SCIENTIFIC COMMENTS
Sickle cell disease: from the beginning until it was recognized as a public health disease
Paulo Cesar Naoum
Academia de Ciência e Tecnologia de São José do Rio Preto, São José do Rio Preto (SP), Brazil
Correspondence Correspondence: Paulo Cesar Naoum Academia de Ciência e Tecnologia de São José do Rio Preto Rua Bonfá Natale, 1860 - Santos Dumont 15020-130 - São José do Rio Preto (SP), Brazil Phone.: 55 17 3233 4490 a.c.t@terra.com.br
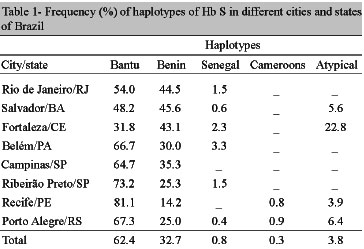
Sickle cell disease in Brazil, when explained in medical, genetic, social or anthropological terms, has a strong relationship with the introduction of Black Africans in our country. In 1932, Nina Rodrigues a Brazilian historian, researched about the origin of the African slaves that came to Brazil. He used data obtained from the customs department of the port in Salvador, Bahia. This researcher concluded that almost all of the African slaves were from two regions on the west coast of Africa: the Mina Coast (approximately the region of Benin, Togo and Ghana) and Angola.(1) Recent studies using mitochondrial DNA analysis, performed by Sales in 2004, showed that 58.8% of the Brazilian Black people originate from Central West Africa which includes Angola, and 32.1% come from West Africa that includes some regions that are believed to have belonged to the Mina Coast.(2) Molecular analysis of Hb S haplotypes were made by several Brazilian researchers in different regions of the country.(3-8) These analyses enable the African origin of Brazilian Black people to be tracked by means of beta S globin gene (Table 1).
Studies showed that the Bantu and Benin haplotypes are prevalent however the frequencies vary according to the region studied. These results reveal a heterogeneous employment of slave workers in the northeastern states of Brazil with incredibly similar results obtained in the cities of Rio de Janeiro and Salvador, as well as in Belém and Campinas.
Knowledge of the Hb S haplotypes of patients with sickle cell anemia is an important molecular marker of the severity of disease, the clinical and hematological repercussions, as well as of the Hb Fetal concentrations in these patients.(9,10) Thus, this article aims at emphasizing the necessity of associating sickle cell disease with its evolution in Brazilian science, setting it in the context of Brazilian public health policies.
The first article published in Brazil in which the cases were probably of sickle cell disease was made by Doctor Cruz Jobim in Rio de Janeiro.(11) This paper had a social basis because the author emphasized that "it is a very specific illness that mostly affects poor black people". After the effectively scientific publication about the clinic characteristics of sickle cell disease described in 1910 by Herrick(12) and the discovery of the distortion of sickled cells that was made by Emmel in 1917,(13) there was a gap of almost thirty years with few scientific advances in sickle cell disease. So a special mention must be made of Accioly who, in 1947, suggested in a scientific article published in Brazil that sickle cell anemia must be the homozygous condition of the gene that causes the sickling phenomenon.(14) The genetic interest about sickle cell disease in the Brazilian population called the attention of the geneticists Tondo and Salzano. These two researchers studied abnormal hemoglobins in the Brazilian Indian population in 1960(15) and the Brazilian Black people in 1962,(16) in particular Hb S. In 1965, Araujo studied the prevalence of hemoglobinopathies in patients of Hospital das Clínicas in São Paulo and concluded that the sickle cell trait (Hb AS) was the most prevalent abnormal hemoglobin, especially in the black people.(17) However, only in 1969, Marinho presented a dissertation to the Brazilian Medical Academy about the clinical characteristics of sickle cell disease of patients from the Instituto de Hematologia Arthur Siqueira Cavalcanti (currently HEMORIO) in Rio de Janeiro.(18) The scientific setting that suggested that sickle cell disease is of importance to public health stimulated Naoum et al.(19) to carry out a scientific study to detect abnormal hemoglobins in the state of São Paulo. During the period from 1978 to 1982 they analyzed 18 thousand individuals from 19 cities that were characterized as important medical centers in the state of São Paulo. Among the different abnormal hemoglobins that were identified, the sickle cell trait was prevalent in 1.6% of the total population (White and Black); the frequency of sickle cell trait in black individuals was 9.0%, while in white people it was 0.96%. This scientific experience stimulated the author of this article to create an educational program on the laboratorial identification of hemoglobinopathies, especially sickle cell disease, aimed at healthcare professionals in several Brazilian regions. With significant collaboration of Claudia Regina Bonini Domingos, Ivan de Lucena Angulo and other colleagues, courses were started in 1980 and were offered for 25 years without interruption. In 1981, Hutz carried out one of the most complete studies on the natural history of sickle cell anemia in Brazil.