Abstracts
INTRODUCTION AND OBJECTIVE: Cardiovascular disease begins at infancy and it has been linked to the presence of cardiovascular risk factors (CRF). Prevalence of these factors varies a lot among different Brazilian populations and has been mostly studied in big and medium size cities. Thus, this study assessed the prevalence of CRF and physical activity (PA) in children and adolescents from Muzambinho, a small city in the state of Minas Gerais. METHODS: 205 subjects (7 to 18 years - 108 males) were studied. Body weight and height, glycemia, cholesterolemia, blood pressure (BP), and PA were measured. Comparisons were made by Qui-square test. RESULTS: Obesity and altered values of BP, glycemia, and cholesterolemia were found, respectively, in 19, 11, 5 and 15% of the subjects. There was no difference between genders, while the prevalence of smokers, drinkers, altered BP, and inactivity increased with age. Seventy-nine percent of the subjects practiced community PA; 10% occupational PA; 97% physical education classes; 72% PA during school recess; and 90% leisure time PA. Ninety-two percent of them were active. Occupational PA was higher in girls, and increased with age in boys. Leisure time and during school recess PA decreased with age in both genders. CONCLUSION: Except for physical inactivity, prevalence of CRF was high, did not differ between genders, and increased with age. High levels of all kinds of PA were found; they differed between genders, and decreased with age.
cardiovascular risk factors; inactivity; obesity; hypertension; hypercholesterolemia
INTRODUÇÃO E OBJETIVO: A doença cardiovascular inicia na infância e está atrelada à presença de fatores de risco cardiovascular (FRC). A prevalência desses fatores varia em diferentes populações brasileiras, tendo sido estudada principalmente em cidades de médio e grande porte. Este estudo avaliou a prevalência dos FRC e da prática de atividade física (AF) em crianças e adolescentes de Muzambinho, uma cidade de pequeno porte. MÉTODO: Foram avaliados 205 sujeitos (entre sete e 18 anos - 108 do gênero masculino). Foram medidos: peso, estatura, glicemia, colesterolemia, pressão arterial (PA) e prática de AF. As comparações foram realizadas pelo teste do Qui-quadrado. RESULTADOS: A prevalência de sobrepeso foi de 19% e de valores alterados de PA, glicemia e colesterolemia foram de, respectivamente, 11, 5 e 15%. Não houve diferença na prevalência dos FRC entre os sexos. O tabagismo, o alcoolismo, a PA alterada e a insuficiência de AF aumentaram com a idade. Setenta e nove por cento dos sujeitos praticavam AF de locomoção, 10% ocupacional, 97% nas aulas de educação física, 72% no recreio e 90% de lazer. Noventa e dois por cento foram considerados ativos. A prática de AF ocupacional foi maior nas meninas e aumentou nos meninos com a idade. A prevalência de AF de lazer e recreio diminuiu com a idade nos dois sexos. CONCLUSÃO: A prevalência de FRC, exceto do sedentarismo, foi expressiva, não diferiu entre os sexos e aumentou com a idade. A prática de AF de todos os tipos foi alta, diferenciou-se entre os sexos e diminuiu com a idade.
fatores de risco cardiovascular; sedentarismo; obesidade; hipertensão arterial; hipercolesterolemia
ORIGINAL ARTICLE
EXERCISE AND SPORTS MEDICINE CLINIC
ISchool of Physical Education and Sport - University of São Paulo - São Paulo - Brazil
IISchool of Physical Education of Muzambinho - Minas Gerais - Brazil
IIIFaculty of Physical Education and Sports, Universidade Pedagogica Maputo - Mozambique
IVSports Faculty - University of Porto - Portugal
Mailing address
ABSTRACT
INTRODUCTION AND OBJECTIVE: Cardiovascular disease begins at infancy and has been linked to the presence of cardiovascular risk factors (CRF). Prevalence of these factors varies a lot among different brazilian populations and has been mostly studied in big and medium size cities. Thus, this study assessed the prevalence of CRF and physical activity (PA) in children and adolescents from Muzambinho, a small city in the state of Minas Gerais.
