Abstracts
The adult T-cell leukemia/lymphoma (ATLL) is a rare type of lymphoma caused by human T lymphotropic virus type 1 (HTLV-1). The clinical manifestations include cutaneous lesions, adenopathies, myelopathy/ tropical spastic paraparesis, uveitis, ophthalmological diseases, leukocytosis with lymphocytosis and atypical lymphocytes. The main objective of this study was to report a case of a female patient with ATLL, a farmer with leukocytosis, lymphocytosis, bilateral ocular erythema, cervical lymphadenopathy, in the abdominal visceromegalies and with positive markers for T-cell lymphocytes (CD45, CD2, CD3, CD5, CD4 and CD25). Although ATLL is a rare disease, its delayed diagnosis may lead to serious complications and fatal outcome.
T cell leukemia; flow cytometry; human T-lymphotropic virus 1; chronic lymphoproliferative disorders
O linfoma/leucemia de células T do adulto (ATLL) é um tipo raro de linfoma causado pelo vírus T-linfotrópico humano tipo I (HTLV-1). O quadro clínico inclui lesões de pele, adenomegalias, mielopatia/paraparesia espástica tropical, uveíte, doença oftalmológica, leucocitose com linfocitose e linfócitos atípicos. O objetivo deste estudo foi relatar o caso de uma paciente com ATLL, agricultora, com leucocitose, linfocitose, eritema ocular bilateral, linfadenopatia cervical, sem visceromegalias abdominais e com marcadores positivos para linfócitos T (CD45, CD2, CD3, CD5, CD4 e CD25). Embora a ATLL seja uma doença rara, a demora no seu diagnóstico pode levar a sérias complicações e ocasionar a morte do paciente.
leucemia de células T; citometria de fluxo; vírus linfotrópico de células T humanas tipo 1; neoplasias linfoproliferativas crônicas
CASE REPORT
Case report of adult T-cell lymphoma/leukemia
Relato de caso de linfoma/leucemia de células T do adulto
Lacy Cardoso de Brito JuniorI; Euzamar Gaby RochaII; Sérgio Antônio Batista dos SantosIII; Larissa Tatiane Martins FrancêsIV
IDoctor in Medical Science with emphasis on Experimental Pathology from Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (FMRPUSP); head of the Graduation and Post Graduation Service of Fundação Hospital de Clínicas Gaspar Viana
IISpecialist in Hematology from Universidade Estadual do Rio de Janeiro (UERJ); hematologist at the Fundação Centro de Hemoterapia e Hematologia do Pará (HEMOPA)
IIISpecialist in Hemotherapy from Universidade do Estado do Pará; doctor at the Hemotherapy and Hematology HEMOPA
IVSpecialist in Hematology from Santa Casa de Misericórdia de São Paulo; hematologist at the Hemotherapy and Hematology HEMOPA
Mailing address Mail address: Lacy Cardoso de Brito Junior Universidade Federal do Pará Instituto de Ciências Biológicas Laboratório de Patologia Geral Imunopatologia e Citologia Av. Augusto Corrêa, 01 - Guamá CEP: 66075-900 - Belém-PA, Brazil Phone.: (091) 3201-7565 e-mail: lcdbrito@ufpa.br ou lcdbrito@bol.com.br
ABSTRACT
The adult T-cell leukemia/lymphoma (ATLL) is a rare type of lymphoma caused by human T lymphotropic virus type 1 (HTLV-1). The clinical manifestations include cutaneous lesions, adenopathies, myelopathy/ tropical spastic paraparesis, uveitis, ophthalmological diseases, leukocytosis with lymphocytosis and atypical lymphocytes. The main objective of this study was to report a case of a female patient with ATLL, a farmer with leukocytosis, lymphocytosis, bilateral ocular erythema, cervical lymphadenopathy, in the abdominal visceromegalies and with positive markers for T-cell lymphocytes (CD45, CD2, CD3, CD5, CD4 and CD25). Although ATLL is a rare disease, its delayed diagnosis may lead to serious complications and fatal outcome.
