Abstracts
The purpose of this investigation was to comparatively evaluate the cephalometric changes in soft and hard tissues related to treatment of Class II, division 1 malocclusion with activator-headgear and Bionator appliances. Twenty-four individuals formed the activator-headgear group and twenty-five comprised the Bionator group, while other twenty-four presenting the same malocclusion did not receive any intervention and served as controls. Lateral headfilms were taken at the beginning and at the end of the observation period and were digitized with computerized cephalometrics; cephalometric analysis was performed and the results were submitted to statistical test. According to the methodology employed, our findings suggested that both appliances do not significantly alter the growth path, and also they were not able to modify the posterior inferior height and the sagittal and vertical position of the upper lip. The lower lip and the soft menton were only slightly modified by the orthopedic appliances, but the mentolabial sulcus showed a significant decrease in deepness compared to the control group. Of statistical significance, only the anterior inferior hard and soft facial heights and the lower lip height increased more in the treated groups.
Malocclusion; Orthopedics; Removable appliances
Esta pesquisa teve por objetivo avaliar, comparativamente, as alterações cefalométricas tegumentares e esqueléticas, decorrentes do tratamento das más oclusões de classe II, 1a divisão, com o ativador combinado com a ancoragem extrabucal e com o bionator. O grupo tratado com o ativador combinado com a ancoragem extrabucal foi composto por 24 indivíduos e o grupo tratado com o bionator compreendeu 25 pacientes, enquanto que outros 24 indivíduos compuseram o grupo controle, apresentando a mesma má oclusão, porém sem terem sido submetidos a nenhuma terapia ortodôntica. Obteve-se telerradiografias laterais de todos os indivíduos no início e final do período de observação que foram digitalizadas e seus traçados cefalométricos computadorizados realizados e submetidos ao teste estatístico. De acordo com a metodologia empregada, os resultados sugerem que ambos os aparelhos não foram capazes de alterar, significaticamente, o padrão de crescimento facial assim como a altura facial posterior inferior e o posicionamento sagital e vertical do lábio superior. Os aparelhos ortopédicos alteraram ligeiramente o lábio inferior e o mento tegumentar, porém o sulco mentolabial foi signifivativamente reduzido nos grupos tratados em comparação com o grupo controle. As alturas faciais esquelética e tegumentar, bem como a altura do lábio inferior foram significativamente aumentadas com a terapia ortopédica, alcançando diferença estatística em relação ao grupo controle.
Má oclusão; Ortopedia; Aparelhos Removíveis
ORIGINAL ARTICLES
Influence of orthopedic treatment on hard and soft facial structures of individuals presenting with Class II, Division 1 malocclusion. A comparative study
A influência do tratamento ortopédico nas estruturas faciais de indivíduos com má oclusão de Classe II, 1ª Divisão. Um estudo comparativo
Liliana Ávila MaltagliatiI; José Fernando Castanha HenriquesII; Guilherme JansonII; Renato Rodrigues de AlmeidaII; Marcos Roberto de FreitasII
IGraduate Student Department of Orthodontics Bauru Dental School, University of são Paulo, Bauru SP Brazil. Recipient of FAPESP scholarship. Assistant Professor of the UMES São Paulo
IIProfessor Department of Orthodontics Bauru Dental School, University of São Paulo, Bauru SP Brazil
Correspondence Correspondence to Liliana Ávila Maltagliati Rua do Sacramento, 230 Ed. Lambda, sala 241 - Rudge Ramos São Bernardo do Campo - SP - CEP:09640-000 Phone: 55 11 4366-5562 - Fax: 55 11 4366-5826 e-mail: lilianamaltagliati@hotmail.com
ABSTRACT
The purpose of this investigation was to comparatively evaluate the cephalometric changes in soft and hard tissues related to treatment of Class II, division 1 malocclusion with activator-headgear and Bionator appliances. Twenty-four individuals formed the activator-headgear group and twenty-five comprised the Bionator group, while other twenty-four presenting the same malocclusion did not receive any intervention and served as controls. Lateral headfilms were taken at the beginning and at the end of the observation period and were digitized with computerized cephalometrics; cephalometric analysis was performed and the results were submitted to statistical test. According to the methodology employed, our findings suggested that both appliances do not significantly alter the growth path, and also they were not able to modify the posterior inferior height and the sagittal and vertical position of the upper lip. The lower lip and the soft menton were only slightly modified by the orthopedic appliances, but the mentolabial sulcus showed a significant decrease in deepness compared to the control group. Of statistical significance, only the anterior inferior hard and soft facial heights and the lower lip height increased more in the treated groups.