(20) She used the data of 409 patients registered in the HEMORIO in Rio de Janeiro; the results of this study are medical references until today. In this same period two pioneer researches were performed to identify Hb S in newborn babies. The first study was made in 1976 by Ramalho et al. in newborns from Campinas(21) and the second study was made in 1986 by Ruiz et al. with newborns from Santos.(22)
The gradual development in the diagnosis of the sickle cell disease stimulated Ramalho to publish a book about the importance of this disease to public health in Brazil.(23) The possibility that this disease may be a real problem in public health caused both scientific and political measures. One pioneer study was organized in the 1990s by Bandalise et al. in Campinas, the results of which were published in 2004.(24) The Campinas experience made the local government of the city establish the first screening program of newborns in Brazil to detect sickle cell anemia.(25) Special mention must go to José Nelio Januario who, in 1993, founded the Núcleo de Ações e Pesquisas em Apoio ao Diagnóstico (NUPAD) in Belo Horizonte, MG. During 17 years NUPAD analyzed more than four million blood samples of newborns with the purpose of identifying sickle cell disease and other important diseases, such as congenital hypothyroidism, phenylketonuria and cystic fibrosis.
The result of all this effort over many years with scattered and diverse studies on the general aspects of sickle cell disease was compensated in 2001 with the publication of a decree by the Health Ministry of Brazil that established the National Newborn Screening Program.(26) The immediate success of this program caused the Health Ministry of Brazil to extend it to the government healthcare plan in 2005.(27,28) In 2010, during the V Brazilian Symposium of Sickle Cell Disease and other Hemoglobinopathies, in Belo Horizonte, MG, with the support of the Health Ministry of Brazil, it was revealed that about 3500 newborns are born every year with sickle cell disease in Brazil and that 200 thousand are born with the sickle cell trait. The highest prevalence of newborns with sickle cell disease occurs in Bahia (Table 2).
To complete this article it is also very important to recognize the effort that many Brazilian researchers have dedicated to study sickle cell disease and other hemoglobinopathies in different regions of Brazil, as well as the associations of sickle cell anemia formed by patients and collaborates, and scientific societies, in particular the Brazilian Society of Hematology and Hemotherapy and the Brazilian College of Hematology, recently merged as the Brazilian Association of Hematology and Hemotherapy.
Submitted: 1/26/2011
Accepted: 1/31/2011
- 1. Rodrigues N. Os africanos no Brasil. São Paulo: Editora Nacional; 1932. 408 p.
- 2. Sales A, Richards M, Lareu MV, Scozzari R, Coppa A, Torroni A, et al. The African diaspora: mitochondrial DNA and the Atlantic Slave Trade. Am J Human Genet. 2004;74(3):522-4. Comment in: Am J Hum Genet. 2004;75(3):522-4; author reply 524-6
- 3. Adorno EV, Zanette A, Lyra I, Souza CC, Santos LF, Menezes JF, et al. The beta-globin gene cluster haplotypes in sickle cell anemia patients from Northeast Brazil: a clinical and molecular view. Hemoglobin. 2004;28(3):267-71.
- 4. Figueiredo MS, Kerbauy J, Gonçalves MS, Arruda VR, Saada ST, Sonati MF, et al. Effect of alpha-thalassemia and beta globin gene cluster haplotypes on the hematological and clinical features of sickle cell anemia in Brazil. Am J Hematol. 1996;53(2):72-6.
- 5. Fleury MK. Determinação dos haplótipos do cluster da globina beta em pacientes com anemia falciforme no Rio de Janeiro [tese]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2000. 182 p.
- 6. Wagner S, Friedrish J, Job F, Hutz MH. Caracterização molecular de pacientes com anemia falciforme de Porto Alegre. Rev Bras Genet. 1996:19(Suppl):244 (abstract).
- 7. Zago MA, Figueiredo MS, Ogo SH. Bantu beta S cluster haplotype predominant among Brazilian blacks. Am J Phys Anthropol. 1992;88(3):295-8.
- 8. Bezerra MA, Santos MN, Araújo AS, Gomes YM, Abath FG, Bandeira FM. Molecular variations linked to the grouping of beta- and alpha-globin genes in neonatal patients with sickle cell disease in the State of Pernambuco, Brazil. Hemoglobin.2007;31(1):83-8.