METHODS: 205 subjects (7 to 18 years - 108 males) were studied. Body weight and height, glycemia, cholesterolemia, blood pressure (BP), and PA were measured. Comparisons were made by Qui-square test.
RESULTS: Obesity and altered values of BP, glycemia, and cholesterolemia were found, respectively, in 19, 11, 5 and 15% of the subjects. There was no difference between genders, while the prevalence of smokers, drinkers, altered BP, and inactivity increased with age. Seventy-nine percent of the subjects practiced commuting PA; 10% occupational PA; 97% physical education classes; 72% PA during school recess; and 90% leisure time PA. Ninety-two percent of them were active. Occupational PA was higher in girls, and increased with age in boys. Leisure-time and during school recess PA decreased with age in both genders.
CONCLUSION: Except for physical inactivity, prevalence of CRF was high, did not differ between genders, and increased with age. High levels of all kinds of PA were found; they differed between genders, and decreased with age.
Keywords: cardiovascular risk factors, inactivity, obesity, hypertension, hypercholesterolemia.
INTRODUCTION
Cardiovascular disease is the main cause of death in adults in Brazil(1) and worldwide(2). Its onset is partly due to the presence of cardiovascular risk factors (CRF)(3). The atherosclerotic process, however, already begins in childhood. A classical study(4) observed fatty strains and fibrous plaques in the coronaries of children and adolescents who died of other causes. Even at this age group, the presence of these injuries was associated with the presence of these CRF(4).
The prevalence of CRF has been increasing in the modern society, both in adults and children and adolescents(5). Epidemiological studies have reported prevalences that considerably vary in the young population among different brazilian cities(6-13). For example, the prevalence of altered blood pressure (BP) was of 3.9% in Ouro Preto(6) and of 28% in Campinas(7), while sedentarism reached 58.2% of the pediatric population of Pelotas(9) and 93.5% of Maceió(12). Due to this diversity, it is important to study the prevalence of these factors in further brazilian populations for a broader mapping.
The prevalence of CRF in each population can be influenced by aspects such as gender and age. Although gender is considered an important factor in adults(14,15), studies with children(11,12,16) did not observe difference in the CRF between genders. However, the practice of physical activity (PA), especially leisure-time ones, is more frequent amongst boys(9,16). Concerning age, while the study from Ouro Preto(6) demonstrated increase of many CRF with age progression, the study from Bento Gonçalves(8) did not demonstrate difference. Thus, it seems clear that the correlation between age, gender and CRF prevalence may vary in different populations and should be further researched.
The majority of studies on CRF was carried out in medium or large cities. Nevertheless, part of the brazilian society still lives in small cities, whose social, economical and cultural characteristics are different and can result in different patterns of CRF which needs to be further investigated. Muzambinho is a small city placed in the southern region of Minas Gerais state and has a population of 19,925 inhabitants in a territory extension of 409 km2(17). These characteristics determined the choice for this city for the study.
The study had as aims: 1) to verify the prevalence of CRF of children and adolescents from Muzambinho, 2) to evaluate the PA habits of this population, and 3) to evaluate the effect of the gender and age in the prevalence of CRF and PA.
METHODS
Materials
The sample of this study was selected among 10-year old children and their siblings, who participated in a theme study which tried to evaluate 25% of the students of the public chain from the city of Muzambinho. This city has 5,650 inhabitants aged between five and 19 years from whom 3,105 are in the elementary school and 1,157 in the high school(17). The final sample was composed of 205 children and adolescents between seven and 18 years, out of which 108 were boys and 104 aged < 10.7 years, totalizing 4.8% of the school target-population. The study was approved by the Ethics Committee of the School of Physical Activity and Sport of University of São Paulo.
