Abstract
OBJECTIVE: To assess the burden and quality of life of caregivers of patients with sickle cell anemia taking hydroxyurea versus those of patients not taking hydroxyurea. METHODS: A cross-sectional study was performed of caregivers of outpatients with sickle cell anemia in two public hospitals in Campo Grande, MS, from January through June 2010. The World Health Organization Quality of Life-BREF Scale and the Caregiver Burden Scale were used. RESULTS: Of the 37 caregivers in this study, 81.1% were women, 73.0% were mothers, 59.5% were married, 54.1%were mulattos, 48.6% were housewives, 54.1% had family incomes of up to one minimum wage and 75.7% had onlycompleted elementary education. The mean duration of care provided (time after diagnosis) was 16.08 ± 9.88 yearsand 89.2% reported that they provided 24-hour care. Regarding health, 27.0% of study participants reported having physical and 13.5% emotional problems. There were no significant relationships between these variables either with the different domains or the total score of the WHOQOL-BREF comparing caregivers of patients taking hydroxyurea versusthose of patients not taking hydroxyurea. There was a moderate negative linear correlation between the WHOQOL-BREF and the Caregiver Burden Scale scores (linear correlation test of Pearson: p-value = 0.003, r = -0.477). The burden of caregivers of patients who did not take hydroxyurea was significantly higher than those of patients who took the medication in terms of general tension, disappointment, environment and total score (student t-test: p-value < 0.05). CONCLUSION: In the perception of the caregiver, looking after sickle cell anemia patients represents a moderate negative burden.
Anemia, sickle cell; Caregivers; Quality of life; Hydroxyurea
ORIGINAL ARTICLE
The burden and quality of life of caregivers of sickle cell anemia patients taking hydroxyurea versus those not taking hydroxyurea
Luiz Bernardino Lima da Silva; Maria Lúcia Ivo; Albert Schiaveto de Souza; Elenir Rose Jardim Cury Pontes; Alexandra Maria Almeida Carvalho Pinto; Olinda Maria Rodrigues de Araujo
Universidade Federal de Mato Grosso do Sul - UFMS, Campo Grande, MS, Brazil
Corresponding author Corresponding author: Maria Lúcia Ivo Universidade Federal de Mato Grosso do Sul - UFMS Av. Senador Filinto Müller, s/nº, Bloco 9, Bairro Vila Ipiranga 79080-190 Campo Grande, MS, Brazil ivoms@terra.com.br
ABSTRACT
OBJECTIVE: To assess the burden and quality of life of caregivers of patients with sickle cell anemia taking hydroxyurea versus those of patients not taking hydroxyurea.
METHODS: A cross-sectional study was performed of caregivers of outpatients with sickle cell anemia in two public hospitals in Campo Grande, MS, from January through June 2010. The World Health Organization Quality of Life-BREF Scale and the Caregiver Burden Scale were used.
RESULTS: Of the 37 caregivers in this study, 81.1% were women, 73.0% were mothers, 59.5% were married, 54.1%were mulattos, 48.6% were housewives, 54.1% had family incomes of up to one minimum wage and 75.7% had onlycompleted elementary education. The mean duration of care provided (time after diagnosis) was 16.08 ± 9.88 yearsand 89.2% reported that they provided 24-hour care. Regarding health, 27.0% of study participants reported having physical and 13.5% emotional problems. There were no significant relationships between these variables either with the different domains or the total score of the WHOQOL-BREF comparing caregivers of patients taking hydroxyurea versusthose of patients not taking hydroxyurea. There was a moderate negative linear correlation between the WHOQOL-BREF and the Caregiver Burden Scale scores (linear correlation test of Pearson: p-value = 0.003, r = -0.477). The burden of caregivers of patients who did not take hydroxyurea was significantly higher than those of patients who took the medication in terms of general tension, disappointment, environment and total score (student t-test: p-value < 0.05).
CONCLUSION: In the perception of the caregiver, looking after sickle cell anemia patients represents a moderate negative burden.
Keywords: Anemia, sickle cell; Caregivers; Quality of life; Hydroxyurea
Introduction
The change observed in sickle cell anemia results from a substitution of the glutamic acid residue at position β6 with a valine residue (β6 Glu→Val) leading to the polymerization of hemoglobin (Hb) S molecules when deoxygenated(1). The complexity of the clinical status of homozygous individuals includes, among other complications, severe hemolysis and painful crises resulting from vascular obstruction. This has direct consequences for patients and indirect effects on caregivers causing tension within the relationship(2).
