Abstract
Ehlers-Danlos Syndrome (EDS) is a rare inherited connective tissue disease arising from an abnormality of collagen synthesis. The main feature of EDS is the extreme fragility of connective tissues, which can result in uterine rupture, spontaneous intestinal drilling and vascular diseases such as aneurysms, pseudoaneurysms, arterial dissections and spontaneous ruptures. This paper describes the case of an 11-year-old patient who presented a pulsatile mass in the left popliteal fossa after a minor trauma caused by a soccer ball. A pseudoaneurysm of the popliteal artery was diagnosed with arterial Doppler ultrasound and confirmed using angiography. An exploratory investigation revealed that the artery wall was too weak to allow reconstruction and the proximal artery was ligated. The patient developed severe limb ischemia and after authorization by the family the limb was amputated. Two days after surgery, the patient died as a result of acute thoracic aortic dissection.
Keywords:
pseudoaneurysm; popliteal artery; Ehlers-Danlos syndrome
Resumo
A Síndrome de Ehlers-Danlos (EDS) é uma rara doença hereditária do tecido conjuntivo proveniente de uma alteração da síntese do colágeno. A principal característica da EDS é a extrema fragilidade do tecido conjuntivo, que pode resultar em rotura uterina, perfuração intestinal espontânea e várias doenças vasculares como aneurismas, pseudoaneurismas, dissecções arteriais e roturas espontâneas. Os autores relatam o caso de um paciente de 11 anos de idade que apresentava tumor pulsátil na fossa poplítea esquerda após trauma leve com bola de futebol. Diagnosticado pseudoaneurisma de artéria poplítea pelo doppler arterial, confirmado através da angiografia, optou-se pela exploração arterial e devido à fragilidade da parede não foi possível a sua reconstrução. Realizada a ligadura simples da artéria proximal. Evoluiu com isquemia grave do membro e após autorização da família foi realizada a sua amputação. No segundo dia do pós-operatório o paciente apresentou uma dissecção aguda da aorta torácica, evoluindo a óbito.
Palavras-chave:
pseudoaneurisma; artéria poplítea; Síndrome de Ehlers-Danlos
INTRODUCTION
Ehlers-Danlos Syndrome is a hereditary disease of the connective tissues characterized by joint hypermobility, fragile skin and hyperextensibility. Type VI is an autosomal recessive variant of the syndrome that is characterized by neonatal kyphoscoliosis, generalized loose joints, fragile skin and severe muscle hypotonia at birth. Biochemically, there is an abnormality of collagen biosynthesis caused by a deficiency of the lysyl hydroxylase enzyme, resulting in a hydroxylation deficiency of lysine and proline residues in the procollagen chains. These residues provide bonding locations for galactose and glucosyl-galactose and also play a role in the reticulation process that gives collagen resistance and traction. The condition is related to a mutation of the PLOD1 gene, on chromosome 1p36.22.11 Beighton P, Paepe AD, Steinmann B, Tsipouras P, Wenstrup RJ. Ehlers-Danlos syndromes: revised nosology, Villefranche, 1997. Am J Med Genet. 1998;77(1):31-7. http://dx.doi.org/10.1002/(SICI)1096-8628(19980428)77:1<31::AID-AJMG8>3.0.CO;2-O. PMid:9557891.
http://dx.doi.org/10.1002/(SICI)1096-862...
2 Heim P, Raghunath M, Meiss L, et al. Ehlers-Danlos syndrome type VI (EDS VI): problems of diagnosis and management. Acta Paediatr. 1998;87(6):708-10. http://dx.doi.org/10.1111/j.1651-2227.1998.tb01537.x. PMid:9686670.
http://dx.doi.org/10.1111/j.1651-2227.19...
3 Ihme A, Risteli L, Krieg T, et al. Biochemical characterization of variants of the Ehlers-Danlos syndrome type VI. Eur J Clin Invest. 1983;13(4):357-62. http://dx.doi.org/10.1111/j.1365-2362.1983.tb00113.x. PMid:6413223.
http://dx.doi.org/10.1111/j.1365-2362.19...
