Abstracts
OBJECTIVE: To compare clinical, radiological and laboratory aspects of household contacts, aged 15 or younger, of patients presenting a positive culture for Mycobacterium tuberculosis. METHODS: This was a cohort study comparing children and adolescents (< 15 years of age) who were household contacts of TB cases presenting positive sputum smear and positive culture results (exposed group, n = 100) or negative sputum smear and positive culture results (unexposed group, n = 55). All of the contacts were evaluated via the TB control program of a university hospital in the city of Vitória, Brazil, between July of 2003 and December of 2006. RESULTS: Of the 155 minors evaluated, 87 (56.1%) were female and 68 (43.9%) were male. Of those 155, 28 (18%) were aged 5 or younger, 62 (40%) were aged 5-9, and 65 (42%) were aged 10-15. Symptoms of the disease were found in 17 (17%) of the 100 contacts in the exposed group and in 9 (16%) of the 55 in the unexposed group (p = 0.86). Chest X-rays showed alterations in 20 (21%) and 2 (4%) of the contacts in the exposed and unexposed groups, respectively (RR = 6.9; p = 0.004). In the exposed and unexposed groups, respectively, 35 (38%) and 10 (18%) of the contacts presented positive results in the tuberculin skin test (RR = 2.8; p = 0.01). Of the 100 contacts in the exposed group, 5 (5%) were diagnosed with TB, which was not diagnosed in any of those in the unexposed group (p = 0.08). CONCLUSIONS: Although no significant difference was found between the two groups regarding the incidence of TB, it is of note that there is a greater risk of becoming infected with M. tuberculosis if the bacterial load of the index case is high.
Tuberculosis; Mycobacterium tuberculosis; Tuberculosis, pulmonary; Child; Adolescent
OBJETIVO: Comparar aspectos clínicos, radiológicos e laboratoriais de contatos domiciliares, menores de 15 anos, de pacientes com cultura positiva para Mycobacterium tuberculosis. MÉTODOS: Realizou-se um estudo de coorte comparando crianças e adolescentes (< 15 anos) que eram contatos domiciliares de casos de TB com baciloscopia e cultura positiva (grupo exposto, n = 100) ou com baciloscopia negativa e cultura positiva (grupo não-exposto, n = 55). Todos os contatos foram avaliados no período de julho de 2003 a dezembro de 2006, no programa de controle da TB de um hospital universitário na cidade de Vitória (ES). RESULTADOS: Das 155 contatos avaliados, 87 (56,1%) eram do sexo feminino e 68 (43,9%) do masculino. Do total, 28 (18%) eram menores de 5 anos; 62 (40%), entre 5-9 anos; e 65 (42%), entre 10-15 anos. Foi detectada a presença de sintomas de TB em 17 (17%) dos 100 contatos no grupo exposto e em 9 (16%) dos 55 no grupo não-exposto (p = 0,86). A radiografia de tórax apresentou alterações em 20 (21%) e 2 (4%) dos contatos nos grupos exposto e não-exposto, respectivamente (RR = 6,9; p = 0,004). Nos grupos exposto e não-exposto, respectivamente, 35 (38%) e 10 (18%) dos contatos apresentaram prova tuberculínica positiva (RR = 2,8; p = 0,01). No total, 5 contatos (5%) do grupo exposto foram diagnosticados com TB, ao passo que não houve diagnóstico de TB no grupo não-exposto (p = 0,08). CONCLUSÕES: Apesar desta pesquisa não ter encontrado diferença significativa no surgimento de casos de TB entre os comunicantes dos grupos estudados, deve-se ressaltar que quanto maior a carga bacilar do caso índice, maior é a chance dos seus contatos virem a se infectar por M. tuberculosis.
