Abstracts
Introduction:
Fatigue during voluntary muscle contractions is a complex and multifactorial phenomenon associated with central changes and adaptations of the neuromuscular system.
Objective:
The purpose of this study was to evaluate the fatigue induced by intermittent successive extension of the knee between active and inactive university students. Method: Twenty healthy men (≥18 years), voluntarily participated in this study. To determine the maximum voluntary isometric contraction (MVIC) of the knee extensors muscle group, three sets of isometric contractions of knee extension were performed for five seconds with five minutes of rest between sets. The fatigue protocol consisted of 10 sets of 10 maximal concentric contractions of the extensor on the right knee, performed at 75% of MVIC with an interval of 45".
Results:
Significant reductions were observed (p<0.01), both in isometric strength (-34±4%) and the dynamic strength (-40 ± 3%). In addition, the slope of relationship strength x repetition was -0.79±0.07 Nm/repetitions and the magnitude of the effect reached -8.90.
Conclusion:
The protocol was useful to induce peripheral fatigue, although muscle strength is greater in the active group. In both isometric and dynamic action, muscle fatigue did not differ between groups.
muscle strength; dynamometer; knee; isometric contraction
Introdução:
A fadiga durante contrações musculares voluntárias é um fenômeno complexo e multifatorial, associado a alterações centrais e adaptações do sistema neuromuscular.
Objetivo:
Avaliar a fadiga induzida por sucessivas extensões intermitentes do joelho entre estudantes universitários ativos e inativos.
Métodos:
Vinte homens saudáveis (≥ 18 anos) participaram voluntariamente deste estudo. Para determinar a contração isométrica voluntária máxima (CIVM) do grupo muscular extensores do joelho, foi utilizado o valore médio de três contrações isométrias de extensão do joelho, durante cinco segundos, com cinco minutos de intervalo entre as séries. O protocolo de fadiga foi composto por 10 séries de 10 contrações concêntricas máximas sobre os extensores do joelho direito, realizadas a 75% da CIVM com intervalo de 45".
Resultados:
Reduções significativas (p < 0,01), tanto na força isométrica (-34 ± 4%) quanto na dinâmica (-40 ± 3%). Adicionalmente, a reta da relação força x repetição assumiu inclinação de -0,79 ± 0,07 Nm/repetições e a magnitude do efeito atingiu -8,9.
Conclusão:
O protocolo foi útil para induzir a fadiga periférica, embora a força muscular seja maior no grupo ativo. Tanto na ação isométrica quanto dinâmica, a fadiga muscular não diferiu entre os grupos.
dinamômetro; força muscular; joelho; contração isométrica
Introducción:
La fatiga durante las contracciones musculares voluntarias es un fenómeno complejo y multifactorial, asociado a los cambios centrales y adaptaciones del sistema neuromuscular.
Objetivo:
Evaluar la fatiga inducida por las extensiones sucesivas intermitentes de la rodilla entre los estudiantes universitarios activos e inactivos.
Métodos:
Veinte hombres sanos (≥ 18 años) participaron voluntariamente en este estudio. Para determinar la contracción isométrica voluntaria máxima (CIVM) del grupo de los músculos extensores de la rodilla, se realizaron tres contracciones isométricas de extensión de la rodilla, durante cinco segundos, con cinco minutos de descanso entre las series. El CIVM se determinó por la media de los tres intentos. El protocolo de la fatiga consistió en 10 series de 10 contracciones concéntricas máximas del extensor de la rodilla derecha, realizadas en el 75% de CIVM con un intervalo de 45".
Resultados:
Se observaron reducciones significativas (p < 0,01), tanto en la fuerza isométrica (-34 ± 4%) y la dinámica (-40 ± 3%). Además, la recta de la relación fuerza x repetición presentó inclinación de -0,79 ± 0,07 Nm/repeticiones y la magnitud del efecto alcanzó -8,9.
Conclusión:
El protocolo fue útil para inducir fatiga periférica, aunque la fuerza muscular es mayor en el grupo activo. En acción isométrica y dinámica, la fatiga muscular no difirió entre los grupos.
dinamómetro; fuerza muscular; rodilla; contracción isométrica
INTRODUCTION
Fatigue during voluntary muscular contractions is a complex and multifactorial phenomenon associated with both central changes and adaptations in the neuromuscular system. Generally, muscle fatigue is defined as a progressive and transient reduction of maximal force production induced by repeated muscle contractions independently of task type sustained or not11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46.,22. Enoka RM, Duchateau J. Muscle fatigue: what, why and how it influences muscle function. J Physiol. 2008;586(1):11-23..
