Abstract
OBJECTIVE: The aim of the present study was to use facial analysis to determine the effects of rapid maxillary expansion (RME) on nasal morphology in children in the stages of primary and mixed dentition, with posterior cross-bite. MATERIAL AND METHODS: Facial photographs (front view and profile) of 60 patients in the pre-expansion period, immediate post-expansion period and one year following rapid maxillary expansion with a Haas appliance were evaluated on 2 occasions by 3 experienced orthodontists independently, with a 2-week interval between evaluations. The examiners were instructed to assess nasal morphology and had no knowledge regarding the content of the study. Intraexaminer and interexaminer agreement (assessed using the Kappa statistic) was acceptable. RESULTS: From the analysis of the mode of the examiners' findings, no alterations in nasal morphology occurred regarding the following aspects: dorsum of nose, alar base, nasal width of middle third and nasal base. Alterations were only detected in the nasolabial angle in 1.64% of the patients between the pre-expansion and immediate post-expansion photographs. In 4.92% of the patients between the immediate post-expansion period and 1 year following expansion; and in 6.56% of the patients between the pre-expansion period and one year following expansion. CONCLUSIONS: RME performed on children in stages of primary and mixed dentition did not have any impact on nasal morphology, as assessed using facial analysis.
Palatal expansion technique; Nasal bone; Airway resistance; Morphology
ORIGINAL ARTICLES
Photographic assessment of nasal morphology following rapid maxillary expansion in children
Omar Gabriel da Silva FilhoI; Tulio Silva LaraII; Priscila Vaz AyubIII; Amanda Sayuri Cardoso OhashiIV; Francisco Antônio BertozV
IDDS, MSc in Orthodontics, Araçatuba Dental School, UNESP - Univ. Estadual Paulista, Araçatuba, SP, Brazil; Orthodontist, Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo (HRAC-USP), Bauru, SP, Brazil
IIDDS, MSc in Orthodontics, Araçatuba Dental School, UNESP - Univ. Estadual Paulista, Araçatuba, SP, Brazil; Orthodontist, FUNCRAF, Hospital for Rehabilitation of Craniofacial Anomalies (HRAC-USP), University of São Paulo, Bauru, SP, Brazil
IIIDDS, Federal University of Mato Grosso do Sul, Campo Grande, MS, Brazil; Student, Orthodontic Course, Hospital for Rehabilitation of Craniofacial Anomalies (HRAC-USP), University of São Paulo, Bauru, SP, Brazil
IVDDS, Federal University of Pará, Belém, PA, Brazil; Resident, Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo (HRAC-USP), Bauru, SP, Brazil
VPhD, Orthodontics, Araçatuba Dental School, UNESP - Univ. Estadual Paulista, Araçatuba, SP, Brazil; Professor, Postgraduate Program in Orthodontics, Araçatuba Dental School, Araçatuba, SP, Brazil
Corresponding address Corresponding address: Omar Gabriel da Silva Filho Rua Rio Branco, 20-81 17014-037 - Bauru, SP - Brasil Phone: 55 14 32343348 / 55 14 32343239 e-mail: ortoface@travelnet.com.br
ABSTRACT
OBJECTIVE: The aim of the present study was to use facial analysis to determine the effects of rapid maxillary expansion (RME) on nasal morphology in children in the stages of primary and mixed dentition, with posterior cross-bite.
MATERIAL AND METHODS: Facial photographs (front view and profile) of 60 patients in the pre-expansion period, immediate post-expansion period and one year following rapid maxillary expansion with a Haas appliance were evaluated on 2 occasions by 3 experienced orthodontists independently, with a 2-week interval between evaluations. The examiners were instructed to assess nasal morphology and had no knowledge regarding the content of the study. Intraexaminer and interexaminer agreement (assessed using the Kappa statistic) was acceptable.
RESULTS: From the analysis of the mode of the examiners' findings, no alterations in nasal morphology occurred regarding the following aspects: dorsum of nose, alar base, nasal width of middle third and nasal base. Alterations were only detected in the nasolabial angle in 1.64% of the patients between the pre-expansion and immediate post-expansion photographs. In 4.92% of the patients between the immediate post-expansion period and 1 year following expansion; and in 6.56% of the patients between the pre-expansion period and one year following expansion.
CONCLUSIONS: RME performed on children in stages of primary and mixed dentition did not have any impact on nasal morphology, as assessed using facial analysis.
Key words: Palatal expansion technique. Nasal bone. Airway resistance. Morphology.
