ABSTRACT
Splenic marginal zone lymphoma (SMZL) is a low-grade B-cell non-Hodgkin's lymphoma characterized by massive splenomegaly, moderate lymphocytosis with or without villous lymphocytes, rare involvement of peripheral lymph nodes and indolent clinical course. As a rare disease, with no randomized prospective trials, there is no standard of care for SMZL so far. Splenectomy has been done for many years as an attempt to control disease, but nowadays it has not been encouraged as first line because of new advances in therapy as rituximab, that are as effective with minimal toxicity. Facing these controversies, this review highlights advances in the literature regarding diagnosis, prognostic factors, treatment indications and therapeutic options.
Keywords:
Lymphoma, non-Hodgkin; Splenic marginal zone lymphoma; Splenic lymphoma; Indolent lymphoma; Rituximab
Introduction and clinical features
Splenic marginal zone lymphoma (SMZL) is a rare indolent non-Hodgkin lymphoma (NHL) subtype that originates from B memory lymphocytes present in the marginal zone of secondary lymphoid follicles.11 Zinzani PL. The many faces of marginal zone lymphoma. ASH Educ Progr B. 2012;2012(1):426-32.
2 Lenglet J, Traullé C, Mounier N, Benet C, Munoz-Bongrand N, Amorin S, et al. Long-term follow-up analysis of 100 patients with splenic marginal zone lymphoma treated with splenectomy as first-line treatment. Leuk Lymphoma. 2013;55:1854-60.-33 Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al, editors. World Health Organization classification of tumours of haematopoietic and lymphoid tissues. 4th ed Lyon: International Agency for Research on Cancer (IARC); 2008. International Agency for Research on Cancer (IARC). 422 p.
Patients usually present massive splenomegaly and bone marrow involvement with minimal or absent lymphadenopathy except for the spleen hilum. There is no extranodal involvement, except for the bone marrow and liver.33 Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al, editors. World Health Organization classification of tumours of haematopoietic and lymphoid tissues. 4th ed Lyon: International Agency for Research on Cancer (IARC); 2008. International Agency for Research on Cancer (IARC). 422 p.,44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301. About 25% of the patients are asymptomatic and the presence of B symptoms or high lactate dehydrogenase levels (LDH) at diagnosis is not usual.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.
Lymphocytosis is commonly present. Cytopenias are found in 25% of the cases mostly related to hypersplenism, and less frequently to auto-antibodies or bone marrow infiltration.33 Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al, editors. World Health Organization classification of tumours of haematopoietic and lymphoid tissues. 4th ed Lyon: International Agency for Research on Cancer (IARC); 2008. International Agency for Research on Cancer (IARC). 422 p.,44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.
Small amounts (less than 2 g/dL) of monoclonal protein, usually immunoglobulin (Ig)M kappa, are detected in approximately one third of patients.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,77 Traverse-Glehen A, Baseggio L, Salles G, Felman P, Berger F. Splenic marginal zone B-cell lymphoma: a distinct clinicopathological and molecular entity. Recent advances in ontogeny and classification. Curr Opin Oncol. 2011;23(5):441-8. Hyperviscosity syndromes are not usual,33 Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al, editors. World Health Organization classification of tumours of haematopoietic and lymphoid tissues. 4th ed Lyon: International Agency for Research on Cancer (IARC); 2008. International Agency for Research on Cancer (IARC). 422 p. but 20% of patients present autoimmune hemolytic anemia and other autoimmune disorders, such as thrombocytopenia, cold agglutinin disease, circulating anticoagulants and even angioedema because of acquired C1-esterase inhibitor deficiency.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,77 Traverse-Glehen A, Baseggio L, Salles G, Felman P, Berger F. Splenic marginal zone B-cell lymphoma: a distinct clinicopathological and molecular entity. Recent advances in ontogeny and classification. Curr Opin Oncol. 2011;23(5):441-8.,88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
The rarity of this disease and its indolent course are a challenge to determine standard care in the treatment and management of patients. There are no randomized trials, most of the literature are retrospective series of cases from single centers and few prospective studies have been completed or are ongoing.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
Epidemiology
SMZL is the second most common subtype of marginal zone lymphoma, comprising about 20% of the cases. It represents about 0.9% of all NHL and was considered a specific pathological entity only in 1991.11 Zinzani PL. The many faces of marginal zone lymphoma. ASH Educ Progr B. 2012;2012(1):426-32.,55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,99 Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. 2011;117(19):5019-32.
Median age at diagnosis of SMZL is 69 years. The overall age-adjusted incidence is 0.13/100,000 habitants per year. The percentage change in age-adjusted incidence is 4.81%, with most of the patients being White.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81. Gender prevalence is controversial,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.,77 Traverse-Glehen A, Baseggio L, Salles G, Felman P, Berger F. Splenic marginal zone B-cell lymphoma: a distinct clinicopathological and molecular entity. Recent advances in ontogeny and classification. Curr Opin Oncol. 2011;23(5):441-8. but there is an increasing trend to male predominance.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.,1010 Chacón JI, Mollejo M, Muñoz E, Algara P, Mateo M, Lopez L, et al. Splenic marginal zone lymphoma: clinical characteristics and prognostic factors in a series of 60 patients. Blood. 2002;100(5):1648-54.,1111 Iannitto E, Ambrosetti A, Ammatuna E, Colosio M, Florena AM, Tripodo C, et al. Splenic marginal zone lymphoma with or without villous lymphocytes. Cancer. 2004;101(9):2050-7.
The association of SMZL with hepatitis C (HCV) is common in the south of Europe,33 Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al, editors. World Health Organization classification of tumours of haematopoietic and lymphoid tissues. 4th ed Lyon: International Agency for Research on Cancer (IARC); 2008. International Agency for Research on Cancer (IARC). 422 p.,1212 Arcaini L, Merli M, Volpetti S, Rattotti S, Gotti M, Zaja F. Indolent B-cell lymphomas associated with HCV infection: clinical and virological features and role of antiviral therapy. Clin Dev Immunol. 2012;2012:1-10.,1313 Tasleem S, Sood GK. Hepatitis C associated B-cell non-hodgkin lymphoma: clinical features and the role of antiviral therapy. J Clin Transl Hepatol. 2015;3(2):134-9. and lymphoma development is usually triggered by the glycoprotein E2 of the virus that stimulates CD81 in B cells.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.,1313 Tasleem S, Sood GK. Hepatitis C associated B-cell non-hodgkin lymphoma: clinical features and the role of antiviral therapy. J Clin Transl Hepatol. 2015;3(2):134-9. Although there are controversial data in Brazil regarding the association of HCV and lymphoma, no studies have evaluated this association.1414 Marinho TA. Prevalência da infecção pelo vírus da hepatite C em indivíduos portadores de doenças oncohematológicas em Goiânia-GO. Universidade Federal de Goiás; 2013.,1515 Chindamo M, Spector N, Segadas J, Pimenta G, Vanderborght B, Morais J, et al. Prevalence of hepatitis C infection in patients with non-Hodgkin's lymphomas. Oncol Rep. 2002;9(8):657-9.
The International Lymphoma Epidemiology Consortium Non-Hodgkin Lymphoma Subtypes Project, with a database of 17,471 NHL cases and 23,096 controls, identified an association between SMZL and B cell activating autoimmune conditions, asthma and use of hair dye.1616 Bracci PM, Benavente Y, Turner JJ, Paltiel O, Slager SL, Vajdic CM, et al. Medical history, lifestyle, family history, and occupational risk factors for marginal zone lymphoma: the interlymph non-Hodgkin lymphoma subtypes project. JNCI Monogr. 2014;2014(48):52-65.
Diagnosis
The diagnosis of SMZL can be by the analysis of pathological cells present in bone marrow with blood and spleen analysis not being essential.
Bone marrow infiltration is a very common finding (83-100%), although circulating cells are detected much less frequently (29-75%).77 Traverse-Glehen A, Baseggio L, Salles G, Felman P, Berger F. Splenic marginal zone B-cell lymphoma: a distinct clinicopathological and molecular entity. Recent advances in ontogeny and classification. Curr Opin Oncol. 2011;23(5):441-8. During the course of the disease, 75% of the patients will present lymphocytosis, with characteristic, but not pathognomonic, villous cells.44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.,1717 Vannata B, Stathis A, Zucca E. Management of the marginal zone lymphomas. In: Evens AM, Blum KA, editors. Non-Hodgkin lymphoma. Cham: Springer International Publishing; 2015. p. 227-49 (Cancer Treatment and Research; vol. 165). Bone marrow aspirate is not sufficient for diagnosis; a trephine histology with immunohistochemical analysis is required.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.