Muscle fatigue activities may occur through either peripheral or central pathways, related to muscle failure in generating force at the level of the neuromuscular junction33. Gandevia SC. Spinal and supraspinal factors in human muscle fatigue. Physiol Rev. 2001;81(4):1725-89.. Central fatigue is related to a progressive reduction in voluntary activation that encompasses supraspinal and spinal circuitry44. Allen DG, Lännergren J, Westerblad H. Muscle cell function during prolonged activity: cellular mechanisms of fatigue. Exp Physiol. 1995;80(4):497-527.,55. Stackhouse S, Dean J, Lee S. Measurment of central activation failure of the quadriceps femoris in healthy adults. Muscle Nerve. 2000;23:1706-1712.. Neuromuscular fatigue during sustained static or dynamic contractions is an important limiting factor in the development of performance in many occupations including sports66. Iida N, Kaneko F, Aoki N, Shibata E. The effect of fatigued internal rotator and external rotator muscles of the shoulder on the shoulder position sense. J Electromyogr Kinesiol. 2014;24(1):72-7.,77. Ringheim I, Indahl A, Roeleveld K. Alternating activation is related to fatigue in lumbar muscles during sustained sitting. J Electromyogr Kinesiol. 2014;24(3):380-6.. There are different protocols able to promote muscular fatigue, however, Isokinetic fatigue protocols are88. Astorino TA, Terzi MN, Roberson DW, Burnett TR. Effect of two doses of caffeine on muscular function during isokinetic exercise. Med Sci Sports Exerc.2010;42(12):2205-10.
9. Carregaro RL, Gentil P, Brown LE, Pinto RS, Bottaro M. Effects of antagonist pre-load on knee extensor isokinetic muscle performance. J Sports Sci. 2011;29(3):271-8.-1010. Dipla K, Tsirini T, Zafeiridis A, Manou V, Dalamitros A, Kellis E, et al. Fatigue resistance during high-intensity intermittent exercise from childhood to adulthood in males and females. Eur J Appl Physiol. 2009;106(5):645-53. currently considered as a gold standard in clinical and sports approaches1111. Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43.
12. Theou O, Gareth JR, Brown LE. Effect of rest interval on strength recovery in young and old women. J Strength Cond Res. 2008;22(6):1876-81.-1313. Tiggelen DV, Coorevits P, Witvrouw E. The effects of a neoprene knee sleeve on subjects with a poor versus good joint position sense subjected to an isokinetic fatigue protocol. Clin J Sport Med. 2008;18(3):259-65..
Schwendner et al.1414. Schwendner KI, Mikesky AE, Holt WS Jr, Peacock M, Burr DB. Differences in muscle endurance and recovery between fallers and nonfallers, and between young and older women. J Gerontol A Biol Sci Med Sci. 1997;52(3):M155-60. reported that no fallers have greater muscle endurance (maximal knee extensions until force output, 50% of maximal voluntary contraction for two consecutive repetitions) than fallers (95 vs. 81 sec). Thus, muscle fatigability may be an important determinant of physical function, although few studies1111. Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43.,1313. Tiggelen DV, Coorevits P, Witvrouw E. The effects of a neoprene knee sleeve on subjects with a poor versus good joint position sense subjected to an isokinetic fatigue protocol. Clin J Sport Med. 2008;18(3):259-65.the rate-limiting precursor of carnosine, has been shown to elevate the muscle carnosine content. We aimed to investigate, using proton magnetic resonance spectroscopy (proton MRS were found that evaluated the fatigability on active and inactive subjects.
Paasuke et al.1515. Pääsuke M, Ereline J, Gapeyeva H. Neuromuscular fatigue during repeated exhaustive submaximal static contractions of knee extensor muscles in endurance-trained, power-trained and untrained men. Acta Physiol Scand. 1999;166(4):319-26. evaluated the neural and muscular strength changes during fatigue produced in repeated submaximal static contractions of knee extensors in endurance-trained, power-trained and untrained men. There were no changes on latency of patellar reflex after repeated exhaustive submaximal static contractions, which indicate no changes on sensory and motor nerve conduction characteristics. Differences in neuromuscular properties were observed in athletes, untrained individuals and endurance-trained athletes1515. Pääsuke M, Ereline J, Gapeyeva H. Neuromuscular fatigue during repeated exhaustive submaximal static contractions of knee extensor muscles in endurance-trained, power-trained and untrained men. Acta Physiol Scand. 1999;166(4):319-26.. According to the authors, the differences in strength may be attributed to the larger muscle cross-sectional area and type I/II fiber area ratios in athletes compared to untrained subjects or endurance trained athletes1616. Häkkinen K, Pakarinen A, Alen M, Kauhanen H, Komi PV. Neuromuscular and hormonal adaptations in athletes to strength training in two years. J Appl Physiol (1985). 1988;65(6):2406-12.,1717. Izquierdo M, Häkkinen K, Gonzalez-Badillo JJ, Ibáñez J, Gorostiaga EM. Effects of long-term training specificity on maximal strength and power of the upper and lower extremities in athletes from different sports. Eur J Appl Physiol. 2002;87(3):264-71..
