Abstract
BACKGROUND:
At the time of diagnosis, more than 50% of patients with myelodysplastic syndrome have a normal karyotype and are classified as having a favorable prognosis. However, these patients often show very variable clinical outcomes. Furthermore, current diagnostic tools lack the ability to look at genetic factors beyond karyotyping in order to determine the cause of this variability.
OBJECTIVE:
To evaluate the impact of p53 protein expression at diagnosis in patients with low-risk myelodysplastic syndrome.
METHODS:
This study enrolled 38 patients diagnosed with low-risk myelodysplastic syndrome. Clinical data were collected by reviewing medical records, and immunohistochemical p53 staining was performed on bone marrow biopsies.
RESULTS:
Of the 38 participants, 13 (34.21%) showed p53 expression in their bone marrow. At diagnosis, this group of patients also presented clinical features characteristic of a poor prognosis more often than patients who did not express p53. Furthermore, patients expressing p53 had a shorter median survival time compared to those without p53 expression.
CONCLUSION:
This study shows that the expression of p53 at diagnosis is a useful indicator of distinct clinical characteristics and laboratory profiles found in low-risk myelodysplastic syndrome patients. These data indicate that the immunohistochemical analysis of p53 may be a prognostic tool for myelodysplastic syndrome and should be used as an auxiliary test to help determine the best therapeutic choice.
Myelodysplastic syndromes; Tumor suppressor protein p53; Prognosis
Introduction
Myelodysplastic syndrome (MDS) is the general term used to define diseases affecting clonal hematopoietic progenitor cells. Patients with a MDS disease often have ineffective hematopoiesis, cytopenias, blood cell dysplasia (of one or more cell types), and are at high risk for developing acute myeloid leukemia (AML).11. Shih AH, Levine RL. Molecular biology of myelodysplastic syndromes. Semin Oncol. 2011;38:613-20. In order to effectively treat MDS patients, the International Prognostic Scoring System (IPSS) is used as a risk stratification tool and is utilized to estimate patient survival and time until the development of AML. Since its release in 1997, the IPSS has become the standard clinical tool for risk assessment of newly diagnosed MDS patients. Using this tool, patients are stratified based on the percentage of bone marrow blasts, number of cytopenias, and the patient karyotype at diagnosis. These data help to rank the patient into one of four distinct categories: low risk, intermediate risk I, intermediate risk II (intermediate prognosis), and high risk (unfavorable prognosis).22. Greenberg P, Cox C, LeBeau MM, Fenaux P, Morel P, Sanz G, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89:2079-88. , 33. Greenberg PL, Attar E, Bennett JM, Bloomfield CD, De Castro CM, Deeg HJ, et al. NCCN Clinical Practice Guidelines in Oncology: myelodysplastic syndromes. J Natl Compr Canc Netw. 2011;9:30-56.
Although the IPSS is a valuable tool, several limitations have become evident over time including a relative overrepresentation of blast percentage, under-representation of cytogenetic abnormalities, and an underestimation of risk for some patients, particularly those with severe cytopenias or a normal karyotype. A recently published revision of the IPSS, that is the IPSS-R,44. Greenberg PL, Tuechler H, Schanz J, Sanz G, Garcia-Manero G, Solé F, et al. Revised International Prognostic Scoring System for myelodysplastic syndromes. Blood. 2012;120:2454-65. addresses some of these deficiencies. Most importantly, the IPSS-R considers a much larger set of chromosomal abnormalities and better stratifies the prognostic risk associated with them. The revised version also decreases the relative weight of bone marrow blasts, with blast proportions between 2% and 5% being recognized as adverse and considers cytopenias individually, weighing their severity instead of just their presence. Finally, the IPSS-R also assigns patients to one of five risk groups instead of just four, as described in the original IPSS.55. Schanz J, Tüchler H, Solé F, Mallo M, Luño E, Cervera J, et al. New comprehensive cytogenetic scoring system for primary myelodysplastic syndromes (MDS) and oligoblastic acute myeloid leukemia after MDS derived from an international database merge. J Clin Oncol. 2012;30:820-9.
