Abstracts
Cryptococcosis is a systemic mycosis caused by two species of the encapsulated basidiomycetes, Cryptococcus neoformans and C. gattii, which, respectively, cause infection in immunocompromised individuals and in immunologically normal hosts. Patients with T-cell deficiencies are more susceptible to this infection. The spectrum of the disease ranges from asymptomatic pulmonary lesions to disseminated infection with meningoencephalitis. The medical relevance of cryptococcosis increased dramatically as a consequence of the AIDS epidemic and organ transplants.
Cryptococcus neoformans; Pneumonia; Acquired immunodeficiency syndrome; Amphotericin B; Fluconazole
Criptococose é uma micose sistêmica causada por duas espécies do basidiomiceto encapsulado, Cryptococcus neoformans e C. gattii, que, respectivamente, causam infecção em indivíduos imunocomprometidos e em hospedeiros imunocompetentes, respectivamente. Pacientes com deficiência em células T são mais suscetíveis. A infecção se inicia por lesões pulmonares assintomáticas e a doença disseminada frequentemente cursa com meningoencefalite. A importância médica da criptococose aumentou significativamente em consequência da epidemia da AIDS e dos transplantes de órgãos.
Cryptococcus neoformans; Pneumonia; Síndrome da imunodeficiência adquirida; Anfotericina B; Fluconazol
CONTINUING EDUCATION COURSE - MYCOSES
Chapter 3 - Pulmonary cryptococcosis*
Cecília Bittencourt SeveroI; Alexandra Flávia GazzoniII; Luiz Carlos SeveroIII
IDoctoral Student in Pulmonology. Postgraduate Program in Pulmonology, Universidade Federal do Rio Grande do Sul - UFRGS, Federal University of Rio Grande do Sul - Porto Alegre, Brazil
IIPostdoctoral Student. Universitat Rovira, Virgili, Spain
IIIAssociate Professor. Department of Internal Medicine of the Universidade Federal do Rio Grande do Sul - UFRGS, Federal University of Rio Grande do Sul - School of Medicine, Porto Alegre, Brazil
Correspondence to
ABSTRACT
Cryptococcosis is a systemic mycosis caused by two species of the encapsulated basidiomycetes, Cryptococcus neoformans and C. gattii, which, respectively, cause infection in immunocompromised individuals and in immunologically normal hosts. Patients with T-cell deficiencies are more susceptible to this infection. The spectrum of the disease ranges from asymptomatic pulmonary lesions to disseminated infection with meningoencephalitis. The medical relevance of cryptococcosis increased dramatically as a consequence of the AIDS epidemic and organ transplants.
Keywords: Cryptococcus neoformans; Pneumonia; Acquired immunodeficiency syndrome; Amphotericin B; Fluconazole.
Introduction
Cryptococcosis is an infection caused by the naturally encapsulated basidiomycete of the genus Cryptococcus, which has recently become the most relevant opportunistic fungal pathogen.(1) The infection caused by the species C. neoformans has become the most critically relevant opportunistic infection as a consequence of the AIDS epidemic. In addition, C. gattii recently caused an isolated cryptococcosis outbreak among apparently immunocompetent humans and animals on Vancouver Island, Canada.(2)
Cryptococcus spp. are currently divided into five capsular serotypes and eight molecular genotypes. The serotype classification is based on the agglutination reactions of capsular polysaccharide antigens. Serotype A and serotype D strains, as well as the AD hybrid, are classified as C. neoformans, whereas serotype B and serotype C strains have been classified as C. gattii. Serotype A strains have been designatedC. neoformans var. grubii, whereas serotype D strains have been designated C. neoformans var. neoformans.(3) This classification was based on the differences in capsular structure and DNA between the strains, as well as on a complete comparison of the genomic sequencing of these two serotypes (strains).(3) In addition, based on new molecular data and on evolutionary studies, each one of the two species comprises four molecular types: VNI to VNIV (C. neoformans); and VGI to VGIV (C. gattii).(1)
The life cycle of Cryptococcus spp. comprises two stages, i.e., sexual and asexual. Cryptococcus neoformans (variants grubii and neoformans) and Cryptococcus gattii are considered to be anamorphic (asexual) strains. The corresponding teleomorphic (sexual) strains are Filobasidiella neoformans and F. bacillispora, respectively.(4)