-44 Wenstrup RJ, Murad S, Pinnell SR. Ehlers-Danlos syndrome type VI: clinical manifestations of collagen lysyl hydroxylase deficiency. J Pediatr. 1989;115(3):405-9. http://dx.doi.org/10.1016/S0022-3476(89)80839-X. PMid:2504907.
http://dx.doi.org/10.1016/S0022-3476(89)...
CASE DESCRIPTION
An 11-year-old, white, male patient presented with pain and edema in the left lower limb and difficulty walking with onset 5 days previously, after suffering a trauma from a soccer ball.
The patient's parents were consanguineous (first-degree cousins) and had a family history of Type VI Ehlers-Danlos Syndrome. The patient had one brother and one sister with the same condition who were receiving outpatients care from the genetics clinic at the PUC-SP Faculdade de Ciências Médicas e da Saúde (Sorocaba campus).
On physical examination, the patient exhibited difficulties with walking, edema of the left lower limb and a pulsating mass in the popliteal fossa, with distal pulses present.
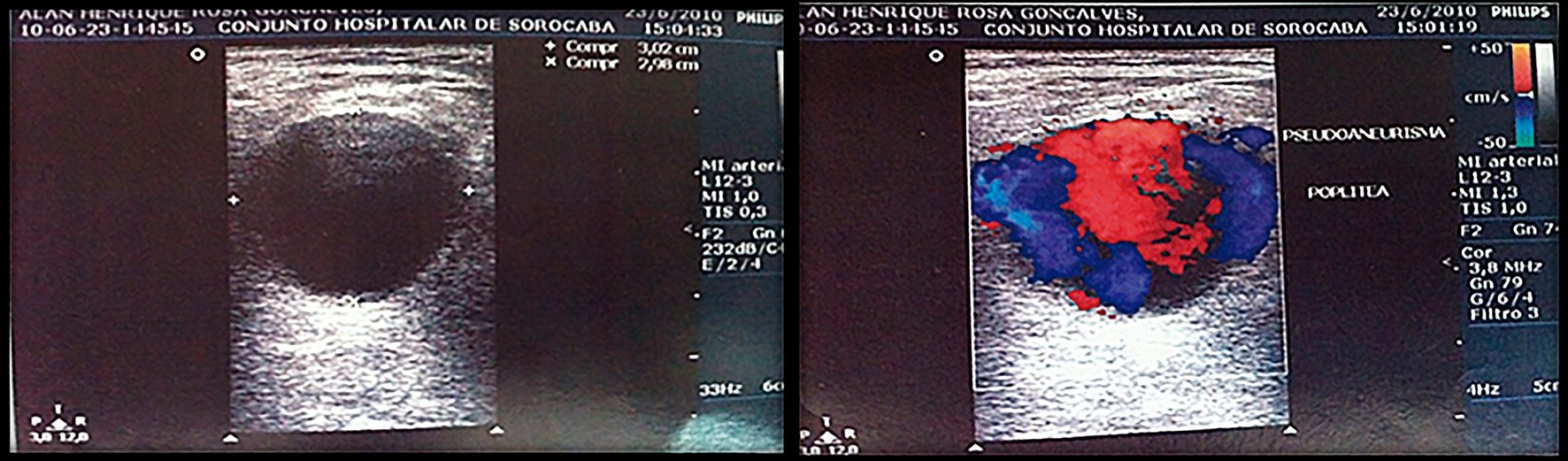
Doppler ultrasonography showed that the popliteal artery was patent, with triphasic flow, and revealed a large hematoma in the popliteal fossa, with turbulent flow inside. The hematoma was 9 cm in length, extending from a point 3 cm above the knee joint line to a point 6 cm below the line (Figure 1).