Pathological cells of SMZL are small- to medium-sized mature B cells with round or oval nuclei and condensed chromatin, basophilic cytoplasm, and most of the cases present with typical unequal membrane projections (villi), the so-called villous cells (Figure 1).44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.
5 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.
6 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.-77 Traverse-Glehen A, Baseggio L, Salles G, Felman P, Berger F. Splenic marginal zone B-cell lymphoma: a distinct clinicopathological and molecular entity. Recent advances in ontogeny and classification. Curr Opin Oncol. 2011;23(5):441-8. Marrow infiltration can be nodular, interstitial or intrasinusoidal.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.
Morphologic features of villous lymphocytes in patients with splenic marginal zone lymphoma.
There is no specific immunophenotypic pattern for SMZL. Pathological cells are usually positive for CD19, CD20, CD22, CD79a, CD79b, FMC7 and IgM and negative for CD5, CD10, CD43, BCL6, cyclin D1 or CD103. The expressions of CD23, IgD and cytoplasmatic Ig are variable,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.,1818 Arcaini L, Lazzarino M, Colombo N, Burcheri S, Boveri E, Paulli M, et al. Splenic marginal zone lymphoma: a prognostic model for clinical use. Blood. 2006;107(12):4643-9. usually scoring 0-2 points in the Modified Matutes scoring system.1919 Moreau EJ, Matutes E, A’Hern RP, Morilla AM, Morilla RM, Owusu-Ankomah KA, et al. Improvement of the chronic lymphocytic leukemia scoring system with the monoclonal antibody SN8(CD79b). Am J Clin Pathol. 1997;108(4):378-82. CD5 are weakly positive in 10-25% of the cases, even with the co-expression of CD23 or CD43.2020 Evens AM, Blum KA. Non-Hodgkin lymphoma. Switzerland: Cancer Treatment and Research; 2015, 343 p. CD11c and CD25 are sometimes positive, but CD103 and CD123 are almost always negative.44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.
Bone marrow immunohistochemistry analysis reveals positivity for CD45RA, CD45RB, CD19, CD20, CD79a, PAX5/BSAP, IgD, Bcl-2, DBA-44 (CD72), TRAP and CD38.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,2121 Troussard X, Valensi F, Duchayne E, Garand R, Felman P, Tulliez M, et al. Splenic lymphoma with villous lymphocytes: clinical presentation, biology and prognostic factors in a series of 100 patients. Br J Haematol. 1996;93(3):731-6.,2222 Salomon-Nguyen F, Valensi F, Troussard X, Flandrin G. The value of the monoclonal antibody, DBA44, in the diagnosis of B-lymphoid disorders. Leuk Res. 1996;20(11/12):909-13. IgM is usually bright, but IgD is variable.44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38. Cells are usually negative for CD3, CD5, CD10, CD23, CD43, cyclin D1, anexin-A1 and BCL6. KI67/Mib1 has a low proliferation index with a characteristic pattern.44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.
The spleen is frequently enlarged, with a median weight of 1750 g (270-5500 g) and many grayish nodules throughout the parenchyma.66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38. White pulp is expanded by neoplastic cells that surround and eventually substitute germinal centers. Nodules are composed of pathological cells, located in an inner zone of small- to medium-sized B cells with round nuclei, clumped chromatin and scanty cytoplasm. Externally there is an outer zone with medium-sized pathological cells, with more irregular nucleus outlines, dispersed chromatin and moderately clear cytoplasm. There are scattered cells in this zone resembling immunoblasts. As the disease progresses, the central germinal center becomes effaced. The red pulp is invariably enveloped to a varying degree by small aggregates of larger cells and sheets of small cells, which often occupy sinuses and cords. There can be epithelioid granulomas and plasmacytic differentiation, the former especially when there is a monoclonal serum component. Immunohistochemical findings are similar to bone marrow findings.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.,99 Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. 2011;117(19):5019-32.
Matutes et al. proposed minimum diagnostic criteria for SMZL:
-
When spleen pathology is available: spleen histology and immunophenotype with a modified Matutes score of <3 points.1919 Moreau EJ, Matutes E, A’Hern RP, Morilla AM, Morilla RM, Owusu-Ankomah KA, et al. Improvement of the chronic lymphocytic leukemia scoring system with the monoclonal antibody SN8(CD79b). Am J Clin Pathol. 1997;108(4):378-82.
-
When the patient has clinical splenomegaly and splenectomy is not performed, it is sufficient to make the diagnosis with typical blood and bone marrow findings by morphology and immunophenotype with intrasinusoidal infiltration by CD20+ cells.
After the diagnosis is performed, it is important to evaluate the clinical stage of the patient, with computed tomography scans and routine exams to detect comorbidities that may affect the choice of treatment. These exams should include complete blood count with differential, serologic tests for hepatitis B and C and human immunodeficiency virus (HIV), renal and liver function tests, serum calcium, LDH, and b2-microglobulin. SMZL is regarded as a none F-18 fluorodeoxyglucose-avid disease; thus, the use of fluorodeoxyglucose positron emission tomography (FDG-PET) should be discouraged in the staging process.2323 Tarella C, Arcaini L, Baldini L, Barosi G, Billio A, Marchetti M, et al. Italian society of hematology, italian society of experimental hematology, and italian group for bone marrow transplantation guidelines for the management of indolent, nonfollicular b-cell lymphoma (marginal zone, lymphoplasmacytic, and small lymphocytic). Clin Lymphoma Myeloma Leuk. 2015;15(2):75-85.
Differential diagnosis
The differential diagnosis requires the joint analysis of clinical, morphological, immunophenotypic and genetic data, as well as immunohistochemistry.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.
Reactive follicular hyperplasia and other small B cell lymphomas should be excluded, as the pattern of splenic micronodular involvement of marginal zone differentiation and the villous lymphocytes in peripheral blood are not pathognomonic.44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.
A diagnostic test should not be performed on spleens weighing less than 300-400 g or in the absence of a standard monotypic pattern.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
CD43 and CD200 positivity and a high (3-5) modified Matutes score helps to differentiate between SMZL and chronic lymphocytic leukemia.1919 Moreau EJ, Matutes E, A’Hern RP, Morilla AM, Morilla RM, Owusu-Ankomah KA, et al. Improvement of the chronic lymphocytic leukemia scoring system with the monoclonal antibody SN8(CD79b). Am J Clin Pathol. 1997;108(4):378-82. Intrasinusoidal infiltration is unusual in chronic lymphocytic leukemia, but often seen in SMZL, in hairy cell leukemia variant (LCP-v) and sometimes in mantle cell lymphoma (MCL).55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95. In rare cases of SMZL, CD5+, morphology, negativity for cyclin D1 and SOX11, and absence of t(11;14) excludes MCL.
Hairy cell leukemia (HCL) subtypes involving the spleen are distinguished by their characteristic morphology and phenotype. CD103 and CD123 negativity exclude HCL.44 Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.
Unlike SMZL, nodules have variable sizes and tumoral cells are seen in white pulp in the case of follicular lymphoma (FL). CD10 and BCL6 expression are useful for the diagnosis of FL. The morphological characteristics of the MIB 1 tumor cell staining pattern, residual mantle cell, IgD staining for tumor cells in addition to histological findings in bone marrow and hilar lymph nodes help establish diagnosis.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.
Differential diagnosis between SZML, splenic diffuse red pulp lymphoma (SDRPL) and HCL-v can be tricky and sometimes impossible only by blood or bone marrow analyses. These are two newly recognized entities with clinicopathologic and immunophenotypic features partially overlapping those of SMZL. The diagnosis in these cases requires detailed clinical information, a comprehensive phenotype and spleen histology, which usually shows a typical pattern of diffuse infiltration with white pulp follicles preserved.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
An immunophenotypic profile with the absence of CD25, CD123, interleukin-3 anti-receptor, annexin A1, HC2 and TRAP and resistance to conventional HCL therapy is observed for HCL-v.66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.,2424 Falini B, Agostinelli C, Bigerna B, Pucciarini A, Pacini R, Tabarrini A, et al. IRTA1 is selectively expressed in nodal and extranodal marginal zone lymphomas. Histopathology. 2012;61(5):930-41.,2525 Venkataraman G, Aguhar C, Kreitman RJ, Yuan CM, Stetler-Stevenson M. Characteristic CD103 and CD123 expression pattern defines hairy cell leukemia: usefulness of CD123 and CD103 in the diagnosis of mature B-cell lymphoproliferative disorders. Am J Clin Pathol. 2011;136(4):625-30. Moreover, HCL-v is positive for the DBA-44, pan-B cells, CD11c, surface monotypic Ig (IgG most often) and CD103 FMC7.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,99 Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. 2011;117(19):5019-32.