The virulence of the genus Cryptococcus is associated with the production of oxidases and proteases, as well as with the antiphagocytic properties of the capsular polysaccharide. Atypical (non-capsulated) forms present lower pathogenicity. An environment in which there are high concentrations of carbon dioxide favors the bioformation of the capsule.(5)
Cryptococcus spp. present in host tissue as encapsulated yeast (asexual form), which makes them unique among pathogenic fungi. Cryptococcus spp. are observed with or without budding; they are also observed as multi-budding, poorly-encapsulated or capsule-deficient fungal elements or as pseudohyphae.(6-9)
In the environment, C. neoformans is found in association with pigeon excreta and in tree hollows worldwide. For years, C. gattiiwas found only in tropical and subtropical regions. C. gattii was primarily associated with eucalypti, which were considered to be its environmental niche. However, the unprecedented emergence of manyC. gattiiisolates on Vancouver Island shows that the distribution and ecology of C. gattii is changing with its ability to associate itself with a wide variety of trees, such as firs and oaks.(1,10)
The most theoretically plausible explanation for the infection is the diameter (1.2-1.8 µm) of the fungal propagules (basidiospores), which can accumulate in the alveoli and, at a temperature of 37ºC, change into capsulated yeasts.(11,12) The host develops a primary pulmonary lymph node complex. In most cases, the inhalation of Cryptococcus spp. causes a self-limiting, asymptomatic pulmonary infection, and the yeasts might remain latent within this complex, die or, in the event of subsequent immunosuppression, be reactivated and cause disease. This primary infection can also cause pulmonary symptoms in the host in cases of immunosuppression or of massive inoculation of the yeast. The dissemination from the lungs to other organs can potentially occur as a result of a primary or secondary infection.
In the stage of dissemination from the lungs, the brain is the organ most likely to be the target of that dissemination and to present clinically relevant disease. Therefore, most data refer to manifestations of the disease in the lungs or in the central nervous system (CNS).(13) This tropism for the CNS is attributed to the optimal cerebrospinal fluid (CSF) concentration of nutrients (thiamine, glutamic acid, glutamine, dopamine, carbohydrates and minerals) that can be assimilated by the fungus, to the inactivity of the complement system in the CSF and to the weakness or absence of inflammatory activity in brain tissue.(14)
Before the HIV epidemic, cryptococcosis was an uncommon systemic infection that affected patients with immunosuppression generally associated with the following: use of corticosteroids; diabetes mellitus; Hodgkin's disease; systemic lupus erythematosus; or other types of immunosuppressive therapy.(15,16) However, the incidence of cryptococcosis has increased dramatically in the last two decades. More than 80% of the cases of cryptococcosis worldwide have been associated with HIV infection.(17)
In the pre-combined antiretroviral (cARV) therapy era, cryptococcosis became the major opportunistic infection and the major cause of death among HIV-infected patients with CD4 < 100 cells/µl. After the potent cARV therapy became available, the incidence of cryptococcosis decreased significantly; however, the incidence of cryptococcosis in patients who are not infected by HIV has not changed during this period.(18,19) Although the increase in cARV therapy use is associated with the decrease in the incidence of cryptococcosis in developed countries, the incidence of and mortality from cryptococcosis remain extremely high in countries in which the HIV epidemic is uncontrolled and in which access to drugs and health care is limited.(1,20) In developed countries, cryptococcosis has not disappeared because the high-risk groups continue to increase, which is due to the advances in transplantation medicine and to the creation of new immunosuppressive therapies.(21) In Brazil, cryptococcosis is a public health issue in patients with AIDS.(22,23)
