Abstract
The diagnosis of Multiple Myeloma is a challenge to the physician due to the non-specific symptoms (anemia, bone pain and recurrent infections) that are commonplace in the elderly population. However, early diagnosis is associated with less severe disease, including fewer patients presenting with acute renal injury, pathological fractures and severe anemia. Since 2006, the serum free light chain test Freelite® has been included alongside standard laboratory tests (serum and urine protein electrophoresis, and serum and urine immunofixation) as an aid in the identification of monoclonal proteins, which are a cornerstone for the diagnosis of Multiple Myeloma. The serum free light chain assay recognizes the light chain component of the immunoglobulin in its free form with high sensitivity. Other assays that measure light chains in the free and intact immunoglobulin forms are sensitive, but unfortunately, due to the nomenclature used, these assays (total light chains) are sometimes used in place of the free light chain assay. This paper reviews the available literature comparing the two assays and tries to clarify hypothetical limitations of the total assay to detect Multiple Myeloma. Furthermore, we elaborate on our study comparing the two assays used in 11 Light Chain Multiple Myeloma patients at presentation and 103 patients taken through the course of their disease. The aim of this article is to provide a clear discrimination between the two assays and to provide information to physicians and laboratory technicians so that they can utilize the International Myeloma Working Group guidelines.
Keywords:
Freelite®; Serum free light chain assay; Total light chain assay; Multiple myeloma
Introduction
Monoclonal Gammopathies (MGs) include premalignant Monoclonal Gammopathies of Uncertain Significance (MGUS), Smoldering/Indolent Multiple Myeloma and malignant [Solitary Plasmocytoma, Multiple Myeloma (MM), Light Chain Amyloidosis or Waldenstrom's Macroglobulinemia (WM)] conditions. These disorders are commonly characterized by the production of monoclonal proteins which may be either intact immunoglobulins (M-Ig), serum free light chains (sFLC), a combination of both, or rarely, free heavy chains only.11 Gertz MA. Immunoglobulin light chain amyloidosis: 2014 update on diagnosis, prognosis, and treatment. Am J Hematol. 2014;89(12):1133-40.,22 Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33. A low percentage of these disorders present without the production of any monoclonal protein.
The asymptomatic disorders are identified through routine laboratory investigations, whilst the diagnosis of the symptomatic disorders can present considerable difficulties to the physician as the symptoms (anemia, recurrent infections, fatigue and bone pain) are common in elderly populations and are not specific to the disease.33 Bridgen ML, Webber D. Clinical Pathology Rounds: the case of the anaplastic carcinoma that was not - potential problems in the interpretation of monoclonal proteins. Lab Med. 2000;31(12):661-5.–55 Chaves Lameiro P, Lazaro de la Osa J, Gonzalez J. Difficulties identifying a monoclonal component in a Bence-Jones multiple myeloma, a clinical case. Biochim Clin. 2013;37:W249a. However, there is a need for timely diagnosis as delays can lead to an increased severity of the disease, including acute renal failure and pathological fractures, which can result in a shorter overall survival.66 Tsakiris DJ, Stel VS, Finne P Fraser E, Heaf J, de Meester J, et al. Incidence and outcome of patients starting renal replacement therapy for end-stage renal disease due to multiple myeloma or light-chain deposit disease: an ERA-EDTA Registry study Nephrol Dial Transplant. 2010;25(4):1200-6.
Immunoglobulin structure and sequence variation
Immunoglobulins are the soluble, secreted form of the B-cell receptor and are composed of repeating mirror images comprising two identical heavy chains (gamma – γ, alpha – α, mu – µ, delta – δ or epsilon – ɛ) and two identical light chains (kappa – κ or lambda – λ). Immunoglobulin heavy and light chains each have constant and variable regions. A pair of heavy and light chain variable regions together forms the antigen-binding site. The variable regions exhibit enormous structural diversity, particularly of antigen-binding contacts, allowing the recognition of a huge variety of antigens.
In humans, it is calculated that there are at least 1011 possible antibody structural variants, which allows for the recognition of a vast number of different antigens.77 Janeway CA Jr, Travers P, Walport M. The generation of diversity in immunoglobulins. Immunobiology: the immune system in health and disease. New York: Garland Science; 2001. The diversity is generated in four main ways.
Firstly, different combinations of gene segments are used in the rearrangement of heavy and light chain genes during early B-cell development. Kappa light chains are constructed from one of approximately 40 functional variable (Vκ) gene segments, one of 5 joining (Jκ) gene segments and a single constant (Cκ) gene. Lambda light chains are constructed from one of approximately 30 variable (Vλ) gene segments, and one of four (or more) pairs of functional joining (Jλ) gene segments and constant (Cλ) genes.77 Janeway CA Jr, Travers P, Walport M. The generation of diversity in immunoglobulins. Immunobiology: the immune system in health and disease. New York: Garland Science; 2001. The heavy chain variable region is formed from one of around 60 variable (VH), one of 30 diversity (DH), and one of six joining (JH) gene segments.77 Janeway CA Jr, Travers P, Walport M. The generation of diversity in immunoglobulins. Immunobiology: the immune system in health and disease. New York: Garland Science; 2001. This combinational diversity accounts for a substantial amount of variable region diversity. Secondly, diversity arises from the addition or removal of nucleotides at the junctions between V (D) and J gene segments during recombination. A third source of diversity arises from the many different combinations of heavy and light chains, and finally, somatic hypermutation introduces point mutations in the variable region genes of light and heavy chains in mature activated B-cells.77 Janeway CA Jr, Travers P, Walport M. The generation of diversity in immunoglobulins. Immunobiology: the immune system in health and disease. New York: Garland Science; 2001.