Although SDRPL have characteristics that overlap classic SMZL, the expression of IgD and the follicular micronodular pattern is absent in most cases.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95. The distinction between those two entities may be merely academic, as the treatment is not different.2626 Perrone S, D’Elia GM, Annechini G, Ferretti A, Tosti ME, Foà R, et al. Splenic marginal zone lymphoma: prognostic factors, role of watch and wait policy, and other therapeutic approaches in the rituximab era. Leuk Res. 2016;44:53-60.
Lymphoplasmacytic lymphoma (LPL) may develop in the spleen, with homogeneous infiltration of the white pulp without standard marginal zone and monocytoid B cells. Deletions of 7q, 3T gains and intrasinusoidal infiltration are characteristic of SMZL, while del(6q) is more characteristic of LPL.2727 Schop RF. Waldenstrom macroglobulinemia neoplastic cells lack immunoglobulin heavy chain locus translocations but have frequent 6q deletions. Blood. 2002;100(8):2996-3001. Another useful marker is the MYD88 L265P mutation, that is frequent in LPL (91-100%) and rare in SMZL (6%).2828 Treon SP, Hunter ZR. A new era for Waldenstrom macroglobulinemia: MYD88 L265P. Blood. 2013;121(22):4434-6.
Moreover, there are overlapping patterns of extranodal marginal zone lymphoma (EMZL) and SMZL with the clinical findings being crucial for differentiation. Splenic involvement is rare in nodal marginal zone lymphoma (NMZL) and Immunoglobulin Superfamily Receptor Translocation Associated 1 (IRTA1), negative in 76% of SMZL, is positive in NMZL.2424 Falini B, Agostinelli C, Bigerna B, Pucciarini A, Pacini R, Tabarrini A, et al. IRTA1 is selectively expressed in nodal and extranodal marginal zone lymphomas. Histopathology. 2012;61(5):930-41. Two useful features to distinguish between SMZL and mucosa-associated lymphoid tissue (MALT) are the absence of the t(11;18)(q21;q21)2929 Remstein ED, James CD, Kurtin PJ. Incidence and subtype specificity of API2-MALT1 fusion translocations in extranodal, nodal, and splenic marginal zone lymphomas. Am J Pathol. 2000;156(4):1183-8. and the frequent IgD expression in SMZL, which is rarely observed in MALT lymphoma.55 Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.,3030 Du MQ, Peng HZ, Diss TC, Liu H, Pan LX, et al. Preferential dissemination of B-cell gastric mucosa-associated lymphoid tissue (MALT) lymphoma to the splenic marginal zone. Blood. 1997;90(10):4071-7.
Prognosis
Although most of the cases of SMZL have an indolent course with median overall survival of about ten years,1818 Arcaini L, Lazzarino M, Colombo N, Burcheri S, Boveri E, Paulli M, et al. Splenic marginal zone lymphoma: a prognostic model for clinical use. Blood. 2006;107(12):4643-9.,2222 Salomon-Nguyen F, Valensi F, Troussard X, Flandrin G. The value of the monoclonal antibody, DBA44, in the diagnosis of B-lymphoid disorders. Leuk Res. 1996;20(11/12):909-13. about 30% of the patients develop aggressive disease, with median overall survival of only four years.1010 Chacón JI, Mollejo M, Muñoz E, Algara P, Mateo M, Lopez L, et al. Splenic marginal zone lymphoma: clinical characteristics and prognostic factors in a series of 60 patients. Blood. 2002;100(5):1648-54.,1818 Arcaini L, Lazzarino M, Colombo N, Burcheri S, Boveri E, Paulli M, et al. Splenic marginal zone lymphoma: a prognostic model for clinical use. Blood. 2006;107(12):4643-9. There are no associated cytogenetic features3131 Salido M, Baro C, Oscier D, Stamatopoulos K, Dierlamm J, Matutes E, et al. Cytogenetic aberrations and their prognostic value in a series of 330 splenic marginal zone B-cell lymphomas: a multicenter study of the Splenic B-Cell Lymphoma Group. Blood. 2010;116(9):1479-88. and prognostic scores for indolent lymphomas such as the International Prognostic Index (IPI)1818 Arcaini L, Lazzarino M, Colombo N, Burcheri S, Boveri E, Paulli M, et al. Splenic marginal zone lymphoma: a prognostic model for clinical use. Blood. 2006;107(12):4643-9.,3232 Federico M, Vitolo U, Zinzani PL, Chisesi T, Clò V, Bellesi G, et al. Prognosis of follicular lymphoma: a predictive model based on a retrospective analysis of 987 cases. Intergruppo Italiano Linfomi. Blood. 2000;95(3):783-9. and Follicular International Prognostic Index (FLIPI)3333 Solal-Celigny P, Roy P, Colombat P, White J, Armitage JO, Arranz-Saez R, et al. Follicular lymphoma international prognostic index. Blood. 2004;104(5):1258-65. are not applicable. The same can be said for the Ann Arbor staging system, which is not adequate because in most cases the bone marrow is involved.3434 Carbone PP, Kaplan HS, Musshoff K, Chairman PP, Smithers DW, Tubiana M. Report of the Committee on Hodgkin's Disease Staging Classification Report of the Committee on Hodgkin's Disease Staging Classification. Cancer Res. 1971;31(11):1860-1.
There are some clinical features associated with a worse outcome such as the development of lymphadenopathy, increase in β2-microglobulin, non-hematopoietic site involvement, leukocyte count >20 × 109/L, lymphocytosis >9 × 109/L, lymphopenia, anemia, thrombocytopenia, use of chemotherapy, monoclonal component, performance status ≥2, incomplete response, advanced age, diffuse pattern of bone marrow infiltration and histologic transformation.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.,1010 Chacón JI, Mollejo M, Muñoz E, Algara P, Mateo M, Lopez L, et al. Splenic marginal zone lymphoma: clinical characteristics and prognostic factors in a series of 60 patients. Blood. 2002;100(5):1648-54.,3535 Tsimberidou AM, Catovsky D, Schlette E, O’Brien S, Wierda WG, Kantarjian H, et al. Outcomes in patients with splenic marginal zone lymphoma and marginal zone lymphoma treated with rituximab with or without chemotherapy or chemotherapy alone. Cancer. 2006;107(1):125-35.
36 Thieblemont C, Davi F, Noguera M-E, Brière J, Bertoni F, Zucca E, et al. Splenic marginal zone lymphoma: current knowledge and future directions. Oncology (Williston Park). 2012;26(2):194-202.
37 Hockley SL, Else M, Morilla A, Wotherspoon A, Dearden C, Catovsky D, et al. The prognostic impact of clinical and molecular features in hairy cell leukaemia variant and splenic marginal zone lymphoma. Br J Haematol. 2012;158(3):347-54.-3838 Matutes E. Splenic marginal zone lymphoma: disease features and management. Expert Rev Hematol. 2013;6(6):735-45.
Many karyotype abnormalities can be found: trisomy 3q (85%) del or translocation of 7q32 (40%), trisomy 18, 17q isochromosome, 13q14 deletion, and structural abnormalities of chr 1.3939 Dreyling M, Thieblemont C, Gallamini A, Arcaini L, Campo E, Hermine O, et al. Esmo consensus conferences: guidelines on malignant lymphoma. Part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. 2013;24(4):857-77. Some molecular aspects, such as NOTCH2 and KLF2 mutations, Ig gene mutation status, TP53 abnormalities and aberrant promoter methylation seem to be related to a worse outcome.3131 Salido M, Baro C, Oscier D, Stamatopoulos K, Dierlamm J, Matutes E, et al. Cytogenetic aberrations and their prognostic value in a series of 330 splenic marginal zone B-cell lymphomas: a multicenter study of the Splenic B-Cell Lymphoma Group. Blood. 2010;116(9):1479-88.,3737 Hockley SL, Else M, Morilla A, Wotherspoon A, Dearden C, Catovsky D, et al. The prognostic impact of clinical and molecular features in hairy cell leukaemia variant and splenic marginal zone lymphoma. Br J Haematol. 2012;158(3):347-54.,4040 Parry M, Rose-Zerilli MJJ, Ljungstrom V, Gibson J, Wang J, Walewska R, et al. Genetics and prognostication in splenic marginal zone lymphoma: revelations from deep sequencing. Clin Cancer Res. 2015;21(18):4174-83.,4141 Gruszka-Westwood AM. p53 abnormalities in splenic lymphoma with villous lymphocytes. Blood. 2001;97(11):3552-8. Studies from a whole exome sequencing study identified the MYD88 L265P missense mutation in 15% of SMZL.4242 Peveling-Oberhag J, Wolters F, Döring C, Walter D, Sellmann L, Scholtysik R, et al. Whole exome sequencing of microdissected splenic marginal zone lymphoma: a study to discover novel tumor-specific mutations. BMC Cancer. 2015;15(1):73.