Uniterms: Malocclusion; Orthopedics; Removable appliances.
RESUMO
Esta pesquisa teve por objetivo avaliar, comparativamente, as alterações cefalométricas tegumentares e esqueléticas, decorrentes do tratamento das más oclusões de classe II, 1a divisão, com o ativador combinado com a ancoragem extrabucal e com o bionator. O grupo tratado com o ativador combinado com a ancoragem extrabucal foi composto por 24 indivíduos e o grupo tratado com o bionator compreendeu 25 pacientes, enquanto que outros 24 indivíduos compuseram o grupo controle, apresentando a mesma má oclusão, porém sem terem sido submetidos a nenhuma terapia ortodôntica. Obteve-se telerradiografias laterais de todos os indivíduos no início e final do período de observação que foram digitalizadas e seus traçados cefalométricos computadorizados realizados e submetidos ao teste estatístico. De acordo com a metodologia empregada, os resultados sugerem que ambos os aparelhos não foram capazes de alterar, significaticamente, o padrão de crescimento facial assim como a altura facial posterior inferior e o posicionamento sagital e vertical do lábio superior. Os aparelhos ortopédicos alteraram ligeiramente o lábio inferior e o mento tegumentar, porém o sulco mentolabial foi signifivativamente reduzido nos grupos tratados em comparação com o grupo controle. As alturas faciais esquelética e tegumentar, bem como a altura do lábio inferior foram significativamente aumentadas com a terapia ortopédica, alcançando diferença estatística em relação ao grupo controle.
Unitermos: Má oclusão; Ortopedia; Aparelhos Removíveis.
INTRODUCTION
It has been reported that the great majority of orthodontic patients present Class II malocclusions, varying on osseous, dental and facial aspects, resulting in a great variety of combined deformities. Thus, in order to treat these malocclusions, several appliances and methods of treatment have been developed.
Class II interceptive appliances can be generally divided into two groups: mechanical appliances, represented by headgear anchorage; and functional appliances, found in a greater variety of models, aiming at protruding the mandible and enhancing mandibular growth. As most Class II patients show retruded mandible9,12, protrusion is often desirable.
Two of the most common devices are Bionator, introduced by Balters5,6,7 in the 1960s, and the activator, introduced by Andresen3, in 1908. Hasund apud Graber, Neumann11, in 1969, was the first professional to incorporate headgear forces into functional appliances, more commonly used when the malocclusion involves maxillary protrusion and long face patterns.
Most studies reported that functional therapy is effective in anterior mandibular displacement, restriction of maxillary growth, enhancement of anterior and posterior inferior facial height, lingual tipping of the maxillary incisors and buccal tipping of the mandibular incisors. Unfortunately, only few studies reported about soft tissue changes and available data are controversial.
In 1993, Henriques, Freitas, Scavone Júnior15 studied some soft tissue parameters and found that the upper lip followed the improvement in maxillary incisors inclination, leading to enhancement of the nasolabial and H.NB angle and reduction of nasal in relation to the H line. Henriques14 compared the use of extraoral anchorage in three ways: cervical traction, associated with a removable appliance and in combination with the activator. Similar effects were found on the nasolabial angle.
Many authors have already mentioned that Bionator appliance therapy could improve balancing on facial height. However, this improvement had not been quantified yet. Then, in 1995, Lange, et al.20 decided to study the changes caused by Bionator appliance therapy on the soft tissue compared to a control group. Results have demonstrated an increase in anterior inferior facial height and posterior facial height of treated individuals, as shown by the ENA-ME and Ar-Go measurements; improvement in facial convexity (G'.Sn.Pog'), due to mandibular advancement; and retraction of the upper lip and nasolabial angle opening, but with no statistical significance. However, most changes were seen on the lower lip - the mentolabial angle became more obtuse in response to labial elongation, resulting in a higher and thinner lip.
Due to the lack of studies reporting on facial analysis of treated and untreated cases, Morris, Illing, Lee21 investigated the influence of treatment on profile and soft tissue morphology of patients, comparing Bionator appliance, Bass appliance and twin-block appliance treatment therapy. Despite of chin advancement, cephalometric results caused by Bionator appliance therapy showed significant reduction of facial convexity when compared to the control group. Major increase was seen on the soft tissue facial height. The nasolabial and mentolabial sulcus measurements, as well as the anterior posterior position and thickness and height of upper and lower lip did not differ in both Bionator group and checking group. Authors reported few changes, probably due to their small dimension and great variability. Thus, these results cannot be considered to recommend the use of a proper device for a given treatment.