In light chains, variations are also found in a region of the variable domain corresponding to the first 23 amino acids of the first framework region (a region not associated with antigen binding). Using monoclonal antibodies, four κ (Vκ I − Vκ IV) and six λ subgroups (Vλ I − Vλ VI) have been identified.88 Solomon A. Light chains of human immunoglobulins. Methods Enzymol. 1985;116:101-21.
Such diversity is best identified using polyclonal antibodies that can recognize an extensive range of different epitopes.
Introduction to Freelite®
Freelite® (The Binding Site, UK) is the only nephelometric/turbidimetric assay cleared by the Food and Drug Administration (FDA) of the United States of America for the measurement of serum FLC (sFLC). It uses polyclonal antibodies produced in sheep that specifically recognize and quantify the kappa (κ) and lambda (λ) sFLC separately, enabling calculation of the kappa/lambda sFLC ratio (rFLC) which can be used to determine clonality.99 Palladini G, Russo P, Bosoni T, Verga L, Sarais G, Lavatelli F, et al. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine. Clin Chem. 2009;55(3):499-504.,1010 Bakshi NA, Gulbranson R, Garstka D, Bradwell AR, Keren DF. Serum free light chain (FLC) measurement can aid capillary zone electrophoresis in detecting subtle FLC-producing M proteins. Am J Clin Pathol. 2005;124(2):214-8. The antibodies specifically recognize epitopes present in the constant region of the light chains, which are hidden when joined to a heavy chain partner (i.e. in the form of the intact immunoglobulin) but are exposed when the light chains are in their free form (Figure 1). The sensitivity of assays has allowed quantification of normal circulating sFLC concentrations for the first time [Reference intervals: κ – median 7.3 mg/L (95th percentile: 3.3–19.4 mg/L); λ – median 12.4 mg/L (95th percentile: 5.7–26.3 mg/L); rFLC is 0.26–1.65].1010 Bakshi NA, Gulbranson R, Garstka D, Bradwell AR, Keren DF. Serum free light chain (FLC) measurement can aid capillary zone electrophoresis in detecting subtle FLC-producing M proteins. Am J Clin Pathol. 2005;124(2):214-8.,1111 Katzmann JA, Clark RJ, Abraham RS, Bryant S, Lymp JF, Bradwell AR, et al. Serum reference intervals and diagnostic ranges for free kappa and free lambda immunoglobulin light chains: relative sensitivity for detection of monoclonal light chains. Clin Chem. 2002;48(9):1437-44. The majority of results of plasma cell dyscrasias show increased production of either the κ or λ sFLC. Individuals who have rFLC values >1.65 may have a monoclonal κ sFLC and those with rFLC values <0.26 may have a monoclonal λ FLC.1212 Abadie JM, Bankson DD. Assessment of serum free light chain assays for plasma cell disorder screening in a Veterans Affairs population. Ann Clin Lab Sci. 2006;36(2):157-62. The applicability of the rFLC in the clinical practice has been proven by a number of scientific publications which led to its inclusion in different international guidelines.1313 Dispenzieri A, Kyle R, Merlini G, Miguel JS, Ludwig H, Hajek R, et al. International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia. 2009;23(2):215-24.
A diagram of intact immunoglobulin showing the structure of the heavy and light chains. Diagram of the kappa (κ) and lambda (λ) free light chains (FLC) showing the different domains of the light chains and the antibody target that are recognized by the serum free light chain assay.