Experimental procedures
The data were collected from March, 2008 to August, 2009. The families of the children selected from the theme Project were initially visited in their households for the explanation about the project and signature of the consent form. Subsequently, a new visit to the household was scheduled for fasting blood collection and then, a third date was set for the family to visit the school in order to take part in other evaluations.
The following variables were studied: demographic (gender and age); cardiovascular risk (hereditariety, hypertension, diabetes mellitus and dyslipidemia); anthropometric (weight, height, body mass index and waist circumference); biochemical (fasting glycemia and cholesterolemia); cardiovascular (BP), social habits (smoking and alcohol ingestion) and PA practice (commuting, occupational, educational, in school recess and leisure-time).
Measurements
Anthropometric - weight (kilos) and height (meters) were measured on a Filizola scale. Waist circumference (WC) was measured with a measuring tape placed at the umbilical scar height. Body mass index (BMI) was calculated. Obesity level was identified using the growth curves by the Center for Disease Control and Prevention(18). BMI was considered altered (risk of overweight and overweight), when it was > percentile 85. WC was considered altered when the value was > percentile 95 for age(19).
Metabolic - fasting glycemia and total cholesterolemia were measured with automatic monitors (Accu-Check-Advantage II and Accutrend GC). In glycemia, values > 100mg/dl were considered altered(20) and, total cholesterolemia, values > 170mg/dl were considered altered(21).
Cardiovascular - BP was measured twice after five minute-rest at sitting position, applying the auscultatory method and a calibrated aneroid sphygmomanoneter. Phases I and V of the Korotkoff sounds were employed to determine the values of systolic blood pressure (SBP) and diastolic blood pressure (DBP), respectively. Arm circumference was measured and an arm cuff of suitable size from five available sizes was chosen. BP of each subject was established by the mean of measurements obtained. Percentile of this pressure concerning gender, age and height was calculated from the BP value. BP was considered altered when the SBP and/or DBP percentiles were > 90, or if SBP and/or DBP were > 120 and/or 80mmHg(22).
Demographic data and known cardiovascular risk - these data were obtained in an interview. Gender and date of birth of the subjects were recorded, calculating age in years and with centesimal rounding. The subjects were asked about smoking and alcohol ingestion. Concerning the known cardiovascular risk, the subjects and their parents were heard about the presence of diseases and CRF, besides the use of medication. The presence of CRF was considered based on criteria by the American College of Sports Medicine(23):
a) Hereditariety: father, mother, siblings with atherosclerotic disease, if man < 55 years and if woman < 65 years; and b) Hypertension, Diabetes and Hypercholesterolemia: medical diagnosis report and/or use of medication.
PA practice - it was evaluated through an interview. The children and adolescents, with their parents' assistance, were heard about PA of commuting, occupational, at physical education classes, at school recess and leisure-time. When these activities were present, their weekly frequency, duration and intensity were asked. Based on this information, it was possible to calculate the PA volume of each type, by multiplying the duration of each activity by its weekly frequency. Total PA weekly volume was calculated by adding the volume of several types of activity. The subjects were classified in insufficiently active when performed less than 300 min per week of PA (23). This classification was performed using the total PA and the leisure-time PA (insufficiently active at leisure-time PA).
Data analysis
Data are presented in mean ± SD and in percentage of occurrence. Age groups were divided with the application of the percentile 50 of the sample, which corresponded to 10.7 years. The comparisons of prevalence between genders and age groups were done by the chi-square test. P < 0.05 was accepted as significant.
RESULTS
Concerning the known diseases and CRF, only 0.5% of the subjects had cardiac disease and 7.2% had hereditariety for cardiac diseases. No one reported high BP, diabetes mellitus or dyslipidemia, but 2.5% of the sample was of smokers and 2.0% ingested alcohol beverages.