However, the IPSS-R does not address the chromosomal variability observed in MDS patients. At diagnosis, more than 50% of patients with MDS have a normal karyotype and are typically classified as having a more favorable prognosis; however, these patients often show very variable clinical outcomes.66. Haase D, Germing U, Schanz J, Pfeilstöcker M, Nösslinger T, Hildebrandt B, et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core dataset of 2124 patients. Blood. 2007;110:4385-95. Thus, studying other markers is particularly important as it provides information beyond the patient's karyotype, allowing clinicians to better characterize patient prognosis, especially for those with a normal karyotype.11. Shih AH, Levine RL. Molecular biology of myelodysplastic syndromes. Semin Oncol. 2011;38:613-20. For example, the tumor suppressor protein, p53, known for its role in cell cycle arrest, apoptosis, and proliferation associated with malignant tumor progression, has been identified as a key factor in phenotypic variability in a MDS mouse model.77. McGowan KA, Pang WW, Bhardwaj R, Perez MG, Pluvinage JV, Glader BE, et al. Reduced ribosomal protein gene dosage and p53 activation in low-risk myelodysplastic syndrome. Blood. 2011;118:3622-33. The objective of this study was to evaluate the impact of p53 protein expression on the phenotypic characteristics and the risk of progression to AML in patients with low-risk MDS.
Methods
Patients
This study enrolled 38 low-risk adult MDS patients of both genders at a specialized clinic in Fortaleza, Ceará, Brazil. The diagnosis of MDS was performed according to the minimum diagnostic criteria established by the 2006 Conference on MDS held in Vienna.88. Valent P, Horny HP, Bennett JM, Fonatsch C, Germing U, Greenberg P, et al. Definitions and standards in the diagnosis and treatment of the myelodysplastic syndromes: consensus statements and report from a working conference. Leuk Res. 2007;31:727-36. By consensus, the minimal diagnostic criteria include the following: marked and constant peripheral cytopenia (>6 months) of at least one major hematopoietic lineage, MDS-related bone marrow features (i.e. one or more of the following in at least one major hematopoietic lineage: dysplasia = 10%, ring sideroblasts = 15%, or myeloblasts = 5%), or an MDS-related karyotype. Furthermore, all other hematopoietic and non-hematopoietic disorders must be ruled out as the primary reason for the dysplasia and/or cytopenia.
The patient group consisted of nine (23.7%) men and 29 (76.3%) women, with ages ranging from 47 to 95 years and a median age of 61. Patients eligible for this study were classified as having low-risk MDS according to the IPSS-R.66. Haase D, Germing U, Schanz J, Pfeilstöcker M, Nösslinger T, Hildebrandt B, et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core dataset of 2124 patients. Blood. 2007;110:4385-95.
This study was approved by the Ethics Committee of the Universidade Federal do Ceará (UFC), and informed consent was obtained from all patients.
Data collection, sample processing, and clinical follow-up
Clinical data related to age, blood count, and bone marrow biopsy at diagnosis were collected by analyzing the patient's medical records.
Immunohistochemical analysis
Immunohistochemical analysis of p53 was performed according to the procedure described by Kitagawa et al.99. Kitagawa M, Yoshida S, Kuwata T, Tanizawa T, Kamiyama R. p53 expression in myeloid cells of myelodysplastic syndrome. Am J Pathol. 1994;145:338-44. Bone marrow biopsy sections from each patient were decalcified using 10% nitric acid and were paraffin embedded prior to immunohistochemical analysis. Then, the bone marrow sections were deparaffinized, hydrated, and washed with buffered saline (pH 7.0). Antigen retrieval was then performed using a 10 mM citrate buffer (pH 6.0) for 30 min, and the sections were subsequently blocked with two cycles of treatment with a methanol solution containing an endogenous peroxidase and 0.03% hydrogen peroxide for 5 min each. The sections were subsequently incubated with a monoclonal antibody specific for p53 (Clone DO-7; DAKO) for 12 h at 4 °C. The slides were washed with buffered saline and incubated for 1 h with biotinylated IgG antibody after which the sections were again washed with buffered saline and incubated with the ABC complex (DAKO) for 45 min. The ABC complex contains 5 µL of avidin and 5 µL of biotin in 5 mL of buffered saline. To visualize the reaction, the slides were treated with 1 mg/mL diaminobenzidine (DAKO) solution, followed by counter staining with hematoxylin. Cover slips were mounted on slides using Canada balsam. The p53 protein expression was defined as being positive or negative based on the level of nuclear staining. Positive levels were indicated when at least 1% of the hematopoietic cells showed nuclear staining.