Current techniques used for the detection of monoclonal proteins
Serum protein electrophoresis (SPEP) is routinely used to identify and quantify intact M-Ig, with immunofixation used to classify according to the heavy chain (γ, α, µ, δ and ɛ) and light chain (κ or λ) isotypes.88 Solomon A. Light chains of human immunoglobulins. Methods Enzymol. 1985;116:101-21. Whilst this technique is adequate for most, grossly elevated intact M-Igs, sensitivity can be limited due to co-migration and at low serum concentrations. Furthermore, SPEP poorly identifies sFLC1414 Katzmann JA, Snyder MR, Rajkumar SV, Kyle RA, Therneau TM, Benson JT, et al. Long-term biologic variation of serum protein electrophoresis M-spike, urine M-spike, and monoclonal serum free light chain quantification: implications for monitoring monoclonal gammopathies. Clin Chem. 2011;57(12):1687-92. meaning the assay is inadequate for the detection and quantitation of paraproteins produced in light chain MM or Amyloidosis.1515 Abraham RS, Clark RJ, Bryant SC, Lymp JF, Larson T, Kyle RA, et al. Correlation of serum immunoglobulin free light chain quantification with urinary Bence Jones protein in light chain myeloma. Clin Chem. 2002;48(4):655-7. Historically, 24-hour urine collection has been recommended for the detection of immunoglobulin free light chains, however there is often poor compliance1616 Fidler CJ, Hussein AK, Gandhi N, Karur V,Sharma M, Klumpp TR, et al. Evaluating trends in diagnostic and prognostic testing for multiple myeloma. Blood. 2011;118:2067.–1818 Beetham R, Wassell J, Wallage MJ, Whiteway AJ, James JA. Can serum free light chains replace urine electrophoresis in the detection of monoclonal gammopathies? Ann Clin Biochem. 2007;44 Pt 6:516-22. and renal function can heavily influence the accuracy of the results.1919 Nowrousian MR, Brandhorst D, Sammet C, Kellert M, Daniels R, Schuett P, et al. Serum free light chain analysis and urine immunofixation electrophoresis in patients with multiple myeloma. Clin Cancer Res. 2005;11 24 (Pt 1):8706-14.
Differences between free light chain and total light chain assays (hypothetical)
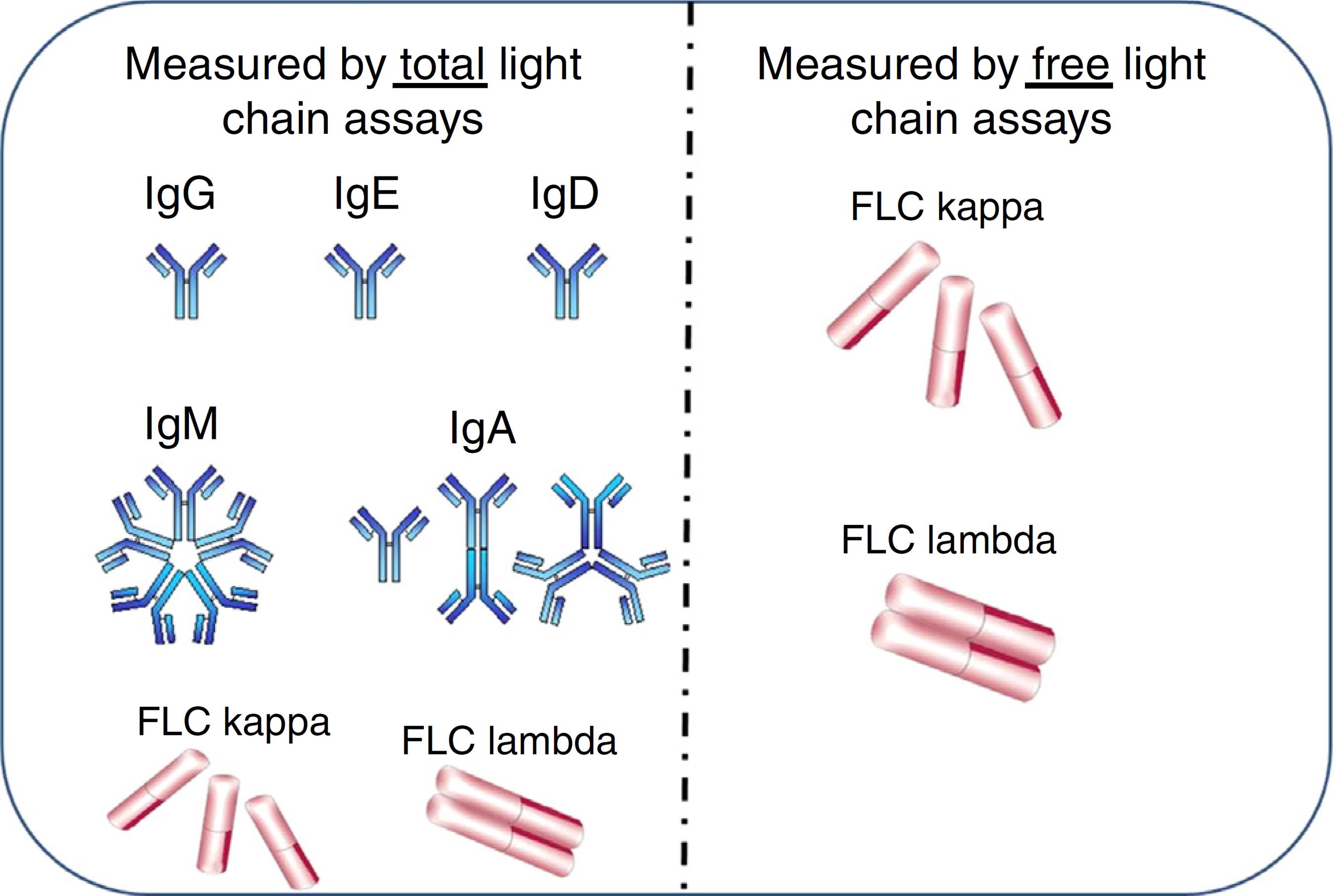
The use of the Freelite assays in the diagnosis of MGs has been well established.1313 Dispenzieri A, Kyle R, Merlini G, Miguel JS, Ludwig H, Hajek R, et al. International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia. 2009;23(2):215-24. However there is often confusion between Freelite and similarly named assays which determine the total light chain concentration in serum and urine. The total light chain assay measures the concentration of all antibodies and free light chains of a particular light chain class i.e. IgG-κ + IgA-κ + IgM-κ + IgD-κ + IgE-κ + free κ. Freelite measures only the free form of the light chain (free κ in our example – Figure 2). Due to the difference in specificity of the assays, total light chain assays identify the light chain component of intact immunoglobulins and free light chains in serum whereas Freelite recognizes only the free light chain component. Therefore, there is a large difference in sensitivity (Table 1) between the two assays. The presence of a polyclonal background prevents the total immunoglobulin assay from being able to distinguish clonality at <4 g/L, whereas the Freelite assay can detect clonality at mg/L concentrations.