In 2002, Almeida, et al.2, on a discussion about the effects of Bionator appliance therapy on the soft tissue profile, reported that protrusion of the upper lip is decreased and that of the lower lip is increased. The nasolabial angle did not show any significant change.
Thus, the controversy presented by these articles has led to the accomplishment of this study, which aims at investigating the influence of functional orthopedics on the soft tissue profile, as well as the changes caused by the combination of activator-headgear appliance and Bionator appliance therapy in treatment, regardless of dental and skeletal effects.
SUBJECTS AND METHODS
Subjects
The sample was collected retrospectively, comprising 146 lateral cephalograms of 73 mesofacial patients treated at the orthodontic clinic of Bauru Dental School, University of Sao Paulo, Brazil, divided into three groups:
- Group A, 24 patients treated with the activator-headgear combination (14 males and 10 females) and initial age of 11y 3m and final 12y 7m;
- Group B, 25 patients treated with Bionator (13 males and 12 females) and initial age of 10y11m and final 12y5m;
- Group C, 24 patients (14 males and 10 females) that did not receive treatment.
First, all patients that had received treatment by the two types of appliances and those who did not receive treatment were included. Then, the initial cephalometric values were compared and only those who displayed similar cephalometric analyses were included in the sample.
Appliances
The headgear used high pull traction and the patients of both appliances were instructed to use them during the whole day and at night. The acrylic over the mandibular teeth was trimmed once a month to allow eruption of the molars and premolars. The construction bite was made in an edge to edge position.
Cephalometric Tracing
The cephalometric tracings were done in an appropriate cephalometric software using windows 989 and the analysis was specially constructed for this study.
Data management
A "t" test and Dahlberg's formula were used to analyze systematic and random methodological errors, respectively. Also, the "t" test was used for comparison between the manual and computer cephalometric tracings to confirm the reliability of the methodology, and the analyses of variance for evaluation of the compatibility of the initial values of the groups.
RESULTS
Methodology reliability
The analyses showed no statistically significant errors in the methodology. Like Houston16 and Sandler25 stated, errors smaller than 1.5o or 1mm are not clinically important. Analyses of the reliability of the cephalometric tracing method used demonstrated that the difference was significant only for three variables, showing good reproducibility, and the analyses of variance could not find statistical differences between the initial values of the three groups, except for one variable. This would confirm that they are very similar and any discrepancy found during the observation period could be attributed to the effect of the appliances.
Group Comparisons (Table 3)
DISCUSSION
Sexual dimorphism was present on three parameters, corresponding to inclination of the palatal plane and skeletal and tegument anterior inferior facial heights. This has been already demonstrated by other authors in previous studies11, 21 and illustrates the more vertical facial growth tendency of females.
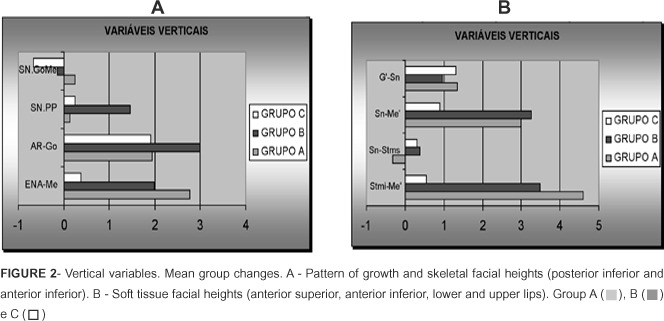
The growth pattern had small changes and there were no relevant differences between the treated and untreated patients, regardless of the appliance used, showing little influence in the mandibular1,7,9,17,18,19,21,23,26 and palatal plane inclination9,12,17,19,23(figure 2A).
During the observation period, no difference could be found on the increment in posterior inferior facial height between groups (figure 2A), though many investigations that analyzed activator-headgear combination1,7,12,13,17 and Bionator9,18,22 revealed more increase with treatment secondary to mandibular advancement. However, as to the anterior inferior facial height, the discrepancy was evident (figure 2A), showing statistically significantly more improvement in response to treatment with the appliances, as occurred in other studies1,12,13,18,21,22,25. This behavior was followed by the corresponding tegument facial height (figure 2B), thus with larger values, probably because of the major nasal base stability in comparison with the anterior nasal spine.
