ABSTRACT
Acute pulmonary thromboembolism (APTE) is a highly prevalent condition (104-183 cases per 100,000 person-years) and is potentially fatal. Approximately 20% of patients with APTE are hypotensive, being considered at high risk of death. In such patients, immediate lung reperfusion is necessary in order to reduce right ventricular afterload and to restore hemodynamic stability. To reduce pulmonary vascular resistance in APTE and, consequently, to improve right ventricular function, lung reperfusion strategies have been developed over time and widely studied in recent years. In this review, we focus on advances in the indication and use of systemic thrombolytic agents, as well as lung reperfusion via endovascular and classical surgical approaches, in APTE.
Keywords:
Embolism; Shock; Hypotension; Thrombolytic therapy; Reperfusion; Hemorrhage
RESUMO
O tromboembolismo pulmonar (TEP) agudo é uma condição altamente prevalente (104-183 por 100.000 pessoas-ano) e potencialmente fatal. Aproximadamente 20% dos pacientes com TEP agudo apresentam-se hipotensos, sendo considerados pacientes com alto risco de morte. Nesses casos, a necessidade de reperfusão pulmonar imediata é mandatória para reduzir a pós-carga do ventrículo direito e restaurar a condição hemodinâmica do paciente. Visando a redução da resistência vascular pulmonar no TEP agudo e, por consequência, a melhora na função ventricular direita, estratégias de reperfusão pulmonar foram desenvolvidas com passar do tempo e vêm sendo muito estudadas nos últimos anos. Avanços na indicação e no uso de trombolíticos sistêmicos, reperfusão pulmonar via abordagem endovascular ou abordagem cirúrgica clássica no TEP agudo são os focos desta revisão.
Descritores:
Embolia; Choque; Hipotensão; Terapia trombolítica; Reperfusão; Hemorragia
INTRODUCTION
Acute pulmonary thromboembolism (APTE), the most severe form of venous thromboembolism (VTE), is a highly prevalent condition-104-183 cases per 100,000 person-years, similar to the prevalence of stroke11 Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol. 2015;12(8):464-74. https://doi.org/10.1038/nrcardio.2015.83
https://doi.org/10.1038/nrcardio.2015.83...
-and is potentially fatal,22 Heit JA. The epidemiology of venous thromboembolism in the community. Arterioscler Thromb Vasc Biol. 2008;28(3):370-2. https://doi.org/10.1161/ATVBAHA.108.162545
https://doi.org/10.1161/ATVBAHA.108.1625...
currently being the third leading cause of cardiovascular death in the world, behind only acute myocardial infarction and stroke.33 Cohen AT, Agnelli G, Anderson FA, Arcelus JI, Bergqvist D, Brecht JG, et al. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007;98(4):756-64. It is believed that, worldwide, more than three million people die annually from PTE.44 ISTH Steering Committee for World Thrombosis Day. Thrombosis: a major contributor to the global disease burden. J Thromb Haemost. 2014;12(10):1580-90. https://doi.org/10.1111/jth.12698
https://doi.org/10.1111/jth.12698...
A study conducted in Brazil identified approximately 100,000 deaths from PTE between 1989 and 2010, and, despite being impressive, that number is probably underestimated.55 Darze ES, Casqueiro JB, Ciuffo LA, Santos JM, Magalhães IR, Latado AL. Pulmonary Embolism Mortality in Brazil from 1989 to 2010: Gender and Regional Disparities. Arq Bras Cardiol. 2016;106(1):4-12. https://doi.org/10.5935/abc.20160001
https://doi.org/10.5935/abc.20160001...
There are signs of pulmonary embolism in 18% of autopsies, and pulmonary embolism was the main or contributing cause of death in 70% of those cases.66 Oger E. Incidence of venous thromboembolism: a community-based study in Western France. EPI-GETBP Study Group. Groupe d'Etude de la Thrombose de Bretagne Occidentale. Thromb Haemost. 2000;83(5):657-60. https://doi.org/10.1055/s-0037-1613887
https://doi.org/10.1055/s-0037-1613887...
Although epidemiological data highlight the potential severity of PTE, a considerable proportion of patients with the disease are known to show a good evolution, becoming oligosymptomatic or even asymptomatic.77 Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002;121(3):877-905. https://doi.org/10.1378/chest.121.3.877
https://doi.org/10.1378/chest.121.3.877...
Scientists have long tried to understand the mechanism behind this constellation of such distinct presentations of the same disease: some patients evolve as asymptomatic; whereas others suffer hemodynamic instability, cardiogenic shock, and eventual death. The response of the right ventricle (RV) to PTE and to the acute increase in pulmonary vascular resistance (PVR) is currently believed to be the main determinant of patient evolution.