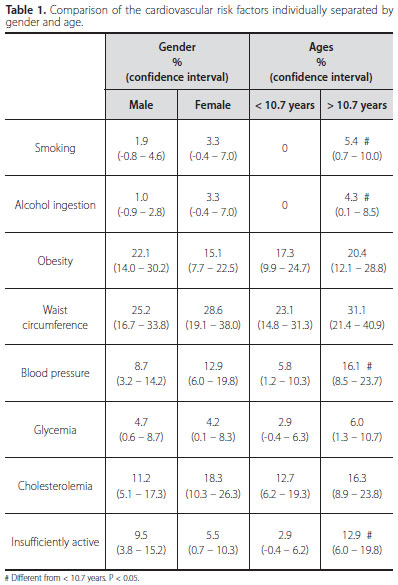
In the measurements performed, 18.8% of the subjects presented overweight or obesity; 26.8% altered waist; 10.7% altered BP; 4.5% altered glycemia; 14.5% altered cholesterolemia and 7.7% were considered insufficiently active.
The comparisons of this prevalence between ages and genders are presented in table 1. There was not significant difference of any of the CRF analysed between genders. However, considering age, the older subjects presented higher prevalence of smoking habit, ingestion of alcohol beverages, altered BP and insufficient total PA.
The CRF prevalence simultaneously sorted by genders and ages are presented in table 2. The increase of altered BP as well as insufficient total PA prevalence between ages was significant only in the boys.
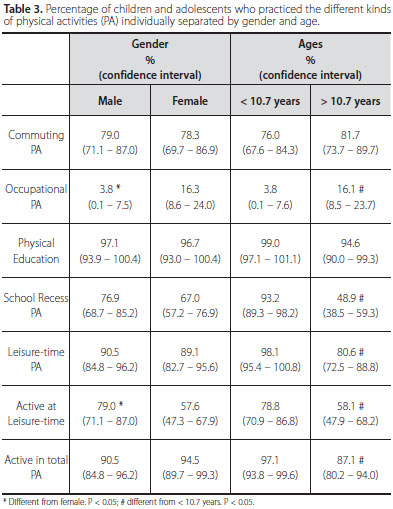
Concerning the PA practice of the total sample, 78.7% of the children and adolescents reported having practiced commuting PA, being walking the commonest; 9.6% reported having practiced occupational PA; 97.0% reported having had physical education classes; 72.3% reported having practiced PA during school recess and 89.8% reported having practiced leisure-time PA, being street play the commonest. 92.3% were considered active concerning total PA, while 69.0% were considered active concerning only leisure-time PA.
The percentages of subjects who performed each kind of PA sorted in gender and age group are presented in table 3. In gender comparison, the percentage of subjects who performed occupational PA was lower, while the active in leisure-time one was higher in boys. As age progresses, the percentage of subjects who performed occupational PA was higher and the percentages of the ones who exercised during school recess and leisure-time were lower in the older ones. Thus, the percentage of active subjects in total and leisure-time PA decreased with age progression.
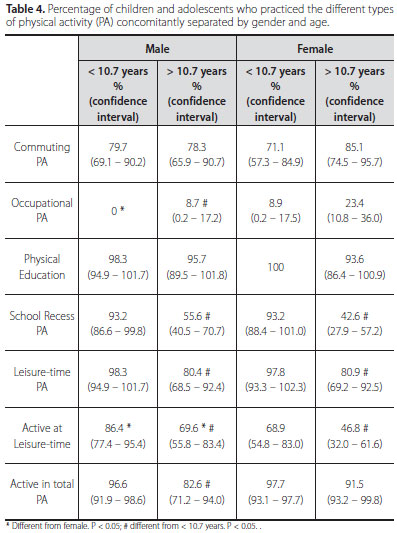
Practice of the different kinds of PA concomitantly separated by gender and age is presented in table 4. It is interesting to observe that the percentage difference between genders for occupational PA occurred only in the younger age group, while the percentage difference between genders for classification in active in leisure-time PA was evident in the two age groups. Concerning the comparisons between ages, only the boys presented increase in occupational PA and decrease in total PA when compared to the younger subjects, while the decrease of school recess and leisure-time PA as well as being classified as leisure-time active were observed in the two genders.