Among the cases of cryptococcosis in humans, C. neoformans var. grubii (serotype A) is the species that is most commonly isolated from clinical samples worldwide.(24) This serotype accounts for more than 95% of the cases of cryptococcosis. C. neoformans var. neoformans (serotype D, less thermotolerant) commonly causes disease in certain European countries and in the United States.(1) Until recently, C. gattii (serotypes B and C) was found to cause cryptococcosis in tropical and subtropical areas such as Australia, southern Asia and Central Africa, as well as in tropical and subtropical areas of the Americas.(25) In Brazil, studies have shown that serotype A is the most prevalent, followed by serotypes B, D and AD.(26)
Clinical manifestations
The organs that constitute the CNS and the respiratory tract are the most affected by C. neoformans and C. gattii infections, although other organs, such as the skin, prostate, eyes, bones and urinary tract, as well as the blood, might be infected.(27,28) In fact, this yeast can cause disease in any organ of the human body, and cryptococcosis can disseminate to multiple organs in severely immunocompromised patients.(29-31)
It was previously believed that the clinical manifestations of C. neoformans infection and of C. gattii infection were similar. However, evidence has confirmed that the clinical manifestations of C. neoformans infection and of C. gattii infection can be different.(32,33)C. gattii, for instance, causes disease in immunocompetent hosts with large inflammatory masses (cryptococcomas) and commonly produces neurological sequelae that require surgery and long-term antifungal therapy.(33)C. neoformans, however, affects immunocompromised patients, causing small pulmonary lesions (seen on X-rays) associated with meningitis (Figure 1), and, due to its proteolytic activity, presents cryptococcemia and cryptococcuria, manifestations that are rarely found in C. gattii infections.(7)
The presentation of cryptococcosis in HIV-infected patients is somewhat different from that in non-HIV-infected patients.(30) The association between HIV and cryptococcosis causes greater extrapulmonary and CNS involvement and a high rate of positive India ink (nigrosin) test results and of positive blood culture results. In addition, this association results in few inflammatory cells in the CSF. These clinical results suggest that HIV-infected patients present a high concentration of organisms and a minimal inflammatory reaction at the site of infection.
In addition to being the main point of entry for these fungi, the lung is the site that is most commonly affected by cryptococcosis and presents various clinical manifestations that range from asymptomatic infection, such as a solitary nodule, to severe pneumonia.(30) Patients with acute pulmonary cryptococcosis can present fever, productive cough, chest pain and weight loss.(34)
The organs that constitute the CNS are the most commonly affected by C. neoformans and C. gattii, which can cause acute, subacute or chronic meningitis, as well as severe meningoencephalitis. The signs and symptoms are generally present for various weeks and include headache, fever, cranial neuropathy, altered level of consciousness, lethargy, memory loss, signs of meningeal irritation and coma.(30)
Radiological diagnosis
The principal radiological findings are solitary or multiple nodules, subpleural masses and consolidation with air bronchogram. Other findings, less common, include pleural effusion, hilar lymphadenopathy, diffuse reticulonodular opacity and endobronchial lesions resulting in airway obstruction with pulmonary collapse, as well as findings that mimic pulmonary metastases.(1,35,36)
Isolated pulmonary cryptococcosis (without brain metastasis) or pulmonary cryptococcosis accompanied by brain mass (with brain metastasis) caused by C. gattii can mimic lung cancer clinically and radiologically (Figures 2 and 3).(37) Cases of upper lobe consolidation with atypical presentation of Pancoast syndrome have been described.(38)
Pulmonary manifestations are more common than CNS manifestations in immunocompromised patients with cryptococcosis.(39) In fact, the authors of one study found that more than 90% of HIV/AIDS patients with pulmonary cryptococcosis have previously been diagnosed with CNS cryptococcosis.(1) In contrast, CNS involvement in HIV-negative patients with pulmonary cryptococcosis is less common.(1)
Laboratory diagnosis
Direct examination