Statistical analysis
Results are expressed as means ± standard error. Data analysis was performed using the GraphPad Prism 5.0 statistics program. The Kolmogorov-Smirnov test was used to check for normal distribution of the data, and statistical differences between groups were observed using a t-test or the Mann-Whitney test. A Kaplan-Meier curve was constructed, and the log-rank test was applied to verify statistical differences between the times of combined event-free survival (progression to AML or death). The combined event-free survival was defined as the time interval between date of diagnosis and date of the first negative event (death related to disease progression or progression to AML). The level of significance was set for a p-value < 0.05 in all analyses.
Results
Table 1 shows the clinical characteristics for patients as well as their status for p53 expression at diagnosis. Of the 38 patients who participated in the study, 13 (34.21%) showed p53 protein expression in the nuclei of hematopoietic cells from their bone marrow (Figure 1). Interestingly, p53 expression appears to be correlated with a higher age at diagnosis (66.88 years), while patients who were diagnosed at a younger age (54.78 years) were less likely to express p53 protein (p-value = 0.0341). The hemoglobin level, hematocrit concentration, and white blood cell count were significantly lower in patients with p53 expression (95.41 g/dL, 29.91%, 3.255 × 109/L, respectively) than in patients without p53 expression (11.17 g/dL, 33.86% and 5.236 × 109/L, respectively) (p-value < 0.05).
Strong staining (40%) of the p53 protein in bone marrow (streptavidin-biotin - magnification: 400×).
While some clinical characteristics seemed to correlate with p53 expression, there were no statistically significant differences in p53 expression in relation to gender, MDS duration, or chromosomal aberrations (p-value > 0.05). The mean corpuscular volume (MCV) was also analyzed for each patient, and the mean level found for p53-positive patients was similar to that found for p53-negative patients (p-value > 0.05). Moreover, the IPSS-R classifications for all patients in this study were low or very low and the difference between these two categories showed no significant correlation with the p53 expression. However, using the original IPSS criteria, most patients negative for p53 (92%) were stratified in the low risk category while only 53.8% of patients with p53 expression were included in this category (p-value = 0.011).
At the time of this study, none of the patients were receiving chemotherapy, except for those who progressed to AML during the study. These patients were treated with hypomethylation agents (azacitidine) and/or an immunomodulator (lenalidomide) during disease progression. Only one patient, who was negative for p53, was treated with azacitidine for severe isolated thrombocytopenia. This patient did not progress to AML.
Figure 2 shows p53 expression in relation to reticulin, a marker for fibrosis, and bone marrow iron in the sample. Patients with p53 expression had a higher frequency of more advanced fibrosis levels (II/III) at diagnosis (46.15%), while the patients without p53 expression showed a significantly lower frequency (12%; p-value = 0.041). Furthermore, patients with p53 expression also showed higher bone marrow iron at diagnosis compared to patients without p53 expression (27.3% versus 5.5%, respectively). While this observation was not statistically significant, there was a marked tendency for bone marrow iron to be higher when p53 was expressed.
Influence of the p53 expression on the reticulin and bone marrow iron in myelodysplastic patients at diagnosis.
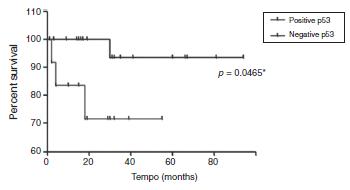
In the group of patients expressing p53, two died and one progressed to AML (progression time: two months). On the other hand, in the group of patients without p53 expression, only one progressed to AML 30 months after diagnosis. The median follow-up time was 31 months after diagnosis, ranging from 9 to 94 months (interquartile range: 16-44.5 months). Analysis of combined, event-free survival (i.e. progression to AML or disease-related death) showed that patients with p53 expression had a significantly lower median survival time compared to patients without p53 expression, 18.5 and 32.5 months, respectively (p-value = 0.046) (Figure 3).