Currently, physical inactivity had been considered a main risk factors for the development of chronic diseases and disability1818. Matsudo SM, Matsudo VR, Araújo T, Andrade D, Andrade E, Oliveira L. Nível de atividade física da população do Estado de São Paulo: análise de acordo com o gênero, idade, nível socioeconômico , distribuição geográfica e de conhecimento. Rev Bras Ciên Mov. 2002;10(4):41-50.,1919. González-Gross M, Meléndez A. Sedentarism, active lifestyle and sport: Impact on health and obesity prevention. Nutr Hosp. 2013;28(Suppl 5):89-98.. From an epidemiological point of view, studies2020. Pinheiro MC, Westphal MF, Akerman M. Equity in health according to reports by the Brazilian National Health Conferences since enactment of the 1988 Federal Constitution. Cad Saude Publica. 2005;21(2):449-58. have shown high rates of physical inactivity worldwide. Whereas these properties are strongly influential in muscle performance, non-active individuals have lower strength development, yet little is known about the fatigue of these individuals1111. Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43.. Considering this, the aim of the present study was to assess the ability of a protocol used to induce knee extension fatigue by multiple sets of intermittent Isokinetic exercise in both active and inactive adult subjects.
METHOD
Twenty adult healthy men (≥ 18 years), physically independent, voluntarily participated in this study (table 1). The International Physical Activity Questionnaire (IPAQ) was used to estimate physical activity levels. All participants were interviewed using the IPAQ short form. The questions were based on the preceding weeks physical activity levels, exploring the frequency and duration of physical activity including walking, moderate and vigorous physical exercise and sitting time. Individuals were considered active if they participated in physical activity for more than 150 minutes per week, and inactive if their participation levels were less than 150 minutes per week2121. World Health Organization. Glossary of health promotion terms. Geneva: World Health Organization/Division of Health Promotion, Educations and Communications/Health Education and Health Promotion Unit; 1998.. After IPAQ analyzes the subjects were distributed in inactive (n: 10) and active (n: 10) groups. Exclusion criteria were: positive clinical diagnosis of diabetes mellitus, smoker and musculoskeletal complications and/or cardiovascular alterations confirmed by medical evaluation. This study was approved by the University research ethics committee and all subjects read and signed an approved informed consent document (#786.066/2014).
The experimental design is presented in Figure 1. Subjects attended in the Laboratory four times to perform the Isokinetic evaluation by using a Biodex System 3 (Biodex, Inc., Shirley, NY). The validity coefficient of this instrument is 0.99, and the reproducibility measuring peak torque during knee extension was 0.92 at younger's subjects. Briefly, on the first day the subjects signed consent forms and completed the IPAQ. On the second day the anthropometric data (height, and weight) was evaluated. Third day the subjects were placed on the Isokinetic Dynamometer in a comfortable, upright, seated position for familiarization procedures. Straps were used to fix the thigh, pelvis, and trunk to prevent extraneous body movement. The axis of the dynamometer was aligned with the axis of right knee joint rotation. Arms were placed across the chest with hands grasping the straps. All subjects performed eight repetitions of submaximun concentric knee extension/flexion at 120o.s-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46.. The knee joint range of motion was 90 to 10º of knee flexion. The calibration of the Isokinetic Dynamometer was performed according to the specifications of the manufacturer before each test, and finally, on the fourth day the fatigue protocol was performed. All testing and experimental procedures were performed on the same time of day to exclude diurnal variation.
Anthropometric measurements: Height was measured by a Cardiomed (WCS model) stadiometer, with an accuracy of 115/220 cm. The measurement was performed with the cursor at an angle of 90° with respect to scale, with the patient in a standing position with feet together in contact with Stadiometer. The subjects were instructed to stay in inspiratory apnea and head parallel to the ground. Total body mass was measured by a calibrated Filizola electronic scale (Personal Line Model 150) with a 100g scale and a maximum capacity of 150 kg. Body mass index (BMI, kg/m2) was calculated using the equation BMI = weight/height22. Enoka RM, Duchateau J. Muscle fatigue: what, why and how it influences muscle function. J Physiol. 2008;586(1):11-23..