DISCUSSION
Cardiovascular risk
Taking the aims of this study concerning the CRF into consideration, the results showed that, in children and adolescents from the city of Muzambinho, despite the little previous knowledgement about the presence of CRF, there was considerable prevalence of these factors in this population, namely: overweight/obesity; high BP; high glycemia, high cholesterolemia and smoking. The prevalence of these CRF was the same between genders, but the prevalence of smokers, use of alcohol, altered BP and insufficient PA increased with age, especially in the boys.
The prevalence of the several CRF in children and adolescents varies greatly amongst the investigations(6-13,16). Differences in samples (age, origin and selection), applied methods (ways of measurement, instruments and measurement techniques) and abnormality criteria of the CRF are the main determinants of these variations.
In the present investigation, great part of the prevalence observed for the different CRF is within the variation range reported in the literature. The prevalence of overweight/obesity (18.8%) and altered BP (10.7%) were higher than what was reported by the brazilian Society of Cardiology(24), but lower than the one observed in Embu(13) (obesity= 27.2%) and in Campinas(7) (high BP= 28%). Prevalence of high cholesterolemia (14.5%) is also within the variation range observed(6,8,11,13) and the smoking prevalence was similar to what was reported in Maceió (2.4%)(12). It is worth mentioning that the smoking rate may have been underestimated due to the parents' presence during the interview. On the other hand, the prevalence of altered glycemia (4.5%) is above the reported one(13). However, few studies(6,13) assessed this variable and the ones which did used the laboratory measurement and not the digital puncture used in this study.
The main discrepancy between this study and the others was the low prevalence of sedentarism in Muzambinho (7.7%). In Ouro Preto, Pelotas and Maceió, the prevalence was 79.3, 58.2 and 93.5%, respectively (6,9,12). One factor for this discrepancy is the applied evaluation. In this study an interview on the many kinds of PA was used, and the previous studies applied a questionnaire(12) or only evaluated some kinds of PA(6,9,10,16); moreover, the sedentarism criteria vary between studies. Another aspect is the characteristics of the city. Muzambinho is a small city which does not have a good public transportation system and whose people walk to everywhere; moreover, it still cherishes the old habit of street play. Due to these peculiarities, an interview was the chosen instrument for the study because it allows a more detailed analysis of the practiced PA.
Likewise in other studies(6,8,11,12), the presence of CRF was not different between genders. In adult women and men the differences observed have been attributed to the presence of estrogen in women, which promotes cardiovascular protection(25). Since the estrogen levels in girls increase only in puberty, the low levels of this hormone in the studied female population (children and adolescents) may explain explains the lack of difference between genders.
Concerning the age, while the study performed in Bento Gonçalves-1997 did not demonstrate difference in the CRF prevalence among the youngest and the oldest(8), the present study, as well as the one from Ouro Preto-2009(6), demonstrated increase in some CRF with age. This difference may be partly due to the chronological time of the studies' execution, since youngsters nowadays are more exposed to less healthy life and eating habits and PA(26). This study did not evaluate the eating habits of the sample, but the PA during school recess and leisure-time decreased with age.
The early detection of CRF has important clinical implication. Thus, when CRF were detected, two actions were taken: 1) orientation on healthy habits, when the CRF were at borderline levels, or 2) recommendation of a medical visit, when the CRF were abnormal(18-22). Therefore, 33.7% of the subjects received guidance and 13.5% were sent to a medical visit.
PA practice
Considering PA practice, the results revealed that generally speaking, the youngsters from the city of Muzambinho were very active in all kinds of activity. However, the boys presented higher prevalence of leisure-time PA and the girls in occupational PA. Moreover, as age progressed, there was increase in the occupational activity, especially in boys, and there was decrease in PA during school recess and leisure-time, decreasing hence the prevalence of active subjects with age progression.