Arteriography showed fusiform dilation compatible with a pseudoaneurysm of the popliteal artery (Figure 2).

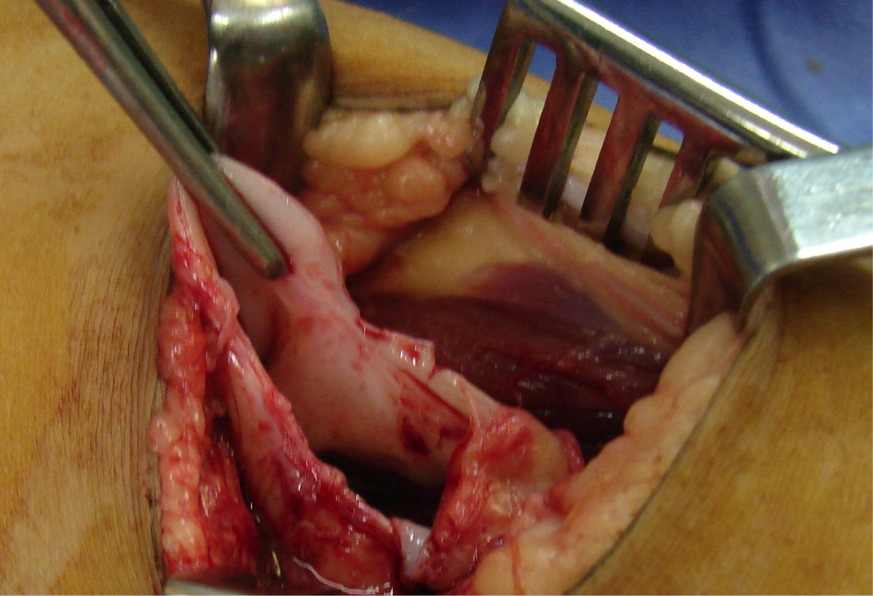
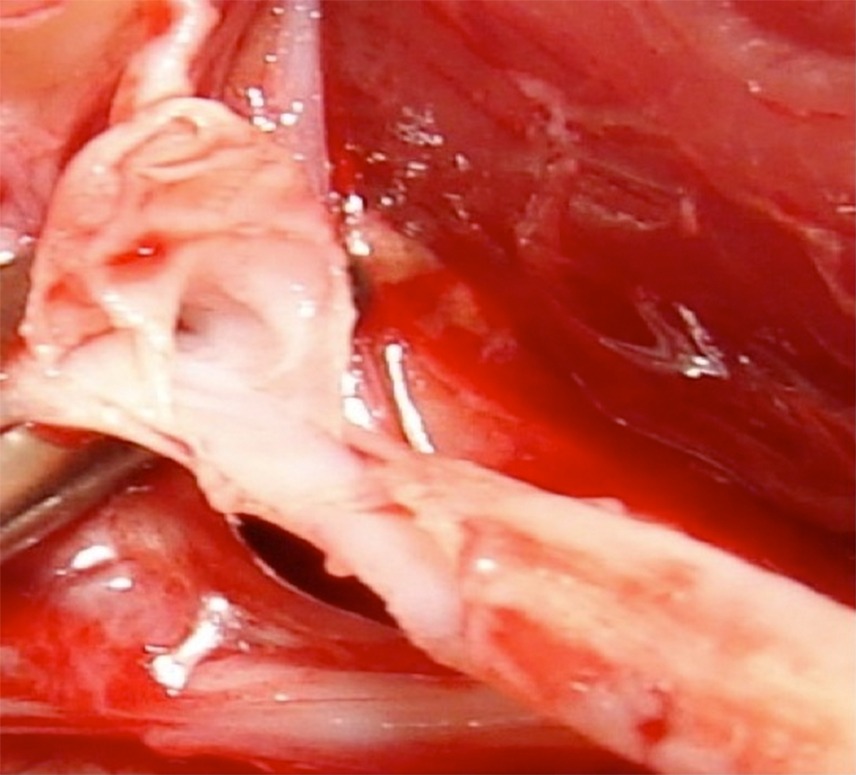
The decision was taken to treat the patient surgically. A Z-shaped incision was made to provide posterior access to the popliteal vessels and allow direct dissection of the pseudoaneurysm. The extreme fragility of these tissues was notable (Figures 3, 4 and 5).