Direct microscopic examination of the CSF using India ink staining to screen for encapsulated yeasts is a low-cost, widely used test that does not require advanced technology. This technique can be employed immediately after a lumbar puncture to visualize encapsulated yeasts of 5-20 µm in diameter on average. Microscopy has a sensitivity of 30-50% in cases of cryptococcal meningitis in patients without AIDS and a sensitivity of up to 80% in patients with AIDS-related cryptococcal meningitis.(1)
Histopathological examination
The histopathological identification of cryptococcosis is achieved through basic histochemical techniques, namely H&E staining and the Grocott-Gomori methenamine-silver stain (GMS) technique, as well as through special histochemical techniques, namely Mayer's mucicarmine (MM) staining and the Fontana-Masson (FM) staining (Table 1).(40,41)
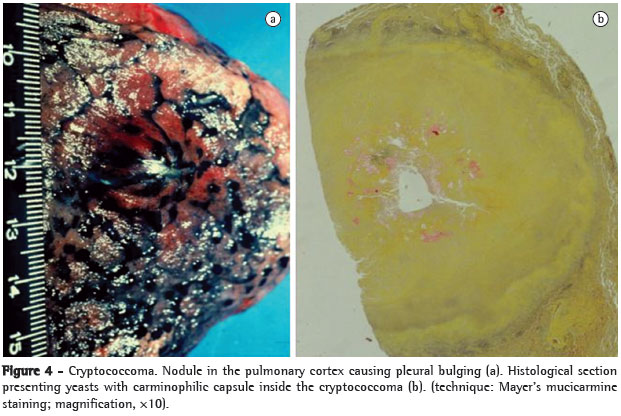
According to the classification proposed by Schwartz, cryptococcosis is divided into two histological categories, i.e., reactive and minimally reactive, based on the tissue reactions of the host and revealed by H&E staining.(42) The reactive pattern is characterized by a granulomatous inflammatory response composed of histiocytes, multinucleated giant cells and lymphocytic infiltration.(41-46) The yeasts are primarily intracellular (phagocytosis).(41,46) Regions of necrosis are occasionally associated with neutrophilic infiltrates.(42,43,46) Fibrotic nodules-cryptococcomas, considered to be a variant of the reactive pattern-are also found. Fibrotic nodules are formed by surrounding fibrotic tissue and present central areas of necrosis that contain yeasts and a variable number of inflammatory cells (Figure 4).(42,47) According to data from the literature, the variant form is related to infection caused by C. gattii.(48)
The minimally reactive pattern is characterized by minimal or no inflammatory response.(42,43) Numerous spherical microorganisms or oval microorganisms (or a combination of the two) of 2-20 µm in diameter, surrounded by a light halo and arranged extracellularly, are seen.(40,42,43) In some cases, complete destruction of tissue architecture is observed (Figure 5).(40) According to some authors, the minimally reactive inflammatory pattern can be suggestive of poor prognosis.(42,43)
The GMS technique is widely used to screen for fungal elements in tissue sections and in smears.(41) The GMS technique reveals morphological characteristics, such as cell wall and budding, and light perinuclear halos surrounding the microorganisms. Active lesions contain numerous budding fungal structures. Single or multiple buds with narrow bases are common (Figure 5).(40) Uncommon forms, which include pseudohyphae, germ tube-like structures and chains of budding yeasts, are easily identified by the GMS technique.(9,40,49)
According to various studies, MM staining (Figure 5) is a specific method for visualizing the mucopolysaccharide capsules of Cryptococcus spp.(8,30,40,42) Through the magenta staining of the capsule, it is possible to distinguish between yeast and other fungi, similar in size and shape.(41,50)
The FM staining (Figure 5) reveals the melanin present on the fungal cell wall.(30,41) The use of the FM staining is limited to cases in which MM staining results do not suffice to confirm the presence of Cryptococcus spp. Therefore, the FM staining is an alternative for diagnosing cases of infections caused by capsule-deficient organisms morphologically suggestive of Cryptococcus spp.(41)
The budding index and carminophilic index
The biological activity of Cryptococcus spp. is characterized through a reliable scale developed to determine the budding index (BI) and the carminophilic index (CI) of the yeast.(42,43) The BI is calculated through the percentage of microorganisms that exhibit one or more buds, and it is indicative of in vivo replication.(42) The CI is calculated by determining the percentage of microorganisms with capsule (stained by the histochemical technique of MM staining) and is indicative of capsular synthesis.(43) According to one group of authors, the BI and CI are both higher in the minimally reactive histological pattern than in the reactive pattern.(42) Therefore, there is an inverse correlation between high capsular production and a less intense inflammatory response. According to Schwartz, the scale is potentially useful for interpreting the inflammatory response of the host, for prognosis and for biological activity, demonstrating that the granulomatous response is associated with the control of infection.