Tuberculose; Mycobacterium tuberculosis; Tuberculose pulmonar; Criança; Adolescente
ORIGINAL ARTICLE
Juvenile household contacts aged 15 or younger of patients with pulmonary TB in the greater metropolitan area of Vitória, Brazil: a cohort study*
Ethel Leonor Noia MacielI; Luiza Werner Heringer VieiraII; Lucília Pereira Dutra MolinaIII; Rosana AlvesIV; Thiago Nascimento do PradoV; Reynaldo DietzeVI
IAdjunct Professor of Epidemiology. Infectious Diseases Center, Health Sciences Center, Federal University of Espírito Santo, Vitória, Brazil
IIDatabase manager. Infectious Diseases Center, Health Sciences Center, Federal University of Espírito Santo, Vitória, Brazil
IIIMasters Student. Postgraduate Program in Infectious Diseases, Federal University of Espírito Santo, Vitória, Brazil
IVProfessor of Clinical Medicine. Faculdade Brasileira - UNIVIX, Brazilian College - Vitória, Brazil
VMasters Student. Postgraduate Program in Infectious Diseases, Federal University of Espírito Santo, Vitória, Brazil
VICoordinator. Infectious Diseases Center, Health Sciences Center, Federal University of Espírito Santo, Vitória, Brazil
Correspondence to
ABSTRACT
OBJECTIVE: To compare clinical, radiological and laboratory aspects of household contacts, aged 15 or younger, of patients presenting a positive culture for Mycobacterium tuberculosis.
METHODS: This was a cohort study comparing children and adolescents (< 15 years of age) who were household contacts of TB cases presenting positive sputum smear and positive culture results (exposed group, n = 100) or negative sputum smear and positive culture results (unexposed group, n = 55). All of the contacts were evaluated via the TB control program of a university hospital in the city of Vitória, Brazil, between July of 2003 and December of 2006.
RESULTS: Of the 155 minors evaluated, 87 (56.1%) were female and 68 (43.9%) were male. Of those 155, 28 (18%) were aged 5 or younger, 62 (40%) were aged 5-9, and 65 (42%) were aged 10-15. Symptoms of the disease were found in 17 (17%) of the 100 contacts in the exposed group and in 9 (16%) of the 55 in the unexposed group (p = 0.86). Chest X-rays showed alterations in 20 (21%) and 2 (4%) of the contacts in the exposed and unexposed groups, respectively (RR = 6.9; p = 0.004). In the exposed and unexposed groups, respectively, 35 (38%) and 10 (18%) of the contacts presented positive results in the tuberculin skin test (RR = 2.8; p = 0.01). Of the 100 contacts in the exposed group, 5 (5%) were diagnosed with TB, which was not diagnosed in any of those in the unexposed group (p = 0.08).
CONCLUSIONS: Although no significant difference was found between the two groups regarding the incidence of TB, it is of note that there is a greater risk of becoming infected with M. tuberculosis if the bacterial load of the index case is high.
Keywords: Tuberculosis; Mycobacterium tuberculosis; Tuberculosis, pulmonary; Child; Adolescent.
Introduction
Worldwide, TB continues to be one of the principal public health problems, as well as one of the leading causes of morbidity and mortality, accounting for approximately 9 million new cases and 2 million deaths per year.(1) This situation is aggravated in developing countries, where approximately 95% of new TB cases and 98% of the deaths are concentrated.(2)
Regarding pediatric TB, the actual situation remains unknown. This is principally due to the difficulty in diagnosing the disease, since signs and symptoms are nonspecific in this age bracket.(3) In addition, the information provided by the World Health Organization (WHO) typically refers to cases that have been bacteriologically confirmed. However, children find it difficult to produce sputum for the performance of the bacteriological diagnosis. In addition, 80% of sputum test results are negative.(4)
It is estimated that, in developing countries, there are approximately 1,300,000 new cases and 450,000 deaths from TB per year among individuals under the age of 15.(5,6) It is also estimated that 15% of all TB cases reported in Brazil are in children and adolescents aged 15 or younger.(7) In the state of Espírito Santo, 85 (5.7%) of the 1,490 cases reported in 2005 were cases of pediatric TB.(8)
In an attempt to control this problem, the WHO launched the first international guide related to pediatric TB-Guidance for National Tuberculosis Programmes on the Management of Tuberculosis in Children-in 2006.(9) This guide emphasizes the importance of clinical, radiological and epidemiological data consistent with TB for definition of the diagnosis. In addition, it shows one of the principal risk factors for pediatric TB: the household contact with patients who had been recently diagnosed with infectious TB. Therefore, this guide underscores the diagnostic importance of reviewing the history of contacts with adult TB patients. The Brazilian National Ministry of Health (NMH) ratifies that concept, emphasizing the surveillance of contacts of patients with active pulmonary TB as a relevant strategy, since it allows the transmission to be interrupted when cases of infection and disease are identified.(10)
Based on this information, the Programa de Controle da Tuberculose do Hospital Universitário Cassiano Antonio de Moraes (PCT/HUCAM, Tuberculosis Control Program of the Cassiano Antonio de Moraes University Hospital) has been developing measures, since 2003, related to TB control in this age bracket. One of these measures is the evaluation of contacts aged 15 or younger. In this context, we conducted this study at the PCT/HUCAM, in order to compare clinical, radiological and laboratory aspects of children and adolescents who had been in contact with patients presenting positive or negative sputum smear results for Mycobacterium tuberculosis and positive culture results.