An attempt at distal anastomosis of the posterior tibial artery was made using the reversed ipsilateral great saphenous vein, but the attempt was unsuccessful because of the fragility of the artery wall.
Proximal anastomosis of the distal superficial femoral artery was attempted, but could not be accomplished because there was no structure that was firm enough to anchor the sutures.
The decision was then taken to ligate the femoral artery, using 2-0 cotton thread, which was extremely difficult because of the fragility of the artery.
The patient was transferred to the ICU where a transfemoral amputation was performed because of ischemia.
The patient died two days after the operation and was sent to the department responsible for assessment of in-hospital deaths, where the cause of death was identified as thoracic hemorrhage caused by dissection of the thoracic aorta.
DISCUSSION
In Ehlers-Danlos Syndrome, the disease is present from birth, but the symptoms, when detected, are identified later in life. To date, 11 variants of the syndrome have been identified and all of these forms exhibit typical clinical characteristics, of varying intensity.11 Beighton P, Paepe AD, Steinmann B, Tsipouras P, Wenstrup RJ. Ehlers-Danlos syndromes: revised nosology, Villefranche, 1997. Am J Med Genet. 1998;77(1):31-7. http://dx.doi.org/10.1002/(SICI)1096-8628(19980428)77:1<31::AID-AJMG8>3.0.CO;2-O. PMid:9557891.
http://dx.doi.org/10.1002/(SICI)1096-862...
Type VI, autosomal recessive, Ehlers-Danlos Syndrome is extremely rare. Clinical presentation is with normal or tall stature, marfanoid appearance, ophthalmological involvement (keratoconus, microcornea, myopia, retinal detachment, ocular rupture, blue sclera, epicanthus, glaucoma and blindness), low bridge of the nose, abnormalities of the implantation of teeth, cardiac disorders, arterial rupture, pulmonary dysfunctions caused by deformities of the thorax, gastrointestinal hemorrhage, inguinal hernia, bladder diverticulum, loose ligaments, osteoporosis, joint luxations, kyphoscoliosis, arachnodactyly, flat feet, hyperextensible and velvety skin and hypotonia.11 Beighton P, Paepe AD, Steinmann B, Tsipouras P, Wenstrup RJ. Ehlers-Danlos syndromes: revised nosology, Villefranche, 1997. Am J Med Genet. 1998;77(1):31-7. http://dx.doi.org/10.1002/(SICI)1096-8628(19980428)77:1<31::AID-AJMG8>3.0.CO;2-O. PMid:9557891.
http://dx.doi.org/10.1002/(SICI)1096-862...
2 Heim P, Raghunath M, Meiss L, et al. Ehlers-Danlos syndrome type VI (EDS VI): problems of diagnosis and management. Acta Paediatr. 1998;87(6):708-10. http://dx.doi.org/10.1111/j.1651-2227.1998.tb01537.x. PMid:9686670.
http://dx.doi.org/10.1111/j.1651-2227.19...
3 Ihme A, Risteli L, Krieg T, et al. Biochemical characterization of variants of the Ehlers-Danlos syndrome type VI. Eur J Clin Invest. 1983;13(4):357-62. http://dx.doi.org/10.1111/j.1365-2362.1983.tb00113.x. PMid:6413223.
http://dx.doi.org/10.1111/j.1365-2362.19...
-44 Wenstrup RJ, Murad S, Pinnell SR. Ehlers-Danlos syndrome type VI: clinical manifestations of collagen lysyl hydroxylase deficiency. J Pediatr. 1989;115(3):405-9. http://dx.doi.org/10.1016/S0022-3476(89)80839-X. PMid:2504907.
http://dx.doi.org/10.1016/S0022-3476(89)...