The Italian Intergroup for Lymphomas (IIL), now Fondazione Italiana Linfomi (FIL) developed the first prognostic score after a multicenter trial with 309 patients. Specific event survival (SES) related to death by lymphoma was analyzed, as was overall survival. The 5-year cause-specific survival rate was 76%. The three most important parameters in multivariate analysis were hemoglobin <12 g/dL, LDH higher than normal and low albumin (<3.5 g/dL). Patients were grouped in three categories according to 0, 1 or 2-3 parameters, respectively, low risk (41% of the cases, 5-year SES of 88%), intermediate risk (34% of the cases, 5-year SES of 73%) and high risk (25% of the cases, 5-year SES of 50%).1818 Arcaini L, Lazzarino M, Colombo N, Burcheri S, Boveri E, Paulli M, et al. Splenic marginal zone lymphoma: a prognostic model for clinical use. Blood. 2006;107(12):4643-9. A recent study by Perrone et al. validated the score.2626 Perrone S, D’Elia GM, Annechini G, Ferretti A, Tosti ME, Foà R, et al. Splenic marginal zone lymphoma: prognostic factors, role of watch and wait policy, and other therapeutic approaches in the rituximab era. Leuk Res. 2016;44:53-60.
In 2012, the Hemoglobin-Platelet-LDH-extra-hilar-Lymphadenopathy (HPLL) score was proposed by the SMZL Study Group after a retrospective analysis of 593 patients. Patients were stratified in three groups as shown in Table 1. The criteria of the IIL were applied to the same population but the stratification power for SES of the HPLL score were better,4343 Montalbán C, Abraira V, Arcaini L, Domingo-Domenech E, Guisado-Vasco P, Iannitto E, et al. Simplification of risk stratification for splenic marginal zone lymphoma: a point-based score for practical use. Leuk Lymphoma. 2014;55(4):929-31.,4444 Montalbán C, Abraira V, Arcaini L, Domingo-Domenech E, Guisado-Vasco P, Iannitto E, et al. Risk stratification for splenic marginal zone lymphoma based on haemoglobin concentration, platelet count, high lactate dehydrogenase level and extrahilar lymphadenopathy: development and validation on 593 cases. Br J Haematol. 2012;159(2):164-71. so this seems to be the most suitable score so far.
Hemoglobin-platelet-LDH-extra-hilar-lymphadenopathy score for splenic marginal zone lymphoma as proposed by the Splenic Marginal Zone Lymphoma Study Group.
Indication for treatment
There are no standard criteria to indicate treatment. The overall survival of asymptomatic patients can be as high as 88% at five years without treatment2323 Tarella C, Arcaini L, Baldini L, Barosi G, Billio A, Marchetti M, et al. Italian society of hematology, italian society of experimental hematology, and italian group for bone marrow transplantation guidelines for the management of indolent, nonfollicular b-cell lymphoma (marginal zone, lymphoplasmacytic, and small lymphocytic). Clin Lymphoma Myeloma Leuk. 2015;15(2):75-85..
Tarella et al.,2323 Tarella C, Arcaini L, Baldini L, Barosi G, Billio A, Marchetti M, et al. Italian society of hematology, italian society of experimental hematology, and italian group for bone marrow transplantation guidelines for the management of indolent, nonfollicular b-cell lymphoma (marginal zone, lymphoplasmacytic, and small lymphocytic). Clin Lymphoma Myeloma Leuk. 2015;15(2):75-85. proposed some criteria to indicate treatment (Table 2).
The SMZL Study Group also considered low hemoglobin levels, extranodal disease and a positivity for HCV as important to indicate treatment even though these factors have not been validated yet.4444 Montalbán C, Abraira V, Arcaini L, Domingo-Domenech E, Guisado-Vasco P, Iannitto E, et al. Risk stratification for splenic marginal zone lymphoma based on haemoglobin concentration, platelet count, high lactate dehydrogenase level and extrahilar lymphadenopathy: development and validation on 593 cases. Br J Haematol. 2012;159(2):164-71.
A recent study by Perrone et al. suggested that patients should undergo an evaluation of the tumor burden similar to follicular patients, but this awaits further validation.2626 Perrone S, D’Elia GM, Annechini G, Ferretti A, Tosti ME, Foà R, et al. Splenic marginal zone lymphoma: prognostic factors, role of watch and wait policy, and other therapeutic approaches in the rituximab era. Leuk Res. 2016;44:53-60.
Types of treatment
As a rare disease with an indolent course, determining the standard treatment and management is a challenge as there have been no randomized trials and most reports are of single-center series of retrospective cases; few prospective trials have been completed or are ongoing.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81. Therefore, nowadays there is no standard care for SMZL.
Therapeutic options for SMZL comprise splenectomy, chemotherapy and the use of the anti-CD20 monoclonal antibody rituximab alone or in chemotherapy combinations.3535 Tsimberidou AM, Catovsky D, Schlette E, O’Brien S, Wierda WG, Kantarjian H, et al. Outcomes in patients with splenic marginal zone lymphoma and marginal zone lymphoma treated with rituximab with or without chemotherapy or chemotherapy alone. Cancer. 2006;107(1):125-35.,4545 Thieblemont C, Felman P, Berger F, Dumontet C, Arnaud P, Hequet O, et al. Treatment of splenic marginal zone B-cell lymphoma: an analysis of 81 patients. Clin Lymphoma. 2002;3(1):41-7.
46 Kalpadakis C, Pangalis GA, Maria KA, Sachanas S, Kontopidou FN, Yiakoumis X, et al. Treatment of splenic marginal zone lymphoma with rituximab monotherapy: progress report and comparison with splenectomy. Oncologist. 2013;18(2):190-7.
47 Else M, Marín-Niebla A, de la Cruz F, Batty P, Ríos E, Dearden CE, et al. Rituximab, used alone or in combination, is superior to other treatment modalities in splenic marginal zone lymphoma. Br J Haematol. 2012;159(3):322-8.
48 Iannitto E. How I diagnose and treat splenic lymphomas. Blood. 2011;117(9):2585-95.
49 Bennett M, Schechter GP. Treatment of splenic marginal zone lymphoma: splenectomy versus rituximab. Semin Hematol. 2010;47(2):143-7.
50 Kalpadakis C, Pangalis GA, Vassilakopoulos TP, Sachanas S, Kyrtsonis MC, Dimopoulou M, et al. Splenectomy versus Rituximab in the treatment of splenic marginal zone lymphoma. Haematologica. 2009;94(Suppl. 2):168-9.
51 Cervetti G, Galimberti S, Pelosini M, Ghio F, Cecconi N, Petrini M. Significant efficacy of 2-chlorodeoxyadenosine + rituximab in the treatment of splenic marginal zone lymphoma (SMZL): extended follow-up. Ann Oncol. 2013;24(9):2434-8.-5252 Kalpadakis C, Pangalis GA, Vassilakopoulos TP, Sachanas S, Angelopoulou MK. Treatment of splenic marginal zone lymphoma: should splenectomy be abandoned?. Leuk Lymphoma. 2014;55(7):1463-70.
Splenectomy
Splenectomy was the therapy of choice for decades and is still frequently used, although there is a tendency to prescribe rituximab monotherapy upfront, as most patients are old and with co-morbidities.1010 Chacón JI, Mollejo M, Muñoz E, Algara P, Mateo M, Lopez L, et al. Splenic marginal zone lymphoma: clinical characteristics and prognostic factors in a series of 60 patients. Blood. 2002;100(5):1648-54.,1111 Iannitto E, Ambrosetti A, Ammatuna E, Colosio M, Florena AM, Tripodo C, et al. Splenic marginal zone lymphoma with or without villous lymphocytes. Cancer. 2004;101(9):2050-7.,5252 Kalpadakis C, Pangalis GA, Vassilakopoulos TP, Sachanas S, Angelopoulou MK. Treatment of splenic marginal zone lymphoma: should splenectomy be abandoned?. Leuk Lymphoma. 2014;55(7):1463-70.