Key words: T cell leukemia; flow cytometry; human T-lymphotropic virus 1; chronic lymphoproliferative disorders.
RESUMO
O linfoma/leucemia de células T do adulto (ATLL) é um tipo raro de linfoma causado pelo vírus T-linfotrópico humano tipo I (HTLV-1). O quadro clínico inclui lesões de pele, adenomegalias, mielopatia/paraparesia espástica tropical, uveíte, doença oftalmológica, leucocitose com linfocitose e linfócitos atípicos. O objetivo deste estudo foi relatar o caso de uma paciente com ATLL, agricultora, com leucocitose, linfocitose, eritema ocular bilateral, linfadenopatia cervical, sem visceromegalias abdominais e com marcadores positivos para linfócitos T (CD45, CD2, CD3, CD5, CD4 e CD25). Embora a ATLL seja uma doença rara, a demora no seu diagnóstico pode levar a sérias complicações e ocasionar a morte do paciente.
Unitermos: leucemia de células T; citometria de fluxo; vírus linfotrópico de células T humanas tipo 1; neoplasias linfoproliferativas crônicas.
INTRODUCTION
The adult T-cell leukemia/lymphoma (ATLL) is a mature T cell neoplasia commonly associated with infections caused by human T lymphotropic virus type 1 (HTLV-1)(2, 12, 15). Nevertheless, only 2% to 5% of infected patients ultimately develop ATLL(2), mainly in regions where HTLV-1 infections are endemic, namely in Japan(7, 12). In addition to ATLL, other diseases are connected with HTVL-1 infection such as mielopathy/tropical spastic paraparesis (HAM/TSP), uveitis and infectious dermatitis during childhood(12). Despite the fact that HTLV-1 infections are regarded as endemic in Brazil and highly prevalent in Bahia, Pernambuco and Pará, HTVL-1 and HTVL-2 infections are present in all regions, though with low prevalence among the general population(3, 9).
ATLL pathogenesis, though not totally elucidated in humans, is linked with CD4T cell and HTLV-1 infections(17) and some risk factors such as the following : (1) gender, with higher prevalence among women due to their higher vulnerability to sexual transmission(4); (2) heredity, linked with higher genetic predisposition to the development of this type of leukemia(18); (3) direct correlation between the increase in atypical lymphocytes, proviral load and the aggravation of clinical symptoms(6, 11, 13); (4) low levels of serum HTLV-1 TAX antibody (escape mechanism of infected cells), inasmuch as in normal conditions TAX is able to cause intracellular changes in CD4+ lymphocytes and induce immunological response(5, 10, 16); (5) HTVL-1 vertical transmission via breast-feeding(1, 2, 18).
The clinical and laboratory features associated with ATLL are the following: skin lesions, adenopathies, hypercalcemia, increase in lactate dehydrogenase (LDH). alteration in the number of leucocytes in peripheral blood with presence of atypical lymphocytes (flower cells), increase in anti-HTLV-1 antibody, and presence of neoplastic T lymphoid cells with immunophenotype connected with CD2+,CD3+,CD4+ e CD25+(2, 3, 8).
Therefore, the objectives of the present investigation were to report the case of a patient with ATLL and review some aspects related to this disease.
CASE REPORT
A 53-year-old female patient, a farmer from Santa Izabel-Pará, was admitted at the Fundação Centro de Hemoterapia e Hematologia do Pará (HEMOPA) on July 29 2010. The patient presented clinical history of ophthalmological problem, erythema with tearing and sensation of foreign body in eye, finger and toe nails had fallen off, cyanosis of extremities, swollen right ankle and breast discharge that remained clinically unsolved for over 19 years. Physical exam revealed cyanosis of extremities (feet and hands, bilateral ocular erythema with opacification of the right cornea, painless bilateral cervical lymphadenopathy with no visceromegalies or cutaneous lesions.
