Abstract
OBJECTIVE: This study aimed to verify the association between human leukocyte antigens and the bcr-abl fusion protein resulting from t(9;22)(q34;q11) in chronic leukemia myeloid and acute lymphoblastic leukemia patients. METHODS: Forty-seven bcr-abl positive individuals were evaluated. Typing was performed bymicrolymphocytotoxicity and molecular biological methods (human leukocyte antigens Class I and Class II). A control group was obtained from the data of potential bone marrow donors registered in the Brazilian Bone Marrow Donor Registry (REDOME). RESULTS: Positive associations with HLA-A25 and HLA-B18 were found for the b2a2 transcript, as well as a tendency towards a positive association with HLA-B40 and a negative association with HLA-A68. The b3a2 transcript showed positive associations with HLA-B40 and HLA-DRB1*3. CONCLUSION: The negative association between human leukocyte antigens and the BCR-ABL transcript suggests that binding and presentation of peptides derived from the chimeric protein are effective to increase a cytotoxic T lymphocyte response appropriate for the destruction of leukemic cells.
HLA antigens; Fusion proteins, BCR-ABL; Genetic predisposition to disease; Philadelphia chromosome; Leukemia, myelogenous, chronic, BCR-ABL positive; Precursor cell lymphoblastic leukemia-lymphoma
ORIGINAL ARTICLE
Association of HLA antigens and BCR-ABL transcripts in leukemia patients with the Philadelphia chromosome
Daiana Landenberger de Carvalho; Cristian Dias Barbosa; André Luiz de Carvalho; Sandra Trevisan Beck
Universidade Federal de Santa Maria - UFSM, Santa Maria, RS, Brazil
Corresponding author Corresponding author: Daiana Landenberger de Carvalho Centro de Ciências da Saúde Universidade de Santa Maria - UFSM Prédio 26, Sala 1205 97105900 Santa Maria, RS, Brazil daianinh@yahoo.com.br
ABSTRACT
OBJECTIVE: This study aimed to verify the association between human leukocyte antigens and the bcr-abl fusion protein resulting from t(9;22)(q34;q11) in chronic leukemia myeloid and acute lymphoblastic leukemia patients.
METHODS: Forty-seven bcr-abl positive individuals were evaluated. Typing was performed bymicrolymphocytotoxicity and molecular biological methods (human leukocyte antigens Class I and Class II). A control group was obtained from the data of potential bone marrow donors registered in the Brazilian Bone Marrow Donor Registry (REDOME).
RESULTS: Positive associations with HLA-A25 and HLA-B18 were found for the b2a2 transcript, as well as a tendency towards a positive association with HLA-B40 and a negative association with HLA-A68. The b3a2 transcript showed positive associations with HLA-B40 and HLA-DRB1*3.
CONCLUSION: The negative association between human leukocyte antigens and the BCR-ABL transcript suggests that binding and presentation of peptides derived from the chimeric protein are effective to increase a cytotoxic T lymphocyte response appropriate for the destruction of leukemic cells.
Keywords: HLA antigens; Fusion proteins, BCR-ABL; Genetic predisposition to disease; Philadelphia chromosome;Leukemia, myelogenous, chronic, BCR-ABL positive; Precursor cell lymphoblastic leukemia-lymphoma
Introduction
The immune system directs its adaptive response mainly against foreign molecules bound to proteins on the surface of human cells which are encoded by genes of the major histocompatibility complex (MHC) group. These are considered the most polymorphic genes found in humans. The molecules originated from these genes are proteins called human leukocyte antigens (HLA)(1).
HLA genes involved in immune responses are divided into two classes, Class I and Class II(2). The molecules encoded by these genes (surface glycoproteins) have three portions in common, the cytosol, the transmembrane and the extracellular portion, responsible for the presentation of cytosolic/endogenous peptides to T cells. The Class I region includes HLA-A, -B and -C loci which encode the molecules found on almost all nucleated cells. Class I molecules play an important role in the presentation of viral/endogenous peptides to cytotoxic T cells which are responsible for cell-mediated immunity and the removal of infected and modified cells (eg. tumor cells). The HLA-DR, DQ and DP genes, in the Class II region, codify molecules involved in graft rejection and in the presentation of peptides to receptors of T-helper cells, which produce lymphokines that activate the immune response(3). Studies show that endogenous proteins may also be presented by Class II molecules and recognized by CD4+ T lymphocytes(4). Typically the individual inherits two copies of each gene locus, one from each parent, but with co-dominant expression. Thus, the individual has a total of six HLAClass I and six HLA Class II molecules(1).