- 9. Steinberg MH, Hsu H, Nagel RL, Milner PF, Adams JG, Benjamin L, et al. Gender and haplotype effects upon hematological manifestations of adult sickle cell anemia. Am J Hematol. 1995; 48(3):175-81.
- 10. Naoum PC, Naoum FA. Doença das células falciformes. São Paulo: Sarvier; 2004. 224 p.
- 11. Cruz Jobim JM. As moléstias que mais afligem a classe pobre do Rio de Janeiro. Rev Méd Flum. 1835.
- 12. Herrick JB. Peculiar elongated and sickle-shaped red blood corpuscles in a case of severe anemia. Arch Int Med 1910;6:517-20.
- 13. Emmel VE. A study of the erythrocytes in a case of severe anemia with elongated sickle shaped red blood corpuscles. Arch Intern Med. 1917;20:586-98.
- 14. Accioly J. Anemia falciforme. Arq Fac Med Univ Bahia. 1947; 2:169-98.
- 15. Tondo CV, Salzano FM. Hemoglobin types of Caingang Indians of Brazil. Science. 1960;132:1893-94.
- 16. Tondo CV, Salzano FM. Abnormal hemoglobins in a Brazilian Negro population. Am J Hum Genet. 1962;14:401-9.
- 17. Araujo JT. Hemoglobinas anormais em São Paulo, métodos de estudo, incidência. J Bras Med. 1965;9:1264-83.
- 18. Marinho HM. Hemoglobinopatia S - doença eritrofalcêmica. Rio de Janeiro: Academia Nacional de Medicina; 1969.
- 19. Naoum PC, Mattos LC, Cury PR. Prevalence and geographic distribution of abnormal hemoglobins in State of São Paulo, Brazil. Bull Pan Am Health Organ. 1984;18(2):127-38.
- 20. Hutz MH. História natural da anemia falciforme em pacientes da região metropolitana do Rio de Janeiro [tese]. Porto Alegre: Universidade Federal do Rio Grande do Sul; 1981. 270 p.
- 21. Ramalho AS, Nassim-Jorge R, Oliveira JA, Pereira DA. Hemoglobina S em recém-nascidos brasileiros. J Pediatr (Rio J). 1976; 41:9-10.
- 22. Ruiz MA, Guerra CC, Naoum PC. Detecção de hemoglobinas anormais em sangue de cordão de recém-nascidos na cidade de Santos, SP, através de eletroforese em gel de ágar amido. Bol Soc Bras Hematol Hemot. 1986;8(1): 8-13.
- 23. Ramalho AS. As hemoglobinopatias hereditárias. Um problema de saúde pública no Brasil. Ribeirão Preto: Editora Sociedade Brasileira de Genética; 1986.
- 24. Brandalise S, Pinheiro V, Gabetta CS, Hambleton I, Searjeant G. New-born screening for sickle cell disease in Brazil: the Campinas experience. Clin J Lab Haematol. 2004;26(1):15-9.
- 25. Campinas. Prefeitura Municipal de Campinas. Programa de triagem neonatal para anemia falciforme [Internet]. Campinas (SP): PMC; 1997. [citado 2010 Jul 27]. Disponível em: http://2009.campinas.sp.gov.br/saude/programas/anemia_falciforme/nota_tecnica.htm
-
26Brasil. Ministério da Saúde. Portaria GM/MS nº 822/GM em 6 de junho de 2001. Estabelece a obrigatoriedade de que os hospitais e demais estabelecimentos de atenção à saúde de gestantes, públicos e particulares, procedam a exames visando o diagnóstico e terapêutica de anormalidades no metabolismo do recém-nascido, bem como prestar orientação aos pais [Internet]. Brasília, DF: MS; 2001. [citado 2010 Jan 21]. Disponível em: http://dtr2001.saude.gov.br/sas/PORTARIAS/Port2001/GM/GM-822.htm
-
27Brasil. Ministério da Saúde. Portaria GM/MS nº 1391, 16 de agosto de 2005. Institui no âmbito do Sistema Único de Saúde, as diretrizes para a Política Nacional de Atenção Integral às Pessoas com Doença Falciforme e outras Hemoglobinopatias [Internet]. Brasília, DF: MS; 2005. [citado 2010 Set 15]. Disponível em: http://dtr2001.saude.gov.br/sas/PORTARIAS/Port2005/GM/GM-1391.htm
-
28Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Especializada. Manual de Educação em Saúde, Autocuidado na Doença Falciforme [Internet] . Brasília: Editora do Ministério da Saúde; 2008. [citado 2010 Out 15]. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/manual_educacao_saude_volume1.pdf
Correspondence:
Publication Dates
-
Publication in this collection
05 May 2011 -
Date of issue
Feb 2011