Fatigue protocol: The subjects performed a standardized warm-up comprising of five submaximal concentric and eccentric contractions at 120os-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46. in test position prior to data collection. Following the warm-up, subjects were asked to perform three maximal isometric voluntary contractions on the right knee extensors at 90° during five seconds to determine the maximal torque before and after the fatigue protocol. A rest interval of 45 seconds was prescribed between each set of muscular action, in order to minimize repetition effects especially during the post-test session. All test sessions were supervised by the same researcher. After the determination of maximal torque, all subjects performed a fatiguing protocol (concentric extension and eccentric flexion on the knee joint) comprising 10 sets of 10 maximal concentric contraction on right knee extensors at 75% of maximal isokinetic torque2222. Escamilla RF, Fleisig GS, Zheng N, Barrentine SW, Wilk KE,. Biomechanics of the knee during closed kinetic chain and open kinetic chainexercises. Med Sci Sports Exerc. 1998;30(4):556-69.. The angular velocity was 120os-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46., over range of motion of maximum flexion and extension, with 45 seconds of rest observed between sets2222. Escamilla RF, Fleisig GS, Zheng N, Barrentine SW, Wilk KE,. Biomechanics of the knee during closed kinetic chain and open kinetic chainexercises. Med Sci Sports Exerc. 1998;30(4):556-69.. During the test, all subjects were encouraged to exert maximal tension throughout the entire range of motion for all sets (Figure 1).
Statistical analyses
The D'Agostino-Pearson test was applied to Gaussian distribution analysis. The paired Student's t-test and One-way ANOVA followed by Kruskal-Wallis or Bonferroni's post-hoc test were performed to compare differences on fatigue protocol. Comparison analysis between inactive and active groups was performed by a repeated-measures ANOVA, followed by Kruskal-Wallis or Bonferroni's post-hoc test. Cohen's effect sizes (ES) were calculated, and evaluated based on the following criteria proposed by Rhea (2004) : < 0.50 trivial, 0.50 to 1.25 small, 1.25 to 1.9 moderate and > 2 large. An alpha of 0.05 was used to determine statistical significance. All data values were expressed as mean ± standard deviation. All analyses were performed using SPSS software (v 15.0; IBM, Armonk, NY, USA).
RESULTS
The anthropometric parameters are described in table 1. There were no significant differences for age and anthropometric parameters between groups as showed in table 1.
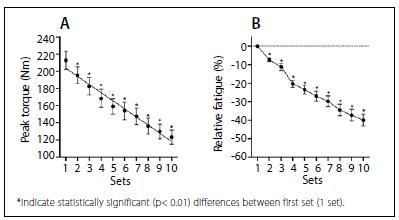
The absolute peak torque is observed in Figure 2. No participant had or reported any discomfort during the test sessions, however, both in maximal torque (Panel A: Before: 307 ±12, After: 209 ±13; Nm) with fatigability at -34 ± 4%. Additionally, a large effect size was observed in both to peak torque (-8.16).
Values expressed as the mean ± standard error deviation of isometric peak torque (panel A) and relative fatigue (Panel B).
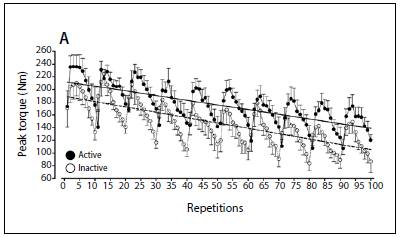
In Figure 3 shows a decline in torque production during repetitions of fatigue protocol. The values of the linear correlation coefficients (r) ranged value of 0.7505. The slopes range of maximum torque was -0.79 ± 0.07 Nm/repetitions.
Values expressed as mean ± SE. Panel A: decline in peak torque production in inactive and active after 10 sets of 10 concentric isokinetic mode knee extensions at 120º sec-1 with 45 seconds rest between sets (repetition one eliminated from analysis).
Considering the dynamic torque peak between absolute fatigue (Figure 4A) and relative fatigue (Figure 4B) analysis, there was a significant decrease (40 ± 3%, p< 0.001) through sets in relation to first set, and a large effect size to absolute fatigue (-8.9 %).
Significant differences (p<0.0001) were found between time spent weekly by physical activity (table 1) between groups. The differences on inactive and active isometric peak torque can be observed in Figure 5. The maximal torque (Figure 5A) of active group was higher (p <0.001) than the inactive group. After the applied muscle fatigue protocol, a significant decrease (p<0.01) on torque peak in both groups (Active: before: 330±13Nm, after: 220±13Nm; Inactive: before: 281±17Nm, after: 189± 22Nm) were found. There was no significant difference on fatigability (Figure 5B) between groups (Active: 35±6%; Inactive: 33±5%). In both groups a large effect size was observed after to torque peak (Active: 8.46; Inactive: 4.18).
Decline of absolute fatigue (Panel B) and relative fatigue (Panel C) after 10 sets of 10 concentric isokinetic mode knee extensions at 120º sec-1.
Values expressed as the mean ± standard error deviation of isometric peak torque (panel A) and relative fatigue (Panel B) of inactive and active subjects. Different letters indicate statistically significant (p< 0.05) differences between groups.