Besides the importance in immune response, studies have shown a relationship between HLA in a wide variety of diseases of different etiologies, including autoimmune, infectious, neoplastic and idiopathic diseases(3,5).
Leukemias constitute a special group of severe hematopoietic malignancies; although they have been well studied in morphological, genetic and biological terms, further investigations are still required in relation to their real etiology. Many associations related to the development of leukemia, such as genetic predisposition, and exposure to chemicals and irradiation, have been proven(6). The main types of leukemia are: acute lymphoblastic leukemia (ALL), chronic lymphocytic leukemia (CLL), acute myeloid leukemia (AML), chronic myeloid leukemia (CML) and chronic myelomonocytic leukemia (CMML)(7).
In 95% of CML patients and 15-30% of ALL patients the translocation, t(9;22)(q34;q11), which results in the Philadelphia chromosome, is observed(8). This translocation juxtaposes segment 3' of the c-abl proto-oncogene in chromosome 9 to fragment 5' of the bcr gene in chromosome 22; this is observed by karyotyping(9,10).
Breaks in the c-abl gene generally involve exon 2. Breaks in the bcr gene occur in one of three regions: the major breakpoint cluster region (Mbcr), the minor breakpoint cluster region (mbcr)or the micro-breakpoint cluster region (µbcr). The breakpoints that occur in mbcr involve introns 13 and 14 and exon 13 or 14 join to the abl gene resulting in the e13a2(b2a2) and e14a2(b3a2) fusion transcripts, respectively. These transcripts encode a chimericprotein of 210 ĸD (p210) with tyrosine kinase activity that regulates cell growth(11). This recombinant kinase phosphorylates its target proteins continuously and this is associated with unlimited cell proliferation. Furthermore, the exacerbation of phosphorylation produces changes in the adhesive properties of these cells and induces a decrease in the apoptosis rate. Together these changes lead to the development of CML(12).
The b3a2 and b2a2 fusions account for most CML cases and some ALL cases(9). These breakpoints have different implications for the aggressiveness of disease(12).
Several studies indicate an association between HLA and leukemia. However, the few studies that associated these antigens to proteins resulting from the bcr-abl fusion of the translocation, t(9; 22)(q34, q11), show divergent results(10,13). These differences may be related to the multifactorial nature of leukemias and the great heterogeneity observed in subtypes, especially for CML. Moreover, due to the differences observed in the frequencies of HLA alleles between different populations, some associations can be found in certain population groups and not in others(14). Therefore, it seems to be important to investigate the profile and any possible association between HLA and the resulting proteins from the bcr-abl fusion of t(9; 22)(q34, q11) in patients diagnosed with CML and ALL and treated in the Hematology-Oncology Unit of Hospital Universidade de Santa Maria (HUSM).
Methods
Forty-seven patients diagnosed with Philadelphia-chromosome positive leukemia (44 CML patients and 3 ALLpatients) and the BCR-ABL transcript with known HLA typing were analyzed in the Hematology-Oncology Unit of the HUSM. The data of the CML and ALL patients were analyzed together as they presented the same molecular findings and, according to the present consensus, they correspond to the same pathophysiological process or are even different spectra of the same disease. The patients enrolled in this study are from mixed ethnicities from the state of Rio Grande do Sul, Brazil.
Control Group data were obtained from records of potential bone marrow donors registered by the Brazilian Bone Marrow Donor Registry (REDOME), typified by the Laboratory of Transplant Immunology (LIT) of the Hospital Dom Vicente Scherer, in Porto Alegre, RS, Brazil. This group consists of healthy people of both genders, unrelated to the patients, from different ethnicities, but from the same geographic region as the patients. The size of the Control Group was established based on the number of individuals registered in the system by the LIT in REDOME (approximately 30,000). Based on a calculation with a sampling error of 1.7%, 3006 individuals were randomly selected. A low sampling error was chosen because of the extensive polymorphisms of the HLA system.
The b2a2 and b3a2 transcripts were identified using molecular weight markers. Whole blood or bone marrow aspirate subjected to Ficoll-Paque centrifugation to separate leukocytes was used to typethe BCR-ABL transcript in RNA. Extraction was carried out by themethod described by Chomcynski & Sacchi(15). Total RNA sampleswere converted to cDNA using the SS III RT kit (Invitrogen ®).Each sample was amplified using specific primers for a t(9,22)in agreement with those cited by van Dongen(9). The RT-PCR product was subjected to 2% agarose electrophoresis, stained withethidium bromide, visualized on an ultraviolet transilluminator and documented and analyzed using the Kodak EDAS system.