Management of these patients includes an annual physical examination, echocardiogram and ultrasound of the carotids and the abdomen. Arteriography is only indicated if embolization is suspected. Vascular complications include spontaneous rupture, dissection and dissecting aneurysms.55 Artázcoz AV, Montoya JJ, Vilardell PL. Rotura espontânea de artéria femoral em paciente afecto de Ehlers-Danlos syndrome type IV o Sacks-Barbara. Cir Esp. 2009;86:179-89. PMid:19539900.,66 Freeman RK, Swegle J, Sise MJ. The surgical complications of Ehlers-Danlos syndrome. Am Surg. 1966;62(10):869-73. PMid:8813174. Hemorrhages caused by ruptured arteries are most common among young men, with greatest incidence in arteries of the abdominal cavity, followed by the popliteal artery.55 Artázcoz AV, Montoya JJ, Vilardell PL. Rotura espontânea de artéria femoral em paciente afecto de Ehlers-Danlos syndrome type IV o Sacks-Barbara. Cir Esp. 2009;86:179-89. PMid:19539900. Patients with asymptomatic complications are treated conservatively. Patients with active bleeding require emergency surgery or endovascular embolization.
A bibliographic search conducted on PubMed did not identify any similar case reports involving Ehlers-Danlos type VI, but 11 related published articles were identified.
Freeman et al.66 Freeman RK, Swegle J, Sise MJ. The surgical complications of Ehlers-Danlos syndrome. Am Surg. 1966;62(10):869-73. PMid:8813174. reviewed case reports published between January 1975 and July 1995, totaling 45 cases of vascular complications related to Ehlers-Danlos Syndrome type VI. They concluded that vascular complications should be treated without surgery and without invasive imaging exams.77 Oderich GS, Panneton JM, Bower TC, et al. The spectrum, management and clinical outcome of Ehlers-Danlos syndrome type IV: A 30 year experience. J Vasc Surg. 2005;42(1):98-106. http://dx.doi.org/10.1016/j.jvs.2005.03.053. PMid:16012458.
http://dx.doi.org/10.1016/j.jvs.2005.03....
8 Domenick N, Cho JS, Abu Hamad G, Makaroun MS, Chaer RA. Endovascular repair of multiple infrageniculate aneurysms in a patient with vascular type Ehlers-Danlos syndrome. J Vasc Surg. 2011;54(3):848-50. http://dx.doi.org/10.1016/j.jvs.2011.01.035. PMid:21458207.
http://dx.doi.org/10.1016/j.jvs.2011.01....
-99 Onnessen BH, Sternbergh WC 3rd, Mannava K, Money SR. Endovascular repair of na iliac artery aneurysm in a patient with Ehlers-Danlos syndrome type IV. J Vasc Surg. 2007;45(1):177-9. http://dx.doi.org/10.1016/j.jvs.2006.08.071. PMid:17210404.
http://dx.doi.org/10.1016/j.jvs.2006.08....
Arteriography involves a high risk of hemorrhage, dissection, pseudoaneurysm and arteriovenous fistula, and so ultrasound or magnetic resonance angiography should be preferred.55 Artázcoz AV, Montoya JJ, Vilardell PL. Rotura espontânea de artéria femoral em paciente afecto de Ehlers-Danlos syndrome type IV o Sacks-Barbara. Cir Esp. 2009;86:179-89. PMid:19539900.
When surgery is unavoidable, treatment should be restricted to ligature of the affected vessel, since 28 of the 45 cases covered in the review involved surgical treatment: 20 reconstructions and eight ligations. The number of deaths was 20 (30%), which was all of the 20 patients who underwent reconstruction. The morbidity and mortality rates of invasive imaging exams were 5% to 16%.55 Artázcoz AV, Montoya JJ, Vilardell PL. Rotura espontânea de artéria femoral em paciente afecto de Ehlers-Danlos syndrome type IV o Sacks-Barbara. Cir Esp. 2009;86:179-89. PMid:19539900.
