LETTER TO THE EDITOR
IResident, Kameda Medical Center, Kamogawa, Japan
IIChief, Kameda Medical Center, Kamogawa, Japan
IIIChief, Kameda Medical Center, Kamogawa, Japan
IVChief, Kameda Medical Center, Kamogawa, Japan
VChief, Kameda Medical Center, Kamogawa, Japan
To the Editor:
Lung cancer remains the leading cause of cancer death, and approximately 13% of all patients with lung cancer are diagnosed as having small cell lung cancer (SCLC).(1) Although SCLC is highly sensitive to first-line chemotherapy and radiation therapy, most SCLC patients experience relapse within two years and die from systemic metastasis.(2,3) Despite the fact that bone marrow is well known to be one of the organs affected by metastasis,(4) there is no established treatment for bone marrow metastasis of SCLC.
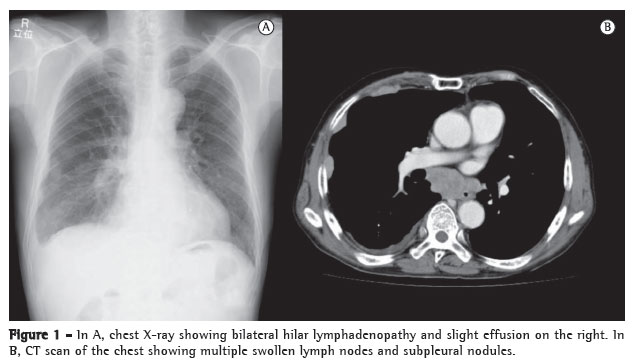
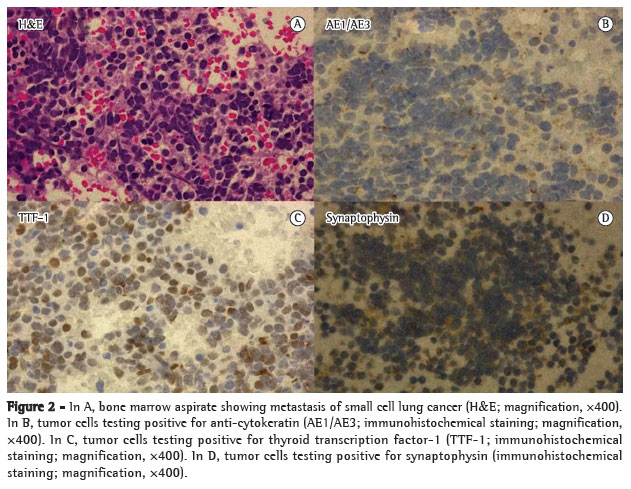
To our knowledge, this is the first case report of extensive disease SCLC (ED-SCLC) and bone marrow metastasis successfully treated with low-dose amrubicin alone. A 71-year-old male patient presenting with a one-week history of general fatigue and eventual disorientation was referred to us. Laboratory tests revealed hyponatremia (104 mEq/L) and pancytopenia (white blood cells, 1,900/µL; hemoglobin, 8.0 g/dL; and platelet count, 1.9 µg/mL). In addition, there was an abnormal shadow with multiple swollen lymph nodes on chest X-ray and CT scans (Figure 1). Bone marrow aspiration revealed bone marrow metastasis of SCLC (Figure 2). He was diagnosed with ED-SCLC (tumor-node-metastasis staging system cT4N3M1, stage IV) and bone marrow metastasis. Enhanced magnetic resonance imaging of the brain showed no evidence of brain metastasis. Treatment was started with a low dose (30 mg/m2) of amrubicin and platelet transfusion (100,000 units). His pancytopenia and disorientation improved after two courses of amrubicin. We administered escalating doses (from 30 to 35 mg/m2) of amrubicin based on the performance status of the patient. A total of six courses of amrubicin were administered (two and four cycles of 30 mg/m2 and 35 mg/m2, respectively), resulting in complete response, as determined by Response Evaluation Criteria in Solid Tumors. After a six-month follow-up period, the SCLC remained in complete remission.
Amrubicin is a fully synthetic 9-aminoanthracycline, which is converted in the body to amrubicinol by reduction of the ketone in position 13. Amrubicinol has a higher antitumor activity than does the parent molecule. Although they are classified as anthracycline agents, amrubicin and amrubicinol exert cytotoxic effects as DNA topoisomerase II inhibitors rather than as DNA intercalators.(5-7) In Japan, a phase II study showed the results of intravenous administration of single-agent amrubicin at 40 mg/m2 for three consecutive days in previously treated SCLC patients. The overall response rates were 52% and 50% in cases of sensitive SCLC and refractory/relapsed SCLC, respectively, and the mean survival times were 11.6 and 10.3 months.(5) That study demonstrated that amrubicin was superior to topotecan in terms of response rates and overall survival. However, grade 3-4 neutropenia, thrombocytopenia, anemia, and febrile neutropenia were seen in 83%, 20%, 33%, and 5% of the patients, respectively.(8) The efficacy of low-dose amrubicin therapy has recently been reported, amrubicin having been reported as a first-line chemotherapeutic agent for the elderly(9) and as a third-line chemotherapeutic agent for refractory/relapsed SCLC.(10) Despite its hematologic toxicity, amrubicin is safe and effective when dose modulation techniques are used on the basis of the condition of the patient.