Considering the fatigue protocol load, there was no significant difference between groups (Inactive: 199±12 Nm, Active: 217±10 Nm, p =0.8765). Figure 6 shows the decrease in torque production during individual repetitions of the fatigue test. The values of linear correlation coefficients(r) ranged from 0.6951(active) to 0.7417(inactive). When was considered the slopes of maximum torque there was no significant differences through sets between groups (inactive: -0.84 ±0.24Nm/repetitions; and, active: -0.73 ±0.19 Nm/repetitions; p =0.7401).
Values expressed as mean ± SE. Panel A: decline in peak torque production in inactive and active after 10 sets of 10 concentric isokinetic mode knee extensions at 120º sec-1 with 45 seconds rest between sets (the first repetition was eliminated from analysis) of inactive and active subjects.
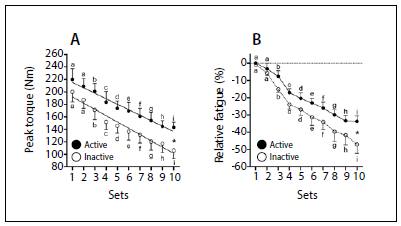
After absolute fatigue analysis (Figure 7A), there were significant (p< 0.001), decreases on dynamic peak torque through sets in both groups. However, there was significant differences between the groups (inactive: 106 ±13Nmand active: 143 ± 8Nm, p <0.001) only at 10º set between. Although, there was found high values of relative fatigue (Figure 7B) on inactive group (-46±5%) related to active group (-31±4%), indicating that both groups presented same tolerance to fatigue. The analysis of the effect size to both inactive (7.23) and active (9.25) groups presented values of great influence.
Decline of absolute fatigue (Panel A) and relative fatigue (Panel B) after 10 sets of 10 concentric isokinetic mode knee extensions at 120º sec-1 of active and inactive subjects. Different letters indicate statistically significant (p< 0.05) differences between sets. * statistically significant (p< 0.01) differences between groups.
DISCUSSION
The major findings of the present study were: 1) a reliable peripheral fatigue exercise protocol in healthy adults; 2) active adults were more able to develop muscle strength than inactive subjects; 3) although active subjects develop strength there is no difference between the fatigue responses of dynamic muscle action between groups.
Our data in isometric and dynamic fatigue protocol presented in general association to physical activity level respectively were lower than other studies88. Astorino TA, Terzi MN, Roberson DW, Burnett TR. Effect of two doses of caffeine on muscular function during isokinetic exercise. Med Sci Sports Exerc.2010;42(12):2205-10.
9. Carregaro RL, Gentil P, Brown LE, Pinto RS, Bottaro M. Effects of antagonist pre-load on knee extensor isokinetic muscle performance. J Sports Sci. 2011;29(3):271-8.
10. Dipla K, Tsirini T, Zafeiridis A, Manou V, Dalamitros A, Kellis E, et al. Fatigue resistance during high-intensity intermittent exercise from childhood to adulthood in males and females. Eur J Appl Physiol. 2009;106(5):645-53.-1111. Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43.,2323. Rawson ES. Enhanced fatigue resistence in older adults during repeated sets of intermittent contractions. J Strength Cond Res. 2010;24(1):251-256. found variations between 50% to 86%. The differences presented in our study might be explained by the contractile action that is given by the eccentric and concentric actions promoted by skeletal muscle responsible to knee extension, moreover24.
Some parameters could be clarifying this large difference between protocols. The first point to address is protocol duration. Studies have indicated variation in time of 210 seconds99. Carregaro RL, Gentil P, Brown LE, Pinto RS, Bottaro M. Effects of antagonist pre-load on knee extensor isokinetic muscle performance. J Sports Sci. 2011;29(3):271-8., 270 seconds88. Astorino TA, Terzi MN, Roberson DW, Burnett TR. Effect of two doses of caffeine on muscular function during isokinetic exercise. Med Sci Sports Exerc.2010;42(12):2205-10. and 390 seconds1111. Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43.. In our study, the protocol length was 505 seconds corresponding to 28% over time of1111. Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43. data with highest term realization, additionally this fact could be able to promote a higher metabolic stress. The second point corresponds to the angular velocity used on studies, such as Carregaro et al.99. Carregaro RL, Gentil P, Brown LE, Pinto RS, Bottaro M. Effects of antagonist pre-load on knee extensor isokinetic muscle performance. J Sports Sci. 2011;29(3):271-8. that used the angular velocity of 60° s-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46. and 180° s-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46. with three sets of 10 repetitions and rest of 60 seconds between sets found a peak torque drop by 20.8% and 13.3%. Astorino et al.88. Astorino TA, Terzi MN, Roberson DW, Burnett TR. Effect of two doses of caffeine on muscular function during isokinetic exercise. Med Sci Sports Exerc.2010;42(12):2205-10. used the angular velocity of 180° s-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46., using two sets of 40 repetitions totaling a total work of 80 repetitions with three minute rest between sets found reduction (35.6%) similar to our study. Third point, the total volume of work performed could be considered as an important factor to induce muscular fatigue. Rawson2323. Rawson ES. Enhanced fatigue resistence in older adults during repeated sets of intermittent contractions. J Strength Cond Res. 2010;24(1):251-256. used the angular velocity of 180° s-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46. in 30 repetitions by one minute rest, totalizing 150 repetitions, founded a drop at 45% of peak torque. Mercer et al.2525. Mercer TH, Gleeson NP, Wren K. Influence of prolonged intermittent high-intensity exercise on knee flexor strength in male and female soccer players. Eur J Appl Physiol. 2003;89(5):506-8. used the angular velocity of 60° s-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46. with one series with five repetitions fell by 22.3%, showing a decrease in the total volume of working, but with exponentially increased overhead. In this way, it is possible that protocols with higher total work volume are more efficient at this angular speed higher than 120° s-11. Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46., therefore the protocols tend to reach the approximate time of 10 minutes. Metabolically, it is possible to speculate that the time element in these protocols has glycolitic predominance.