The patients who took part in the study were typed for HLA-Aand -B by serology or molecular biology. The complement-dependentmicrolymphotoxicity serological technique with monoclonal antibody (Lambda Monoclonal Trays SMT1A72, CA, USA) wasperformed at the Histocompatibility Laboratory of HUSM.
HLA Class I typing was performed by polymerase chain reaction sequence-specific primers (PCR-SSP) or polymerase chain reaction and sequence-specific oligonucleotide probe hybridization (PCR-SSO).
DRB1 gene typing was performed by PCR-SSP and PCR-SSO or sequence-specific oligonucleotide reverse hybridization (SSOr) and sequence-based typing and sequencing (SBT).
The Control Group was HLA typed by PCR-SSO (One Lambda, CA, USA).
To standardize data of the typing using the two techniques (serology and molecular biology), the B60 and B61 splits were classified as B40 and the B62, B63, B71 and B72 splits as B15.
The frequency of HLA alleles (not phenotype frequency) was calculated in two different populations: healthy individuals and CML and ALL patients with the BCR-ABL transcript. The HLA-A, -B and -DRB1 frequencies of the patients were compared with the frequencies of these genes in the healthy population. HLA frequencies were assessed in 21 patients with the b2a2 transcript and 30 patients with the b3a2 transcript.
A total of 6012 HLA were analyzed in the healthy population remembering that each individual has two alleles for each antigen.
Odds Ratio test was used with a 95% confidence interval (95% CI) for statistical analysis. The probability values were considered significant when they were less than 0.05, whereas values greater than 0.05 and less than or equal to 0.09 were considered as atendency for the association with disease; for this the StatisticalAnalysis System program (version 9.3) was employed.
The study was approved by the Research Ethics Committee of the Universidade Federal de Santa Maria (UFSM - CAAE0118.0.243.00008).
Results
Of the 47 patients, 17 had the b2a2 breakpoint, 26 had the b3a2 breakpoint and 4 patients had both breakpoints; thus the 4 latter patients took part in two analyses in relation to HLA.
The results obtained from the analysis of the association between HLA and the transcripts including both positive and negative associations, are listed in Tables 1-4. Antigens that were not found in either population were excluded because of the inability to calculate statistical correlation.
There was a tendency towards a positive association with the HLA-B40 antigen (p-value = 0.062: OR = 2.82). A statistically significant negative association was found between the b2a2 transcript and the HLA-A68 antigen (p-value = 0.011: OR = 0.45) and a positive association with the HLA-A25 (p-value = 0.001: OR = 2.04) and HLA-B18 antigens (p-value = 0.003: OR = 4.12 - Table 1).
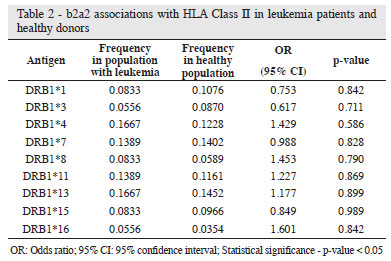
HLA Class II and b2a2 transcript frequency analysis did not show any statistically significant associations (Table 2).
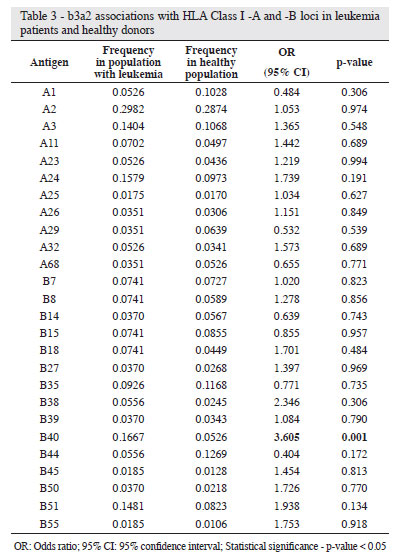
The b3a2 transcript presented a strong positive association (Tables 3 & 4) with HLA-B40 (p-value = 0.001: OR = 3.60) and HLA-DRB1*3 (p-value = 0.001: OR = 1.74), while other associations could not be confirmed by statistical analysis.
Discussion
The association between histocompatibility antigens of the HLA system and disease is well known with studies of CML and ALL demonstrating this association. The presence of the BCR-ABL transcript has been studied in respect to its connection with different HLA. The most frequently encountered fusion transcripts are b2a2 and b3a2.