The very diagnosis and communication of the disease to the family can bring about changes(3). Although in recent decades changes in structural functions within families have been reported, most patients are cared for by female relatives(4). The role of looking after someone without being properly prepared can cause personal and family conflicts and even conflicts at work, triggering strain, stress, embarrassment, fatigue and depression(5), thuscreating a burden for caregivers and influencing their quality of life.
In these terms, burden can be defined as an objective or subjective impact, pressure or overloadon caregivers(6). 'Subjective' refers to attitudes and emotional reactions related to the experienceof caring and 'objective' relates to changes and adjustments in the domestic sphere and daily lifeof caregivers(7). Quality of life is related to lifestyle and includes the mental state, well-being andsatisfaction. These constructs are formed by knowledge and experience, by moral, religious andpsychological principles and by social and cultural values which together give the individual aperceptive ability to discriminate whether the quality of life has increased or diminished(8).
As the severity of the clinical status of sickle cell anemia imposes differing degrees of suffering to patients and their relatives(9), it is important to evaluate the burden and quality of life of caregivers because they also have needs and difficulties(10,11). The aim of this study was to assess the burden and quality of life of caregivers of patients with sickle cell anemia taking hydroxyurea versus those of patients not taking hydroxyurea.
Methods
A cross-sectional study was conducted of primary caregivers of sickle cell anemia patients under treatment in the outpatient clinics of two teaching hospitals in Campo Grande, Mato Grosso do Sul, Brazil from January through June 2010. This study defined the primary caregiver as the individual with the greatest responsibility of caring for the patient during the course of the disease(12).
Only individuals who had been taking care of the patient for more than two years were included in this study. Exclusion criteria were patients who were their own caregivers, caregivers who looked after more than one patient, the existence of a severe cognitive impairment that prevented the caregiver from understanding the questionnaire and those who did not answer 20% or more of the research instruments. The study was approved by the Ethics Committee of the Universidade Federal de Mato Grosso do Sul (UFMS - # 1609).
The first step was a survey of the two outpatient units toidentify patients with sickle cell anemia with crisis (D57.0)according to the International Classification of Diseases 10th revision (ICD-10) or sickle cell anemia without crisis (D57.1 ofICD-10). This identified 43 patients under treatment. Each patientwas then visited by one of the authors to check if they had aprimary caregiver; 37 patients (86.0%) met the inclusion criteria. The questionnaires were completed individually at a time and place(home or medical unit) chosen by the caregiver except for residentsfrom other municipalities who filled in the questionnaire at theoutpatient clinic, always supervised of the same researcher.
The quality of life (QOL) was evaluated using the WorldHealth Organization Quality of Life-BREF (WHOQOL-BREF)Scale, an abbreviated version of the WHOQOL-100 validatedin Brazil in 2000(13). The Portuguese version is supported by theassumptions that QOL is a subjective (perception of the individual)multidimensional construct that consists of positive and negativedimensions. The WHOQOL-100 comprises 100 questions dividedinto 24 groups of four questions, each of which addresses one facet,plus two open questions. A set of facets corresponds to one domain; the domains have from one to eight facets(14). This instrument is structured as domains and facets and consists of 26 questions, two general about the quality of life and 24 corresponding to each of the facets of the original instrument. These are divided into four domains: physical health (7), psychologicalhealth (6), social relationships (3) and environment (8).
The burden of caregivers was assessed by the Caregiver BurdenScale, which consists of 22 questions divided into five dimensions:general strain (8), isolation (3), disappointment (5), emotionalinvolvement (3) and environment (3). The scores for each questionrange from 1 to 4 (1 - not at all; 2 - seldom; 3 - sometimes; 4 often). The items assess emotional aspects of the individual, exceptthose referring to the environment, which is evaluated by objectivequestions, for example difficulties related to the physical environmentof the home. In order to obtain the score for each factor, the arithmeticmean of the scores assigned to each factor was calculated.