Methods
A cohort study was conducted, comparing children and adolescents aged 15 or younger whose index case presented positive direct sputum smear and positive culture results (exposed group) with those whose index case presented negative sputum smear and positive culture results (unexposed group). The index cases were PCT/HUCAM participants between July of 2003 and December of 2006. This is a referral program for the treatment of patients with TB in the state of Espírito Santo.
The exposed group comprised contacts (children and adolescents aged 15 or younger) whose index case presented positive direct sputum smear and positive culture results. The unexposed group comprised contacts within the same age bracket whose index case presented negative direct sputum smear and positive culture results.
After the diagnosis of the index case, an interview was conducted in order to identify any household contacts. These family members were then invited to the facility and, when there was any family member aged 15 or younger, the index cases and their contacts were invited to participate in the study.
For data collection, we used a research instrument designed to categorize and list the data related to demographic characteristics, clinical history and epidemiological history of the participants registered in the charts. In addition, chest X-ray results, tuberculin skin test results and bacteriological test results were collected for the index cases. Laboratory data (sputum smear microscopy and culture for mycobacteria) were obtained directly from the Mycobacteriology Laboratory of the Infectious Diseases Center of the Federal University of Espírito Santo.
Chest X-ray findings were considered suspicious when at least one of the following patterns was identified: right hilar lymph node enlargement, infiltration, cavitation, atelectasis and miliary pattern. As recommended by the NMH, cough, fever, weight loss or any other symptom deemed as significant by the physician were considered TB symptoms. The tuberculin skin test was defined as positive when the induration was > 10 mm in patients who had been vaccinated more than two years prior, and > 15 mm in those who had been vaccinated within the last two years.(10)
We designed a data collection form containing all of the items of the NMH scoring system (Chart 1). The forms were used by physician researchers in order to collect patient data and to classify the children into one of three diagnostic categories: unlikely (criterion 0), possible (criterion 1) and highly likely (criterion 2). In case of classification as criterion 1, the child was referred for gastric lavage.(11)
Suspected cases were monitored immediately following diagnosis and two months after the gastric lavage was performed, in order to make the definitive diagnosis. In addition, the legal guardians were instructed to seek medical attention at any time if they noticed a change in the clinical profile of the child.
After the interviews had been carried out, all of the questionnaires were reviewed by the interviewer and, subsequently, by one of the field supervisors. The questionnaires were then grouped into lots and sent for data compilation. For quality control purposes, approximately 5% of the interviews were repeated with the mothers or legal guardians of the child, using an abbreviated version of the questionnaire. The main objective of the quality control was not to validate the questions but rather to guarantee that the interviews were being carried out in a thorough and appropriate fashion.
Data compilation of the questionnaires followed an independent double data entry strategy, carried out by two data entry clerks. At the end of the data entry of each lot, the two data entries were compared and errors were listed. Subsequently, each of the data entry clerks made the necessary corrections, which were followed by a new comparison. If necessary, a new cycle of corrections was carried out. Typically, few inconsistencies remained; those were corrected by the data entry supervisor, and the process was concluded. At the end of the consistency-checking process, the data were stored in a database so that variables could be established. All personal information that was necessary for the identification of the index case and of the children for subsequent cohort visits, were entered into a separate database and forwarded to the study coordinator, so that it would not be possible to identify the index cases or children in any of the phases of data analysis. Data entry was carried out using the Epi Info program, version 6.4, and validated using a programmed routine of the STATA program, version 9.0 (Stata Corp, College Station, TX, USA). The entire consistency-checking process and the establishment of variables process were conducted using this program.