Measurement of kappa (κ) and lambda (λ) light chains in free and total assays. Total light chain assays measure light chains when bound to heavy chains in intact immunoglobulins plus free light chains (FLC). The free light chain assay measures only free light chains.
Reference intervals and lower limits of sensitivity of free light chain assays and total light chain assays in serum.
Differences between the Freelite and total light chain assays (data)
Recently, Hungria et al.2020 Hungria VT, Kampanis P, Drayson MT, Plant T, Crusoe EQ, Peres AL, et al. Comparison of kappa and lambda Freelite to total kappa and lambda immunoassays for the detection of monoclonal gammopathies, both as standalone tests and alongside serum protein electrophoresis. Blood. 2014;124(21):5705. published a study comparing the sensitivity of the sFLC assays to the total light chain assays for samples obtained from 114 light chain MM (LCMM) patients taken through the course of their disease. In keeping with previous reports1515 Abraham RS, Clark RJ, Bryant SC, Lymp JF, Larson T, Kyle RA, et al. Correlation of serum immunoglobulin free light chain quantification with urinary Bence Jones protein in light chain myeloma. Clin Chem. 2002;48(4):655-7.,1919 Nowrousian MR, Brandhorst D, Sammet C, Kellert M, Daniels R, Schuett P, et al. Serum free light chain analysis and urine immunofixation electrophoresis in patients with multiple myeloma. Clin Cancer Res. 2005;11 24 (Pt 1):8706-14.,2121 Bradwell AR, Carr-Smith HD, Mead GP, Harvey TC, Drayson MT. Serum test for assessment of patients with Bence Jones myeloma. Lancet. 2003;361(9356):489-91.–3434 Wolff F, Thiry C, Willems D. Assessment of the analytical performance and the sensitivity of serum free light chains immunoassay in patients with monoclonal gammopathy. Clin Biochem. 2007;40(5-6):351-4. the FLC identified clonality in 11/11 samples at presentation and identified persistent disease in 80/103 samples taken throughout the course of the disease. In contrast, the total light chain assay identified only 2/11 samples at presentation and 25/103 samples taken throughout the course of the disease. Somewhat confusingly, the light chain isotype was misreported in 11 samples as the opposite light chain.