To our knowledge, there is only one study1515. Pääsuke M, Ereline J, Gapeyeva H. Neuromuscular fatigue during repeated exhaustive submaximal static contractions of knee extensor muscles in endurance-trained, power-trained and untrained men. Acta Physiol Scand. 1999;166(4):319-26. available in the scientific literature that evaluated the influence of physical activity level and neuromuscular fatigue development in healthy individuals. In our study, active individuals presented higher levels of muscle strength in both isometric and dynamic protocols compared to inactive. However, there were no differences in fatigue process between the active (Isometric: 35 ± 6%; Dynamic: 31 ± 4%) and inactive (Isometric: -33 ± 5%; Dynamic: -46 ± 5%) groups.
Similar results were found in other studies2626. Klass M, Baudry S, Duchateau J. Voluntary activation during maximal contraction with advancing age: a brief review. Eur J Appl Physiol. 2007;100(5):543-51. compared young and old subjects strength and fatigue in muscle, showing that young people produce higher levels of forces in elderly subjects, with no differences on fatigue levels. A possible mechanism for this may be to address central and peripheral muscular activation independently of age and sex2727. Russ DW, Towse TF, Wigmore DM, Lanza IR, Kent-Braun JA. Contrasting influences of age and sex on muscle fatigue. Med Sci Sports Exerc. 2008;40(2):234-41.. We believe an explanation of no differences on muscular fatigue found in this study may be related to central and peripheral muscle activation, taking into account differences between activation of muscle fibers, also in the development of muscle fibers and biochemical changes2727. Russ DW, Towse TF, Wigmore DM, Lanza IR, Kent-Braun JA. Contrasting influences of age and sex on muscle fatigue. Med Sci Sports Exerc. 2008;40(2):234-41.
28. Ascensão A, Magalhães J, Oliveira J, Duarte J, Soares J. Fisiologia da fadiga muscular. Delimitação conceptual, modelos de estudo e mecanismos de fadiga de origem central e periférica. Rev Portug Ciênc Desp. 2003;3(1):108-23.-2929. Olkoski MM, Matheus SC, Alexandre F. Respostas bioquímicas e físicas ao treinamento realizado dentro e fora da água em atletas de futsal. Motriz, Rio Claro. 2013;19(2):432-40..
During isometric exercise with a constant submaximal load, there is a time-dependent increase in electromyographic signal. An increase may be due to increased peak amplitude, the change in motor unit recruitment order or increasing motor neuron firing rates, that could be used as a compensation factor to the loss of motor function. In this way, Paasuke et al.1515. Pääsuke M, Ereline J, Gapeyeva H. Neuromuscular fatigue during repeated exhaustive submaximal static contractions of knee extensor muscles in endurance-trained, power-trained and untrained men. Acta Physiol Scand. 1999;166(4):319-26. found no differences on reflex latency patellar during isometric contractions indicating no changes in sensory and motor nerve conduction during submaximal protocol isometric fatigue knee extensors in power athletes, strength and untrained subjetcs. Considering the differences present between active and non-active individuals, we can comment on the muscle and neural properties already observed between athletes and non athletes1111. Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43.. Thus, it is possible to consider that athletes and active individuals within its particularities, have greater transverse muscular segment1616. Häkkinen K, Pakarinen A, Alen M, Kauhanen H, Komi PV. Neuromuscular and hormonal adaptations in athletes to strength training in two years. J Appl Physiol (1985). 1988;65(6):2406-12., greatest difference in the ratio of
type I / II fibers than non-trained individuals and resistance athletes22. Enoka RM, Duchateau J. Muscle fatigue: what, why and how it influences muscle function. J Physiol. 2008;586(1):11-23.. Similar results were found by Leme et al.3030. Leme V, Panissa G, Julio UF. Effects of interval time between high-intensity intermittent aerobic exercise on strength performance: analysis in individuals with different training background. J Hum Sport Exerc. 2012;7(4):815-25., their study observed that in individuals with high aerobic capacity lower strength maintenance in high intensity activities, may be due to typing predominance of muscle fiber.