PHYSIOPATHOLOGY OF HEMODYNAMIC INSTABILITY IN APTE
The RV has certain anatomical and functional characteristics that determine its peculiar response to acute oscillations in the RV afterload. The RV has low muscle mass in comparison with the left ventricle (LV), and perfusion of the RV occurs during systole and diastole.88 Hoette S, Jardim C, Souza Rd. Diagnosis and treatment of pulmonary hypertension: an update. J Bras Pneumol. 2010;36(6):795-811. https://doi.org/10.1590/S1806-37132010000600018
https://doi.org/10.1590/S1806-3713201000...
In APTE, there is a sudden increase in PVR, representing the ventricular afterload, by obstruction of the arterial lumen and by vasoconstriction, mediated by endothelial dysfunction induced by the presence of a clot.99 Torbicki A. Acute and long term management of pulmonary embolism. Heart. 2010;96(17):1418-24. https://doi.org/10.1136/hrt.2008.153957
https://doi.org/10.1136/hrt.2008.153957...
The increase in arterial pulmonary pressure due to the increase in PVR is transmitted to the RV wall, leading to its dilation and consequent loss of its best position for distention, decreasing its contractile efficiency (the Frank-Starling mechanism).1010 Sequeira V, van der Velden J. Historical perspective on heart function: the Frank-Starling Law. Biophys Rev. 2015;7(4):421-447. https://doi.org/10.1007/s12551-015-0184-4
https://doi.org/10.1007/s12551-015-0184-...
The interventricular septum may also be affected by the acute increase in the afterload and in the pressure of the right chambers, altering its natural conformation and bulging into the interior of the LV, hindering the filling and contraction of the latter. Simultaneously, the increased tension in the RV wall increases the local demand for oxygen, causing relative ischemia of the RV and reducing its contractility. The interaction of these three factors results in reduced right cardiac output, with consequently reduced LV preload and, therefore, reduced LV cardiac output. This reduced cardiac output causes systemic hypotension and, subsequently, cardiogenic shock, and eventually death.1111 Konstantinides S, Torbicki A. Management of venous thrombo-embolism: an update. Eur Heart J. 2014;35(41):2855-63. https://doi.org/10.1093/eurheartj/ehu243
https://doi.org/10.1093/eurheartj/ehu243...
Therefore, the best strategy to predict the outcome of a patient with APTE is the evaluation of RV function, when that specific thromboembolic stimulus is present.1212 Kasper W, Konstantinides S, Geibel A, Tiede N, Krause T, Just H. Prognostic significance of right ventricular afterload stress detected by echocardiography in patients with clinically suspected pulmonary embolism. Heart. 1997;77(4):346-9. https://doi.org/10.1136/hrt.77.4.346
https://doi.org/10.1136/hrt.77.4.346...
The most recent consensus of the European Society of Cardiology, developed in conjunction with the European Respiratory Society, recognizes the central role of the RV and considers the evaluation of the RV to be the main focus of the risk stratification of patients with APTE.1313 Konstantinides SV. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(45):3145-6. The risk stratification model proposed jointly by the two societies can be seen in Table 1.
Once APTE has been diagnosed, the next step is to evaluate the clinical repercussions of the event. Significant clinical repercussions, identified by the application of a clinical score, such as the simplified Pulmonary Embolism Severity Index,1414 Jiménez D, Aujesky D, Moores L, Gómez V, Lobo JL, Uresandi F, et al. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med. 2010;170(15):1383-9. https://doi.org/10.1001/archinternmed.2010.199
https://doi.org/10.1001/archinternmed.20...
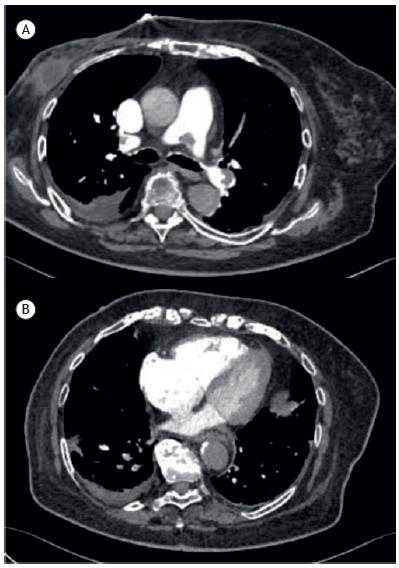
are not seen in low-risk patients. Patients that are not considered low risk by the simplified Pulmonary Embolism Severity Index should be further stratified. Intermediate-low-risk patients, despite some clinical repercussions, do not show signs of significant RV dysfunction, as evidenced by the absence of biochemical and radiological signs. Intermediate-high-risk patients show acute RV dysfunction, due to the increase in afterload, but can still maintain cardiac output and, consequently, arterial pressure, although that can result in myocardial injury (identified by the serum presence of markers of injury in association with signs of ventricular dysfunction visible by imaging tests, whether echocardiography or tomography), as depicted in Figure 1. Lastly, high-risk patients are hypotensive and, therefore, show pronounced RV failure.