Clinical exams were performed at admittance on July 15 2010 and patient's return was scheduled for July 30. The exams yielded the following results: (1) hemogram - erythrocytes = 4.54 million/mm3; hemoglobin = 12.8 g/dl; hematocrit = 37.5%; red cell distribution width (RDW) = 15.8%; platelets = 207 thousand/mm3, leucocytes = 38,000/mm3, with 86% of lymphocytes from which 15% showed moderate nucleocytoplasmatic relation, pleomorphic nuclei (tetra-lobed nuclei) and basophilic cytoplasm without granules (Figure 1); (2) negative serology for Chagas disease, human immunodeficiency virus (HIV) 1 and 2, syphilis and hepatitis; (3) tests for antinuclear factor, Ro/SS-A and La/SS-B autoantibodies, anti-deoxyribonucleic acid, rheumatoid factor and antistreptolysin O were also non reactive; (4) negative C reactive protein (CRP); (5) negative direct Coombs; (6) negative lupus anticoagulant. On the same day of collection, other exams were required (hemogram, myelogram and immunophenotyping by flow cytometry) in order to exclude the diagnostic possibility of chronic lymphocytic leukemia/small lymphocytic lymphoma.
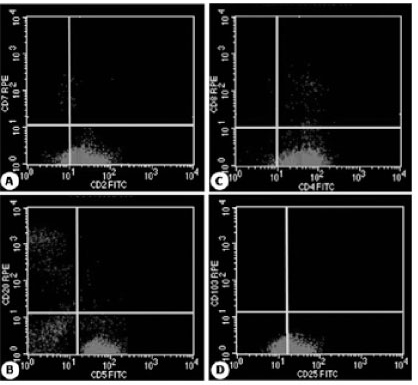
- Histograms of immunophenotyping by flow cytometry with mature T lymphocyte populations (A) CD2+ and negative for CD7; (B) CD5+ and negative for CD20; (C) CD4+ and negative for CD8; (D) CD25+ and negative for CD103. RPE: R-phycoerythrin; FITC: fluorescein.
On September 22 2010 the exams yielded the following results: (1) hemogram - erythrocytes = 4.37 million/mm3; hemoglobin = 13.8 g/dl; hematocrit = 38.8%; RDW = 16.6%; platelets = 201 thousand/mm3; leucocytes = 44,700/mm3 with 83% of lymphocytes; (2) myelogram with normal cellularity for granulocytic, erythrocytic and megacariocytic activity and hyper cellularity of lymphoplasmacytic activity with prevalence of mature lymphocytes with cleaved nuclei, suggesting lymphoproliferative neoplasia; (3) immunophenotyping by flow cytometry of peripheral blood showed the presence of 69% of mature T lymphocytes with CD45, CD5, CD2, CD25, CD4 and CD3 expression in the membrane and in the cytoplasm and absence of CD7 and CD8 expression (Figure 2), suggesting ATLL. Serologic analysis (reactive) and PCR (positive) were recommended for HTLV-1 and 2. On November 08 2010 the patient was referred to the Hematology center of Ophir Loyola Hospital for chemotherapeutic treatment.
- Photomicrographs showing pleomorphic morphology (tetra-lobed) of T lymphocyte nuclei (flower cell), which are associated with HTVL infection and are observed in the peripheral blood HTLV: Human T-lymphotropic virus.
As this is a retrospective study, the clinical case was referred to the Ethical Research Committee of HEMOPA Foundation for pre-informed consent according to standard procedure in this area of investigation.
DISCUSSION
According to the medical literature, ATLL diagnosis is rare among chronic lymphoproliferative neoplasias. It affects individuals in their third decade of life, mainly between 40 to 60 years of age. As it has clinical features that are similar to other chronic lymphoproliferative neoplasias, its diagnosis remains underestimated in several counties, including Brazil(14).
Cutaneous lesions, adenopathies, ocular ulcerations and changes in the number of leucocytes with lymphocytosis in peripheral blood are some of the most frequent features of ATLL and other chronic lymphoproliferative neoplasias(2, 15).