Commuting PA practice was fairly high (78.7%), which may be due to the size of the city. Likewise, participation in the official school PA (physical education classes - 97.0%) was very high, which is in agreement with other national studies - 99.1% in Pelotas(9) and 89.4% in Goiânia(10).
Practice of PA of choice, that is to say, those which the child do out of own will, such as during school recess (72.3%) and leisure-time (89.8%), was also high and higher than the one observed in other studies, such as leisure-time PA = 62.2% in Goiânia(10) and 40.4% in Florianópolis(16). Once again, a small city which still conserves old life habits, may explain this high prevalence, especially because the main PA reported was street play, as riding a bike, playing ball and playing children's circle game. These activities are fairly scarce in bigger cities.
PA practice was different between sexes, which may be related to cultural characteristics. Higher occupational PA in younger women may be explained by the fact that, traditionally, girls start to help moms in the housework from an early age. On the other hand, in small cities as well as in poorer populations, boys when entering adolescence start to help fathers with their work. These were the occupational PA reported in the study.
Considering the totality of PA, the prevalence of active children and adolescents (92.3%) was very high, being higher than the ones observed in a study with adolescents aged between 16 and 17 years from Florianópolis (69.4%)(16). This difference may be due to the age group studied, since practice of total PA decreased with age progression. Engagement in social appointments, such as the need to work and study, may have been responsible for the decrease of PA practice.
This study presented some limitations. The sample was defined based on a sample previously selected for another study and not on a random selection specific to this study. However, 4.8% of the target-population was investigated, which is very broad and surpasses other studies with this method.
CONCLUSION
It can be concluded that, except for sedentarism, prevalence of CRF is expressive in children and adolescents from Muzambinho. Such prevalence is not different between genders; however, it increases with age, especially concerning smoking, alcohol ingestion and high BP. Concerning PA practice, the children and adolescents from Muzambinho present great prevalence of practice in all kinds of PA. Nevertheless, this practice decreases with age, especially in the PA whose choice depends on self will, such as PA during school recess and leisure-time. This practice differs between genders, especially concerning occupational and leisure-time PA.
ACKNOWLEDGEMENTS
The authors thank the Secretaria Municipal de Educação e Saúde de Muzambinho for the support to this study; to the teachers and principals of the educational institutions which participated in this project; to the technicians, who participated in the data collection of the project; and to the children and their parents, who volunteered to this study. This study had financial supported by CNPq (478249/2007-1) and Pró-Reitoria de Graduação da USP (2009.1.9397.1.9).
REFERENCES
-
1Ministério da Saúde. Secretaria de Gestão Estratégica e Participativa - Departamento de Monitoramento e Avaliação da Gestão do SUS. http://www.datasus.gov.br 2006.
» link - 2. Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics-2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008;117:e25-146.
- 3. Cannon CP. Cardiovascular disease and modifiable cardiometabolic risk factors. Clin Cornerstone 2007;8:11-28.
- 4. Berenson GS, Srinivasan SR, Bao W, Newman WP, 3rd, Tracy RE, Wattigney WA. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. The Bogalusa Heart Study. N Engl J Med 1998;338:1650-6.
- 5. De Ferranti SD, Osganian SK. Epidemiology of paediatric metabolic syndrome and type 2 diabetes mellitus. Diab Vasc Dis Res 2007;4:285-96.
- 6. Candido AP, Benedetto R, Castro AP, Carmo JS, Nicolato RL, Nascimento-Neto RM, et al. Cardiovascular risk factors in children and adolescents living in an urban area of Southeast of Brazil: Ouro Preto Study. Eur J Pediatr 2009;168:1373-82.
- 7. Coronelli CL, de Moura EC. Hypercholesterolemia and its risk factors among schoolchildren. Rev Saude Publica 2003;37:24-31.
- 8. Gerber ZR, Zielinsky P. Risk factors for atherosclerosis in children: an epidemiologic study. Arq Bras Cardiol 1997;69:231-6.