Regarding the dynamic actions, our data are similar to the study of Blacker et al.3131. Blacker SD, Fallowfield JL, Bilzon JL, Willems ME. Neuromuscular function following prolonged load carriage on level and downhill gradients. Aviat Space Environ Med. 2010;81(8):745-53. being shown that individuals who performed strength training showed marked decrease in torque percentage (16.5%), in the eccentric phase, when compared with groups that performed predominantly aerobic exercises (7.2%) and compared to physically active individuals to presented drop was 6.5%. Leme et al.3030. Leme V, Panissa G, Julio UF. Effects of interval time between high-intensity intermittent aerobic exercise on strength performance: analysis in individuals with different training background. J Hum Sport Exerc. 2012;7(4):815-25. presented results showing subjects with different types of training completed the same amount of total work during the sessions of strength training. The authors considered that endurance athletes have greater resistance to fatigue compared to sprinters, wrestlers and weightlifters. This information corroborates to our dynamic muscle strength parameters that showed the same fatigue level but with lower peak force when compared to the inactive group. Additionally, the time protocol could be considered as an important parameter to promote metabolic substrate accumulation or be able to increase acidosis, indicating impairment on muscular performance during a dynamic protocol. It is therefore unclear from the scientific literature, how fitness status or just physical activity levels can influence the kinetics of blood lactate concentrations, or how the peak concentrations that occur during or immediately post exercise could contribute to peripheral acute fatigue.
CONCLUSION
The present study demonstrated that physically active adults presented higher strength than inactive subjects. Additionally, the fatigue protocol applied in this study is useful to promote acute peripheral muscle fatigue on isometric and dynamic strength in both groups. On the other hand, the fatigue slope was similar in both groups suggesting that neuromuscular responses were affected by the fatigue protocol due to specific metabolic pathways and neurological profile of subjects.
ACKNOWLEDGEMENT
The authors thank CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) fellowships addressed to F. S. Suzuki. The fund providers had no role in decision to publish and preparation of the paper.
REFERENCES
-
1Bigland-Ritchie B, Johansson R, Lippold OC, Smith SW. Changes in motoneurone firing rates during sustained maximal voluntary contractions. J Physiol. 1983;340:335-46.
-
2Enoka RM, Duchateau J. Muscle fatigue: what, why and how it influences muscle function. J Physiol. 2008;586(1):11-23.
-
3Gandevia SC. Spinal and supraspinal factors in human muscle fatigue. Physiol Rev. 2001;81(4):1725-89.
-
4Allen DG, Lännergren J, Westerblad H. Muscle cell function during prolonged activity: cellular mechanisms of fatigue. Exp Physiol. 1995;80(4):497-527.
-
5Stackhouse S, Dean J, Lee S. Measurment of central activation failure of the quadriceps femoris in healthy adults. Muscle Nerve. 2000;23:1706-1712.
-
6Iida N, Kaneko F, Aoki N, Shibata E. The effect of fatigued internal rotator and external rotator muscles of the shoulder on the shoulder position sense. J Electromyogr Kinesiol. 2014;24(1):72-7.
-
7Ringheim I, Indahl A, Roeleveld K. Alternating activation is related to fatigue in lumbar muscles during sustained sitting. J Electromyogr Kinesiol. 2014;24(3):380-6.
-
8Astorino TA, Terzi MN, Roberson DW, Burnett TR. Effect of two doses of caffeine on muscular function during isokinetic exercise. Med Sci Sports Exerc.2010;42(12):2205-10.
-
9Carregaro RL, Gentil P, Brown LE, Pinto RS, Bottaro M. Effects of antagonist pre-load on knee extensor isokinetic muscle performance. J Sports Sci. 2011;29(3):271-8.
-
10Dipla K, Tsirini T, Zafeiridis A, Manou V, Dalamitros A, Kellis E, et al. Fatigue resistance during high-intensity intermittent exercise from childhood to adulthood in males and females. Eur J Appl Physiol. 2009;106(5):645-53.
-
11Derave W, Ozdemir MS, Harris RC, Pottier A, Reyngoudt H, Koppo K, et al. Beta-Alanine supplementation augments muscle carnosine content and attenuates fatigue during repeated isokinetic contraction bouts in trained sprinters. J Appl Physiol (1985). 2007;103(5):1736-43.