Differential diagnosis
The histopathological identification of fungal agents is an excellent diagnostic method because the structures are easily detected through histochemical techniques.(14)
The micromorphological characteristics of Cryptococcus spp. with intact capsule are distinct, and the diagnosis is unique, since the microorganisms are usually associated with a minimal inflammatory response.(14,40) In capsule-deficient fungi, the histological characteristics are rather unspecific, being also found in other pathologies of infectious origin.(41)
The use of special staining techniques is justified by the fact that Cryptococcus spp., due to their variable micromorphology, mimic other yeast-like fungi.(51) The identification of the capsule through MM staining is the first step to distinguish the yeast from other fungi of similar size and shape.(40,41,51) The greatest difficulty lies in identifying capsule-deficient microorganisms because, due to their smaller size, they are mistaken for the following: Histoplasma capsulatum; immature spherules of Coccidioides immitis; small forms of Blastomyces dermatitidis and Paracoccidioides brasiliensis; Candida glabrata; and Sporothrix schenckii.(7,51-54) In these cases, the special histochemical staining of FM is used, allowing the differential diagnosis between unusual micromorphological forms of Cryptococcus spp. and the fungal structures that mimic this type of yeast.(41,51)
Culture
C. neoformans and C. gattii grow easily from biological samples smeared onto standard culture media such as Sabouraud dextrose agar, and colonies can be observed after 48-72 h of incubation at 30-35ºC under aerobic conditions.
The Cryptococcus spp. isolates can be distinguished from Candida spp. through a medium enriched with seeds of Guizotia abyssinica (Niger seed agar), which contains phenolic substrates and detects the phenoloxidase activity in Cryptococcus spp. by forming melanin, therefore staining the colonies brown.
The species can be determined based on the characteristics of the colors on the L-canavanine-glycine-bromothymol blue medium.(55)
Serology
Tests to detect the capsular polysaccharide antigen of Cryptococcus spp. in the serum and CSF have been widely used and are some of the principal serological tests performed in mycology. The tests use latex particles covered with polyclonal antibodies to the cryptococcal capsule. The sensitivity and specificity of latex agglutination tests for cryptococcal antigen range from 93 to 100% and from 93 to 98%, respectively.(56)
Treatment
Regarding the diagnosis of pulmonary cryptococcosis, it is essential to guarantee that the disease has not disseminated, especially to the CNS, due to the need for a more aggressive treatment strategy if neurocryptococcosis has developed. The choice of antifungal agent depends on the site of infection and on the immunity of the patient. The principal antifungal agents are amphotericin B (0.5-1.0 mgkg-1day-1) and its lipid derivatives, i.e., fluconazole (400 mg/day) and 5-flucytosine (100 mgkg-1day-1 in combination with amphotericin B because resistance to monotherapy is common).(5) Unfortunately, 5-flucytosine is not available in Brazil.
In cases of mild or moderate isolated pulmonary cryptococcosis, treatment with fluconazole or itraconazole (200-400 mg/day) can be administered for 6-12 months. In case of dissemination to the CNS, itraconazole should not be used because it does not penetrate the CSF efficiently.(5)
Amphotericin B deoxycholate has been successfully used to treat patients with cryptococcal meningitis because it promotes rapid Cryptococcus spp. clearance. However, this drug can cause severe nephrotoxicity. The use of liposomal amphotericin B has the advantage of reducing this toxicity.(5)
Treatment varies according to the species of Cryptococcus. C. gattii requires a higher dose of amphotericin B, longer treatment duration and, more often than not, surgery. Likewise, sequelae are more common, and mortality is higher.
The correct use of antifungal agents significantly decreases mortality; however, long-term continuous therapy is required in order to prevent recurrence.(57)
Prevention
Prevention of infection
There is no evidence that exposure to pigeon feces is associated with an increased risk of developing cryptococcosis. However, it is advisable to avoid sites contaminated with bird feces.
Prevention of disease
The latex test for the presence of cryptococcal antigen in the serum of asymptomatic individuals should not be routinely performed, due to a low probability of diagnosis.(57)
Prospective clinical studies have shown that the use of fluconazole and itraconazole can reduce the frequency of the disease among patients with AIDS. However, antifungal prophylaxis should not be routinely performed for the following reasons: the mycosis is uncommon; antifungal prophylaxis has little impact on survival; drug interactions can occur; antifungal resistance can develop; and treatment costs are high. However, prophylaxis should be considered for patients with CD4+ T lymphocyte < 50 cells/µl. In these cases, fluconazole (100-200 mg/day) is the drug of choice.(57)
The use of secondary prophylaxis in previously treated, cured patients prevents the recurrence of the infection.(43) Secondary prophylaxis should be maintained until CD4+ T lymphocyte levels remain higher than 200 cells/µl for more than 6 months.(57)
References
- 1. Chayakulkeeree M, Perfect JR. Cryptococcosis. Infect Dis Clin North Am. 2006;20(3):507-44, v-vi.