INTRODUCTION AND LITERATURE REVIEW
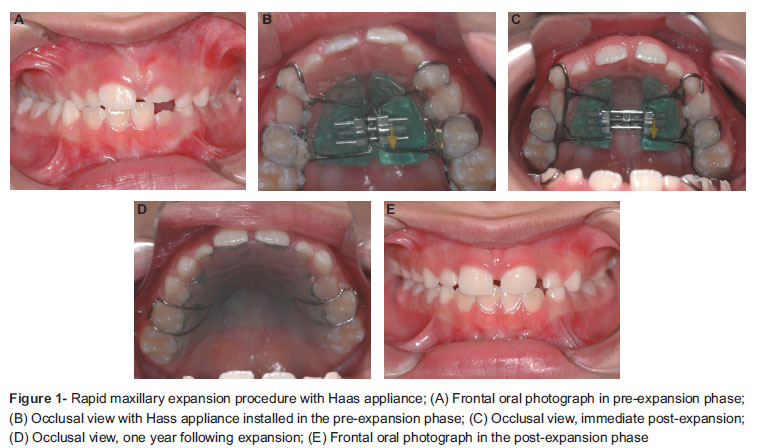
Maxillary atresia can be corrected with orthopedic expansion in a procedure known as rapid maxillary expansion (Figure 1)12. During this procedure, the halves of the maxilla are pushed apart in a pendulous manner in both the horizontal and frontal directions. Studies involving anteroposterior radiography have revealed important skeletal alterations attributed to the orthopedic expansion of the maxilla, such as enlargement of the width of the nose, maxilla and zygomatic process18,22,24. Hence, rapid maxillary expansion (RME) causes a variable increase in the width of the nasal cavity and volume, especially in the lower and anterior region3,6,8,12,13,16,18,20,24.
The distancing of the lateral walls of the nasal cavity improves the permeability of the nasal airway, as has been mentioned in subjective reports19. A number of authors have used rhinomanometry to objectively demonstrate that orthopedic expansion causes a significant reduction in nasal resistance10,13,25-27. Studies employing acoustic rhinometry corroborate the increase in volume of the nasal cavity following RME, with significant variations in nasal resistance with and without surgical assistance (LeFort I) in adult patients1,5,7,9,19.
Subjective and objective data suggest the possibility of structural and functional changes in the nasal cavity following RME. The structural change could contraindicate RME in children in the primary dentition stage due to the risk of producing undesirable clinical changes to the nose. The controversy increases with an interesting, isolated case report of a possible fracture of nasal bones caused by maxillary disjunction21. However, when a fracture of nasal bones occurs in children, it does not lead to medium- or long-term functional and morphological problems. The only implication is a temporarily altered nasal morphology and increased sensitivity to touch. The assessment of the behavior of the intercanthal distance (measured on a frontal facial photograph)4 has revealed an insignificant increase in adults with surgically assisted expansion as well as in pre-adolescents submitted to orthopedic expansion, thereby confirming the relative stability of the base of the skull during maxillary expansion.
The only article to assess facial alterations induced in the soft tissue by orthopedic expansion of the maxilla used measurements taken on standardized frontal photographs4. The most important result was the increase in nose width (measured at the height of the alas) of around 2 mm, which remained stable for at least 12 months after removing the expansion appliance. There are no other data in the literature addressing the influence of RME on the mid face using clinical facial analysis.
The aim of the present study was to use facial analysis of standardized frontal and profile facial photographs to determine the immediate and short-term effects of RME on nasal morphology in children in the stages of primary and mixed dentition, with posterior cross-bite.
MATERIAL AND METHODS
The sample was composed of 60 children (17 boys and 43 girls) with mean age of 8 years 7 months (maximum patient age: 12 years 10 months and minimum patient age: 6 years 1 month), selected from the files of the Service of Interceptive Orthodontics of the Hospital for Rehabilitation of Craniofacial Anomalies of the University of São Paulo, Bauru, SP, Brazil. All patients were either in the primary or mixed dentition stage, with posterior cross-bites, and were subjected to rapid maxillary expansion RME using a Haas appliance (Figure 1). The RME protocol involved one complete turn of the expander screw per day until obtaining adequate maxillary morphology. The parameter to expansion amount was the morphology of inferior dental arch. The screw was activated until the correction of posterior cross-bite with 2-3 mm of over-correction.
To be included in the study, the patients needed to have good-quality digital photographs of the face, with the head in the natural position (bi-pupil line parallel to the ground). Six photographs of each child were selected - three frontal (Figure 2) and three in profile (Figure 3). The three photographs corresponded to the pre-expansion period, immediate post-expansion period and one year following expansion.