53 Parry-Jones N, Matutes E, Gruszka-Westwood AM, Swansbury GJ, Wotherspoon AC, Catovsky D. Prognostic features of splenic lymphoma with villous lymphocytes: a report on 129 patients. Br J Haematol. 2003;120(5):759-64.-5454 Lenglet J, Traull C, Mounier N, Benet C, Munoz-bongrand N, Amorin S, et al. Long-term follow-up analysis of 100 patients with splenic marginal zone lymphoma treated with splenectomy as first-line treatment. Leuk Lymphoma. 2014;55(8):1854-60. Laparoscopy should be preferred whenever possible in patients with advanced age or comorbidities.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
Although marrow involvement is not treated, splenectomy allows quick remission of the symptoms of hypersplenism and cytopenias, such as a significant reduction of circulating lymphocytes in 90% of patients. Regarding clinical improvement, in a series report, seven patients (25%) had increases in bone marrow infiltration by pathological cells, there was a modification of the pattern in five of them.
The median overall survival in most series is about ten years and 70% of the patients can remain treatment free for five years.1717 Vannata B, Stathis A, Zucca E. Management of the marginal zone lymphomas. In: Evens AM, Blum KA, editors. Non-Hodgkin lymphoma. Cham: Springer International Publishing; 2015. p. 227-49 (Cancer Treatment and Research; vol. 165).,3636 Thieblemont C, Davi F, Noguera M-E, Brière J, Bertoni F, Zucca E, et al. Splenic marginal zone lymphoma: current knowledge and future directions. Oncology (Williston Park). 2012;26(2):194-202.,5353 Parry-Jones N, Matutes E, Gruszka-Westwood AM, Swansbury GJ, Wotherspoon AC, Catovsky D. Prognostic features of splenic lymphoma with villous lymphocytes: a report on 129 patients. Br J Haematol. 2003;120(5):759-64. There is no survival benefit for the association of chemotherapy with splenectomy,1717 Vannata B, Stathis A, Zucca E. Management of the marginal zone lymphomas. In: Evens AM, Blum KA, editors. Non-Hodgkin lymphoma. Cham: Springer International Publishing; 2015. p. 227-49 (Cancer Treatment and Research; vol. 165). although some studies report increases in overall response rates.4747 Else M, Marín-Niebla A, de la Cruz F, Batty P, Ríos E, Dearden CE, et al. Rituximab, used alone or in combination, is superior to other treatment modalities in splenic marginal zone lymphoma. Br J Haematol. 2012;159(3):322-8. Tables 3 and 4 summarize the studies regarding different types of therapy for SMZL.
Pata et al. reported perioperative complications in one quarter of 41 patients submitted to splenectomy as first-line treatment: eight cases (19.5%) of pulmonary dysfunction, one case (2.4%) of deep vein thrombosis, one case (2.4%) of portal vein thrombosis and nine cases (22%) of major bleeding.5555 Pata G, Damiani E, Bartoli M, Solari S, Anastasia A, Pagani C, et al. Peri-operative complications and hematologic improvement after first-line splenectomy for splenic marginal zone lymphoma. Leuk Lymphoma. 2016;57(6):1467-70.
Infections caused by encapsulated bacteria are the major risk associated with splenectomy and vaccination against capsulated bacteria is mandatory at least two weeks before elective splenectomy.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
Splenectomy should not be performed if the patient has nodal involvement outside the splenic hilum and, conversely, it should not be omitted in cases with suspected transformation.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
Chemotherapy
Alkylating agents and purine analogs have been used as have many chemotherapy combinations such as cyclophosphamide, vincristine and prednisone (CVP); cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP), and fludarabine and cyclophosphamide (FC).3535 Tsimberidou AM, Catovsky D, Schlette E, O’Brien S, Wierda WG, Kantarjian H, et al. Outcomes in patients with splenic marginal zone lymphoma and marginal zone lymphoma treated with rituximab with or without chemotherapy or chemotherapy alone. Cancer. 2006;107(1):125-35.,4545 Thieblemont C, Felman P, Berger F, Dumontet C, Arnaud P, Hequet O, et al. Treatment of splenic marginal zone B-cell lymphoma: an analysis of 81 patients. Clin Lymphoma. 2002;3(1):41-7.
46 Kalpadakis C, Pangalis GA, Maria KA, Sachanas S, Kontopidou FN, Yiakoumis X, et al. Treatment of splenic marginal zone lymphoma with rituximab monotherapy: progress report and comparison with splenectomy. Oncologist. 2013;18(2):190-7.
47 Else M, Marín-Niebla A, de la Cruz F, Batty P, Ríos E, Dearden CE, et al. Rituximab, used alone or in combination, is superior to other treatment modalities in splenic marginal zone lymphoma. Br J Haematol. 2012;159(3):322-8.
48 Iannitto E. How I diagnose and treat splenic lymphomas. Blood. 2011;117(9):2585-95.
49 Bennett M, Schechter GP. Treatment of splenic marginal zone lymphoma: splenectomy versus rituximab. Semin Hematol. 2010;47(2):143-7.
50 Kalpadakis C, Pangalis GA, Vassilakopoulos TP, Sachanas S, Kyrtsonis MC, Dimopoulou M, et al. Splenectomy versus Rituximab in the treatment of splenic marginal zone lymphoma. Haematologica. 2009;94(Suppl. 2):168-9.-5151 Cervetti G, Galimberti S, Pelosini M, Ghio F, Cecconi N, Petrini M. Significant efficacy of 2-chlorodeoxyadenosine + rituximab in the treatment of splenic marginal zone lymphoma (SMZL): extended follow-up. Ann Oncol. 2013;24(9):2434-8. About two-thirds of patients do not respond to first-line treatment with chorambucil.66 Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.
Rituximab monotherapy
Rituximab as monotherapy is effective in SMZL with results similar to splenectomy; it has the potential to provide better responses and has less toxicity compared to chemotherapy.88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81. Rituximab has little impact on the quality of life, has reduced risk of infections, seems to induce durable remissions and can be used again at relapse.4646 Kalpadakis C, Pangalis GA, Maria KA, Sachanas S, Kontopidou FN, Yiakoumis X, et al. Treatment of splenic marginal zone lymphoma with rituximab monotherapy: progress report and comparison with splenectomy. Oncologist. 2013;18(2):190-7.,4949 Bennett M, Schechter GP. Treatment of splenic marginal zone lymphoma: splenectomy versus rituximab. Semin Hematol. 2010;47(2):143-7.,5050 Kalpadakis C, Pangalis GA, Vassilakopoulos TP, Sachanas S, Kyrtsonis MC, Dimopoulou M, et al. Splenectomy versus Rituximab in the treatment of splenic marginal zone lymphoma. Haematologica. 2009;94(Suppl. 2):168-9.,5656 Olszewski AJ, Ali S. Comparative outcomes of rituximab-based systemic therapy and splenectomy in splenic marginal zone lymphoma. Ann Hematol. 2014;93(3):449-58. Clinical and laboratorial responses are fast, with improvement in blood counts in about eight weeks.5757 Kalpadakis C, Pangalis GA, Dimopoulou MN, Vassilakopoulos TP, Kyrtsonis M-C, Korkolopoulou P, et al. Rituximab monotherapy is highly effective in splenic marginal zone lymphoma. Hematol Oncol. 2007;25(3):127-31.
Some studies report inferior outcomes of rituximab monotherapy compared to splenectomy, but in non-randomized retrospective clinical trials there may be a bias of selecting younger and fitter patients for splenectomy (Table 3).88 Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
Kalpadakis et al. reported a retrospective study of 58 patients treated with rituximab 375 mg/m2 in an induction phase (weekly for six weeks) followed by a maintenance phase with rituximab every two months for one to two years. The complete response (CR) rate after the induction phase was 45%, unconfirmed CR was 26% and partial response was 24%. The 5-year overall survival and progression-free survival were 92% and 73%, respectively (p-value <0.001)4646 Kalpadakis C, Pangalis GA, Maria KA, Sachanas S, Kontopidou FN, Yiakoumis X, et al. Treatment of splenic marginal zone lymphoma with rituximab monotherapy: progress report and comparison with splenectomy. Oncologist. 2013;18(2):190-7.. There are other regimens using rituximab; weekly for four weeks with or without maintenance as reported by Bennet et al.5858 Bennett M, Yegena S, Chubar E, Schechter G. Rituximab monotherapy in splenic marginal zone lymphoma instead of splenectomy. Br J Haematol. 2010;149(Suppl. 1):45. The best regimen, whether to use maintenance or retreatment at relapse, is also areas that need to be clarified.