Event-free survival curve of patients with low risk myelodysplastic syndrome and positive or negative for p53.
Discussion
Despite the utility of scoring systems, such as the IPSS, it is difficult to consider all the variables that contribute to the prediction of patient prognosis by using a single test. Other clinical features, such as the presence of comorbidities,1010. Della Porta MG, Malcovati L, Strupp C, Ambaglio I, Kuendgen A, Zipperer E, et al. Risk stratification based on both disease status and extra-hematologic comorbidities in patients with myelodysplastic syndrome. Haematologica. 2011;96:441-9. as well as altered levels of ferritin, ß2-microglobulin, and albumin in the blood1111. Garcia-Manero G, Shan J, Faderl S, Cortes J, Ravandi F, Borthakur G, et al. A prognostic score for patients with low risk myelodysplastic syndrome. Leukemia. 2008;22:538-43. , 1212. Armand P, Kim HT, Cutler CS, Ho VT, Koreth J, Alyea EP, et al. Prognostic impact of elevated pretransplantation serum ferritin in patients undergoing myeloablative stem cell transplantation. Blood. 2007;109:4586-8. , 1313. Komrokji RS, Corrales-Yepez M, Kharfan-Dabaja MA, Al Ali NH, Padron E, Rollison DE, et al. Hypoalbuminemia is an independent prognostic factor for overall survival in myelodysplastic syndromes. Am J Hematol. 2012;87:1006-9. can all have a significant influence on patient health and survival. Furthermore, the most notable element missing from the commonly used prognostic scoring systems is the identification of specific molecular genetic features, particularly mutations of individual genes.
The prognostic significance of some recently described mutations, such as TET2,1414. Smith AE, Mohamedali AM, Kulasekararaj A, Lim Z, Gäken J, Lea NC, et al. Next-generation sequencing of the TET2 gene in 355 MDS and CMML patients reveals low abundance mutant clones with early origins, but indicates no definite prognostic value. Blood. 2010;116:3923-32. EZH2,1515. Ernst T, Chase AJ, Score J, Hidalgo-Curtis CE, Bryant C, Jones AV, et al. Inactivating mutations of the histone methyltransferase gene EZH2 in myeloid disorders. Nat Genet. 2010;42:722-6. SF3B1,1616. Malcovati L, Papaemmanuil E, Bowen DT, Boultwood J, Della Porta MG, Pascutto C, et al. Clinical significance of SF3B1 mutations in myelodysplastic syndromes and myelodysplastic/myeloproliferative neoplasms. Blood. 2011;118:6239-46. IDH1/IDH2,1717. Patnaik MM, Hanson CA, Hodnefield JM, Lasho TL, Finke CM, Knudson RA, et al. Differential prognostic effect of IDH1 versus IDH2 mutations in myelodysplastic syndromes: a Mayo Clinic Study of 277 patients. Leukemia. 2012;26:101-5. and DNMT3A 1818. Walter MJ, Ding L, Shen D, Shao J, Grillot M, McLellan M, et al. Recurrent DNMT3A mutations in patients with myelodysplastic syndromes. Leukemia. 2011;25:1153-8. in MDS remains unclear, but mutations in TP53, the gene encoding the p53 protein, have been consistently associated with the complex karyotypes involved in complete or partial deletion of chromosome 7 (-7/7q-) and chromosome 5 (-5/5q-) and appear to predict poor patient outcome. The tumor suppressor TP53 gene is located on the short arm of chromosome 17, and its p53 protein product has been directly related to cell cycle regulation and apoptosis induction.1919. Zhang XD, Qin ZH, Wang J. The role of p53 in cell metabolism. Acta Pharmacol Sin. 2010;31:1208-12. The active form of p53 has a very short half-life (approximately 6 min), making it extremely difficult to detect. In contrast, mutated or inactive forms of the protein tend to accumulate in the cell nucleus and can be easily detected by immunological methods such as immunohistochemistry.2020. Milner J. Structures and functions of the tumour suppressor p53. Pathol Biol. 1997;45:797-803. Thus, high levels of accumulated p53 protein are associated with mutations in TP53 and, consequently, the stopping of the cell cycle, uncontrolled cell proliferation, and the appearance of additional genetic mutations. Each of these mechanisms could be expected to contribute to the progression of MDS as well as to resistance to therapy.2121. Horiike S, Kita-Sasai Y, Nakao M, Taniwaki M. Configuration of the TP53 gene as an independent prognostic parameter of myelodysplastic syndrome. Leuk Lymphoma. 2003;44:915-22.