The photographs were entered in the Microsoft Office PowerPoint 2007 program in sets of three. The first screen was mounted with the pre-expansion, immediate post-expansion and 1-year post-expansion photographs in the frontal view. The second screen was mounted with the pre-expansion, immediate post-expansion and 1-year post-expansion photographs of the profile. Hence, three photographs were arranged side-by-side on each screen to be analyzed and compared by three examiners.
The photographs were evaluated at two occasions by three independent experienced orthodontists, with a two-week interval between evaluations for the determination of the error of the method. On the second evaluation, only half of the sample (selected randomly) was evaluated. The examiners were unaware of the therapeutic approach performed on the patients and were instructed to look for alterations in the morphology of the following facial structures: dorsum of the nose, nasal-labial angle, alar base and nasal width of the middle third (Figure 4). The responses (yes or no) were recorded on a standardized chart. If any alteration in the morphology of any structure was found, the examiner was instructed to objectively describe the perceived alteration.
The results were collected and submitted to the Kappa test17 for analysis of the degree of agreement between evaluations. The mode among the examiners was used to determine the percent incidence of the alterations.
RESULTS
The results of the agreement percentages and Kappa values for the intraexaminer and interexaminer analyses are displayed in Tables 1 and 2, respectively.
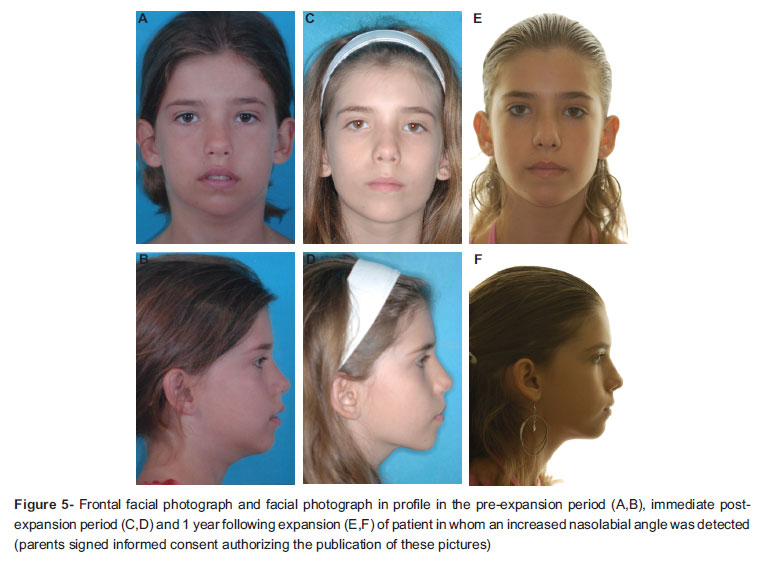
From the analysis of the mode of the examiners' findings, no alterations in nasal morphology were found in any of the patients when assessing the dorsum of the nose, alar base and width of the middle third (Table 3). Alterations were only detected in the nasolabial angle in 1.64% of the patients when comparing the pre-expansion and immediate post-expansion photos; in 4.92% of the patients when comparing the photos of the immediate post-expansion and one year following expansion; and in 6.56% of the patients when comparing the pre-expansion photos to those one year following expansion (Figures 5 and 6)
DISCUSSION
With so much scientific evidence available, RME has not been a novelty since the 1960s12. Since then, innumerous studies have clarified the skeletal and dental effects of RME as well as its positive repercussions on respiration5,7-11,13,16,19,20,24-27. RME thus have a variable orthopedic effect capable of causing favorable morphological changes to the nasomaxillary complex, but with a progressively lesser magnitude with age.
For orthodontists, the positive results of RME are mainly evidenced through occlusal analysis. RME constitutes transversal mechanics with the aim of establishing upper morphology and transversal dimensions compatible with normal, pleasing occlusion.
The present study is the first investigation to employ subjective, qualitative facial analysis with the purpose of evaluating the potential effects of RME on the nose. The sample was made up of children in the stages of primary and mixed dentition with posterior cross-bite of a skeletal nature. The connotation "skeletal" was given mainly considering the buccolingual slant of the posterior teeth ("torque"). The patients had posterior cross-bites with the upper posterior teeth positioned in the vestibular-lingual direction within the alveolar ridge. Thus, expansion would not change the vestibular-lingual slant of the posterior teeth. This implied an increase in the width of the upper dental arch without changing the torque of the posterior teeth. This characteristic is a reference for the diagnosis of skeletal atresia of the upper dental arch. Therefore, all children were subjected to RME using a Haas appliance with the same activation protocol of one complete turn per day (2/4 in the morning and 2/4 at night) until the correction of the posterior cross-bite with overcorrection.