-
12Theou O, Gareth JR, Brown LE. Effect of rest interval on strength recovery in young and old women. J Strength Cond Res. 2008;22(6):1876-81.
-
13Tiggelen DV, Coorevits P, Witvrouw E. The effects of a neoprene knee sleeve on subjects with a poor versus good joint position sense subjected to an isokinetic fatigue protocol. Clin J Sport Med. 2008;18(3):259-65.
-
14Schwendner KI, Mikesky AE, Holt WS Jr, Peacock M, Burr DB. Differences in muscle endurance and recovery between fallers and nonfallers, and between young and older women. J Gerontol A Biol Sci Med Sci. 1997;52(3):M155-60.
-
15Pääsuke M, Ereline J, Gapeyeva H. Neuromuscular fatigue during repeated exhaustive submaximal static contractions of knee extensor muscles in endurance-trained, power-trained and untrained men. Acta Physiol Scand. 1999;166(4):319-26.
-
16Häkkinen K, Pakarinen A, Alen M, Kauhanen H, Komi PV. Neuromuscular and hormonal adaptations in athletes to strength training in two years. J Appl Physiol (1985). 1988;65(6):2406-12.
-
17Izquierdo M, Häkkinen K, Gonzalez-Badillo JJ, Ibáñez J, Gorostiaga EM. Effects of long-term training specificity on maximal strength and power of the upper and lower extremities in athletes from different sports. Eur J Appl Physiol. 2002;87(3):264-71.
-
18Matsudo SM, Matsudo VR, Araújo T, Andrade D, Andrade E, Oliveira L. Nível de atividade física da população do Estado de São Paulo: análise de acordo com o gênero, idade, nível socioeconômico , distribuição geográfica e de conhecimento. Rev Bras Ciên Mov. 2002;10(4):41-50.
-
19González-Gross M, Meléndez A. Sedentarism, active lifestyle and sport: Impact on health and obesity prevention. Nutr Hosp. 2013;28(Suppl 5):89-98.
-
20Pinheiro MC, Westphal MF, Akerman M. Equity in health according to reports by the Brazilian National Health Conferences since enactment of the 1988 Federal Constitution. Cad Saude Publica. 2005;21(2):449-58.
-
21World Health Organization. Glossary of health promotion terms. Geneva: World Health Organization/Division of Health Promotion, Educations and Communications/Health Education and Health Promotion Unit; 1998.
-
22Escamilla RF, Fleisig GS, Zheng N, Barrentine SW, Wilk KE,. Biomechanics of the knee during closed kinetic chain and open kinetic chainexercises. Med Sci Sports Exerc. 1998;30(4):556-69.
-
23Rawson ES. Enhanced fatigue resistence in older adults during repeated sets of intermittent contractions. J Strength Cond Res. 2010;24(1):251-256.
-
24Enoka RM, Stuart DG. Neurobiology of muscle fatigue. J Appl Physiol (1985).1992;72(5):1631-48.
-
25Mercer TH, Gleeson NP, Wren K. Influence of prolonged intermittent high-intensity exercise on knee flexor strength in male and female soccer players. Eur J Appl Physiol. 2003;89(5):506-8.
-
26Klass M, Baudry S, Duchateau J. Voluntary activation during maximal contraction with advancing age: a brief review. Eur J Appl Physiol. 2007;100(5):543-51.
-
27Russ DW, Towse TF, Wigmore DM, Lanza IR, Kent-Braun JA. Contrasting influences of age and sex on muscle fatigue. Med Sci Sports Exerc. 2008;40(2):234-41.
-
28Ascensão A, Magalhães J, Oliveira J, Duarte J, Soares J. Fisiologia da fadiga muscular. Delimitação conceptual, modelos de estudo e mecanismos de fadiga de origem central e periférica. Rev Portug Ciênc Desp. 2003;3(1):108-23.
-
29Olkoski MM, Matheus SC, Alexandre F. Respostas bioquímicas e físicas ao treinamento realizado dentro e fora da água em atletas de futsal. Motriz, Rio Claro. 2013;19(2):432-40.
-
30Leme V, Panissa G, Julio UF. Effects of interval time between high-intensity intermittent aerobic exercise on strength performance: analysis in individuals with different training background. J Hum Sport Exerc. 2012;7(4):815-25.
-
31Blacker SD, Fallowfield JL, Bilzon JL, Willems ME. Neuromuscular function following prolonged load carriage on level and downhill gradients. Aviat Space Environ Med. 2010;81(8):745-53.
Publication Dates
-
Publication in this collection
Mar-Apr 2016
History
-
Received
31 May 2015 -
Accepted
07 Dec 2016