Furthermore, mutations in the TP53 gene have frequently been reported in MDS patients with high risk IPSS; however, in groups at lower risk, this correlation has rarely been found.2222. Kulasekararaj AG, Smith AE, Mian SA, Mohamedali AM, Krishnamurthy P, Lea NC, et al. TP53 mutations in myelodysplastic syndrome are strongly correlated with aberrations of chromosome 5, and correlate with adverse prognosis. Br J Haematol. 2013;160:660-72. , 2323. Kita-Sasai Y, Horiike S, Misawa S, Kaneko H, Kobayashi M, Nakao M, et al. International Prognostic Scoring System and TP53 mutations are independent prognostic indicators for patients with myelodysplastic syndrome. Br J Haematol. 2001;115:309-12. , 2424. Iwasaki T, Murakami M, Sugisaki C, Sobue S, Ohashi H, Asano H, et al. Characterization of myelodysplastic syndrome and aplastic anemia by immunostaining of p53 and hemoglobin F and karyotype analysis: differential diagnosis between refractory anemia and aplastic anemia. Pathol Int. 2008;58:353-60. In a study conducted by Jädersten et al.,2525. Jädersten M, Saft L, Smith A, Kulasekararaj A, Pomplun S, Göhring G, et al. TP53 mutations in low-risk myelodysplastic syndromes with del(5q) predict disease progression. J Clin Oncol. 2011;29:1971-9. an association was found between the immunohistochemical expression of p53 and TP53 mutations; this was corroborated by Kulasekararaj et al.2626. Kurotaki H, Tsushima Y, Nagai K, Yagihashi S. Apoptosis, bcl-2 expression and p53 accumulation in myelodysplastic syndrome, myelodysplastic syndrome-derived acute myelogenous leukemia and de novo acute myelogenous leukemia. Acta Haematol. 2000;102:115-23. Moreover, the authors demonstrated that mutations in the TP53gene in patients with MDS, even those classified as low risk, are related to poor treatment response and disease progression. Additionally, these mutations often occur early in the clinical course of the disease, rarely appearing in more advanced cases.2727. Ramos F, Fuertes-Núñez M, Suárez-Vilela D, Fernández-López A. What does apoptosis have to do with clinical features in myelodysplastic syndrome? Haematologica. 2002;87:381-91.
In the present study, the frequency of p53 expression at diagnosis was 34.21%. These patients showed features of poor prognosis, such as more advanced age at diagnosis and lower hemoglobin levels, hematocrit concentrations, and leukocyte counts, as well as advanced levels (II/III) of fibrosis. Furthermore, the incidence of leukemic transformation was significantly higher in patients expressing p53 than those who were p53 negative. Our findings are similar to previous studies indicating that p53 expression can provide prognostic information for MDS patients regarding the development of acute leukemia and survival.99. Kitagawa M, Yoshida S, Kuwata T, Tanizawa T, Kamiyama R. p53 expression in myeloid cells of myelodysplastic syndrome. Am J Pathol. 1994;145:338-44. , 2626. Kurotaki H, Tsushima Y, Nagai K, Yagihashi S. Apoptosis, bcl-2 expression and p53 accumulation in myelodysplastic syndrome, myelodysplastic syndrome-derived acute myelogenous leukemia and de novo acute myelogenous leukemia. Acta Haematol. 2000;102:115-23. , 2727. Ramos F, Fuertes-Núñez M, Suárez-Vilela D, Fernández-López A. What does apoptosis have to do with clinical features in myelodysplastic syndrome? Haematologica. 2002;87:381-91. However, to our knowledge, this is the first study that reports the initial at-diagnosis clinical features and treatments associated with p53 expression of patients with low-risk MDS.