Although it has an indisputable dental effect corresponding to the slant of the anchorage teeth in the vestibular direction, RME causes an increase in the width of the maxilla and nasal cavity3,6,8,11,12,13,16,18,20,22,24. The part of the maxilla most prone to the effects of RME is that which is closest to the appliance and farthest from the base of the skull. Thus, transversal alterations are more expressive at the point of the occlusal plane and diminished toward the base of the skull24.
As the maxilla is the bone that most contributes to the configuration of the mid face, it is reasonable to expect that the separation of the maxillary bones through RME causes some change to the morphological configuration of the face. This change can be assessed by cephalometric analysis, as done in two studies investigating the possible influences of RME on the soft tissues of the face, suggesting numerical sagittal changes in the soft tissue, such as anterior displacement of the tip of the nose, and an increase in the H angle and facial convexity as a consequence of the immediate maxilla advancement and mandible rotation downward and backward14,15. No changes in nasal prominence, thickness of the upper lip or thickness of the chin following RME were recorded15. These results reveal that RME is incapable of directly influencing the soft tissues. If there were some impact on the soft tissue, it would be reflected in changes in the subjacent hard tissues.
Frontal radiographs have proven the orthopedic effect on the maxilla, with increases in the width of the nasal cavity from 1 to 3 mm, 1.7 to 2.5 mm, around 2.08 mm, from 2 to 4.5 mm and of 3.47 mm3,12,13,16,24. One study employing computed tomography quantified a mean increase of 25% in the area and 15% in the volume of the nasal cavity20. Do such alterations imply changes in facial morphology? If so, are these changes positive or negative?
One report in the literature stimulated the development of the present investigation. This report discusses an undesirable change in the nasal morphology of a 5-year-old girl after activation of the expansion screw for 10 days, revealing the frailty of the inter-nasal suture at this age2. In the present study, we employed RME in the primary dentition, starting at 5 years of age23. Therefore, we decided to carry out a detailed assessment of the face of children subjected to orthopedic expansion of the maxilla, with special attention to nasal morphology. The analysis was performed using photographs of the patients prior to RME, immediately after the active phase of RME and 12 months following the conclusion of the active phase of RME. The goal was to assess the impact of the anatomical changes caused by RME in the primary and mixed dentition stages, above all, on the nasal area in the front and side views. The five structures evaluated were the dorsum of the nose, nasolabial angle, alar base, nasal width of the middle third and nasal base. Based on the results of the Kappa test for intraexaminer and interexaminer reliability (Tables 1 and 2), subjective facial analysis is a reliable method for the assessment of morphological alterations. According to the assessment of the three experienced orthodontists, only the nasolabial angle proved altered in 6% of the patients. The examiners were unanimous in stating that there was no change in the frontal and profile views of the face when comparing the three periods analyzed. This result reinforces what we have observed in the clinic: RME does not alter nasal morphology in children in the stages of primary and mixed dentition.
Facial analysis demonstrates that rapid RME has a minimal potential to alter facial morphology in the front view and profile. In practice, this finding is not surprising. In cases in which facial alteration is desired, such as in maxillary deficiency, facial convexity is increased with the reverse traction of the maxilla.
CONCLUSIONS
Facial analysis with standardized photographs of the frontal and profile views allows the conclusion that RME in children in the primary and mixed dentition stages does not lead to changes in the mid face or nasal morphology.
Received: July 22, 2009
Modification: March 20, 2010
Accepted: May 25, 2010
- 1- Babacan H, Sokucu O, Doruk C, Ay S. Rapid maxillary expansion and surgically assisted rapid maxillary expansion effects on nasal volume. Angle Orthod. 2006;76:66-71.
- 2- Bailey LJ, Sarver DM, Turvey TA, Profft WR. Class III problems. In: Profft WR, White RP, Sarver DM. Contemporary treatment of dentofacial deformity. St. Louis: Mosby; 2003. p.507-73.
- 3- Basciftci FA, Mutlu N, Karaman AI, Malkoc S, Küçükkolbasi H. Does the timing and method of rapid maxillary expansion have an effect on the changes in nasal dimensions? Angle Orthod. 2002;72:118-23.
- 4- Berger JL, Pangrazio-Kulbersh V, Thomas BW, Kaczynski R. Photographic analysis of facial changes associated with maxillary expansion. Am J Orthod Dentofacial Orthop. 1999;116:563-71.