Rituximab with chemotherapy
The aforementioned chemotherapy options are used alone or with rituximab. Purine analogs are more toxic and should be reserved for refractory or relapsed cases. Fludarabine has high response rates, with CR in 70% of cases and progression-free survival of 4.7 years.5757 Kalpadakis C, Pangalis GA, Dimopoulou MN, Vassilakopoulos TP, Kyrtsonis M-C, Korkolopoulou P, et al. Rituximab monotherapy is highly effective in splenic marginal zone lymphoma. Hematol Oncol. 2007;25(3):127-31.,5858 Bennett M, Yegena S, Chubar E, Schechter G. Rituximab monotherapy in splenic marginal zone lymphoma instead of splenectomy. Br J Haematol. 2010;149(Suppl. 1):45. A combination with Cladribine increased the CR from 21.4% to 62.5%, and four-year progression-free survival from 52.4% to 83.4%.5151 Cervetti G, Galimberti S, Pelosini M, Ghio F, Cecconi N, Petrini M. Significant efficacy of 2-chlorodeoxyadenosine + rituximab in the treatment of splenic marginal zone lymphoma (SMZL): extended follow-up. Ann Oncol. 2013;24(9):2434-8.
There are no results from randomized trials specific for SMZL, but there are some ongoing studies, such as the BRISMA phase II trial with Bendamustin plus rituximab, NCT01332968 with obinutuzumab plus CHOP/CVP/BR, ibrutinib (NCT01980628 and NCT01974440), and PI3K inhibitors (NCT01282424, NCT01732926, NCT02369016, NCT02367040, and NCT01732913) (Table 4).
Treatment of patients with splenic marginal zone lymphoma and hepatitis C
Patients with hepatitis C who do not require an immediate cytoreductive treatment should receive first-line antiviral treatment with pegylated alpha-interferon and ribavirin, because a CR of SMZL occurs in about 75% of the cases.3939 Dreyling M, Thieblemont C, Gallamini A, Arcaini L, Campo E, Hermine O, et al. Esmo consensus conferences: guidelines on malignant lymphoma. Part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. 2013;24(4):857-77.,5959 Arcaini L, Vallisa D, Rattotti S, Ferretti VV, Ferreri AJ, Bernuzzi P, et al. Antiviral treatment in patients with indolent B-cell lymphomas associated with HCV infection: a study of the Fondazione Italiana Linfomi. Ann Oncol. 2014;25(7):1404-10.
Splenic irradiation
Splenic irradiation has historical interest and there are isolated reports of its use before the era of rituximab therapy.2121 Troussard X, Valensi F, Duchayne E, Garand R, Felman P, Tulliez M, et al. Splenic lymphoma with villous lymphocytes: clinical presentation, biology and prognostic factors in a series of 100 patients. Br J Haematol. 1996;93(3):731-6.,6060 El Weshi A, Ribrag V, Girinski T, El Hajj M, Dhermain F, Bayle C. Low and medium dose spleen radiation therapy are able to induce long-term responses in splenic lymphoma with villous lymphocytes. Br J Haematol. 1998;103(4):1212-3.
Treatment considerations
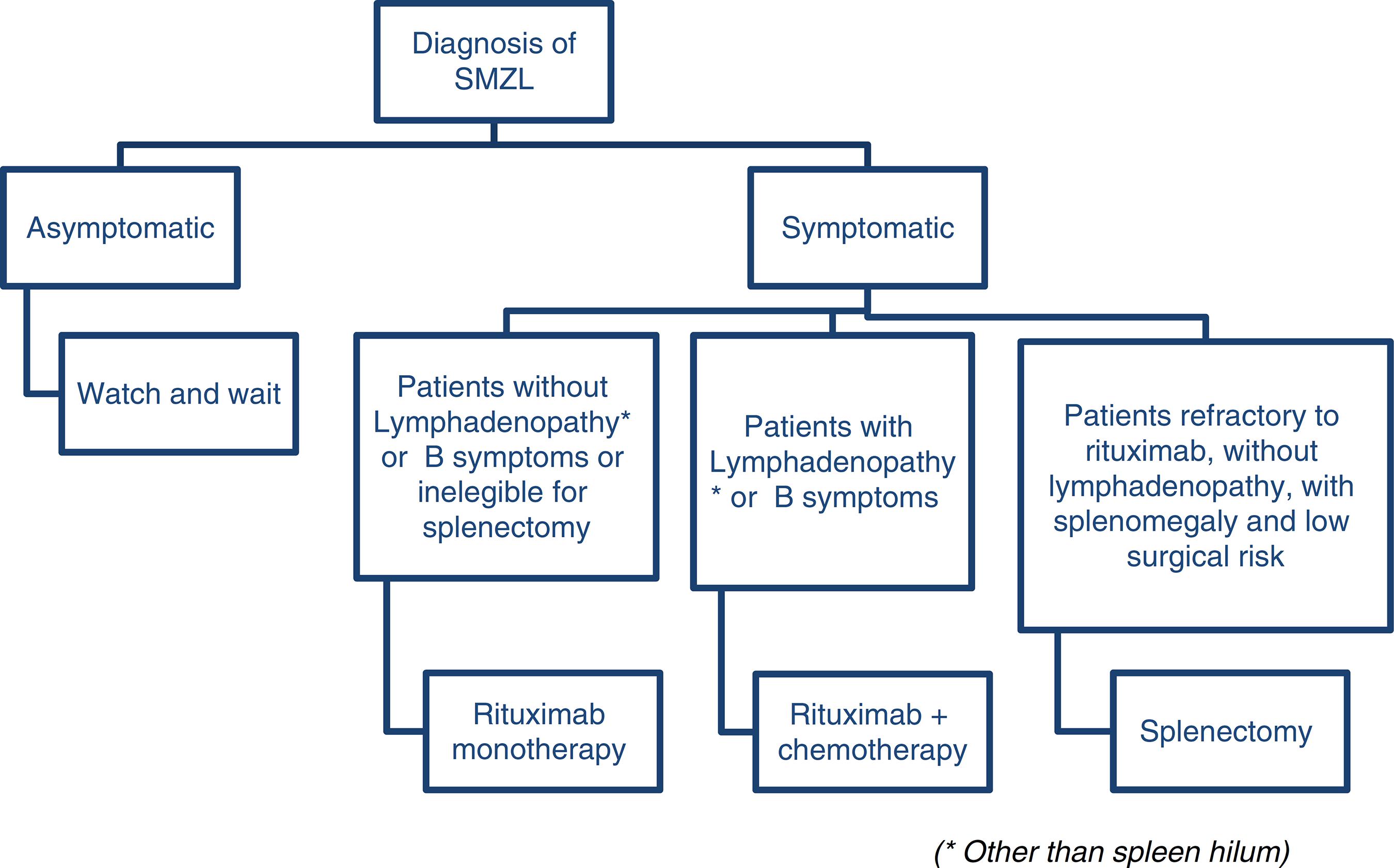
Arcaini et al. proposes a consensus using the guidelines of both the European Society for Medical Oncology3939 Dreyling M, Thieblemont C, Gallamini A, Arcaini L, Campo E, Hermine O, et al. Esmo consensus conferences: guidelines on malignant lymphoma. Part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. 2013;24(4):857-77. and the Società Italiana di Ematologia.2323 Tarella C, Arcaini L, Baldini L, Barosi G, Billio A, Marchetti M, et al. Italian society of hematology, italian society of experimental hematology, and italian group for bone marrow transplantation guidelines for the management of indolent, nonfollicular b-cell lymphoma (marginal zone, lymphoplasmacytic, and small lymphocytic). Clin Lymphoma Myeloma Leuk. 2015;15(2):75-85. According to the European Society, rituximab monotherapy is a reasonable first-line therapy and a less traumatic alternative to splenectomy and according to the Italian Society, rituximab is a good option for patients without disseminated disease (no lymphadenopathy other than spleen hilum, no constitutional symptoms or signs of high-grade transformation) who need treatment and are not eligible for splenectomy. The group of patients with constitutional symptoms or signs of high-grade transformation may be eligible for rituximab-chemotherapy combinations. There is no standard care so far, but combinations with CVP and chlorambucil are accepted as first line.2323 Tarella C, Arcaini L, Baldini L, Barosi G, Billio A, Marchetti M, et al. Italian society of hematology, italian society of experimental hematology, and italian group for bone marrow transplantation guidelines for the management of indolent, nonfollicular b-cell lymphoma (marginal zone, lymphoplasmacytic, and small lymphocytic). Clin Lymphoma Myeloma Leuk. 2015;15(2):75-85.