As expected, the anterior superior facial height showed similar changes in all groups, as there is no influence from treatment in this region (figure 2B). However, the knowledge of how much it increases with growth provides important information about facial height proportions. The magnitude of the changes obtained supports the results of Wisth26, who verified approximately 1mm/year of nasal height growth.
Concerning the lip behavior, the main alterations in lower facial height were found to be originated from the lower lip, furthermore showing statistical difference between the control and experimental groups (figure 2B). This was also found in a study conducted by Lange et al.20. This result may be assigned to elongation of the lower lip, since it should be considered that the lower lip is frequently positioned behind the maxillary anterior teeth in Class II cases, and this led to lip deflection and deep mentolabial sulcus. As the orthopedic treatment induces lingual tipping of the maxillary incisors and proclination of the mandibular incisors, and then a reduction in overjet 1,7,9,10,12,13,17,19,21,23,25, the physical obstruction of the incisors will be eliminated, allowing normal position of the lip. There were similar changes on upper lip height between groups, reflecting the results of Lange et al.20 and Morris, Illing, Lee21. These authors mentioned the weak capacity of appliances to influence this structure (figure 2B).
The soft tissue convexity showed small decrease in all groups, yet which was more pronounced in groups A and B, though not significantly (figure 3A). Nasolabial angle did not differ between groups, but the direction of change was evidently distinct (figure 3A). While the combined activator-headgear appliance showed an increase in nasolabial angle, the other two caused a decrease, probably because of the major influence that this appliance has on maxillary growth1,10,21. The great individual variability and standard deviation could have made the statistical test unable to find behavior discrepancies in this variable24.
Labial protrusion at the level of point A', as of point labrale superius, did not demonstrate clear modifications in any group, and they were statistically similar (figures 3A and B, table III). This was also observed for the upper lip sulcus, as demonstrated by other investigators (Genecov, Sinclair, Dechow10). These data support the observations of Lange, et al.20 and Morris, Illing, Lee21. On the other hand, lower lip behavior was more influenced by the appliances. Sulcus depth decreased significantly more in experimental groups than in the control, following its increase in height, and also showed more lip protrusion, though the values did not achieve statistical significance (figure 3B). This result was already mentioned on a previous study1 and also occurred on the soft menton (figure 3A).
The different behavior tendency of the experimental groups in relation to the control should be considered. In this context, more subjects should be included in further studies, what would induce reduction in individual variability and, with a longer period of observation, could probably provide more capacity for the statistical test to find group discrepancies.
SUMMARY AND CONCLUSIONS
The purpose of this study was to evaluate the influence of Class II, division 1 treatment either with activator combined with extra-oral anchorage or Bionator on the soft tissue profile, growth pattern and facial heights. Twenty-four subjects were maintained as controls. Based on the methodology employed, the following was concluded:
1- The growth pattern was not significantly altered with treatment.
2- Posterior inferior facial height increased similarly in all groups, but the anterior showed significantly more increment in the two treated groups in relation to the control.
3- There was no difference in the soft tissue profile between groups as to the anterior superior facial height changes. On the other hand, the inferior followed its skeletal corresponding structure, meaning that it increased much more with treatment than without it, and was even more pronounced.
4- There was no or little influence of treatment on the upper lip and nose.
5- The lower lip demonstrated to be more influenced by treatment, though the only variable that expresses sulcus depth showed statistically significant changes between treated and untreated groups. The observation period was too small to detect differences on anterior soft menton advancement between all groups.
ACKNOWLEDGEMENTS
We would like to thank FAPESP for supporting this work.
Received: August 05, 2003 - Retturned for modification: Ovtober 10, 2003 - Accepted: February 19, 2004
- 1- Almeida MR. Avaliação cefalométrica comparativa da interceptação da má oclusão de classe II, 1ª divisão utilizando o aparelho de Fränkel e o Bionator de Balters. Bauru; 2000. [Thesis Bauru Dental School, University of São Paulo].
- 2- Almeida MR. Estudo cefalométrico comparativo, da ação de dois tipos de aparelhos ortopédicos, sobre as estruturas dentoesqueléticas e tegumentares de jovens de ambos os sexos com más oclusões de classe II, 1ª divisão. Bauru, 1997. [Thesis Bauru Dental School, University of São Paulo].
- 3- Andresen V apud Graber R, Neumann B. Removable orthodontic appliances. Philadelphia: W.B. Saunders; 1977 p. 103.
- 4- Andresen V, Häupl K apud Graber R, Neumann B. Removable orthodontic appliances. Philadelphia: W.B. Saunders; 1977 p. 105.