Currently, p53 expression is not considered during MDS prognosis scoring. Although the present study only focused on low-risk patients, p53 expression at diagnosis helped identify distinct clinical and laboratory profiles in this group, indicating that p53 immunohistochemical analysis in MDS patients may be an important prognostic tool and should be considered for auxiliary analysis when determining the therapeutic options for a patient. Furthermore, the previously described immunohistochemical sensitivity of p53 in predicting the presence of TP53 mutations2222. Kulasekararaj AG, Smith AE, Mian SA, Mohamedali AM, Krishnamurthy P, Lea NC, et al. TP53 mutations in myelodysplastic syndrome are strongly correlated with aberrations of chromosome 5, and correlate with adverse prognosis. Br J Haematol. 2013;160:660-72. is encouraging and developing these types of methodologies for routine diagnostic analysis will help advance our understanding of the diseases associated with MDS.
REFERENCES
-
1Shih AH, Levine RL. Molecular biology of myelodysplastic syndromes. Semin Oncol. 2011;38:613-20.
-
2Greenberg P, Cox C, LeBeau MM, Fenaux P, Morel P, Sanz G, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89:2079-88.
-
3Greenberg PL, Attar E, Bennett JM, Bloomfield CD, De Castro CM, Deeg HJ, et al. NCCN Clinical Practice Guidelines in Oncology: myelodysplastic syndromes. J Natl Compr Canc Netw. 2011;9:30-56.
-
4Greenberg PL, Tuechler H, Schanz J, Sanz G, Garcia-Manero G, Solé F, et al. Revised International Prognostic Scoring System for myelodysplastic syndromes. Blood. 2012;120:2454-65.
-
5Schanz J, Tüchler H, Solé F, Mallo M, Luño E, Cervera J, et al. New comprehensive cytogenetic scoring system for primary myelodysplastic syndromes (MDS) and oligoblastic acute myeloid leukemia after MDS derived from an international database merge. J Clin Oncol. 2012;30:820-9.
-
6Haase D, Germing U, Schanz J, Pfeilstöcker M, Nösslinger T, Hildebrandt B, et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core dataset of 2124 patients. Blood. 2007;110:4385-95.
-
7McGowan KA, Pang WW, Bhardwaj R, Perez MG, Pluvinage JV, Glader BE, et al. Reduced ribosomal protein gene dosage and p53 activation in low-risk myelodysplastic syndrome. Blood. 2011;118:3622-33.
-
8Valent P, Horny HP, Bennett JM, Fonatsch C, Germing U, Greenberg P, et al. Definitions and standards in the diagnosis and treatment of the myelodysplastic syndromes: consensus statements and report from a working conference. Leuk Res. 2007;31:727-36.
-
9Kitagawa M, Yoshida S, Kuwata T, Tanizawa T, Kamiyama R. p53 expression in myeloid cells of myelodysplastic syndrome. Am J Pathol. 1994;145:338-44.
-
10Della Porta MG, Malcovati L, Strupp C, Ambaglio I, Kuendgen A, Zipperer E, et al. Risk stratification based on both disease status and extra-hematologic comorbidities in patients with myelodysplastic syndrome. Haematologica. 2011;96:441-9.
-
11Garcia-Manero G, Shan J, Faderl S, Cortes J, Ravandi F, Borthakur G, et al. A prognostic score for patients with low risk myelodysplastic syndrome. Leukemia. 2008;22:538-43.
-
12Armand P, Kim HT, Cutler CS, Ho VT, Koreth J, Alyea EP, et al. Prognostic impact of elevated pretransplantation serum ferritin in patients undergoing myeloablative stem cell transplantation. Blood. 2007;109:4586-8.