At the present study, in accordance with literature data(2, 8, 10), this pathology was associated with the female gender, after the third decade of live, with clinical history of leukocytosis, lymphocytosis and presence of atypical lymphoid shapes (flower cell).
Clinical laboratory exams commonly altered by ATLL are the following: calcium dosage and lactic dehydrogenase (DHL), which are relevant to the clinical classification of ATLL (acute, chronic, smoldering or lymphoma type)(2, 3, 8, 12); uric acide and Beta 2 microglobulin, albumin, renal and hepatic functions, which are import to assess tumor load; ophthalmologic exam to assess the causes of ocular erythema and opacification of the right cornea; radiographic exams to evaluate lytic bone lesions; abdominal ultrasonography. However, they were not carried out at primary service inasmuch as the initial diagnostic hypothesis was not ATLL. Following the positive sorology, PCR for HTLV-1 and 2 and immunofenotyping by flow cytometry, the patient was immediately referred to specialized treatment, hence limiting the performance of complementary exams such as the ones above mentioned, which are major to the characterization and classification of ATLL. Moreover, it was not possible to collect further information pertaining the patient's treatment and clinical evolution.
The reported case draws attention due to the long period between the beginning of clinical symptomatology and definite diagnosis. Furthermore, it demonstrates the importance of diagnosing this pathology in view of varied clinical approach and confirmatory triage exams for HTLV-1 and 2 infection, which is endemic in Brazil, though with low prevalence among the general population.
According to studies conducted with blood donors from blood centers in Brazil who were diagnosed with HTVL-1 and 2, the prevalence of HTVL-1 varies from 0.07% to 0.13% and HTVL-2 from 0.02% to 0.03%(9, 14). Similar data were observed in the State of Pará(9, 14), where the patient resides.
By characterizing T cells with CD2, mCD3, CD5 and CD4 expression and CD38, CD30+/-, HLADr and CD25(3, 8, 12, 14, 15) cellular activation antigens, the use of immunophenotyping by flow cytometry in association with clinical and morphologic data has proved to be an invaluable tool to the differential diagnosis of ATLL. Similarly, the data observed in the case report corroborated the presence of atypical T lymphocytes with CD45, CD2 and CD3 expressions (membrane and cytoplasm) as well as CD5, CD4 and CD25.
Thus this case report evinces the vulnerability of the epidemiological State follow-up system as to cases diagnosed as ATLL insofar as these patients are diagnosed with chronic lymphoproliferative neoplasia and not with HTLV-1 infection that evolved to ATLL. Family investigation (husband, children and grandchildren) is also required in order to assess their contamination by the same agent. In accordance with the medical literature, a higher genetic predisposition to ATLL among relatives infected by HTLV-18 and 10 has been proved.
ACKNOWLEDGMENTS
We would like to thank Dr. Mylner O. F. Souza sincerely for the technical support to obtain the photomicrographs of this study.
First submission on 28/02/12
Last submission on 11/07/12
Accepted for publication on 25/09/12
Published on 20/02/13
- 1. BARMAK, K.; HARHAJ, E.; GRANT, C.; ALEFANTIS, T.; WIGDAHL, B. Human T cell leukemia virus type I-induced disease: pathways to cancer and neurodegeneration. Human T cell leukemia virus type I-induced disease: pathways to cancer and neurodegeneration. Virology, v. 308, n. 1, p. 1-12, 2003.
- 2. BRAND, H.; ALVES, J. G. B.; PEDROSA, F.; LUCENA-SILVA, N. Leucemia de células T do adulto. Rev Bras Hematol Hemoter, v. 31, n. 5, p. 375-83, 2009.
- 3. CARNEIRO-PROIETTI, A. B. F. et al Infecção e doença pelos vírus linfotrópicos humanos de células T (HTLV-I/II) no Brasil. Rev Soc Bras Med Trop, v. 35, p. 499-508, 2002.
- 4. GRANT, C.; BARMAK, K.; ALEFANTIS, T.; YAO, J.; JACOBSON, S.; WIGDAHL, B. Human T cell leukemia virus type I and neurologic disease: events in bone marrow, peripheral blood, and central nervous system during normal immune surveillance and neuroinflammation. J Cell Physiol, v. 190, n. 2, p. 133-59, 2002.