The literature does not contain clinical medical reports that could provide a basis for definition of standard treatment, because of the low incidence of this disease and its high mortality rate. Theoretically, the treatment of choice would appear to be endovascular, because it is less aggressive, but it can also have fatal results linked to difficulties controlling the location of catheterization and to arteries ruptured by balloon angioplasty or stent techniques.55 Artázcoz AV, Montoya JJ, Vilardell PL. Rotura espontânea de artéria femoral em paciente afecto de Ehlers-Danlos syndrome type IV o Sacks-Barbara. Cir Esp. 2009;86:179-89. PMid:19539900. The authors conclude that best surgical options is ligature, due to the fragility of vessels, and that noninvasive examinations should be preferred.1010 Singh M, Puppala S, Pollitt RC, Sobey GJ, Scott DJ. Femoral artery dissection in vascular type Ehlers-Danlos syndrome: leave well alone? Eur J Vasc Endovasc Surg. 2012;43(3):341-2. http://dx.doi.org/10.1016/j.ejvs.2011.12.005. PMid:22226700.
http://dx.doi.org/10.1016/j.ejvs.2011.12...
11 Lum YW, Brooke BS, Arnaoutakis GJ, Williams TK, Black JH 3rd. Endovascular procedures in patient with Ehlers-Danlos syndrome: review of clinical outcomes and iatrogenic complications. Ann Vasc Surg. 2012;26(1):25-33. http://dx.doi.org/10.1016/j.avsg.2011.05.028. PMid:21945330.
http://dx.doi.org/10.1016/j.avsg.2011.05...
12 Kimura K, Sakai-Kimura M, Takahashi R, et al. Too friable to treat? Lancet. 2010;375(9725):1578. http://dx.doi.org/10.1016/S0140-6736(10)60238-3. PMid:20435230.
http://dx.doi.org/10.1016/S0140-6736(10)...
-1313 Nasser M, Vega MB, Pivetta LGA, et al. Dissecção da artéria carótida interna em paciente com síndrome de Ehlers-Danlos tipo IV: diagnóstico e manejo. J Vasc Bras. 2013;12:174-9. They also recommend clinical treatment, such as control of arterial blood pressure, to reduce the risk of rupture and, if necessary, beta blockers to prevent expansion of arteries. High impact exercise such as gymnastics and long distance running should be avoided. Genetic counseling is also part of care. Identification and early diagnosis are indispensable to minimize complications, improving patients' quality of life.
-
Financial support: None.
-
The study was carried out at the School of Medical and Health Sciences, Pontifícia Universidade Católica de São Paulo (PUC-SP), Sorocaba, SP, Brazil.
REFERÊNCIAS
-
1Beighton P, Paepe AD, Steinmann B, Tsipouras P, Wenstrup RJ. Ehlers-Danlos syndromes: revised nosology, Villefranche, 1997. Am J Med Genet. 1998;77(1):31-7. http://dx.doi.org/10.1002/(SICI)1096-8628(19980428)77:1<31::AID-AJMG8>3.0.CO;2-O. PMid:9557891.
» http://dx.doi.org/10.1002/(SICI)1096-8628(19980428)77:1<31::AID-AJMG8>3.0.CO;2-O -
2Heim P, Raghunath M, Meiss L, et al. Ehlers-Danlos syndrome type VI (EDS VI): problems of diagnosis and management. Acta Paediatr. 1998;87(6):708-10. http://dx.doi.org/10.1111/j.1651-2227.1998.tb01537.x. PMid:9686670.
» http://dx.doi.org/10.1111/j.1651-2227.1998.tb01537.x -
3Ihme A, Risteli L, Krieg T, et al. Biochemical characterization of variants of the Ehlers-Danlos syndrome type VI. Eur J Clin Invest. 1983;13(4):357-62. http://dx.doi.org/10.1111/j.1365-2362.1983.tb00113.x. PMid:6413223.