-
13Komrokji RS, Corrales-Yepez M, Kharfan-Dabaja MA, Al Ali NH, Padron E, Rollison DE, et al. Hypoalbuminemia is an independent prognostic factor for overall survival in myelodysplastic syndromes. Am J Hematol. 2012;87:1006-9.
-
14Smith AE, Mohamedali AM, Kulasekararaj A, Lim Z, Gäken J, Lea NC, et al. Next-generation sequencing of the TET2 gene in 355 MDS and CMML patients reveals low abundance mutant clones with early origins, but indicates no definite prognostic value. Blood. 2010;116:3923-32.
-
15Ernst T, Chase AJ, Score J, Hidalgo-Curtis CE, Bryant C, Jones AV, et al. Inactivating mutations of the histone methyltransferase gene EZH2 in myeloid disorders. Nat Genet. 2010;42:722-6.
-
16Malcovati L, Papaemmanuil E, Bowen DT, Boultwood J, Della Porta MG, Pascutto C, et al. Clinical significance of SF3B1 mutations in myelodysplastic syndromes and myelodysplastic/myeloproliferative neoplasms. Blood. 2011;118:6239-46.
-
17Patnaik MM, Hanson CA, Hodnefield JM, Lasho TL, Finke CM, Knudson RA, et al. Differential prognostic effect of IDH1 versus IDH2 mutations in myelodysplastic syndromes: a Mayo Clinic Study of 277 patients. Leukemia. 2012;26:101-5.
-
18Walter MJ, Ding L, Shen D, Shao J, Grillot M, McLellan M, et al. Recurrent DNMT3A mutations in patients with myelodysplastic syndromes. Leukemia. 2011;25:1153-8.
-
19Zhang XD, Qin ZH, Wang J. The role of p53 in cell metabolism. Acta Pharmacol Sin. 2010;31:1208-12.
-
20Milner J. Structures and functions of the tumour suppressor p53. Pathol Biol. 1997;45:797-803.
-
21Horiike S, Kita-Sasai Y, Nakao M, Taniwaki M. Configuration of the TP53 gene as an independent prognostic parameter of myelodysplastic syndrome. Leuk Lymphoma. 2003;44:915-22.
-
22Kulasekararaj AG, Smith AE, Mian SA, Mohamedali AM, Krishnamurthy P, Lea NC, et al. TP53 mutations in myelodysplastic syndrome are strongly correlated with aberrations of chromosome 5, and correlate with adverse prognosis. Br J Haematol. 2013;160:660-72.
-
23Kita-Sasai Y, Horiike S, Misawa S, Kaneko H, Kobayashi M, Nakao M, et al. International Prognostic Scoring System and TP53 mutations are independent prognostic indicators for patients with myelodysplastic syndrome. Br J Haematol. 2001;115:309-12.
-
24Iwasaki T, Murakami M, Sugisaki C, Sobue S, Ohashi H, Asano H, et al. Characterization of myelodysplastic syndrome and aplastic anemia by immunostaining of p53 and hemoglobin F and karyotype analysis: differential diagnosis between refractory anemia and aplastic anemia. Pathol Int. 2008;58:353-60.
-
25Jädersten M, Saft L, Smith A, Kulasekararaj A, Pomplun S, Göhring G, et al. TP53 mutations in low-risk myelodysplastic syndromes with del(5q) predict disease progression. J Clin Oncol. 2011;29:1971-9.
-
26Kurotaki H, Tsushima Y, Nagai K, Yagihashi S. Apoptosis, bcl-2 expression and p53 accumulation in myelodysplastic syndrome, myelodysplastic syndrome-derived acute myelogenous leukemia and de novo acute myelogenous leukemia. Acta Haematol. 2000;102:115-23.
-
27Ramos F, Fuertes-Núñez M, Suárez-Vilela D, Fernández-López A. What does apoptosis have to do with clinical features in myelodysplastic syndrome? Haematologica. 2002;87:381-91.
Publication Dates
-
Publication in this collection
May-Jun 2014
History
-
Received
27 Nov 2013 -
Accepted
09 Jan 2014