The Student's t-test was used to compare caregivers of patientstaking hydroxyurea versus those of patients not taking hydroxyureain respect to the Caregiver Burden Scale and WHOQOL-BREF. The linear correlation between the Caregiver Burden Scale andthe WHOQOL-BREF was evaluated by Pearson's correlation forwhich the coefficient ranges from -1 to +1. Positive values of rindicate a direct relationship between variables (high values of onevariable correspond to high values of the other); a negative r relatesto an inverse relation (high values of one variable correspond to lowvalues of the other); null or approximately null r values indicate the inexistence of a linear correlation. Correlation values between 0.0 and 0.3 are considered weak, between 0.3 and 0.6 moderate andbetween 0.6 and 1.0 as strong(15). The other results of the variables evaluated in this study are presented as descriptive statistics or in tables and graphs. The SPSS Software, version 13.0 was used, withan alpha error of 5% being considered significant.
Results
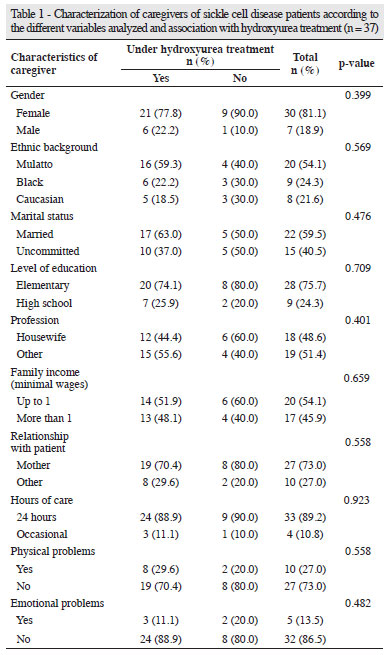
Of the 37 caregivers of patients with sickle cell anemia taking hydroxyurea or not, 81.1% were women, 54.1% were mulattos, 59.5% were married, 75.7% had only completed elementary education, the family income was up to one minimum wage for 54.1% and 48.6% were housewives. Most of the caregivers (73.0%) were mothers and the majority of caregivers (89.2%) said they cared for the patient for 24 hours per day. In regard to health, 27.0% reported having physical problems and 13.5% reported emotional issues (Table 1).
The caregivers' ages ranged from 18 to 69 years (mean age: 42.95 ± 12.97 years). The mean duration of care (from diagnosis) was 16.08 ± 9.88 years (n = 37); it was 10 years or less for 37.8% of caregivers, from 11 to 20 years for 29.7%, from 21 to 30 years for 21.6% and more than 30 years for 10.8% (Table 1).
Table 2 shows the WHOQOL-BREF scores for the physical health, psychological health, social relationships and environment domains and total score of caregivers of patients with sickle cell disease. There was no significant difference in relation to the domains and total score of the WHOQOL-BREF between caregivers of sickle cell disease patients under hydroxyurea treatment and those not taking this medication (Student's t test; p-value > 0.05).
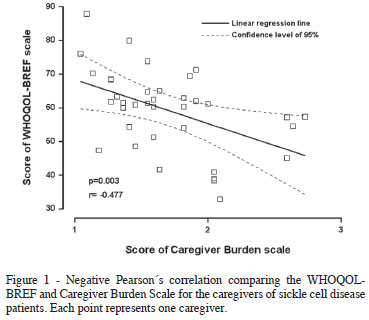
There was a moderate negative linear correlation between the WHOQOL-BREF scores and those obtained from the Caregiver Burden Scale (Pearson's correlation; p-value = 0.003, r = -0.477) between caregivers of sickle cell disease patients (Figure 1).
Figure 2 shows the scores (mean ± standard deviation) of the general strain, isolation, disappointment, emotional involvement and environment domains and total score of the Caregiver Burden Scale of caregivers of patients taking hydroxyurea versus those of patientsnot taking hydroxyurea. The burden of caregivers of patients whodid not take this medication was significantly higher than those who used it in respect to the general tension, disappointment, environment domains and total score (Student's t-test: p-value < 0.05).
Discussion
Studies targeting the burden and quality of life of primary caregivers of sickle cell disease patients are scarce in Brazil. However the number of studies on caregivers of chronic diseases in general has increased(16-18). In this study, primary caregivers of sickle cell disease patients were predominantly mulatto, women, mothers, married, with onlyelementary school, who work outside and at home and have a familyincome of up to one minimum wage (equivalent of US$ 303.45).