- 2. Kidd SE, Hagen F, Tscharke RL, Huynh M, Bartlett KH, Fyfe M, et al. A rare genotype of Cryptococcus gattii caused the cryptococcosis outbreak on Vancouver Island (British Columbia, Canada). Proc Natl Acad Sci USA. 2004;101(49):17258-63.
- 3. Franzot SP, Salkin IF, Casadevall A. Cryptococcus neoformans var. grubii: separate varietal status for Cryptococcus neoformans serotype A isolates. J Clin Microbiol. 1999;37(3):838-40.
- 4. Kwon-Chung KJ, Bennett JE, Rhodes JC. Taxonomic studies on Filobasidiella species and their anamorphs. Antonie Van Leeuwenhoek. 1982;48(1):25-38.
- 5. Subramanian S, Mathai D. Clinical manifestations and management of cryptococcal infection. J Postgrad Med. 2005;51 Suppl 1:S21-6.
- 6. Capone D, Gonçalves AJ, Andrade EM, Peyneau A, Wanke B, Montessi J, et al. Criptococose pulmonar por Cryptococcus neoformans não capsulado. J Bras Med. 1986;50(5):67, 69-70.
- 7. Severo LC. Criptococose: duas doenças? [thesis]. Porto Alegre: Fundação Faculdade Federal de Ciências Médicas de Porto Alegre; 1993
- 8. Severo LC, Londero AT, Martins SC, Reolon M, Geyer RG. Provável criptococose pulmonar causada por Cryptococcus neoformans não-capsulado. Rev Inst Med Trop Sao Paulo. 1981;23(6):283-6.
- 9. Williamson JD, Silverman JF, Mallak CT, Christie JD. Atypical cytomorphologic appearance of Cryptococcus neoformans: a report of five cases. Acta Cytol. 1996;40(2):363-70.
- 10. Kwon-Chung KJ, Bennett JE. Epidemiologic differences between the two varieties of Cryptococcus neoformans. Am J Epidemiol. 1984;120(1):123-30.
- 11. Cohen J, Perfect JR, Durack DT. Cryptococcosis and the basidiospore. Lancet. 1982;1(8284):1301.
- 12. Zimmer BL, Hempel HO, Goodman NL. Pathogenicity of the basidiospores of Filobasidiella neoformans. Mycopathologia. 1984;85(3):149-53.
- 13. Cohen J. The pathogenesis of cryptococcosis. J Infect. 1982;5(2):109-16.
- 14. Littman ML, Schneierson SS. Cryptococcus neoformans in pigeon excreta in New York City. Am J Hyg. 1959;69(1):49-59.
- 15. Kwon-Chung KJ, Kozel TR, Edman JC, Polacheck I, Ellis D, Shinoda T, et al. Recent advances in biology and immunology of Cryptococcus neoformans. J Med Vet Mycol. 1992;30 Suppl 1:133-42.
- 16. Mitchell TG, Perfect JR. Cryptococcosis in the era of AIDS--100 years after the discovery of Cryptococcus neoformans. Clin Microbiol Rev. 1995;8(4):515-48.
- 17. Hajjeh RA, Conn LA, Stephens DS, Baughman W, Hamill R, Graviss E, et al. Cryptococcosis: population-based multistate active surveillance and risk factors in human immunodeficiency virus-infected persons. Cryptococcal Active Surveillance Group. J Infect Dis. 1999;179(2):449-54.
- 18. Mirza SA, Phelan M, Rimland D, Graviss E, Hamill R, Brandt ME, et al. The changing epidemiology of cryptococcosis: an update from population-based active surveillance in 2 large metropolitan areas, 1992-2000. Clin Infect Dis. 2003;36(6):789-94.
- 19. Dromer F, Mathoulin-Pélissier S, Fontanet A, Ronin O, Dupont B, Lortholary O, et al. Epidemiology of HIV-associated cryptococcosis in France (1985-2001): comparison of the pre- and post-HAART eras. AIDS. 2004;18(3):555-62.