The study of the relationship between different HLA and the presence of the BCR-ABL transcript suggests a possible role for cytotoxic T cells in the pathogenesis of disease. The individual's ability to develop an effective immune response to destroy tumor cells depends, among other things, on the ability to present this chimeric protein. This capability can be better or worse depending on the HLA inherited by individuals(10). There have been in vitro demonstrations that bcr-abl synthetic peptides are capable of binding to certain HLA Class I molecules inducing response from peptide-specific CD8+ cytotoxic T lymphocytes(16,17). These studies suggest that CD4+ T lymphocytes can distinguish CMLfrom normal cells directly by recognition of the bcr-abl fusion peptide presented by the HLA Class II leukemic cell(18-20).
Individuals with certain HLA alleles which are able to bind to peptides derived from the bcr-abl fusion transcript can be regardedas having a "biological advantage" in the fight against the diseasecompared with individuals without these HLA alleles. A positiveassociation between an HLA and the BCR-ABL transcript suggeststhat this particular allele does not efficiently bind to or presentthe peptides derived from the transcript. On the other hand, anegative association suggests that the binding and the presentationof peptides is effective and the T lymphocyte cytotoxic response,suitable for the destruction of leukemic cells, is increased.
In relation to HLA Class I and II antigens, the presence of the BCR-ABL transcript in leukemia patients seems to be associated to both antigens as either positive or negative associations.
The present study found a positive association between the b2a2 transcript and the HLA-A25 and HLA-B18 antigens, a tendency towards a positive association with the HLA-B40 antigen and a negative association with the HLA-A68 antigen. The b3a2 transcript showed a positive association with the HLA-B40 and DRB1*3 antigens.
Mundhada et al.(10), on studying the North American population, showed the same negative association between the b2a2 transcript and HLA-A68, however, these authors found no association with HLA-B18. They also showed a negative association with HLA-B40 while the current study showed a tendency towards a positive association. Moreover, the study of Mundhada et al.(10) suggested a positive association of HLA-A25 with the b3a2 transcript, different to this study that found a positive association with the b2a2 transcript. Similar associations in relation to HLA Class II molecules were not found.
In Italy, Richiardi et al.(21) could not find any significant difference between the frequencies of the HLA-A and HLA-B alleles in CML patients and the b2a2 and b3a2 breakpoints.
Yasukawa et al.(13) investigated the association between HLA-DRB1 alleles and CML in patients from Kumamoto, Japan with theb2a2 and b3a2 breakpoints. HLA Class II data were analyzed andthere was no correlation different to the current study.
Based on descriptions in the scientific literature, there are still conflicting data regarding the associations between genetic polymorphisms of the HLA system and the BCR-ABL transcript. It is known that there are large differences in HLA allele and haplotype frequencies in different populations worldwide and leukemias are multifactorial diseases so that analyses are complicated.
There is an assumption that the action of cytotoxic Tlymphocytes is dependent and restricted to HLA; this assumes particular importance in the genesis of leukemia with the BCR-ABL transcript.
The negative association of the BCR-ABL transcript with specific HLA suggests that this molecule acts in the presentation of peptides derived from chimeric proteins and stimulates a satisfactory response by T cells, considering the genetic frequency in the studied population.
The different associations found in this study suggest heterogeneity in the immune response linked to HLA.
Studies with greater numbers of patients are necessary to identify other possible associations between the HLA and BCR-ABL transcripts and check the associations found for the Brazilian population. The importance of studies between the HLA system and leukemia is not only to define the predisposition to disease. The stratification of leukemia patients with a BCR-ABL transcript into groups according to HLA typing may indicate a marker for prognosis. With this classification it would be possible to establish adequate therapy according to risk. It is suggested that multicenter studies with larger populations should be carried out to investigate the associations of HLA with the BCR-ABL transcripts and response to therapy with conventional drugs, bone marrow transplant, immunotherapy or combinations.
Acknowledgements
The authors are thankful to Dr. Jorge Neumann for the data on the control group, typified by the Immunology Laboratory of the Hospital Dom Vicente Scherer, in Porto Alegre, RS, Brazil.
Submitted: 2/17/2012
Accepted: 4/27/2012
Conflict-of-interest disclosure: The authors declare no competing financial interest
- 1. FM Brodsky. Apresentação do antígeno e complexo principal de histocompatibilidade. In: Stites DP, Terr AI, Parslow TG. Imunologia médica. Rio de Janeiro: Guanabara Koogan; 2000. p.70.
- 2. Klein J, Sato A. The HLA system. First of two parts. N Engl J Med. 2000;343(10):702-9:
- 3. Donadi EA. Como entender a nomenclatura e os mecanismos de associação entre os antígenos e os alelos de histocompatibilidade com as doenças. Medicina (Ribeirão Preto). 2000;33(1):7-18.