Contrast-enhanced computed tomography scan in a patient with intermediate-high-risk pulmonary thromboembolism. Note the presence of clot in the branch of the pulmonary artery (in A); and the dilation of the right ventricle and atrium, the narrowing of the interventricular septum, and the resulting compression of the left ventricle (in B).
The frequency of APTE, by severity, was evaluated in the International Cooperative Pulmonary Registry study.1515 Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353(9162):1386-9. https://doi.org/10.1016/S0140-6736(98)07534-5
https://doi.org/10.1016/S0140-6736(98)07...
In that study, 20% of the APTEs were classified as high risk, 48% were classified as low risk, and 32% were classified as intermediate risk. Therefore, although most patients do not show a severe form of the disease, a considerable proportion show some degree of RV dysfunction and are therefore at an increased risk of death. To reduce PVR in APTE and, consequently, to improve RV function, lung reperfusion strategies have been developed over time and widely studied in recent years. In this review, we focus on advances in the indication and use of systemic thrombolytic agents, as well as lung reperfusion via endovascular and classical surgical approaches, in APTE.
SYSTEMIC THROMBOLYTIC AGENTS
Since the 1960s, the use of intravenous or even oral anticoagulants has been effective in reducing the recurrence of VTE, as well as reducing mortality rates.1616 Fernandes CJ, Alves Júnior JL, Gavilanes F, Prada LF, Morinaga LK, Souza R. New anticoagulants for the treatment of venous thromboembolism. J Bras Pneumol. 2016;42(2):146-54. https://doi.org/10.1590/S1806-37562016042020068
https://doi.org/10.1590/S1806-3756201604...
However, for a certain patient population this treatment was insufficient and mortality remained high. Systemic thrombolytic agents, already widely used for coronary reperfusion in acute myocardial infarction, were subsequently evaluated also for APTE. In 1971, Miller et al. demonstrated that the use of streptokinase, 72 h after the acute event, reduced the pulmonary artery systolic pressure, the total pulmonary resistance, and the values of the angiographic severity index in PTE, in comparison with the use of heparin.1717 Miller GA, Sutton GC, Kerr IH, Gibson RV, Honey M. Comparison of streptokinase and heparin in treatment of isolated acute massive pulmonary embolism. Br Heart J. 1971;33(4):616. https://doi.org/10.1136/bmj.2.5763.681
https://doi.org/10.1136/bmj.2.5763.681...
That information sparked enthusiasm for the use of thrombolytic agents in PTE. However, experience demonstrated two inconveniences in the use of thrombolytic agents. The first was that the comparison between thrombolytic agents and heparin as treatments for APTE showed them to be identical in terms of the rates of pulmonary reperfusion, evaluated by quantitative lung scintigraphy in the medium term (two weeks) and long term (one year).1818 Bell WR, Simon TL, Stengle JM, Sherry S. The urokinase-streptokinase pulmonary embolism trial (phase II) results. Circulation. 1974;50(6):1070-1. https://doi.org/10.1161/01.CIR.50.6.1070
https://doi.org/10.1161/01.CIR.50.6.1070...
In other words, despite acutely promoting a higher reperfusion rate and, therefore, acutely reducing PVR, the use of thrombolytic agents did not have a long-term effect on pulmonary reperfusion. The second inconvenience, which could affect the use of the new therapy, was the fact that the use of thrombolytic agents for PTE promoted significantly higher rates of bleeding than did that of conventional anticoagulants. Some studies reported rates of up to 22%1515 Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353(9162):1386-9. https://doi.org/10.1016/S0140-6736(98)07534-5
https://doi.org/10.1016/S0140-6736(98)07...
of clinically relevant bleeding with the use of thrombolytic agents. The rates of intracranial hemorrhage, 2-3%,1515 Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353(9162):1386-9. https://doi.org/10.1016/S0140-6736(98)07534-5
https://doi.org/10.1016/S0140-6736(98)07...
