Abstracts
Giant prostatic hyperplasia is a rare condition characterized by very high volume benign prostatic enlargement (>500g). Few cases have been reported so far and most of them are associated with severe lower urinary symptoms. We report the first case of asymptomatic giant prostatic hyperplasia in an elderly man who had a 720g prostate adenoma, sudden gross hematuria and hypovolemic shock. The patient was successfully treated with open transvesical prostatectomy and had an uneventful postoperative recovery.
Prostatic hyperplasia; Prostatectomy; Hematuria; Hemorrhage; Shock, Lower urinary tract symptoms
A hiperplasia prostática gigante é uma condição rara caracterizada por aumento benigno prostático significativo, com volume maior que 500g. Existem poucos casos relatados e, em sua maioria deles está associada a sintomas graves do trato urinário inferior. Relatamos aqui o primeiro caso de hiperplasia prostática benigna assintomática em paciente idoso com próstata de 720g, hematúria macroscópica de início súbito e choque hipovolêmico. O paciente foi submetido com sucesso à prostatectomia suprapúbica, sem intercorrências no intra e pós-operatório.
Hiperplasia prostática; Prostatectomia; Hematúria; Hemorragia; Choque; Sintomas do trato urinário inferior
INTRODUCTION
Benign prostatic hyperplasia (BPH) is a common condition that affects many aging men and it may be associated with significant quality of life issues.
"Giant prostatic hyperplasia" (GPH) is a term that describes rare cases of extremely enlarged prostate glands, weighing greater than 500g.(11 Fishman JR, Merrill DC. A case of giant prostatic hyperplasia. Urology. 1993;42(3):336-7. Review.) Typically, patients with GPH have severe symptoms and seek medical care to treat their voiding complaints.
We report the first case, to our knowledge, of a man with GPH and without voiding symptoms, who presented sudden gross hematuria and hypovolemic shock.
CASE REPORT
An afro-descendent, 82-year-old man was admitted to the emergency room with painless macroscopic hematuria for 5 days without clots.
The patient denied any prior episodes of hematuria and did not complain of voiding symptoms. There was no history of smoking, alcohol abuse, severe comorbidities (the patient was treated with angiotensin-converting enzyme inhibitor to control mild arterial hypertension), or use of anti-coagulants or blood thinners.
On physical examination the patient was dehydrated and with pale mucosa. Upon admission his heart rate was 112bpm and blood pressure was 90/70mmHg. Abdominal palpation did not reveal any evident masses. The digital rectal examination revealed a large prostate with an estimated volume significantly greater than 100g, but with benign consistency and without nodules.
The individual underwent prompt bladder catheterization (with large catheter) and vesical irrigation with saline solution.
He also had acute renal insufficiency, with creatinine and urea levels of 1.9mg/dL and 64.0mg/dL, respectively. The patient underwent immediate volume resuscitation with saline and blood transfusion.
An abdominal ultrasound was performed when the patient was hospitalized in the emergency room, which demonstrated moderate bilateral hydronephrosis and a pelvic mass measuring 15x16x16cm. The computerized tomography (CT) scan had confirmed the evidence of urinary obstruction and a large pelvic mass representing the prostate (Figure 1).
Computerized tomography scan showing urinary obstruction (hydronephrosis) and a large pelvic mass representing the prostate
Prostatic specific antigen (PSA) levels measured after lower urinary tract manipulation were as high as 122.0ng/mL. Therefore, prostate trans-rectal ultrasound guided biopsies were performed to assess the possibility of a prostate adenocarcinoma or sarcoma. No evidence of malignancy was identified in the biopsy specimens.
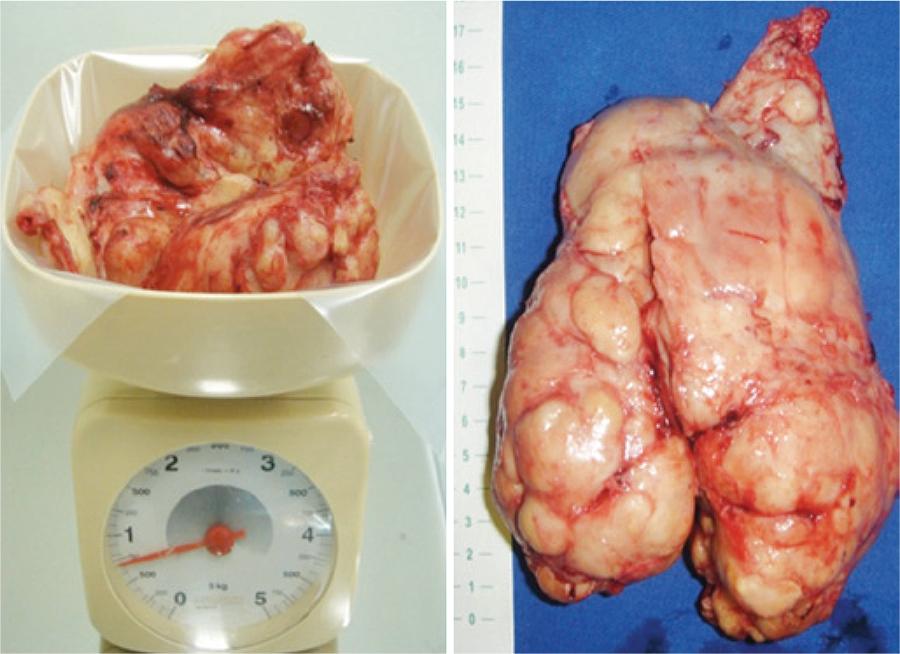
Subsequently, the patient underwent an uneventful open trans-vesical prostatectomy (TVP). The procedure time was about 100 minutes and the no further blood transfusions were required. The prostatic adenoma, extirpated as a single piece, measured 17x16x13.5cm and weighed 720g (Figure 2).