Research performed in Nigeria to assess the burden of caregiversof children with sickle cell disease revealed that in families with more than three children and a background of two or more hospitaladmissions, the financial aspect was often associated with stress.A significant correlation was seen between stress, finances and theparents' difficulty in dealing with episodes of illness(3).
In this study, 37.8% of caregivers have been primary caregivers as an occupation for two to ten years and 10.8% have been in this position for over 30 years. There are studies that show that the longer the duration of care, the worse the quality of life of caregivers(12).
Considering that the disease often causes changes in family dynamics that involve restructuring daily activities, the condition itself can be the source of anxiety, fear and awareness of the possibility of death; thereby removing any control of the health status(19).
In relation to the physical health, psychological health, social relationships and environment domains and the total score of the WHOQOL-BREF, this study showed that there are no significant differences between caregivers of patients taking hydroxyurea versus those of patients not taking hydroxyurea (Student's t-test: p-value > 0.05).
The results of a study that measured the quality of life in relation to the health of 221 informal caregivers of AIDS patients in Barcelona were used to discuss these findings. Among the most common effects, the authors detected increased fatigue, depression, change in the family life, less free time, a drop in economic status and ingestion of medications to relieve nervousness. The last two items were related to the age of the caregiver and were more common in older people(20).
In the present study there was a moderate negative linear correlation between the WHOQOL-BREF scores and those obtained from the Caregiver Burden Scale, demonstrating that the caregivers with a greater burden have a worse quality of life.
A study conducted in the Netherlands evaluated 54 caregivers of children with sickle cell disease and 28 caregivers of a control group with the same socioeconomic status. The TNO-AZL (Adult) Quality of Life questionnaire was used. The results showed that the caregivers had, compared with the normal Dutch population, a lowered quality of life in all domains. Lower quality of life scores were also seen in subscales regarding depressed mood, daily activity and vitality. The authors explain that these differences may be due to the low socioeconomic and educational levels and the high number of single parents, which can bring additional pressure to the caregiver(21).
It is worth noting that, in the present study, 72.97% of sicklecell disease patients took hydroxyurea and that for the caregivers ofthese patients there was significant difference compared to caregiversof patients not taking this medication in respect to general strain,disappointment and environment in the Caregiver Burden Scale.
The difference in burden of caregivers of patients taking hydroxyurea versus those of patients not taking hydroxyurea is related to some aspects of the drug. Among other actions, hydroxyurea increases the mean corpuscular volume (MCV), improves hemoglobin concentration, acts on nitric oxide production and decreases cell adhesion. Hydroxyurea is reserved for moderate to severe manifestations of the disease(22). It is the first drug that has proved to prevent clinical complications(23).
Conclusion
There was no significant difference in quality of life between caregivers of patients with sickle cell disease taking hydroxyurea versus those of patients not taking hydroxyurea in relation to the physical health, psychological health, social relationships, environmental domains and total score of the WHOQOL-BREF instrument.
There was a moderate negative linear correlation between the scores of the WHOQOL-BREF and Caregiver Burden Scales, demonstrating that caregivers with a greater burden have a lower quality of life.
Caregivers of patients taking hydroxyurea had less burden than those caring for patients who did not take this medication in respect to the general strain, disappointment, environment domains and the total score of the Caregiver Burden Scale.
Finally, in the perception of caregivers, caring for sickle cell disease patients is a moderate negative burden.
Acknowledgments
The authors wish to thank the UFMS Teaching Hospital, the Regional Hospital of Campo Grande, MS and the hematologists of these institutions whose information contributed to this study.
Submitted: 2/3/2012
Accepted: 4/26/2012
Conflict-of-interest disclosure: The authors declare no competing financial interest
- 1. Zago MA, Pinto AC. Fisiopatologia das doenças falciformes: da mutação genética à insuficiência de múltiplos órgãos. Rev Bras Hematol Hemoter. 2007;29(3):207-14.
- 2. Ramalho AS, Magna LA, de Paiva-e-Silva RB. [Government Directive MS # 822/01: unique aspects of hemoglobinopathies for public health in Brazil]. Cad Saude Publica. 2003 Jul-Aug;19(4):1195-9. Portuguese.