- 5- Ascher F. The Bionator. In: Graber R, Neumann B. Removable orthodontic appliances. Philadelphia: W.B. Saunders; 1977 p. 229-46.
- 6- Balters, W. Guia de la técnica del Bionator. Buenos Aires: Círculo Argentino de Odontologia; 1969.
- 7- Bishara SE, Ziaja, RR. Functional appliances: a review. Am J Orthod Dentofac Orthop. 1989; 95: 250-8.
- 8- Brangeli LAM, Henriques JFC, Vasconcelos MHF, Janson G. Estudo comparativo da análise cefalométrica pelo método manual e computadorizado. Rev Assoc Paul Cirurg Dent 2000; 54: 234-41.
- 9- Drelich RC. A cephalometric study of untreated class II, division 1 malocclusion. Angle Orthod 1948; 18: 70-5.
- 10- Genecov JS, Sinclair PM, Dechow PC. Development of the nose and soft tissue profile. Angle Orthod; 60: 191-8.
- 11- Hasund A apud Graber R, Neumann B. Removable orthodontic appliances. Philadelphia: W.B. Saunders, 1977 p. 633.
- 12- Henriques JFC, Maltagliati LA, Pinzan A, Freitas MR. Estudo longitudinal das características da má oclusão de classe II, 1a divisão sem tratamento, em jovens brasileiros, leucodermas, por um período médio de 3 anos e 4 meses. Rev Dental Press Ortod e Ortop Fac 1998; 3: 52-66.
- 13- Henriques JFC, Almeida MR, Janson GRP, Freitas MR, Alemida RR. Tratamento da má oclusão de classe II, 1a divisão com retrusão mandibular, utilizando o Bionator previamente à aparelhagem fixa: relato de um caso clínico. Ortodontia 1997; 30(3): 74-9.
- 14- Henriques JFC, Freitas MR, Santos-Pinto PR, Santos-Pinto CCM, Atta JY. Tratamento de uma classe II, divisão 1 com protrusão maxilar e retrusão mandibular, por meio de ortopedia associada à ortodontia. Ortodontia 1992; 25(3): 44-9.
- 15- Henriques JFC, Freitas MR, Scavone Júnior, H. Ativador conjugado ao aparelho extrabucal, durante o tratamento ortopédico-ortodôntico. Descrição do aparelho e relato de um caso clínico, Ortodontia 1993; 26: 46-56.
- 16- Houston WJB. A comparison of the reliability of measurement of cephalometric radiographs by tracings and direct digitization. Swed Dent J 1982; 15 Suppl: 99-103.
- 17- Kigele E. Cephalometric changes from activator-headgear treatment of Class II, division 1malocclusion. J Clin Orthod 1987; 21: 466-9.
- 18- Kumar S, Shidu SS, Kharbanda DP. A cephalometric evaluation of the dental and facial-skeletal effects using the Bionator with stepwise protrusive activations. J Clin Pedia Dent 1996; 20: 101-8.
- 19- Lagerström LO, Nielsen L, Lee R, Isaacson RJ. Dental and skeletal contributions to occlusal correction in patients treated with the high-pull headgear-activator combination. Am J Orthod Dentofac Orthop 1990; 97(6): 495-504.
- 20- Lange DW, Kalra V, Orth D, Broadbent BH, Powers M, Nelson S. Changes in soft tissue profile following treatment with the Bionator. Angle Orthod 1995; 65: 423-30.
- 21- Morris DO, Illing HM, Lee RT. A prospective evaluation of Bass, Bionator and Twin Block appliances. Part II -the soft tissues, Eur J Orthod 1998; 20: 663-84.
- 22- Ngan P, Wilson S, Florman M, Wei SHY. Treatment of class II open bite in the mixed dentition with a removable functional appliance and headgear. Quintessence Int 1992; 23: 323-33.
- 23- Öztürk Y, Tankuter N. Class II: a comparison of activator and activator headgear combination appliances. Eur J Orthod 1994; 16: 149-57.
- 24- Remmelink HJ, Tan BG. Cephalometric changes during headgear-reactivator treatment. Eur J Orthod 1991; 13: 466-70.
- 25- Sandler PJ. Reproducibility of cephalometric measurements. Br J Orthod 1988; 15: 105-10.
- 26- Wisth PJ. Changes of the soft tissue profile during growth. Trans Eur Orthod Soc 1973; 123-31.
Publication Dates
-
Publication in this collection
27 July 2004 -
Date of issue
June 2004
History
-
Received
05 Aug 2003 -
Reviewed
10 Oct 2003 -
Accepted
19 Feb 2004