- 5. HASEGAWA, H. et al. Thymusderived leukemia-lymphoma in mice transgenic for the tax gene of human tlymphotropic virus type I. Nat Med, v. 12, p. 466-72, 2006.
- 6. HISADA, M.; OKAYAMA, A.; SHIOIRI, S.; SPIEGELMAN, D. L.; STUVER, S. O.; MUELLER, N. E. Risk factors for adult T-cell leukemia among carriers of human T-lymphotropic virus type I. Blood, v. 92, n. 10, p. 3557-61, 1998.
- 7. MANNS, A.; HISADA, M.; Da GRENADE, L. Human T- lymphotropic virus type I infection. Lancet, v. 353, p. 1951-8, 1999.
- 8. ROMANELLI, L. C. F.; CARAMELLI, P.; PROIETTI, A. B. F. C. O vírus linfotrópico de células T humanos tipo 1 (HTLV-1): quando suspeitar da infecção? Rev Assoc Med Bras, v. 56, n. 3, p. 340-7, 2010.
- 9. SANTOS, E. L. et al. Caracterização molecular do HTLV-1/2 em doadores de sangue em Belém, Estado do Pará: primeira descrição do subtipo HTLV-2b na região Amazônica. Rev Soc Bras Med Trop, v. 42, n. 3, p. 271-6, 2009.
- 10. SATOU, Y. et al HTLV-1 bZIP factor induces T-Cell lymphoma and systemic inflammation in vivo Plos Pathog, v. 7, n. 2, p. 1-14, 2011.
- 11. SHIMAMOTO, Y. Clinical indications of multiple integrations of human T-cell lymphotropic virus type I proviral DNA in adult T-cell leukemia/lymphoma. Leuk Lymphoma, v. 27, n. 1-2, p. 43-51, 1997.
- 12. SILVA, F. A.; MEIS, E.; DOBBIN, J. A.; OLIVEIRA, M. S. P. Leucemia-linfoma de células T do adulto no Brasil: epidemiologia, tratamento e aspectos controversos. Rev Bras Cancer, v. 48, n. 4, p. 585-95, 2002.
- 13. SOARES, R. M. G.; MORAES JÚNIOR, H. V. Manifestações oculares observadas em indivíduos infectados por HTLV-I no Rio de Janeiro. Arq Bras Oftal, v. 63, n. 4, p. 293-8, 2000.
- 14. SOUZA, L. A. et al. Caracterização molecular do HTLV-1 em pacientes com paraparesia espástica tropical/mielopatia associada ao HTLV-1 em Belém, Pará. Rev Soc Bras Med Trop, v. 39, n. 5, p. 504-6, 2006.
- 15. SWERDLOW, SH. et al World Health Organization Classification of Tumours. Pathology and genetics of tumours of haematopoietic and lymphoid tissues. IARC: Lyon; 2008. p. 111-7.
- 16. TABAKIN-FIX, Y.; AZRAN, I.; SCHAVINKY-KHRAPUNSKY, Y.; LEVY, O.; ABOUD, M. Functional inactivation of p53 by human T-cell leukemia virus type 1 Tax protein: mechanisms and clinical implications. Carcinogenesis, v. 27, n. 4, p. 673-81, 2006.
- 17. TOULZA, F. et al. FoxP3+ regulatory T cells are distinct from leukemia cells in HTLV-1-associated adult T-cell leukemia. Int J Cancer, v. 125, p. 2375-82, 2009.
- 18. YASUNAGA, J.; MATSUOKA, M. Human T-cell leukemia virus type I induces adult T-cell leukemia: from clinical aspects to molecular mechanisms. Cancer Control, v. 14, n. 2, p. 133-40, 2007.
Publication Dates
-
Publication in this collection
20 May 2013 -
Date of issue
Feb 2013
History
-
Received
28 Feb 2012 -
Accepted
25 Sept 2012