The prostatic adenoma, extirpated as a single piece, measuring 17.0x16.0x13.5cm and weighing 720g
Final pathological analysis revealed a whitish, firm and multinodular surface with cysts and diffuse hemorrhagic areas compatible with prostatic nodular hyperplasia with multiple anemic infarction foci and glandular squamous metaplasia.
At 1 year of follow-up, the patient returned to clinic with normal renal function, satisfactory urinary flow, and complete continence, although currently he is on treatment with anti-muscarinic medications due to urinary urgency.
DISCUSSION
The term "giant prostatic hyperplasia" was defined by Fishman and Merrill as glands exceeding 500g.(11 Fishman JR, Merrill DC. A case of giant prostatic hyperplasia. Urology. 1993;42(3):336-7. Review.) In our case, the preoperative CT showed a large pelvic mass representing the prostate and, after surgery, the specimen weight was 720g.
It is well-known that anatomic measurements of the prostate do not adequately distinguish patients who seek medical care from those who do not.(22 Jacobsen SJ, Girman CJ, Guess HA, Panser LA, Chute CG, Oesterling JE, et al. Do prostate size and urinary flow rates predict health care-seeking behavior for urinary symptoms in men? Urology. 1995;45(1):64-9.) Prostatic volume measured either by trans-rectal ultrasound or magnetic resonance imaging is poorly correlated with frequency, quality of life, urinary flow rate, residual urine, and pressure-flow parameters. However, it is unexpected for a man with such a large gland to remain asymptomatic prior to admission to the emergency room with hematuria and class III hemorrhagic, and hypovolemic shock, which require urgent blood transfusion.
Gross hematuria is an uncommon complaint in men with enlarged prostate, which is rarely seen as an initial presentation. Prior series report an prevalence rate of approximately 2.5% of macroscopic hematuria in men with BPH.(33 Hunter DJ, Berra-Unamuno A, Martin-Gordo A. Prevalence of urinary symptoms and other urological conditions in Spanish men 50 years old or older. J Urol. 1996;155(6):1965-70.)
The exact etiology of bleeding in men with enlarged prostate is unclear but may be attributable to increased microvessel density level(44 Foley SJ, Bailey DM. Microvessel density in prostatic hyperplasia. BJU international. 2000;85(1):70-3.) and vascular endothelial growth factors over-expression.(55 Häggström S, Tørring N, Møller K, Jensen E, Lund L, Nielsen JE, et al. Effects of finasteride on vascular endothelial growth factor. Scand J Urol Nephrol. 2002;36(3):182-7.) In addition, in these patients hypertension has been associated as a risk factor for hematuria.(66 Guo LJ, Tang Y, Guo CM, Zhang XH. Impact of primary hypertension on hematuria of the patients with benign prostatic hyperplasia. Chin Med J (Engl). 2010;5;123(9):1154-7.)
Biopsies to ensure malignancy status prior to initiate definitive treatment are of utmost importance given its potential impact on therapeutic choice. Prostate adenocarcinoma was one of the main concern in our patient given his age and elevated PSA (over 100ng/mL). Because of the size of the prostate, the sarcoma was another possibility that needed to be excluded,(77 Varghese SL, Grossfeld GD. The prostatic gland: malignancies other than adenocarcinomas. Radiol Clinics North Am. 2000;38(1):179-202. Review.) although such affection rarely induces PSA elevation.
Upper urinary tract deterioration and gross hematuria leading to hypovolemic shock are well-known indications for BPH surgical treatment. Although minimally invasive approaches such as robot-assisted simple prostatectomy(88 Vora A, Mittal S, Hwang J, Bandi G. Robot-assisted simple prostatectomy: multi-institutional outcomes for glands larger than 100 grams. J Endourol. 2012;26(5):499-502.) can be used for the treatment of BPH, the open surgery remains the gold standard procedure for benign, large volume, prostatic hyperplasia.(99 Rigatti P, Cestari A, Gilling P. The motion: large BPH should be treated by open surgery. Eur Urol. 2007;51(3):845-7; discussion 847-8.)