- 4. Yasukawa M, Ohminami H, Kaneko S, Yakushijin Y, Nishimura Y, Inokuchj K, et al. CD4+ cytotoxic T-cell clones specific for bcr-abl b3a2 fusion peptide augment colony formation by chronic myelogenous leukemia cells in a b3a2-specific and HLA-DR restricted manner. Blood. 1998;92(9):3355-61.
- 5. Schlosstein L, Terasaki PI, Bluestone R, Pearson CM. High association of an HL-A antigen, W27,with ankylosing spondylitis. N Engl J Med. 1973;288(14):704-6.
- 6. Yamamoto M, Figueiredo VLP. Epidemiologia da leucemia linfocítica crônica e leucemia linfocítica crônica familiar. Rev Bras Hematol Hemoter. 2005;27(4):229-32.
- 7. Barion LA, Tsuneto LT, Testa GV, Lieber SR, Persoli LB, Marques SB, et al. Associação entre HLA e leucemia em uma população brasileira de etnia mista. Rev Assoc Med Bras. 2007;53(3):252-6.
- 8. Kalidas M, Kantarjian H, Talpaz M. Chronic myelogenous leukemia. JAMA. 2001;286(8):895-8.
- 9. van Dongen JJ, Macintyre EA, Gabert JA, Delabesse E, Rossi V, Saglio G, et al. Standardized RT-PCR analysis of fusion gene transcripts from chromosome aberrations in acute leukemia for detection of minimal residual disease. Report of the BIOMED-1 Concerted Action: investigation of minimal residual disease in acute leukemia. Leukemia. 1999;13(12):1901-28.
- 10. Mundhada S, Luthra R, Cano P. Association of HLA Class I and Class II genes with BCR-ABL transcripts in leukemia patients with t(9;22) (q34;q11). BMC Cancer. 2004;4:25-31.
- 11. Funke VM, Bitencourt H, Vigorito AC, Aranha FJ. Leucemia mieloide crônica e outras doenças mieloproliferativas crônicas. Rev Bras Hematol Hemoter. 2010;32(Supp 1):71-90.
- 12. Sessions J. Chronic myeloid leukemia in 2007. Am J Health Syst Pharm. 2007;64(24 Suppl 15):S4-9.
- 13. Yasukawa M, Ohminami H, Kojima K, Inokuchi K, Nishimura Y, Fujita S. Analysis of HLA-DRB1 alleles in Japanese patients with chronic myelogenous leukemia. Am J Hematol. 2000;63(2):99-101.
- 14. Ghodke Y, Joshi K, Chopra A, Patwardhan B. HLA and disease. Eur J Epidemiol. 2005;20(6):475-88.
- 15. Chomcynski P, Sacchi N. Single step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal biochem. 1987;162(1):156-9.
- 16. Greco G, Fruci D, Accapezzato D, Barnaba V, Nisini R, Ajimena G, et al. Two bcr-abl junction peptides bind HLA-A3 molecules and allow specific induction of human cytotoxic T lymphocytes. Leukemia. 1996;10(4):693-9.
- 17. Buzyn A, Ostankovitch M, Zerbib A, Kemula M, Connan F, Varet B, et al. Peptides derived from the whole sequence of BCR-ABL bind to several Class I molecules allowing specific induction of human cytotoxic T lymphocytes. Eur J Immunol. 1997;27(8):2066-72.
- 18. Takahashi T, Chapman PB, Yang SY, Hara I, Vijayasaradhi S, Houghton AN. Reactivity of autologous CD41 T lymphocytes against human melanoma: Evidence for a shared melanoma antigen presented by HLADR15. J Immunol. 1995;154(2):772-9.
- 19. Oxenius A, Bachmann MF, Mathis D, Benoist C, Zinkemagel RM, Hengartner H. Functional in vivo MHC Class II loading by endogenously synthesized glycoprotein during viral infection. J Immunol. 1997;158(12):5717-26.
- 20. Armstrong TD, Clements VK, Marti BK, Ting JP, Ostrand-Rosenberg S. Major histocompatibility complex Class II-transfected tumor cells present endogenous antigen and are potent inducers of tumor-specific immunity. Proc Natl Acad Sci U S A. 1997;94(13):6886-91.
- 21. Richiardi PM, Tosi R, Martinelli G, Saglio G, Conte R, Barbanti M, et al. The HLA Class I-CML association revisited taking into account the two forms of gene fusions in the Philadelphia chromosome. A multicenter study. Leukemia. 1994;8(12):2134-7.
Corresponding author:
Publication Dates
-
Publication in this collection
06 Sept 2012 -
Date of issue
2012
History
-
Received
17 Feb 2012 -
Accepted
27 Apr 2012