,1919 Dalen JE, Alpert JS, Hirsh J. Thrombolytic therapy for pulmonary embolism: is it effective? Is it safe? When is it indicated? Arch Intern Med. 1997;157(22):2550-6. https://doi.org/10.1001/archinte.1997.00440430026003
https://doi.org/10.1001/archinte.1997.00...
were particularly concerning, and the mortality in this population was up to 75%.
Two meta-analyses2020 Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110(6):744-9. https://doi.org/10.1161/01.CIR.0000137826.09715.9C
https://doi.org/10.1161/01.CIR.000013782...
,2121 Stein PD, Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465-70. https://doi.org/10.1016/j.amjmed.2011.10.015
https://doi.org/10.1016/j.amjmed.2011.10...
demonstrated the role of systemic thrombolysis in high-risk APTE (hemodynamically unstable) patients. The first meta-analysis, published in 2004, evaluated a subgroup of 154 patients with PTE and hypotension, from several smaller studies, and showed that thrombolysis had a favorable impact on a compound outcome of death and recurrence of VTE, in comparison with heparin (9.4 vs. 19%; OR = 0.45; 95% CI: 0.22-0.92).2020 Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110(6):744-9. https://doi.org/10.1161/01.CIR.0000137826.09715.9C
https://doi.org/10.1161/01.CIR.000013782...
The second meta-analysis, published in 2012, evaluated a collective total of two million patients hospitalized with PTE.2121 Stein PD, Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465-70. https://doi.org/10.1016/j.amjmed.2011.10.015
https://doi.org/10.1016/j.amjmed.2011.10...
In that study, 21,390 hemodynamically unstable patients received thrombolytic agents, and the mortality rate among those patients was 8.4%, compared with 42.0% among the 50,840 hemodynamically unstable patients who did not receive thrombolytic agents, for a variety of reasons. Therefore, the use of systemic thrombolytic agents in the presence of hemodynamic instability reduced the relative risk of death by 80% (95% CI: 0.19-0.22)2121 Stein PD, Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465-70. https://doi.org/10.1016/j.amjmed.2011.10.015
https://doi.org/10.1016/j.amjmed.2011.10...
. Therefore, the use of systemic thrombolytic agents is considered an important alternative for reperfusion in patients with PTE and hemodynamic instability.2222 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-352. https://doi.org/10.1016/j.chest.2015.11.026
https://doi.org/10.1016/j.chest.2015.11....
The benefit in terms of mortality is maintained even when thrombolytic therapy is implemented 14 days after the acute event. However, the maximum benefit occurs when therapy is implemented in the first 48 h after the initial clinical presentation.2323 Goldhaber SZ. Thrombolytic therapy. Adv Intern Med. 1999;44:311-25. The recommended agents and doses are described in Table 2.
Absolute contraindications to the use of thrombolytic agents are recent major surgery (less than 10 days), intracranial neoplasm, active bleeding, major trauma (less than two weeks), stroke in the last three months, any history of hemorrhagic stroke, and significant coagulopathy. These contraindications should be properly evaluated because there is a risk of fatal bleeding in these circumstances. However, studies demonstrate that up to two thirds of patients with PTE and hypotension do not receive fibrinolytic therapy.2424 Moorjani N, Price S. Massive pulmonary embolism. Cardiol Clin. 2013;31(4):503-18, vii. https://doi.org/10.1016/j.ccl.2013.07.005
https://doi.org/10.1016/j.ccl.2013.07.00...
Considering that the absolute contraindications cannot be present in all of those patients, it is clear that physicians fear bleeding. But such fear cannot justify not administering the best therapy available for patients with high-risk PTE. To better manage this condition and other conditions in patients with APTE, some institutions recently opted for the model of multidisciplinary care teams, known as rapid response teams (pulmonary embolism response teams).2525 Kabrhel C, Rosovsky R, Channick R, Jaff MR, Weinberg I, Sundt T, et al. A Multidisciplinary Pulmonary Embolism Response Team: Initial 30-Month Experience With a Novel Approach to Delivery of Care to Patients With Submassive and Massive Pulmonary Embolism. Chest. 2016;150(2):384-93. https://doi.org/10.1016/j.chest.2016.03.011
https://doi.org/10.1016/j.chest.2016.03....
Therefore, responsibility is shared among team members (pulmonologists, cardiologists, radiologists, intensivists, and surgeons) and the patient, all of whom must act in an assertive and timely manner, 24 h/day, in order to promote an individualized approach based on the best evidence in the field of pulmonary embolism research. This initiative began at Massachusetts General Hospital, in Boston, Massachusetts, and now extends to multiple centers in the United States and worldwide, with encouraging results.