» http://dx.doi.org/10.1111/j.1365-2362.1983.tb00113.x -
4Wenstrup RJ, Murad S, Pinnell SR. Ehlers-Danlos syndrome type VI: clinical manifestations of collagen lysyl hydroxylase deficiency. J Pediatr. 1989;115(3):405-9. http://dx.doi.org/10.1016/S0022-3476(89)80839-X. PMid:2504907.
» http://dx.doi.org/10.1016/S0022-3476(89)80839-X -
5Artázcoz AV, Montoya JJ, Vilardell PL. Rotura espontânea de artéria femoral em paciente afecto de Ehlers-Danlos syndrome type IV o Sacks-Barbara. Cir Esp. 2009;86:179-89. PMid:19539900.
-
6Freeman RK, Swegle J, Sise MJ. The surgical complications of Ehlers-Danlos syndrome. Am Surg. 1966;62(10):869-73. PMid:8813174.
-
7Oderich GS, Panneton JM, Bower TC, et al. The spectrum, management and clinical outcome of Ehlers-Danlos syndrome type IV: A 30 year experience. J Vasc Surg. 2005;42(1):98-106. http://dx.doi.org/10.1016/j.jvs.2005.03.053. PMid:16012458.
» http://dx.doi.org/10.1016/j.jvs.2005.03.053 -
8Domenick N, Cho JS, Abu Hamad G, Makaroun MS, Chaer RA. Endovascular repair of multiple infrageniculate aneurysms in a patient with vascular type Ehlers-Danlos syndrome. J Vasc Surg. 2011;54(3):848-50. http://dx.doi.org/10.1016/j.jvs.2011.01.035. PMid:21458207.
» http://dx.doi.org/10.1016/j.jvs.2011.01.035 -
9Onnessen BH, Sternbergh WC 3rd, Mannava K, Money SR. Endovascular repair of na iliac artery aneurysm in a patient with Ehlers-Danlos syndrome type IV. J Vasc Surg. 2007;45(1):177-9. http://dx.doi.org/10.1016/j.jvs.2006.08.071. PMid:17210404.
» http://dx.doi.org/10.1016/j.jvs.2006.08.071 -
10Singh M, Puppala S, Pollitt RC, Sobey GJ, Scott DJ. Femoral artery dissection in vascular type Ehlers-Danlos syndrome: leave well alone? Eur J Vasc Endovasc Surg. 2012;43(3):341-2. http://dx.doi.org/10.1016/j.ejvs.2011.12.005. PMid:22226700.
» http://dx.doi.org/10.1016/j.ejvs.2011.12.005 -
11Lum YW, Brooke BS, Arnaoutakis GJ, Williams TK, Black JH 3rd. Endovascular procedures in patient with Ehlers-Danlos syndrome: review of clinical outcomes and iatrogenic complications. Ann Vasc Surg. 2012;26(1):25-33. http://dx.doi.org/10.1016/j.avsg.2011.05.028. PMid:21945330.
» http://dx.doi.org/10.1016/j.avsg.2011.05.028 -
12Kimura K, Sakai-Kimura M, Takahashi R, et al. Too friable to treat? Lancet. 2010;375(9725):1578. http://dx.doi.org/10.1016/S0140-6736(10)60238-3. PMid:20435230.
» http://dx.doi.org/10.1016/S0140-6736(10)60238-3 -
13Nasser M, Vega MB, Pivetta LGA, et al. Dissecção da artéria carótida interna em paciente com síndrome de Ehlers-Danlos tipo IV: diagnóstico e manejo. J Vasc Bras. 2013;12:174-9.
Publication Dates
-
Publication in this collection
Oct-Dec 2015
History
-
Received
12 Aug 2015 -
Accepted
23 Oct 2015