- 9. Hallal PC, Bertoldi AD, Goncalves H, Victora CG. Prevalence of sedentary lifestyle and associated factors in adolescents 10 to 12 years of age. Cad Saude Publica 2006;22:1277-87.
- 10. Monego ET, Jardim PC. Determinants of risk of cardiovascular diseases in schoolchildren. Arq Bras Cardiol 2006;87:37-45.
- 11. Rodrigues AN, Moyses MR, Bissoli NS, Pires JG, Abreu GR. Cardiovascular risk factors in a population of Brazilian schoolchildren. Braz J Med Biol Res 2006;39:1637-42.
- 12. Silva MA, Rivera IR, Ferraz MR, Pinheiro AJ, Alves SW, Moura AA, et al. Prevalence of cardiovascular risk factors in child and adolescent students in the city of Maceio. Arq Bras Cardiol 2005;84:387-92.
- 13. Strufaldi MW, Silva EM, Puccini RF. Metabolic syndrome among prepubertal Brazilian schoolchildren. Diab Vasc Dis Res 2008;5:291-7.
- 14. Nunes Filho JR, Debastiani D, Nunes AD, Peres KG. Prevalence of cardiovascular risk factors in adults living in Luzerna, Santa Catarina, in 2006. Arq Bras Cardiol 2007;89:319-24.
- 15. Capilheira MF, Santos IS, Azevedo Jr MR, Reichert FF. Risk factors for chronic non-communicable diseases and the CARMEN Initiative: a population-based study in the South of Brazil. Cad Saude Publica 2008;24:2767-74.
- 16. Araújo EDS BN, Oliveira WF. Atividade física e hábitos alimentares de adolescentes de três escolas públicas de Florianópolis/SC. Rev Bras Cineantrop Desempenho Hum 2009;11:428-34.
- 17. Instituto Brasileiro de Geografia e Estatística. Ministério da Educação, Instituto Nacional de Estudos e Pesquisas Educacionais - INEP - Censo da Educação Superior. 2007.
-
18Centers for Disease Control and Prevention (CDC). www.cdc.gov./nchs/about/major/nhanes/growthcharts/clinical_charts.htl. 2000
» link - 19. McCarthy HD, Jarrett KV, Crawley HF. The development of waist circumference percentiles in British children aged 5.0-16.9 y. Eur J Clin Nutr 2001;55:902-7.
- 20. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2006;29:S43-8.
- 21. Sposito AC, Caramelli B, Fonseca FA, Bertolami MC, Afiune Neto A, Souza AD, et al. IV Brazilian Guideline for Dyslipidemia and Atherosclerosis prevention: Department of Atherosclerosis of Brazilian Society of Cardiology. Arq Bras Cardiol 2007;88:S2-19.
- 22. V Brazilian Guidelines in Arterial Hypertension. Arq Bras Cardiol 2007;89:e24-79.
- 23. American College of Sports Exercise. ACSM's Guidelines for Exercise Testing and Prescription. Philadelphia: Lippincott Williams and Wilkins; 2006.
- 24. Back Giuliano Ide C, Caramelli B, Pellanda L, Duncan B, Mattos S, Fonseca FH. I guidelines of prevention of atherosclerosis in childhood and adolescence. Arq Bras Cardiol 2005;85:S4-36.
- 25. Canderelli R, Leccesse LA, Miller NL, Unruh Davidson J. Benefits of hormone replacement therapy in postmenopausal women. J Am Acad Nurse Pract 2007;19:635-41.
- 26. Mendonça CP, dos Anjos LA. Dietary and physical activity factors as determinants of the increase in overweight/obesity in Brazil. Cad Saude Publica 2004;20:698-709.
Cardiovascular risk and physical activity practice in children and adolescents of Muzambinho/MG: influence of gender and age
Publication Dates
-
Publication in this collection
30 Nov 2011 -
Date of issue
Aug 2011