Figure 2 illustrates a suggested algorithm for the treatment of SMZL patients based on these guidelines.
Response evaluation
The criteria used to evaluate response of patients with SMZL to treatment are shown in Table 5.
Follow-up
Asymptomatic patients should be seen every six months with no more than a physical examination, blood counts, and biochemistry. The interval between visits should be shortened in cases of increasing splenomegaly or the occurrence of cytopenia. Computed tomography and bone marrow biopsy are not indicated unless signs of disease progression are identified.3939 Dreyling M, Thieblemont C, Gallamini A, Arcaini L, Campo E, Hermine O, et al. Esmo consensus conferences: guidelines on malignant lymphoma. Part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. 2013;24(4):857-77.
During the first three months of treatment, blood counts and laboratory work-ups should be performed every four to six weeks and every six months thereafter.3939 Dreyling M, Thieblemont C, Gallamini A, Arcaini L, Campo E, Hermine O, et al. Esmo consensus conferences: guidelines on malignant lymphoma. Part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. 2013;24(4):857-77.
Final considerations
SZML is an indolent lymphoma that presents many unsolved questions, such as standard prognostic criteria and standard treatment. As it comprises less than 2% of lymphomas, large randomized clinical trials are not likely and review articles that clarify some issues are important in the clinical practice.
References
-
1Zinzani PL. The many faces of marginal zone lymphoma. ASH Educ Progr B. 2012;2012(1):426-32.
-
2Lenglet J, Traullé C, Mounier N, Benet C, Munoz-Bongrand N, Amorin S, et al. Long-term follow-up analysis of 100 patients with splenic marginal zone lymphoma treated with splenectomy as first-line treatment. Leuk Lymphoma. 2013;55:1854-60.
-
3Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al, editors. World Health Organization classification of tumours of haematopoietic and lymphoid tissues. 4th ed Lyon: International Agency for Research on Cancer (IARC); 2008. International Agency for Research on Cancer (IARC). 422 p.
-
4Behdad A, Bailey NG. Diagnosis of splenic B-cell lymphomas in the bone marrow: a review of histopathologic, immunophenotypic, and genetic findings. Arch Pathol Lab Med. 2014;138(10):1295-301.
-
5Matutes E, Oscier D, Montalban C, Berger F, Callet-Bauchu E, Dogan A, et al. Splenic marginal zone lymphoma proposals for a revision of diagnostic, staging and therapeutic criteria. Leukemia. 2008;22(3):487-95.
-
6Mendes LS, Du M-Q, Matutes E, Wotherspoon A. Splenic marginal zone lymphoma: a review of the clinical presentation, pathology, molecular biology, and management. Blood Lymph Cancer: Targets Therapy. 2014;4:29-38.
-
7Traverse-Glehen A, Baseggio L, Salles G, Felman P, Berger F. Splenic marginal zone B-cell lymphoma: a distinct clinicopathological and molecular entity. Recent advances in ontogeny and classification. Curr Opin Oncol. 2011;23(5):441-8.
-
8Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-81.
-
9Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. 2011;117(19):5019-32.
-
10Chacón JI, Mollejo M, Muñoz E, Algara P, Mateo M, Lopez L, et al. Splenic marginal zone lymphoma: clinical characteristics and prognostic factors in a series of 60 patients. Blood. 2002;100(5):1648-54.
-
11Iannitto E, Ambrosetti A, Ammatuna E, Colosio M, Florena AM, Tripodo C, et al. Splenic marginal zone lymphoma with or without villous lymphocytes. Cancer. 2004;101(9):2050-7.
-
12Arcaini L, Merli M, Volpetti S, Rattotti S, Gotti M, Zaja F. Indolent B-cell lymphomas associated with HCV infection: clinical and virological features and role of antiviral therapy. Clin Dev Immunol. 2012;2012:1-10.
-
13Tasleem S, Sood GK. Hepatitis C associated B-cell non-hodgkin lymphoma: clinical features and the role of antiviral therapy. J Clin Transl Hepatol. 2015;3(2):134-9.
-
14Marinho TA. Prevalência da infecção pelo vírus da hepatite C em indivíduos portadores de doenças oncohematológicas em Goiânia-GO. Universidade Federal de Goiás; 2013.
-
15Chindamo M, Spector N, Segadas J, Pimenta G, Vanderborght B, Morais J, et al. Prevalence of hepatitis C infection in patients with non-Hodgkin's lymphomas. Oncol Rep. 2002;9(8):657-9.
-
16Bracci PM, Benavente Y, Turner JJ, Paltiel O, Slager SL, Vajdic CM, et al. Medical history, lifestyle, family history, and occupational risk factors for marginal zone lymphoma: the interlymph non-Hodgkin lymphoma subtypes project. JNCI Monogr. 2014;2014(48):52-65.
-
17Vannata B, Stathis A, Zucca E. Management of the marginal zone lymphomas. In: Evens AM, Blum KA, editors. Non-Hodgkin lymphoma. Cham: Springer International Publishing; 2015. p. 227-49 (Cancer Treatment and Research; vol. 165).
-
18Arcaini L, Lazzarino M, Colombo N, Burcheri S, Boveri E, Paulli M, et al. Splenic marginal zone lymphoma: a prognostic model for clinical use. Blood. 2006;107(12):4643-9.
-
19Moreau EJ, Matutes E, A’Hern RP, Morilla AM, Morilla RM, Owusu-Ankomah KA, et al. Improvement of the chronic lymphocytic leukemia scoring system with the monoclonal antibody SN8(CD79b). Am J Clin Pathol. 1997;108(4):378-82.
-
20Evens AM, Blum KA. Non-Hodgkin lymphoma. Switzerland: Cancer Treatment and Research; 2015, 343 p.
-
21Troussard X, Valensi F, Duchayne E, Garand R, Felman P, Tulliez M, et al. Splenic lymphoma with villous lymphocytes: clinical presentation, biology and prognostic factors in a series of 100 patients. Br J Haematol. 1996;93(3):731-6.
-
22Salomon-Nguyen F, Valensi F, Troussard X, Flandrin G. The value of the monoclonal antibody, DBA44, in the diagnosis of B-lymphoid disorders. Leuk Res. 1996;20(11/12):909-13.
-
23Tarella C, Arcaini L, Baldini L, Barosi G, Billio A, Marchetti M, et al. Italian society of hematology, italian society of experimental hematology, and italian group for bone marrow transplantation guidelines for the management of indolent, nonfollicular b-cell lymphoma (marginal zone, lymphoplasmacytic, and small lymphocytic). Clin Lymphoma Myeloma Leuk. 2015;15(2):75-85.
-
24Falini B, Agostinelli C, Bigerna B, Pucciarini A, Pacini R, Tabarrini A, et al. IRTA1 is selectively expressed in nodal and extranodal marginal zone lymphomas. Histopathology. 2012;61(5):930-41.
-
25Venkataraman G, Aguhar C, Kreitman RJ, Yuan CM, Stetler-Stevenson M. Characteristic CD103 and CD123 expression pattern defines hairy cell leukemia: usefulness of CD123 and CD103 in the diagnosis of mature B-cell lymphoproliferative disorders. Am J Clin Pathol. 2011;136(4):625-30.
-
26Perrone S, D’Elia GM, Annechini G, Ferretti A, Tosti ME, Foà R, et al. Splenic marginal zone lymphoma: prognostic factors, role of watch and wait policy, and other therapeutic approaches in the rituximab era. Leuk Res. 2016;44:53-60.
-
27Schop RF. Waldenstrom macroglobulinemia neoplastic cells lack immunoglobulin heavy chain locus translocations but have frequent 6q deletions. Blood. 2002;100(8):2996-3001.
-
28Treon SP, Hunter ZR. A new era for Waldenstrom macroglobulinemia: MYD88 L265P. Blood. 2013;121(22):4434-6.