- 3. Brown BJ, Okereke JO, Lagunju IA, Orimadegun AE, Ohaeri JU, Akinyinka OO. Burden of health-care of carers of children with sickle cell disease in Nigeria. Health Soc Care Community. 2010;18(3):289-95.
- 4. Martins T, Ribeiro JP, Garret C. Estudo de validação do questionário de avaliação da sobrecarga para cuidadores informais. Psicologia, Saúde & Doenças. 2003;4(1):131-48.
- 5. George LK, Gwyther LP. Caregiver well-being: a multidimensional examination of family caregivers of demented adults. Gerontologist. 1986;26(3):253-9.
- 6. Garrido R, Almeida OP. Distúrbios de comportamento em pacientes com demência. Arq Neuropsiquiatr. 1999;57(2B):427-34.
- 7. Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20(6):649-55.
- 8. Costa Neto SB, Araújo TC, Curado MP. Avaliação da qualidade de vida de pessoas portadoras de câncer de cabeça e pescoço. Acta Oncol Bras. 2000;20(3):96-104.
- 9. Loureiro MM. Epidemiologia das internações hospitalares e tratamento farmacológico dos eventos agudos em doenças falciformes [thesis]. Rio de Janeiro: Escola Nacional de Saúde Pública, Fundação Oswaldo Cruz; 2006.130p.
- 10. Stonge M, Lavoie F, Cormier H. Les difficultées perçues par des mères de personnes atteintes de troubles psychotiques face au système de soins professionnels. Sante Ment Que. 1995;20(1):89-117.
- 11. Solomon P, Beck S, Gordon B. Family members perspectives on psychiatric hospitalization and a discharge. Community Ment Health J. 1988;24(2):108-17.
- 12. Medeiros MM, Ferraz MB, Quaresma MR. Cuidadores: as "vítimas ocultas" das doenças crônicas. Rev Bras Reumatol. 1998;38(4):189-92.
- 13. Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Aplicação da versão em português do instrumento abreviado de avaliação de qualidade de vida WHOQOL-BREF. Rev Saude Publica. 2000;34(2):178-83.
- 14. Reis MG, Costa IP. Qualidade de vida relacionada à saúde em pacientes com lúpus eritematoso sistêmico no Centro-Oeste do Brasil. Rev Bras Reumatol 2010;50(4):408-22.
- 15. Anderson TW, Finn JD. The new statistical analysis of data. New York: Springer-Verlag; 1996.
- 16. Camargos AC, Lacerda TT, Viana SO, Pinto LR, Fonseca ML. Avaliação da sobrecarga do cuidador de crianças com paralisia cerebral através da escala Burden Interview. Rev Bras Saúde Mater Infant. 2009;9(1):31-7.
- 17. Lemos ND, Gazzola JM, Ramos LR. Cuidando do paciente com Alzheimer: o impacto da doença no cuidador. Saúde Soc. 2006;15(3):170-9.
- 18. Garrido R, Menezes PR. Impacto em cuidadores de idosos com demência atendidos em um serviço psicogeriátrico. Rev Saude Publica. 2004;38(6):835-41.
- 19. Gil ME, Bertuzzi LD. Desafios para a psicologia no cuidado com o cuidador. Rev Bioética. 2006;14(1):49-59.
- 20. Bonet IU, Gonzalez DB, Comas ML, Roger MR, Perez AM, Mateu CL, et al. Características y calidad de vida de los cuidadores informales de enfermos de sida. Enferm Clin. 2006;16(3):137-43.
- 21. van den Tweell XW, Hatzmann J, Ensink E, van der Lee JH, Peters M, Fijnvandraat K, et al. Quality of life of female caregivers of children with sickle cell disease: a survey. Haematologica. 2008;93(4):588-93.
- 22. Figueiredo MS. Agentes indutores da síntese de hemoglobina fetal. Rev Bras Hematol Hemoter. 2007;29(3):313-5.
- 23. Cançado RD, Lobo C, Ângulo IL, Araujo PI, Jesus JA. Protocolo clínico e diretrizes terapêuticas para uso de hidroxiureia na doença falciforme. Rev Bras Hematol Hemoter. 2009;31(5):361-6.
Corresponding author:
Publication Dates
-
Publication in this collection
06 Sept 2012 -
Date of issue
2012
History
-
Received
03 Feb 2012 -
Accepted
26 Apr 2012