Sutherland et al. reported unsuccessful robot-assisted simple prostatectomy for a man with severe prostatomegaly (260g).(1010 Sutherland DE, Perez DS, Weeks DC. Robot-assisted simple prostatectomy for severe benign prostatic hyperplasia. J Endourol. 2011;25(4):641-4.) Hence, the analysis of a contemporary series of patients revealed that trans-vesical prostatectomy is associated with significant improvement in symptom score scales, post-void residual urine volume, and maximal flow rate, along with a low incidence of long-term complications and need of re-operation as well as a durable therapeutic effect.(1111 Varkarakis I, Kyriakakis Z, Delis A, Protogerou V, Deliveliotis C. Long-term results of open transvesical prostatectomy from a contemporary series of patients. Urology. 2004;64(2):306-10. Review.)
Similar to others,(1212 Ogawa S, Manome M, Yabe M, Kuma Y, Yamaoka M, Sato Y, et al. A giant prostatic hyperplasia treated by open surgery. Int J Gen Med. 2012;5:1009-12.) we consider simple prostatectomy as the primary recommended treatment option for GPH. For this reason, a suprapubic open trans-vesical prostatectomy was performed. Operation time was short and no major complications occurred.
GPH is an extremely rare condition. A MEDLINE/PubMed search revealed no more than 20 reports of prostates weighing greater than 500.(1313 Akpo E, Akpo M. Giant benign prostatic hyperplasia in a nigerian: report of a case. The Internet Journal of Urology. 2010;8(1).,1414 Üçer O, Baser O, Gümüs B. Giant prostatic hyperplasia: Case report and literature review. Dicle Medical Journal. 2011;38(4):489-91.) The above reported case is among the five greatest prostate glands ever described,(1414 Üçer O, Baser O, Gümüs B. Giant prostatic hyperplasia: Case report and literature review. Dicle Medical Journal. 2011;38(4):489-91.) and it is the first one with such unusual presentation, characterized by a complete absence of voiding symptoms followed by sudden gross hematuria that resulted in hypovolemic shock.
REFERENCES
-
1Fishman JR, Merrill DC. A case of giant prostatic hyperplasia. Urology. 1993;42(3):336-7. Review.
-
2Jacobsen SJ, Girman CJ, Guess HA, Panser LA, Chute CG, Oesterling JE, et al. Do prostate size and urinary flow rates predict health care-seeking behavior for urinary symptoms in men? Urology. 1995;45(1):64-9.
-
3Hunter DJ, Berra-Unamuno A, Martin-Gordo A. Prevalence of urinary symptoms and other urological conditions in Spanish men 50 years old or older. J Urol. 1996;155(6):1965-70.
-
4Foley SJ, Bailey DM. Microvessel density in prostatic hyperplasia. BJU international. 2000;85(1):70-3.
-
5Häggström S, Tørring N, Møller K, Jensen E, Lund L, Nielsen JE, et al. Effects of finasteride on vascular endothelial growth factor. Scand J Urol Nephrol. 2002;36(3):182-7.
-
6Guo LJ, Tang Y, Guo CM, Zhang XH. Impact of primary hypertension on hematuria of the patients with benign prostatic hyperplasia. Chin Med J (Engl). 2010;5;123(9):1154-7.
-
7Varghese SL, Grossfeld GD. The prostatic gland: malignancies other than adenocarcinomas. Radiol Clinics North Am. 2000;38(1):179-202. Review.
-
8Vora A, Mittal S, Hwang J, Bandi G. Robot-assisted simple prostatectomy: multi-institutional outcomes for glands larger than 100 grams. J Endourol. 2012;26(5):499-502.
-
9Rigatti P, Cestari A, Gilling P. The motion: large BPH should be treated by open surgery. Eur Urol. 2007;51(3):845-7; discussion 847-8.
-
10Sutherland DE, Perez DS, Weeks DC. Robot-assisted simple prostatectomy for severe benign prostatic hyperplasia. J Endourol. 2011;25(4):641-4.
-
11Varkarakis I, Kyriakakis Z, Delis A, Protogerou V, Deliveliotis C. Long-term results of open transvesical prostatectomy from a contemporary series of patients. Urology. 2004;64(2):306-10. Review.
-
12Ogawa S, Manome M, Yabe M, Kuma Y, Yamaoka M, Sato Y, et al. A giant prostatic hyperplasia treated by open surgery. Int J Gen Med. 2012;5:1009-12.
-
13Akpo E, Akpo M. Giant benign prostatic hyperplasia in a nigerian: report of a case. The Internet Journal of Urology. 2010;8(1).
-
14Üçer O, Baser O, Gümüs B. Giant prostatic hyperplasia: Case report and literature review. Dicle Medical Journal. 2011;38(4):489-91.
Publication Dates
-
Publication in this collection
30 June 2015 -
Date of issue
Jul-Sep 2015
History
-
Received
7 July 2013 -
Accepted
23 Apr 2014