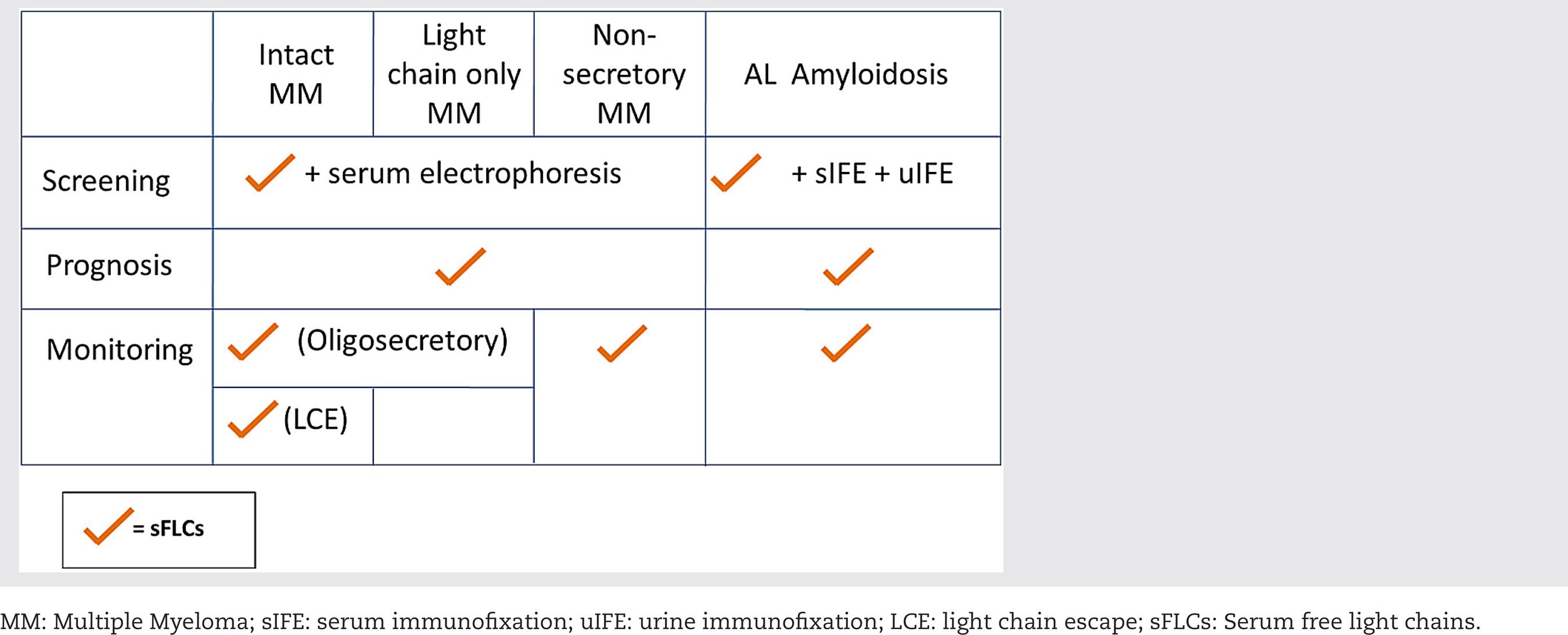
The International Myeloma Working Group (IMWG) guidelines for the identification of monoclonal immunoglobulins at presentation recommend an algorithm of Freelite + SPEP (Table 2). Hungria et al. showed that, in this study, 11/11 patients were identified using the Freelite assay and there was no need for SPEP. In contrast, total light chain + SPEP identified only 8/11 samples, clearly highlighting the lack of sensitivity of this algorithm recommended by the IMWG guidelines (Figure 3).
Scatter charts showing the differences in sensitivity between the Freelite® and total light chain assays for light chain myeloma patients taken at presentation ( n = 11) and through the course of their disease ( n = 103) compared to a 100 percentile normal range indicated by parallel lines. FLC: free light chain; SPE: serum protein electrophoresis; PPV: positive predictive value; NPV: negative predictive value.
The sensitivity of total κ/λ and sFLC assays were compared in a study by Marien et al.3535 Marie G, Oris E, Bradwell AR, Blanckaert N, Bossuyt X. Detection of monoclonal proteins in sera by capillary zone electrophoresis and free light chain measurements. Clin Chem. 2002;48(9):1600-1. Sixteen serum samples from LCMM patients were investigated. Total κ and λ concentrations were measured using Beckman-Coulter reagents on the IMMAGE® nephelometer and sFLC concentrations were measured by Freelite assays (The Binding Site). All samples were abnormal by sFLC assays compared to only five of the 16 samples by total κ and λ assays. In addition, one λ patient was mistyped as κ by the total light chain assay. Other studies have confirmed that total light chain assays are less sensitive than sFLC analysis for the diagnosis of LCMM, Non-secretory MM and Amyloidosis.3636 Cavalcanti E, Barchiesi Y Cuomo M, Di Paola F Morabito F, Cavalcanti S. A particular case of lambda chain multiple myeloma. Biochim Clin. 2013;37:428-30.–3838 Smith LJ, Mead GP, Bradwell AR. Comparative sensitivity of serum and urine assays for free light chains. Clin Chem Lab Med. 2003:41.
Summary of the importance of the serum free light chain assay screening
The IMWG concluded that, for the purpose of screening for all MGs (with the exception of Amyloidosis), Freelite can replace 24-hour urine assessments.1313 Dispenzieri A, Kyle R, Merlini G, Miguel JS, Ludwig H, Hajek R, et al. International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia. 2009;23(2):215-24. Furthermore, Katzmann et al.3939 Katzmann JA, Abraham RS, Dispenzieri A, Lust JA, Kyle RA. Diagnostic performance of quantitative kappa and lambda free light chain assays in clinical practice. Clin Chem. 2005;51(5):878-81. concluded that Freelite costs approximately half as much as 24-hour urine assessment based upon Medicare, USA 2006 reimbursement values.
Recently the IMWG updated the definition of MM to include additional, validated biomarkers alongside CRAB (hypercalcemia, renal failure, anemia, and bone lesions) assessments. A rFLC ≥100, with an involved free light chain concentration of >100 mg/L was included in this validated biomarker list.4040 Rajkumar SV, Dimopolous MA, Palumbo A, Blade J, Merlini G, Mateos MV, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-48.