Some simple procedures facilitated the process of identifying the children and the questionnaires, as well as the data compilation after each visit. For the perfect compilation of records, there should be one unique identifier for each individual. Therefore, from the outset, a number was assigned in order to identify each child, built as follows: the number of the index case (composed of two digits), to which we added two digits in reference to the order in which the under-15 family contact was treated and two additional digits in reference to their age.
Subsequently, statistical analyses were conducted using the STATA statistical package, version 9.0. Absolute and relative values were calculated for each variable. The chi-square test of association was used in the comparison between the groups in terms of the dichotomous variables studied, with the level of significance set at < 0.05.
The study was approved by the Human Research Ethics Committee of the Health Sciences Center of the Federal University of Espírito Santo. Children who presented positive results on the tuberculin skin test or with a confirmed TB diagnosis were referred for chemoprophylaxis or for the initiation of treatment, respectively, as established by the NMH.(10)
Results
During the study period, 345 patients were diagnosed via the PCT/HUCAM. Of these, 52 patients reported no household contacts and did not participate in this study; as did 14 patients who were part of a prison population; 103 patients had no family members under the age of 15; and 39 declined to participate in the study.
The study comprised 155 children and adolescents aged 15 or younger who were household contacts of 137 adult patients with TB. Regarding gender, 87 (56.1%) were females and 68 (43.9%) were males. The age bracket was distributed as follows: 28 (18%) of the contacts were younger than 5 years of age; 62 (40%) were between 5-9 years of age; and 65 (42%) were 10-15 years of age.
The study sample comprised 99 exposed patients and 56 unexposed patients. When we evaluated this variable in the two groups studied, no significant difference was observed between the groups (p = 0.41), as described in Table 1. We observed that 58 individuals in the exposed group (59%) and 29 in the unexposed group (52%) were females. Consequently, 41 (41%) and 27 individuals (48%), respectively, in the exposed and unexposed groups, were males. Regarding age, in the exposed group, 18 contacts (18%) were younger than 5 years of age; 39 (39%) were between 5-9 years of age; and 42 (43%) were between 10-15 years of age. In the unexposed group, 10 (18%) were younger than 5 years of age; 23 (41%) were between 5-9 years of age; and 23 (41%) were between 10-15 years of age. There was no statistically significant difference between the groups regarding age (p = 0.95).
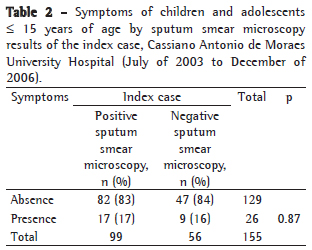
Symptoms of the disease were present in 17 (17%) and in 9 (16%) of the participants in the exposed and unexposed groups, respectively, as demonstrated in Table 2. There were no statistically significant differences (p = 0.86).
Regarding the evaluation of chest X-ray findings, this examination was performed in 97 participants in the exposed group, and the results were suspicious in 20 (21%), as shown in Table 3. In contrast, in the unexposed group, only 2 (4%) of the 55 individuals who were submitted to this test were considered under suspicion (RR = 6.9; p = 0.004). In addition, 35 individuals in the exposed group (38%) and 10 individuals in the unexposed group (18%) presented positive tuberculin skin test results (RR = 2.8; p = 0.01). It should be noted that, in the case of 28 patients, who received the BCG vaccination, on average, within the last two years, the result was only considered positive when the induration was > 15 mm.