- 5- Bicakci AA, Agar U, Sökücü O, Babacan H, Doruk C. Nasal airway changes due to rapid maxillary expansion timing. Angle Orthod. 2005;75:1-6.
- 6- Cameron CG, Franchi L, Baccetti T, McNamara JA Jr. Long term effects of rapid maxillary expansion: a posteroanterior cephalometric evaluation. Am J Orthod Dentofacial Orthop. 2002;121:129-35.
- 7- Ceroni Compadretti G, Tasca I, Alessandri-Bonetti G, Peri S, D'Addario A. Acoustic rhinometric measurements in children undergoing rapid maxillary expansion. Int J Pediatr Otorhinolaryngol. 2006;70:27-34.
- 8- Cross DL, McDonald JP. Effect of rapid maxillary expansion on skeletal, dental, and nasal structures: a postero-anterior cephalometric study. Eur J Orthod. 2000;22:519-28.
- 9- Doruk C, Sökücü O, Sezer H, Canbay EI. Evaluation of nasal airway resistance during rapid maxillary expansion using acoustic rhinometry. Eur J Orthod. 2004;26:397-401.
- 10- Enoki C, Valera FC, Lessa FC, Elias AM, Matsumoto MA, Anselmo-Lima WT. Effect of rapid maxillary expansion on the dimension of the nasal cavity and on nasal air resistance. Int J Pediatr Otorhinolaryngol. 2006;70:1225-30.
- 11- Franchi L, Baccetti T, Cameron CG, Kutcipal EA, McNamara JA. Thin-plate spline analysis of the short and long-term effects of rapid maxillary expansion. Eur J Orthod. 2002;24:143-50.
- 12- Haas AJ. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod. 1961;31:73-90.
- 13- Hershey HG, Steward BL, Warren DW. Changes in nasal airway resistance associated with rapid maxillary expansion. Am J Orthod. 1976;69:274-84.
- 14- Karamman AI, Basciftci FA, Gelgor I, Demir A. Examination of soft tissue changes after rapid maxillary expansion. World J Orthod. 2002;3:217-22.
- 15- Kiliç N, Kiki A, Oktay H, Erdem A. Effects of rapid maxillary expansion on Holdaway soft tissue measurements. Eur. J. Orthod. 2008;30:239-43.
- 16- Krebs A. Expansion on the midpalatal suture, studied by means of metallic implants. Acta Odontol Scand. 1959;92:491-501.
- 17- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159-74.
- 18- Oliveira NL, Silveira ACS, Kusnoto B, Viana G. Three-dimensional assessment of morphologic changes of the maxilla: a comparison of 2 kinds of palatal expanders. Am J Orthod Dentofacial Orthop. 2004;126;354-62.
- 19- Oliveira De Felippe NL, Silveira ACS, Viana G, Kusnoto B, Smith B, Evans CA. Relationship between rapid maxillary expansion and nasal cavity size and airway resistance: short- and long-term effects. Am J Orthod Dentofacial Orthop. 2008;134:370-82.
- 20- Palaisa J, Ngan P, Martin C, Razmus T. Use of conventional tomography to evaluate changes in the nasal cavity with rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2007;132:458-66.
- 21- Profft WR. Contemporary orthodontics. 4th ed. St. Louis: Mosby; 2007.
- 22- Sandikşioğlu M, Hazar S. Skeletal and dental changes after maxillary expansion in the mixed dentition. Am J Orthod Dentofacial Orthop. 1997;111:321-7.
- 23- Silva Filho OG, Ferrari Junior FM, Aiello CA, Zopone N. Correction of posterior crossbite in the primary dentition. J Clin Pediatr Dent. 2000;24:165-80.
- 24- Silva Filho OG, Montes LA, Torelly LF. Rapid maxillary expansion in the deciduous and mixed dentition evaluated through posteroanterior cephalometric analysis. Am J Orthod Dentofacial Orthop. 1995;107:268-75.
- 25- Timms DJ. The effect of rapid maxillary expansion on nasal airway resistance. Br J Orthod. 1986;13:221-8.
- 26- Warren DW, Hershey HG, Turvey TA, Hinton VA, Hairfeld WM. The nasal airway following maxillary expansion. Am J Orthod Dentofacial Orthop. 1987;91:111-6.
- 27- White BC, Woodside DG, Cole P. The effect of rapid maxillary expansion on nasal airway resistance. J Otolaryngol. 1989;18:137-43.
Corresponding address:
Publication Dates
-
Publication in this collection
29 Sept 2011 -
Date of issue
Oct 2011
History
-
Accepted
25 Mar 2010 -
Reviewed
20 Mar 2010 -
Received
22 July 2009