syllables, possibly because they are gestures with initial and final parts classified as slower than the others, minimally co-articulated, which help in the construction of motor representations of consonant segments.
The amplitude of the release of the occlusion was the second acoustic parameter that showed no difference between the groups in this study. However, it is noticed that this parameter also showed few differences in the context of voiceless and voiced plosive sounds in the sample in each group.
This result differs from another research(14), which studied the speech of seven boys with phonological alteration, and found differences in the burst amplitude of voiced and voiceless plosive segments, in order to mark the voicing contrast in deviant speech.
Based on results such as those related to burst amplitude, it is important to note that the speech signal presents a large variety of acoustic properties that help the speaker to encode the linguistic segments. However, not all these information are necessary for discrimination and word recognition(27). This can be stated in the case of plosive phones, which have a large number of redundant clues to their identification(9).
From the results of the GTPD, it is also possible to observe that the acoustic registers that showed higher p-values, hence less tendency to statistical significance, were vowel length and burst amplitude. This suggests that these two clues may be secondary to the acquisition of the voicing contrast of plosive consonants. As previously mentioned, the comparison between groups (GTPD versus GPD) showed no differences in the parameters of vowel length and burst amplitude. Thus, it is assumed that children with PD have a tendency to prioritize secondary clues, i.e., less robust in an attempt to overcome their difficulties in the production of plosives [+voice].
Several studies have been conducted with the aim to investigate the voicing contrasts of deviant speech and, often, relate them to the standards of the target language(17,26,29). One of these studies(17) intended to describe and compare the measures of VOT and vowel length and children with TPD and PD. This study found that children with TPD produced VOT and vowel length differently in the context of voiceless and voiced plosive sounds. However, for children with PD there were no differences between the VOT of voiced and voiceless plosive sounds, as well as between vowels succeeded by a voiceless or voiced sound, as in this study. All plosive VOTs of this group presented lower values than the VOTs of the group with typical speech, suggesting that children with PD, besides not producing the sound, do not emit the voiceless plosive segments with the same standard of normality.
In addition, by contrasting some acoustic registers of children with TPD and PD, other authors(26) observed that some children with PD failed to differentiate VOT values of voiced and voiceless plosive sounds. These results were interpreted in the sense that some children with PD had lower maturation of the control patterns of length of speech. However, as typical in speech, these children showed differences in the vowel length and length of occlusion in voiceless or voiced contexts.
This research, besides its primary objective, which was the characterization of voicing contrasting of plosive segments, also had the aim to disseminate acoustic spectrography of speech as a complement to perceptive-auditory analysis. It is believed that the use of acoustic investigations in the routine of speech-language pathology practice may provide better diagnostics and safer and more effective therapeutic conducts.
And yet, given the prevalence of devoicing in preschoolers and school children in Brazil, the discussions presented here intend to direct the clinical knowledge related to the acquisition of the contrast of voicing during all stages of phonological therapy of these cases, quantifying, thereby, the phonological knowledge of these children front to the use or not of the investigated acoustic clues.
The scientific rigor of the selection criteria adopted for inclusion of the individuals in this research ended up restricting the number of individuals who were able to participate in the study. Thus, it is not possible to answer some questions, as the influence of variables such as gender, age, organization of the phonological system and auditory input in the acquisition of voicing contrast of plosive phones. Therefore, further studies that prioritize those goals are suggested.
CONCLUSION
The marking of voicing contrast in the deviant group was different in relation to the GTPD. The children with PD evaluated in this study did not employ the acoustic characteristics responsible for the voicing contrast in the production of voiced and voiceless plosive consonants.
The VOT and occlusion length of the voiced plosive phones were the most difficult acoustic parameters to be controlled and produced by children with PD. Hence, these two clues can provide much information to the speech therapist regarding the presence or absence of phonological knowledge related to the contrast of voicing, both before and during therapy, thus helping in the acquisition process of the feature [+voice], and in establishing the prognosis and therapeutic discharge.
REFERENCES
- 1. Santos RS. Adquirindo a fonologia de uma língua: produção, percepção e representação fonológica. Alfa. 2008;2(52):465-81.
- 2. Hernandorena CL. Sobre a descrição de desvios fonológicos e de fenômenos da aquisição da fonologia. Letras de Hoje. 1995;30(4):91-110.
- 3. Mota HB. Aquisição segmental do português: um modelo implicacional de complexidade de traços [tese]. Porto Alegre: Pontifícia Universidade Católica do Rio Grande do Sul Curso de Pós-Graduação em Letras; 1996.
- 4. Lamprecht RR, Bonilha GF, Freitas GC, Matzenauer CL, Mezzomo CL, Oliveira CC et al. Aquisição fonológica do português: perfil de desenvolvimento e subsídios para a terapia. Porto Alegre: Artmed; 2004.
- 5. Ghisleni MR, Keske-Soares M, Mezzomo CL. O uso das estratégias de reparo, considerando a gravidade do desvio fonológico evolutivo. Rev CEFAC. 2010;12(5):766-71.