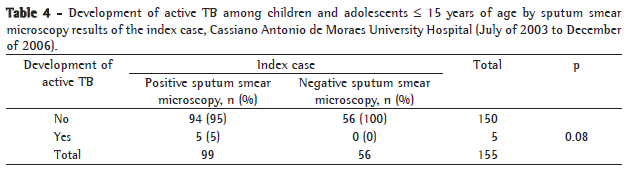
Using the NMH scoring system, we classified 10 children as criterion 1 and referred them for gastric lavage, as follows: 9 from the exposed group and 1 from the unexposed group. As shown in Table 4, there were more contacts of patients with positive sputum smear microscopy. There were 5 individuals (5%) diagnosed with the disease in the exposed group, and none of those in the unexposed group were so diagnosed (p = 0.08). It is notable that these children developed the disease in the first four months after the index case had been identified. Only 1 child presented positive sputum smear microscopy (in one sample) and positive culture, 3 were identified through culture of the gastric lavage fluid, and 1 was identified through sputum culture.
Discussion
Pediatric TB is a neglected problem. According to the WHO, this "orphan disease" exists in the shadow of adult TB and is a significant problem that affects the health of children.(12) However, pediatric TB is neglected because the child typically presents negative sputum smear microscopy and is therefore considered to have little importance in TB transmission.(13) Nevertheless, it is in this age bracket that TB presents the greatest impact, due to its higher rates of morbidity and mortality.(14) Only 5-10% of infected adults will develop the disease at some stage of their lives, versus 43% of infants aged 1 year or less, 24% of children aged 1-5 years and 15% of adolescents (11-15 years).(15)
As stated, the likely source of infection of children with TB is the adults with whom they interact.(7) Therefore, the evaluation of contacts becomes a compulsory strategy in TB programs. Some authors have stated that the investigation of TB in children in contact with bacilliferous adults is one of the most simple and most easily carried out TB control measures.(7)
In our study, we observed that 35 children (38%) whose contacts presented positive sputum smear results also presented positive tuberculin skin test results and, among the unexposed, only 18% presented the same results, demonstrating that these children in contact with adult patients with active TB were 2.8 times more likely to be infected with M. tuberculosis than were those who were contacts of adults with negative sputum smear microscopy. In a study carried out in Rio de Janeiro,(16) of the 181 children submitted to the tuberculin skin test, a strong reaction was observed in 110 contacts (59.8%), and a > 15 mm reaction was detected in 66 children (35.9%). It should be noted that the diagnosis of latent infection with M. tuberculosis through the tuberculin skin test in children is greatly affected by the BCG vaccination or by the exposure to environmental mycobacteria, which affects its specificity. Although the new NMH guidelines define as positive only a > 15 mm reaction in individuals vaccinated within the last two years and a > 10 mm reaction in those vaccinated more than two years before, there is no consensus on these interpretations in the literature.(10,16-18)
In order to avoid the low specificity of the tuberculin skin test, two new commercial tests, based on IFN-γ expression-Interferon Gamma Release Assays (IGRAs)-synthesized by lymphocytes in response to specific antigens of M. tuberculosis (ESAT-6 and CFP-10), have recently been shown to be more specific and more sensitive than are tuberculin tests in the identification of latent infection with M. tuberculosis and of active TB.(19-21) In May of 2005, the ex vivo QuantiFERON®-TB Gold test (Cellestis Ltd., Carnegie, Victoria, Australia) was finally approved by the United States Food and Drug Administration for marketing as an auxiliary method in the diagnosis of infection with M. tuberculosis.(22) Another test, also licensed, T-SPOT.TB (Oxford Immunotec, Oxford, UK), uses the Elispot technique to measure peripheral blood mononuclear cells that produce IFN-γ.
The IGRAs have proven to have various major advantages over the tuberculin skin test, such as high specificity, as well as the fact they require only a single contact with the patient and are carried out ex vivo, thereby reducing the risk of adverse effects and eliminating the booster effect, which is typical of serial testing. Among the disadvantages, the following stand out: the high cost of these tests compared with the tuberculin skin test; the need for a well-equipped laboratory; the careful blood sample collection required; and the subsequent mandatory careful handling in order to maintain the feasibility of the lymphocytes. Unfortunately, there are no data on how well IGRAs perform in children.