- 20. Friedman GD, Jeffrey Fessel W, Udaltsova NV, Hurley LB. Cryptococcosis: the 1981-2000 epidemics. Mycoses. 2005;48(2):122-5.
- 21. Hage CA, Wood KL, Winer-Muram HT, Wilson SJ, Sarosi G, Knox KS. Pulmonary cryptococcosis after initiation of anti-tumor necrosis factor-alpha therapy. Chest. 2003;124(6):2395-7.
- 22. Soares MC, Paula CR, Dias AL, Caseiro MM, Costa SO. Environmental strains of Cryptococcus neoformans variety grubii in the city of Santos, SP, Brazil. Rev Inst Med Trop Sao Paulo. 2005;47(1):31-6.
- 23. Pappalardo MC, Melhem MS. Cryptococcosis: a review of the Brazilian experience for the disease. Rev Inst Med Trop Sao Paulo. 2003;45(6):299-305.
- 24. Bennett JE, Kwon-Chung KJ, Howard DH. Epidemiologic differences among serotypes of Cryptococcus neoformans. Am J Epidemiol. 1977;105(6):582-6.
- 25. Jenney A, Pandithage K, Fisher DA, Currie BJ. Cryptococcus infection in tropical Australia. J Clin Microbiol. 2004;42(8):3865-8.
- 26. Nishikawa MM, Lazera MS, Barbosa GG, Trilles L, Balassiano BR, Macedo RC, et al. Serotyping of 467 Cryptococcus neoformans isolates from clinical and environmental sources in Brazil: analysis of host and regional patterns. J Clin Microbiol. 2003;41(1):73-7.
- 27. Pasqualotto AC, Bittencourt Severo C, de Mattos Oliveira F, Severo LC. Cryptococcemia. An analysis of 28 cases with emphasis on the clinical outcome and its etiologic agent. Rev Iberoam Micol. 2004;21(3):143-6.
- 28. Severo LC, de Mattos Oliveira F, Londero AT. Cryptococcosis due to Cryptococcus neoformans var. gattii in Brazilian patients with AIDS. Report of three cases. Rev Iberoam Micol. 1999;16(3):152-4.
- 29. Garau M, del Palacio A. Cryptococcus neoformans arthritis in a renal transplant recipient [Article in Spanish]. Rev Iberoam Micol. 2002;19(3):186-9.
- 30. Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-74, v-vi.
- 31. Severo LC, Berta-E-Zardo I, Londero AT. Cutaneous cryptococcosis due to Cryptococcus neoformans var. gattii. Rev Iberoam Micol. 2001;18(4):200-1.
- 32. Chen S, Sorrell T, Nimmo G, Speed B, Currie B, Ellis D, et al. Epidemiology and host- and variety-dependent characteristics of infection due to Cryptococcus neoformans in Australia and New Zealand. Australasian Cryptococcal Study Group. Clin Infect Dis. 2000;31(2):499-508.
- 33. Speed B, Dunt D. Clinical and host differences between infections with the two varieties of Cryptococcus neoformans. Clin Infect Dis. 1995;21(1):28-34; discussion 35-6.
- 34. Nadrous HF, Antonios VS, Terrell CL, Ryu JH. Pulmonary cryptococcosis in nonimmunocompromised patients. Chest. 2003;124(6):2143-7.
- 35. Lortholary O, Nunez H, Brauner MW, Dromer F. Pulmonary cryptococcosis. Semin Respir Crit Care Med. 2004;25(2):145-57.
- 36. Su CT, Chen LK, Tsai YF, Kuo CJ, Lu CL, Chen HY. Disseminated cryptococcosis with pulmonary and marrow involvement mimicking radiological features of malignancy. J Chin Med Assoc. 2004;67(2):89-92.
- 37. Oliveira Fde M, Severo CB, Guazzelli LS, Severo LC. Cryptococcus gattii fungemia: report of a case with lung and brain lesions mimicking radiological features of malignancy. Rev Inst Med Trop Sao Paulo. 2007;49(4):263-5.
- 38. Mitchell DH, Sorrell TC. Pancoast's syndrome due to pulmonary infection with Cryptococcus neoformans variety gattii. Clin Infect Dis. 1992;14(5):1142-4.