- 6. Ribas LP. Aquisição das líquidas por crianças com desvio fonológico: aquisição silábica ou segmental? Revista Letras (UFSM). 2008;36(1):129-49.
- 7. Ferrante C, Borsel JV, Pereira MM. Aquisição fonológica de crianças de classe sócio econômica alta. Rev CEFAC. 2008;10(4):154-60.
- 8. Toreti G, Ribas LP. Aquisição fonológica: descrição longitudinal dos dados de fala de uma criança com desenvolvimento típico. Letrônica. 2010;3(1):42-61.
- 9. Levy IP. Uma nova face da nau dos insensatos: a dificuldade de vozear obstruintes em crianças de idade escolar [tese]. Campinas: Universidade Federal de Campinas Doutorado em Ciências; 1993.
- 10. Bonatto MT. Vozes infantis: a caracterização do contraste de vozeamento das consoantes plosivas no Português Brasileiro na fala de crianças de 3 a 12 anos [tese]. São Paulo: Pontifícia Universidade Católica de São Paulo Doutorado em Linguística Aplicada e Estudos da linguagem; 2007.
- 11. Wertzner HF, Pagan LO, Galea DE, Papp AC. Características fonológicas de crianças com transtorno fonológico com e sem histórico de otite média. Rev Soc Bras Fonoaudiol. 2007;12(1):41-7.
- 12. Silva AP. Mudanças fonológicas no tratamento dos desvios fonológicos com o modelo de oposições máximas modificado utilizando 'contraste' e 'reforço' do traço [voz] [dissertação]. Santa Maria: Universidade Federal de Santa Maria; 2007.
- 13. Lowenstein JH, Nittrouer S. Patterns of acquisition of native voice onset time in english-learning children. J Acoust Soc Am. 2008;124(2):1180-91.
- 14. Tyler AA, Figurski GR, Langsdale T. Relationships between acoustically determined knowledge of stop place and voicing contrasts and phonological treatment progress. J Speech Hear Res. 1993;36(4):746-59.
- 15. Forrest K, Rockman BK. Acoustic and perceptual analysis of word-initial stop consonants in phonologically disordered children. J Speech Hear Res. 1988;31(3):449-59.
- 16. Van Alphen PM, Smits, R. Acoustical and perceptual analysis of the voicing distinction in Dutch initial plosives: the role of prevoicing. J Phonetics. 2004;32(4):455-91.
- 17. Gurgueira AL. Estudo acústico dos fonemas surdos e sonoros do Português do Brasil, em crianças com distúrbio fonológico apresentando processo fonológico de ensurdecimento [tese]. São Paulo: Universidade Federal de São Paulo Doutorado em Semiótica e Linguística Geral; 2006.
- 18. Snoerena ND, Halle PA, Seguia J. A voice for the voiceless: production and perception of assimilated stops in French. J Phonetics. 2006;34(2):241-68.
- 19. Barroco MA, Domingues MT, Pires MF, Lousada M, Jesus LM. Análise temporal das oclusivas orais do Português Europeu: um estudo de caso de normalidade e perturbação fonológica. Rev CEFAC. 2007;9(2):154-63.
- 20. Yavas M, Hernandorena CL, Lamprecht RR. Avaliação fonológica da criança: reeducação e terapia. Porto Alegre: Artes Médicas; 1992.
- 21. Bernhardt B. Developmental implications of nonlinear phonological theory. Clin Linguist Phon. 1992;6(4):259-81.
- 22. Hernandorena CL, Lamprecht RR. A aquisição das consoantes líquidas do Português. Letras Hoje. 1997;32(4):7-22.
- 23. Koenig LL. Laryngeal factors in voiceless consonant production in men, women, and 5-year-olds. J Speech Lang Hear Res. 2000;43(5):1211-28.
- 24. Kim M, Stoel-Gammon C. The acquisition of Korean word-initial stops. J Acoust Soc Am. 2009;125(6):3950-61.
- 25. Grigos MI. Changes in articulator movement variability during phonemic development: a longitudinal study. J Speech Lang Hear Res. 2009;52(1):164-77.
- 26. Catts HW, Jensen PJ. Speech timing of phonologically disordered children: voicing contrast of initial and final stop consonants. J Speech Hear Res. 1983;26(4):501-10.
- 27. Van Alphen PM, McQueen JM. The effect of voice onset time differences on lexical access in Dutch. J Exp Psychol Hum Percept Perform. 2006;32(1):178-96.
- 28. Gama-Rossi A. Relações entre percepção e produção na aquisição da duração da vogal no português brasileiro. Letras Hoje. 2001;36(3):177-86.
- 29. Souza AP, Scott LC, Mezzomo CL, Dias RF, Giacchini V. Avaliações acústica e perceptiva de fala nos processos de dessonorização de obstruintes. Rev CEFAC. 2011;13(6):1127-32.
Endereço para correspondência:
Publication Dates
-
Publication in this collection
25 Sept 2012 -
Date of issue
2012
History
-
Received
30 Mar 2011 -
Accepted
29 Nov 2011