Another complementary exam in the diagnosis of pediatric pulmonary TB is the chest X-ray, which is one of the pillars of the diagnosis, albeit not highly specific, for the analysis of the evolution of the lesions and evaluation of the treatment response.(10) However, these findings are often insufficient to warrant treatment initiation, and cavitations are rarer in pediatric TB, hence the need to evaluate other parameters for the definition of the case.(15) In our study, 20 individuals (21%) in the exposed group and only 2 (4%) in the unexposed group were suspected cases, the difference being statistically significant (p = 0.004). Therefore, children in contact with bacilliferous adults were 6.9 times more likely to present chest X-ray results that raise the suspicion of TB.
The signs and symptoms of TB vary considerably, ranging from asymptomatic to severe disseminated forms, with significant weight loss and evolving to death.(23) In the present study, 26 children (16.8%) presented TB symptoms. In a study carried out in Rio de Janeiro,(16) 25% of the children (46/181) were symptomatic, the most common symptom being cough. In our study, there were no statistically significant differences between the groups (p = 0.86) when comparing the presence of symptoms. We observed that 17% and 16% patients, respectively, in the exposed and unexposed groups were symptomatic. Weight loss was the most common symptom (in 38%), followed by cough (in 27%).
The investigation of contacts made it possible to diagnose 5 children (3.2%) with pulmonary TB. The diagnosis of these children was confirmed through positive microbiological results. A similar result was observed in a study carried out in São Paulo,(24) which reported a 3.8% incidence of TB in contacts aged 15 or younger. In our study, although the difference was not statistically significant, all pulmonary TB cases were infant contacts of patients with positive sputum smear microscopy. Studies show the need to identify the presence of cavitations in patients. One group of authors carried out a study comparing bacterial load results from sputum samples collected from patients with pulmonary cavitation and from those without, using quantitative culture methods. Mean detection time of positive cultures using the Bactec 460 method was evaluated in the two groups.(25) The authors observed that patients with cavitary disease presented a greater number of CFU and lower mean detection time than did those without cavitary disease. Our findings support the hypothesis that higher bacterial loads in index cases translate to greater risk of the contacts becoming infected with M. tuberculosis.
This underscores the importance of epidemiological surveillance and pediatric TB control measures, principally through the control of contacts of adult patients with active TB, for the early prevention or identification of TB cases. In addition, in order to institute chemoprophylaxis in this age bracket, it is essential that investigations be conducted in young individuals in contact with patients with positive or negative sputum smear microscopy. Despite the lower bacterial load of the latter, we detected an infection rate of 18% among these cases, which indicates the need to investigate contacts in all patients diagnosed with pulmonary TB.
References
-
1World Health Organization. Global Tuberculosis Control - Surveillance, Planning, Financing. Geneva: WHO; 2006.
-
2World Health Organization. Global Tuberculosis Control - Surveillance, Planning, Financing. Geneva: WHO; 1998.
- 3. Houwert KA, Borggreven PA, Schaaf HS, Nel E, Donald PR, Stolk J. Prospective evaluation of World Health Organization criteria to assist diagnosis of tuberculosis in children. Eur Respir J. 1998;11(5):1116-20.
- 4. Sant'Anna CC, Hijjar MA. Recente contribuição da Organização Mundial de Saúde para o controle da Tuberculose na Infância. Rev Saúde Pública. 2007;41(Suppl 1):S117-S20.
- 5. Starke JR, Jacobs RF, Jereb J. Resurgence of tuberculosis in children. J Pediatr. 1992;120(6): 839-855.
- 6. Starke JR. Childhood tuberculosis. A diagnostic dilemma. Chest. 1993;104(2):329-30.
- 7. Sant'Anna CC, Mourgues LV, Ferrero F, Balanzat AM. Diagnóstico e terapêutica da tuberculose infantil - uma visão atualizada de um antigo problema. Jornal de Pediatr (Rio J). 2002;78(Suppl 2):S205-S14.
- 8. Maciel ELN, Marinato AC, Bandeira CFR, Tonini MS, Dietze R, Ramos MC. O perfil epidemiológico da tuberculose em crianças e adolescente menores de 15 anos na Grande Vitória, Brasil, no período de 1990-2001. Cad Saúde Colet. 2006;14(1):81-94.
- 9. World Health Organization. Guidance for national tuberculosis programmes on the management of tuberculosis in children. Geneva: WHO; 2006.