-
29Remstein ED, James CD, Kurtin PJ. Incidence and subtype specificity of API2-MALT1 fusion translocations in extranodal, nodal, and splenic marginal zone lymphomas. Am J Pathol. 2000;156(4):1183-8.
-
30Du MQ, Peng HZ, Diss TC, Liu H, Pan LX, et al. Preferential dissemination of B-cell gastric mucosa-associated lymphoid tissue (MALT) lymphoma to the splenic marginal zone. Blood. 1997;90(10):4071-7.
-
31Salido M, Baro C, Oscier D, Stamatopoulos K, Dierlamm J, Matutes E, et al. Cytogenetic aberrations and their prognostic value in a series of 330 splenic marginal zone B-cell lymphomas: a multicenter study of the Splenic B-Cell Lymphoma Group. Blood. 2010;116(9):1479-88.
-
32Federico M, Vitolo U, Zinzani PL, Chisesi T, Clò V, Bellesi G, et al. Prognosis of follicular lymphoma: a predictive model based on a retrospective analysis of 987 cases. Intergruppo Italiano Linfomi. Blood. 2000;95(3):783-9.
-
33Solal-Celigny P, Roy P, Colombat P, White J, Armitage JO, Arranz-Saez R, et al. Follicular lymphoma international prognostic index. Blood. 2004;104(5):1258-65.
-
34Carbone PP, Kaplan HS, Musshoff K, Chairman PP, Smithers DW, Tubiana M. Report of the Committee on Hodgkin's Disease Staging Classification Report of the Committee on Hodgkin's Disease Staging Classification. Cancer Res. 1971;31(11):1860-1.
-
35Tsimberidou AM, Catovsky D, Schlette E, O’Brien S, Wierda WG, Kantarjian H, et al. Outcomes in patients with splenic marginal zone lymphoma and marginal zone lymphoma treated with rituximab with or without chemotherapy or chemotherapy alone. Cancer. 2006;107(1):125-35.
-
36Thieblemont C, Davi F, Noguera M-E, Brière J, Bertoni F, Zucca E, et al. Splenic marginal zone lymphoma: current knowledge and future directions. Oncology (Williston Park). 2012;26(2):194-202.
-
37Hockley SL, Else M, Morilla A, Wotherspoon A, Dearden C, Catovsky D, et al. The prognostic impact of clinical and molecular features in hairy cell leukaemia variant and splenic marginal zone lymphoma. Br J Haematol. 2012;158(3):347-54.
-
38Matutes E. Splenic marginal zone lymphoma: disease features and management. Expert Rev Hematol. 2013;6(6):735-45.
-
39Dreyling M, Thieblemont C, Gallamini A, Arcaini L, Campo E, Hermine O, et al. Esmo consensus conferences: guidelines on malignant lymphoma. Part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. 2013;24(4):857-77.
-
40Parry M, Rose-Zerilli MJJ, Ljungstrom V, Gibson J, Wang J, Walewska R, et al. Genetics and prognostication in splenic marginal zone lymphoma: revelations from deep sequencing. Clin Cancer Res. 2015;21(18):4174-83.
-
41Gruszka-Westwood AM. p53 abnormalities in splenic lymphoma with villous lymphocytes. Blood. 2001;97(11):3552-8.
-
42Peveling-Oberhag J, Wolters F, Döring C, Walter D, Sellmann L, Scholtysik R, et al. Whole exome sequencing of microdissected splenic marginal zone lymphoma: a study to discover novel tumor-specific mutations. BMC Cancer. 2015;15(1):73.
-
43Montalbán C, Abraira V, Arcaini L, Domingo-Domenech E, Guisado-Vasco P, Iannitto E, et al. Simplification of risk stratification for splenic marginal zone lymphoma: a point-based score for practical use. Leuk Lymphoma. 2014;55(4):929-31.
-
44Montalbán C, Abraira V, Arcaini L, Domingo-Domenech E, Guisado-Vasco P, Iannitto E, et al. Risk stratification for splenic marginal zone lymphoma based on haemoglobin concentration, platelet count, high lactate dehydrogenase level and extrahilar lymphadenopathy: development and validation on 593 cases. Br J Haematol. 2012;159(2):164-71.
-
45Thieblemont C, Felman P, Berger F, Dumontet C, Arnaud P, Hequet O, et al. Treatment of splenic marginal zone B-cell lymphoma: an analysis of 81 patients. Clin Lymphoma. 2002;3(1):41-7.
-
46Kalpadakis C, Pangalis GA, Maria KA, Sachanas S, Kontopidou FN, Yiakoumis X, et al. Treatment of splenic marginal zone lymphoma with rituximab monotherapy: progress report and comparison with splenectomy. Oncologist. 2013;18(2):190-7.
-
47Else M, Marín-Niebla A, de la Cruz F, Batty P, Ríos E, Dearden CE, et al. Rituximab, used alone or in combination, is superior to other treatment modalities in splenic marginal zone lymphoma. Br J Haematol. 2012;159(3):322-8.
-
48Iannitto E. How I diagnose and treat splenic lymphomas. Blood. 2011;117(9):2585-95.
-
49Bennett M, Schechter GP. Treatment of splenic marginal zone lymphoma: splenectomy versus rituximab. Semin Hematol. 2010;47(2):143-7.
-
50Kalpadakis C, Pangalis GA, Vassilakopoulos TP, Sachanas S, Kyrtsonis MC, Dimopoulou M, et al. Splenectomy versus Rituximab in the treatment of splenic marginal zone lymphoma. Haematologica. 2009;94(Suppl. 2):168-9.
-
51Cervetti G, Galimberti S, Pelosini M, Ghio F, Cecconi N, Petrini M. Significant efficacy of 2-chlorodeoxyadenosine + rituximab in the treatment of splenic marginal zone lymphoma (SMZL): extended follow-up. Ann Oncol. 2013;24(9):2434-8.
-
52Kalpadakis C, Pangalis GA, Vassilakopoulos TP, Sachanas S, Angelopoulou MK. Treatment of splenic marginal zone lymphoma: should splenectomy be abandoned?. Leuk Lymphoma. 2014;55(7):1463-70.
-
53Parry-Jones N, Matutes E, Gruszka-Westwood AM, Swansbury GJ, Wotherspoon AC, Catovsky D. Prognostic features of splenic lymphoma with villous lymphocytes: a report on 129 patients. Br J Haematol. 2003;120(5):759-64.
-
54Lenglet J, Traull C, Mounier N, Benet C, Munoz-bongrand N, Amorin S, et al. Long-term follow-up analysis of 100 patients with splenic marginal zone lymphoma treated with splenectomy as first-line treatment. Leuk Lymphoma. 2014;55(8):1854-60.
-
55Pata G, Damiani E, Bartoli M, Solari S, Anastasia A, Pagani C, et al. Peri-operative complications and hematologic improvement after first-line splenectomy for splenic marginal zone lymphoma. Leuk Lymphoma. 2016;57(6):1467-70.
-
56Olszewski AJ, Ali S. Comparative outcomes of rituximab-based systemic therapy and splenectomy in splenic marginal zone lymphoma. Ann Hematol. 2014;93(3):449-58.
-
57Kalpadakis C, Pangalis GA, Dimopoulou MN, Vassilakopoulos TP, Kyrtsonis M-C, Korkolopoulou P, et al. Rituximab monotherapy is highly effective in splenic marginal zone lymphoma. Hematol Oncol. 2007;25(3):127-31.
-
58Bennett M, Yegena S, Chubar E, Schechter G. Rituximab monotherapy in splenic marginal zone lymphoma instead of splenectomy. Br J Haematol. 2010;149(Suppl. 1):45.
-
59Arcaini L, Vallisa D, Rattotti S, Ferretti VV, Ferreri AJ, Bernuzzi P, et al. Antiviral treatment in patients with indolent B-cell lymphomas associated with HCV infection: a study of the Fondazione Italiana Linfomi. Ann Oncol. 2014;25(7):1404-10.
-
60El Weshi A, Ribrag V, Girinski T, El Hajj M, Dhermain F, Bayle C. Low and medium dose spleen radiation therapy are able to induce long-term responses in splenic lymphoma with villous lymphocytes. Br J Haematol. 1998;103(4):1212-3.
Publication Dates
-
Publication in this collection
Apr-Jun 2017
History
-
Received
25 May 2016 -
Accepted
9 Sept 2016