Hematological response
International guidelines have included Freelite assessments as the most effective monitoring tool in patients with Amyloidosis.4141 Gertz MA, Comenzo R, Falk RH, Fermand JP, Hazenberg BP, Hawkins PN, et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): a consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18-22 April 2004. Am J Hematol. 2005;79(4):319-28.,4242 Bird JM, Cavenagh J, Samson D, Mehta A, Hawkins P, Lachmann H. Guidelines on the diagnosis and management of AL amyloidosis. Br J Haematol. 2004;125(6): 681-700. More recently, new response criteria were defined based upon changes in Freelite values during treatment.4343 Palladini G, Dispenzieri A, Gertz MA, Kumar S, Wechalekar A, Hawkins PN, et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes. J Clin Oncol. 2012;30(36):4541-9. The response criteria utilized the rFLC and the difference between involved and uninvolved free light chains (dFLC); importantly the depth of the assigned response correlated to overall survival.
The IMWG recommend Freelite as the only available and reliable method for the determination of response in patients with Non-secretory and Oligosecretory MM.1313 Dispenzieri A, Kyle R, Merlini G, Miguel JS, Ludwig H, Hajek R, et al. International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia. 2009;23(2):215-24. More recently in LCMM, comparisons of response assessment as determined by 24-hour urine evaluation and Freelite have suggested that Freelite is far superior to the 24-hour urine exam as a tool to measure patient response (Table 2).4444 Corre J, Dejoie T, Caillon H, Attal M, Avet-Loiseau H, Moreau P. Serum free light chains should be the target of response evaluation in light chain multiple myeloma rather than urines: results from the IFM/DFCI 2009 trial. Blood. 2014;124:180a.
In all MM patients, normalization of the Freelite ratio corresponds to superior outcome independently of overall response.4545 Moustafa MA, Rajkumar SV, Dispenzieri A, Gertz MA, Lacy MQ, Buadi FK, et al. Utility of serum free light chain measurements in multiple myeloma patients not achieving complete response to therapy Leukemia. 2015;29(10):2033-8. The IMWG have refined the definition of complete response, (i) negative immunofixation in serum and urine, (ii) disappearance of plasmacytomas, and (iii) bone marrow infiltration of plasma cells below 5%, to include a normal Freelite ratio.4646 Durie BG, Harousseau JL, Miguel JS, Blade J, Barlogie B, Anderson K, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20:1467-73. The new response definition, stringent complete response (sCR) relies on a normal Freelite ratio and negative plasma cell evaluation, and corresponds to an improved overall survival.4747 Kapoor P, Kumar S, Dispenzieri A, Lacy M, Dingli D, Hayman SR, et al. Survival outcomes of patients with multiple myeloma (MM) achieving stringent complete response (sCR) following upfront autologous stem cell transplantation (SCT). J Clin Oncol. 2011;29 Suppl.:8069 [abstract].
Conclusions
Early detection of patients with MM is key to a reduction in comorbidities that can impact the quality and duration of life. The sFLC assay, but not the total light chain assay, is an important part of the routine laboratory test algorithm that contributes to the identification of patients with MGs, including MM. To date, there are two pivotal studies that highlight the limited utility of the total light chain assay in the detection of MGs. In the study presented by Hungria et al., the addition of total light chain to SPEP failed to identify all LCMM patients, highlighting an important insensitivity when utilizing this assay. Similar results were reported by Marien et al. The assays can be easily distinguished based upon their normal ranges and caution is urged to utilize the sFLC assay, but not the total light chain assay for the screening, diagnosis and hematological responses in MGs.
Acknowledgments
The authors are thankful to The Binding Site UK, University of Birmingham, UK and Fundação Hemocentro da Santa Casa de São Paulo, SP for their support.
REFERENCES
-
1Gertz MA. Immunoglobulin light chain amyloidosis: 2014 update on diagnosis, prognosis, and treatment. Am J Hematol. 2014;89(12):1133-40.
-
2Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33.
-
3Bridgen ML, Webber D. Clinical Pathology Rounds: the case of the anaplastic carcinoma that was not - potential problems in the interpretation of monoclonal proteins. Lab Med. 2000;31(12):661-5.
-
4van Zaanen HC, Diderich PP, Pegels JG, Ruizeveld de Winter JA. Renal insufficiency due to light chain multiple myeloma. Ned Tijdschr Geneeskd. 2000;144(45):2133-7.
-
5Chaves Lameiro P, Lazaro de la Osa J, Gonzalez J. Difficulties identifying a monoclonal component in a Bence-Jones multiple myeloma, a clinical case. Biochim Clin. 2013;37:W249a.
-
6Tsakiris DJ, Stel VS, Finne P Fraser E, Heaf J, de Meester J, et al. Incidence and outcome of patients starting renal replacement therapy for end-stage renal disease due to multiple myeloma or light-chain deposit disease: an ERA-EDTA Registry study Nephrol Dial Transplant. 2010;25(4):1200-6.