- 10. Brasil. Ministério da Saúde. Secretaria de Políticas de Saúde. Departamento de Atenção Básica. Manual técnico para o controle da tuberculose: cadernos de atenção básica. Brasília: Ministério da Saúde; 2002.
- 11. Maciel EL, Dietze R, Silva RE, Hadad DJ, Struchiner CJ. Evaluation of a scoring system recommended by the Brazilian Ministry of Health for the diagnosis of childhood tuberculosis [Article in Portuguese]. Cad Saúde Pública. 2008;24(2):402-8.
- 12. World Health Organization. A research agenda for childhood tuberculosis: improving the management of childhood tuberculosis within national tuberculosis programmes: research priorities based on a literature review. Genebra: WHO; 2007.
- 13. Donald PR. Children and tuberculosis: protecting the next generation? Lancet. 1999;353(9157):1001-2.
- 14. Marcondes E, Vaz FA, Ramos, JL, Okay Y, editors. Pediatria Básica. São Paulo: Sarvier; 2003.
- 15. Hartwig SV, Ignotti E, Oliveira BF, Pereira HC, Scatena JH. Evaluation of surveillance of contacts of new tuberculosis cases in the state of Mato Grosso - Brazil. J Bras Pneumol. 2008;34(5):298-303.
- 16. Caldeira ZM, Sant'Anna CC, Aidé MA. Controle de crianças e adolescentes comunicantes de tuberculosos, Rio de Janeiro, RJ. Rev Saúde Publica. 2004;38(3):339-45.
- 17. Tidjani O, Amedome A, ten Dam HG. The protective effect of BCG vaccination of the newborn against childhood tuberculosis in an African community. Tubercle. 1986;67(4):269-81.
- 18. Liebeschuetz S, Bamber S, Ewer K, Deeks J, Pathan AA, Lalvani A. Diagnosis of tuberculosis in South African children with a T-cell-based assay: a prospective cohort study. Lancet. 2004;364(9452):2196-203.
- 19. Kang YA, Lee HW, Yoon HI, Cho B, Han SK, Shim YS, et al. Discrepancy between the tuberculin skin test and the whole-blood interferon gamma assay for the diagnosis of latent tuberculosis infection in an intermediate tuberculosis-burden country. JAMA. 2005;293(22):2756-61.
- 20. Doherty TM, Demissie A, Olobo J, Wolday D, Britton S, Eguale T, et al. Immune responses to the Mycobacterium tuberculosis-specific antigen ESAT-6 signal subclinical infection among contacts of tuberculosis patients. J Clin Microbiol. 2002;40(2):704-6.
- 21. Mazurek GH, Jereb J, Lobue P, Iademarco MF, Metchock B, Vernon A, et al. Guidelines for using the QuantiFERON-TB Gold test for detecting Mycobacterium tuberculosis infection, United States. MMWR Recomm Rep. 2005;54(RR-15):49-55. Erratum in: MMWR Morb Mortal Wkly Rep. 2005;54(50):1288.
- 22. Pai M, Riley LW, Colford JM Jr. Interferon-gamma assays in the immunodiagnosis of tuberculosis: a systematic review. Lancet Infect Dis. 2004;4(12):761-76.
- 23. Houwert KA, Borggreven PA, Schaaf HS, Nel E, Donald PR, Stolk J. Prospective evaluation of World Health Organization criteria to assist diagnosis of tuberculosis in children. Eur Respir J. 1998;11(5):1116-20.
- 24. Morrone N, Solha MSS. Incidência de tuberculose-doença e de teste tuberculino positivo em crianças expostas a pacientes com tuberculose. Importância dos fatores ligados a fonte e a criança, até mesmo vacinação previa com BCG intradérmico. AMB Rev Assoc Med Bras. 1983;29(11/12):182-8.
- 25. Palaci M, Dietze R, Hadad DJ, Ribeiro FK, Peres RL, Vinhas SA, et al. Cavitary disease and quantitative sputum bacillary load in cases of pulmonary tuberculosis. J Clin Microbiol. 2007;45(12):4064-6.
Publication Dates
-
Publication in this collection
19 May 2009 -
Date of issue
Apr 2009
History
-
Accepted
30 Oct 2008 -
Received
06 Oct 2008