- 39. Chang WC, Tzao C, Hsu HH, Lee SC, Huang KL, Tung HJ, et al. Pulmonary cryptococcosis: comparison of clinical and radiographic characteristics in immunocompetent and immunocompromised patients. Chest. 2006;129(2):333-40.
- 40. Chandler FW, Watts JC. Cryptococcosis. In: Connor DH, Chandler FW, Schwartz DA, Manz HJ, Lack EE, editors. Pathology of infectious diseases, Stamford: Appleton & Lange, 1997. p. 989-97.
- 41. Gazzoni AF, Pegas KL, Severo LC. Histopathological techniques for diagnosing cryptococcosis due to capsule-deficient Cryptococcus: case report [Article in Portuguese]. Rev Soc Bras Med Trop. 2008;41(1):76-8.
- 42. Schwartz DA. Characterization of the biological activity of Cryptococcus infections in surgical pathology. The Budding Index and Carminophilic Index. Ann Clin Lab Sci. 1988;18(5):388-97.
- 43. Casadevall A, Perfect JR. Cryptococcus neoformans. Washington: ASM Press; 1998.
- 44. Lee SC, Dickson DW, Casadevall A. Pathology of cryptococcal meningoencephalitis: analysis of 27 patients with pathogenetic implications. Hum Pathol. 1996;27(8):839-47.
- 45. McDonnell JM, Hutchins GM. Pulmonary cryptococcosis. Hum Pathol. 1985;16(2):121-8.
- 46. Shibuya K, Hirata A, Omuta J, Sugamata M, Katori S, Saito N, et al. Granuloma and cryptococcosis. J Infect Chemother. 2005;11(3):115-22.
- 47. Chong PY, Panabokke RG, Chew KH. Omental cryptococcoma. An unusual presentation of cryptococcosis. Arch Pathol Lab Med. 1986;110(3):239-41.
- 48. Lehmann PF, Morgan RJ, Freimer EH. Infection with Cryptococcus neoformans var. gattii leading to a pulmonary cryptococcoma and meningitis. J Infect. 1984;9(3):301-6.
- 49. Alfonso F, Gallo L, Winkler B, Suhrland MJ. Fine needle aspiration cytology of peripheral lymph node cryptococcosis. A report of three cases. Acta Cytol. 1994;38(3):459-62.
- 50. Gal AA, Koss MN, Hawkins J, Evans S, Einstein H. The pathology of pulmonary cryptococcal infections in the acquired immunodeficiency syndrome. Arch Pathol Lab Med. 1986;110(6):502-7.
- 51. Travis WD, Colby TV, Koss MN, Rosado-de-Christenson ML, Muller NL, King TE. Lung Infections. In: Travis WD, Colby TV, Koss MN, Rosado-de-Christenson ML, Muller NL, King TE, editors. Non-Neoplastic disorders of the lower respiratory tract. Washington: American Registry of Pathology; 2002. p. 600-5.
- 52. Gutierrez F, Fu YS, Lurie H. Cryptococcosis histologically resembling histoplasmosis. A light and electron microscopical study. Arch Pathol. 1975;99(7):347-52.
- 53. Harding SA, Scheld WM, Feldman PS, Sande MA. Pulmonary infection with capsule-deficient cryptococcus neoformans. Virchows Arch A Pathol Anat Histol. 1979;382(1):113-8.
- 54. Farmer SG, Komorowski RA. Histologic response to capsule-deficient Cryptococcus neoformans. Arch Pathol. 1973;96(6):383-7.
- 55. Kwon-Chung KJ, Polacheck I, Bennett JE. Improved diagnostic medium for separation of Cryptococcus neoformans var. neoformans (serotypes A and D) and Cryptococcus neoformans var. gattii (serotypes B and C). J Clin Microbiol. 1982;15(3):535-7.
- 56. Kauffman CA, Bergman AG, Severance PJ, McClatchey KD. Detection of cryptococcal antigen. Comparison of two latex agglutination tests. Am J Clin Pathol. 1981;75(1):106-9.
- 57. 1999 USPHS/IDSA guidelines for the prevention of opportunistic infections in persons infected with human immunodeficiency virus. Clin Infect Dis. 2000;30 Suppl 1:S29-65.
Publication Dates
-
Publication in this collection
08 Dec 2009 -
Date of issue
Nov 2009
History
-
Accepted
05 Aug 2009 -
Received
03 Aug 2009