-
7Janeway CA Jr, Travers P, Walport M. The generation of diversity in immunoglobulins. Immunobiology: the immune system in health and disease. New York: Garland Science; 2001.
-
8Solomon A. Light chains of human immunoglobulins. Methods Enzymol. 1985;116:101-21.
-
9Palladini G, Russo P, Bosoni T, Verga L, Sarais G, Lavatelli F, et al. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine. Clin Chem. 2009;55(3):499-504.
-
10Bakshi NA, Gulbranson R, Garstka D, Bradwell AR, Keren DF. Serum free light chain (FLC) measurement can aid capillary zone electrophoresis in detecting subtle FLC-producing M proteins. Am J Clin Pathol. 2005;124(2):214-8.
-
11Katzmann JA, Clark RJ, Abraham RS, Bryant S, Lymp JF, Bradwell AR, et al. Serum reference intervals and diagnostic ranges for free kappa and free lambda immunoglobulin light chains: relative sensitivity for detection of monoclonal light chains. Clin Chem. 2002;48(9):1437-44.
-
12Abadie JM, Bankson DD. Assessment of serum free light chain assays for plasma cell disorder screening in a Veterans Affairs population. Ann Clin Lab Sci. 2006;36(2):157-62.
-
13Dispenzieri A, Kyle R, Merlini G, Miguel JS, Ludwig H, Hajek R, et al. International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia. 2009;23(2):215-24.
-
14Katzmann JA, Snyder MR, Rajkumar SV, Kyle RA, Therneau TM, Benson JT, et al. Long-term biologic variation of serum protein electrophoresis M-spike, urine M-spike, and monoclonal serum free light chain quantification: implications for monitoring monoclonal gammopathies. Clin Chem. 2011;57(12):1687-92.
-
15Abraham RS, Clark RJ, Bryant SC, Lymp JF, Larson T, Kyle RA, et al. Correlation of serum immunoglobulin free light chain quantification with urinary Bence Jones protein in light chain myeloma. Clin Chem. 2002;48(4):655-7.
-
16Fidler CJ, Hussein AK, Gandhi N, Karur V,Sharma M, Klumpp TR, et al. Evaluating trends in diagnostic and prognostic testing for multiple myeloma. Blood. 2011;118:2067.
-
17Robson EJ, Taylor J, Beardsmore C, Basu S, Mead G, LovattT. Utility of serum free light chain analysis when screening for lymphoproliferative disorders. Lab Med. 2009;40(6):325-9.
-
18Beetham R, Wassell J, Wallage MJ, Whiteway AJ, James JA. Can serum free light chains replace urine electrophoresis in the detection of monoclonal gammopathies? Ann Clin Biochem. 2007;44 Pt 6:516-22.
-
19Nowrousian MR, Brandhorst D, Sammet C, Kellert M, Daniels R, Schuett P, et al. Serum free light chain analysis and urine immunofixation electrophoresis in patients with multiple myeloma. Clin Cancer Res. 2005;11 24 (Pt 1):8706-14.
-
20Hungria VT, Kampanis P, Drayson MT, Plant T, Crusoe EQ, Peres AL, et al. Comparison of kappa and lambda Freelite to total kappa and lambda immunoassays for the detection of monoclonal gammopathies, both as standalone tests and alongside serum protein electrophoresis. Blood. 2014;124(21):5705.
-
21Bradwell AR, Carr-Smith HD, Mead GP, Harvey TC, Drayson MT. Serum test for assessment of patients with Bence Jones myeloma. Lancet. 2003;361(9356):489-91.
-
22Drayson MT, Morgan GJ, Jackson GH, Davies FE, Owen RG, Ross FM, et al. Prospective study of serum FLC and other M-protein assays: when and how to measure response? Clin Lymphoma Myeloma. 2009;9 Suppl. 1:S56.
-
23van Rhee F, Bolejack V,Hollmig K, Pineda-Roman M, Anaissie E, Epstein J, et al. High serum-free light chain levels and their rapid reduction in response to therapy define an aggressive multiple myeloma subtype with poor prognosis. Blood. 2007;110(3):827-32.
-
24Kraj M, Kruk B, Poglod R, Szczepinski A. Correlation of serum free light chain quantification with serum and urine immunofixation in monoclonal gammopathies. Haematologica. 2011;96:0861a.
-
25Avet Loiseau H, Mirbahai L, Young P, Mathiot C, Attal M, Moreau P et al. Nephelometric measurements of kFLC and \FLC for monitoring light chain multiple myeloma patients. Lymphoma Myeloma. 2011.
-
26Avet-Loiseau H, Young P, Mathiot C, Attal M, Harousseau J, Bradwell AR, et al. Nephelometric measurements of kFLC and \FLC for monitoring light myeloma patients. Haematologica. 2011;96:0853a.
-
27Kang SY, Suh JT, Lee HJ, Yoon HJ, Lee WI. Clinical usefulness of free light chain concentration as a tumor marker in multiple myeloma. Ann Hematol. 2005;84(9):588-93.