The therapy for bone marrow metastasis has yet to be established. Best supportive care has been commonly prescribed in our practice. However, incremental doses of amrubicin can be used for treating the disease.
One limitation was the fact that the dose modulation of amrubicin was based on the condition of the patient as assessed by the attending physician. This protocol has yet to be established.
In conclusion, we successfully treated a patient with SCLC and bone marrow metastasis. The use of amrubicin in isolation can be useful in the treatment of ED-SCLC with bone marrow metastasis. Further investigations are necessary.
Acknowledgments
We are grateful for the diligent and thorough critical reading of our manuscript by Mr. John Wocher, Executive Vice President and Director, International Affairs/International Patient Services at Kameda Medical Center, Japan.
References
Submitted: 17 April 2012.
Accepted, after review: 06 June 2012.
- 1. Govindan R, Page N, Morgensztern D, Read W, Tierney R, Vlahiotis A, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24(28):4539-44. PMid:17008692. http://dx.doi.org/10.1200/JCO.2005.04.4859
- 2. Noda K, Nishiwaki Y, Kawahara M, Negoro S, Sugiura T, Yokoyama A, et al. Irinotecan plus cisplatin compared with etoposide plus cisplatin for extensive small-cell lung cancer. N Engl J Med. 2002;346(2):85-91. PMid:11784874. http://dx.doi.org/10.1056/NEJMoa003034
- 3. El Maalouf G, Rodier JM, Faivre S, Raymond E. Could we expect to improve survival in small cell lung cancer? Lung Cancer. 2007;57 Suppl 2:S30-4. http://dx.doi.org/10.1016/S0169-5002(07)70425-7
- 4. Govindan R, Page N, Morgensztern D, Read W, Tierney R, Vlahiotis A, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24(28):4539-44. PMid:17008692. http://dx.doi.org/10.1200/JCO.2005.04.4859
- 5. Onoda S, Masuda N, Seto T, Eguchi K, Takiguchi Y, Isobe H, et al. Phase II trial of amrubicin for treatment of refractory or relapsed small-cell lung cancer: Thoracic Oncology Research Group Study 0301. J Clin Oncol. 2006;24(34):5448-53. PMid:17135647. http://dx.doi.org/10.1200/JCO.2006.08.4145
- 6. Ohe Y, Nakagawa K, Fujiwara Y, Sasaki Y, Minato K, Bungo M, et al. In vitro evaluation of the new anticancer agents KT6149, MX-2, SM5887, menogaril, and liblomycin using cisplatin- or adriamycin-resistant human cancer cell lines. Cancer Res. 1989;49(15):4098-102. PMid:2472873.
- 7. Obara N, Imagawa S, Nakano Y, Yamamoto M, Noguchi T, Nagasawa T. Hematological aspects of a novel 9-aminoanthracycline, amrubicin. Cancer Sci. 2003;94(12):1104-6. PMid:14662027. http://dx.doi.org/10.1111/j.1349-7006.2003.tb01407.x
- 8. von Pawel J, Ardizzoni A, Thatcher N, Crofts T, Wissel P, Dane G, et al. The relationship between treatment-free interval (TFI) and outcomes to therapy in patients with relapsed small cell lung cancer (SCLC): a review of 631 patients treated with iv topotecan in 6 studies. Lung Cancer. 2003;41:S235. http://dx.doi.org/10.1016/S0169-5002(03)92536-0
- 9. Igawa S, Yamamoto N, Ueda S, Ono A, Nakamura Y, Tsuya A, et al. Evaluation of the recommended dose and efficacy of amrubicin as second- and third-line chemotherapy for small cell lung cancer. J Thorac Oncol. 2007;2(8):741-4. PMid:17762341. http://dx.doi.org/10.1097/JTO.0b013e31811f46f0
- 10. Asai N, Ohkuni Y, Matsunuma R, Nakashima K, Iwasaki T, Kaneko N. Efficacy and safety of amrubicin for the elderly patients with refractory relapsed small cell lung cancer as third-line chemotherapy. J Cancer Res Ther. 2012;8(2):266-71. PMid:22842373. http://dx.doi.org/10.4103/0973-1482.98983
Incremental low doses of amrubicin for the treatment of bone marrow metastasis in small cell lung cancer
Publication Dates
-
Publication in this collection
11 Mar 2013 -
Date of issue
Feb 2013