-
28Schneider N, Wynckel A, Kolb B, Sablon E, Gillery P Maquart FX. Comparative analysis of immunoglobulin free light chains quantification by Freelite (The Binding Site) and N Latex FLC (Siemens) methods. Ann Biol Clin (Paris). 2013;71(1): 13-9.
-
29Hutchison CA, Plant T, Drayson M, Cockwell P, Kountouri M, Basnayake K, et al. Serum free light chain measurement aids the diagnosis of myeloma in patients with severe renal failure. BMC Nephrol. 2008;9:11.
-
30Mosbauer U, Ayuk F, Schieder H, Lioznov M, Zander AR, Kroger N. Monitoring serum free light chains in patients with multiple myeloma who achieved negative immunofixation after allogeneic stem cell transplantation. Haematologica. 2007;92(2):275-6.
-
31Piehler AP, Gulbrandsen N, Kierulf P,Urdal P.Quantitation of serum free light chains in combination with protein electrophoresis and clinical information for diagnosing multiple myeloma in a general hospital population Clin Chem. 2008;54(11):1823-30.
-
32Harding SJ, Mead GP, Bradwell AR, Berard AM. Serum free light chain immunoassay as an adjunct to serum protein electrophoresis and immunofixation electrophoresis in the detection of multiple myeloma and other B-cell malignancies. Clin Chem Lab Med 2009;47(3):302-4.
-
33Giarin MM, Giaccone L, Caracciolo D, Bruno B, Falco P, Omede P et al. Serum free light chains (SFLC) assay: a suggestive new criteria for evaluating disease response, progression and relapse in plasma-cell disorders (PD) and a prognostic factor in monoclonal gammopathy of undetermined significance (MGUS). Haematologica. 2006;91:PO151a.
-
34Wolff F, Thiry C, Willems D. Assessment of the analytical performance and the sensitivity of serum free light chains immunoassay in patients with monoclonal gammopathy. Clin Biochem. 2007;40(5-6):351-4.
-
35Marie G, Oris E, Bradwell AR, Blanckaert N, Bossuyt X. Detection of monoclonal proteins in sera by capillary zone electrophoresis and free light chain measurements. Clin Chem. 2002;48(9):1600-1.
-
36Cavalcanti E, Barchiesi Y Cuomo M, Di Paola F Morabito F, Cavalcanti S. A particular case of lambda chain multiple myeloma. Biochim Clin. 2013;37:428-30.
-
37Chen HF, Hou J, Yuan ZG, Wang DX, Fu WJ, Chen YB. Detection of serum free light chain and its clinical significance in nonsecretory multiple myeloma. Zhonghua Xue Ye Xue Za Zhi. 2008;29(2):113-6.
-
38Smith LJ, Mead GP, Bradwell AR. Comparative sensitivity of serum and urine assays for free light chains. Clin Chem Lab Med. 2003:41.
-
39Katzmann JA, Abraham RS, Dispenzieri A, Lust JA, Kyle RA. Diagnostic performance of quantitative kappa and lambda free light chain assays in clinical practice. Clin Chem. 2005;51(5):878-81.
-
40Rajkumar SV, Dimopolous MA, Palumbo A, Blade J, Merlini G, Mateos MV, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-48.
-
41Gertz MA, Comenzo R, Falk RH, Fermand JP, Hazenberg BP, Hawkins PN, et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): a consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18-22 April 2004. Am J Hematol. 2005;79(4):319-28.
-
42Bird JM, Cavenagh J, Samson D, Mehta A, Hawkins P, Lachmann H. Guidelines on the diagnosis and management of AL amyloidosis. Br J Haematol. 2004;125(6): 681-700.
-
43Palladini G, Dispenzieri A, Gertz MA, Kumar S, Wechalekar A, Hawkins PN, et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes. J Clin Oncol. 2012;30(36):4541-9.
-
44Corre J, Dejoie T, Caillon H, Attal M, Avet-Loiseau H, Moreau P. Serum free light chains should be the target of response evaluation in light chain multiple myeloma rather than urines: results from the IFM/DFCI 2009 trial. Blood. 2014;124:180a.
-
45Moustafa MA, Rajkumar SV, Dispenzieri A, Gertz MA, Lacy MQ, Buadi FK, et al. Utility of serum free light chain measurements in multiple myeloma patients not achieving complete response to therapy Leukemia. 2015;29(10):2033-8.
-
46Durie BG, Harousseau JL, Miguel JS, Blade J, Barlogie B, Anderson K, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20:1467-73.
-
47Kapoor P, Kumar S, Dispenzieri A, Lacy M, Dingli D, Hayman SR, et al. Survival outcomes of patients with multiple myeloma (MM) achieving stringent complete response (sCR) following upfront autologous stem cell transplantation (SCT). J Clin Oncol. 2011;29 Suppl.:8069 [abstract].
Publication Dates
-
Publication in this collection
Jan-Feb 2016
History
-
Received
8 June 2015 -
Accepted
18 Nov 2015