SYSTEMIC THROMBOLYSIS IN INTERMEDIATE-HIGH-RISK PATIENTS
Even with the risk of bleeding previously described, in the case of APTE, given the imminent risk of death of a patient with pronounced RV insufficiency, the use of systemic fibrinolytic agents is indicated for patients with pulmonary embolism and hypotension.2222 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-352. https://doi.org/10.1016/j.chest.2015.11.026
https://doi.org/10.1016/j.chest.2015.11....
However, in intermediate-high-risk cases, this indication is controversial. The pathophysiological mechanism previously described incites the tempting possibility of preventing circulatory collapse by reducing the RV afterload before the progression to pronounced ventricular insufficiency, thus improving the outlook for the patient. However, would this theoretical benefic supersede the risks of hemorrhage, which are already known for the use of fibrinolytic agents in other situations?
Dalla-Volta et al.2626 Dalla-Volta S, Palla A, Santolicandro A, Giuntini C, Pengo V, Visioli O, et al. PAIMS 2: alteplase combined with heparin versus heparin in the treatment of acute pulmonary embolism. Plasminogen activator Italian multicenter study 2. J Am Coll Cardiol. 1992;20(3):520-6. https://doi.org/10.1016/0735-1097(92)90002-5
https://doi.org/10.1016/0735-1097(92)900...
evaluated this question systematically in 1992. Thirty six patients with APTE and RV dysfunction, without shock, were randomized to receive alteplase or heparin. The study did not identify differences in terms of mortality or severe bleeding; however, there was a reduction in the pulmonary artery pressure and in the angiographic score. Could thrombolysis then have another effect, such as preventing the evolution of APTE to chronic thromboembolic pulmonary hypertension (CTEPH), a known complication of APTE, with its own high morbidity and mortality? In 2002, that possibility was suggested by Konstantinides et al. in a study evaluating 256 patients with APTE and RV dysfunction, without hypotension, receiving alteplase plus heparin or heparin only.2727 Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W; Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002;347(15):1143-50. https://doi.org/10.1056/NEJMoa021274
https://doi.org/10.1056/NEJMoa021274...
Although there was no difference between the two groups in terms of mortality, the rate of intracranial hemorrhage in that study was zero for both groups. In addition, at the end of the study, the pulmonary artery pressure, measured by echocardiography, was higher in the group that received heparin only. Could thrombolysis have reduced the risk of this population evolving to CTEPH?
The Pulmonary Embolism Thrombolysis trial2828 Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-11. https://doi.org/10.1056/NEJMoa1302097
https://doi.org/10.1056/NEJMoa1302097...
provided concrete answers to some of the questions that had arisen in the field of pulmonary embolism research. That multicenter study, conducted in 2014, evaluated 1,006 patients with APTE and RV dysfunction, without shock, and demonstrated that thrombolysis in that clinical situation (with the use of tenecteplase) had a positive effect on the combined outcome of mortality and hemodynamic instability/use of vasoactive drugs-2.6% of events in the thrombolysis group vs. 5.6% in the full anticoagulation only (control) group-with no isolated benefit in terms of mortality. However, that positive result occurred at a price2828 Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-11. https://doi.org/10.1056/NEJMoa1302097
https://doi.org/10.1056/NEJMoa1302097...
: the rate of intracranial bleeding was ten times higher in the thrombolysis group than in the full anticoagulation only group (2.0% vs. 0.2%). Another relevant aspect of the study was the extremely low mortality in the anticoagulation group (1.8%), only 3.4% of this group requiring rescue thrombolysis. Those results decreased the enthusiasm for thrombolysis in APTE without hemodynamic instability, although the question regarding the medium- and long-term effects of the use of fibrinolytic agents remained. Some limitations of that study should be noted.2828 Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-11. https://doi.org/10.1056/NEJMoa1302097
https://doi.org/10.1056/NEJMoa1302097...
The population included had a relatively high median age (70 years), therefore being more prone to bleeding, which increases the risks associated with the use of thrombolysis. Would an intervention for a younger population with less hemorrhagic risk be worth considering?
The long-term findings of the Pulmonary Embolism Thrombolysis trial were recently published,2828 Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-11. https://doi.org/10.1056/NEJMoa1302097
https://doi.org/10.1056/NEJMoa1302097...
and the use of thrombolysis was found to have no effect on two-year mortality (20.3 vs. 18%; p = 0.43) or on residual dyspnea (36.0 vs. 30.1%; p = 0.23). In the population screened for CTEPH (30% of cases), there was no difference in the identification of this diagnosis (2.1 vs. 3.2%; p = 0.79),2929 Konstantinides SV, Vicaut E, Danays T, Becattini C, Bertoletti L, Beyer-Westendorf J, et al. Impact of Thrombolytic Therapy on the Long-Term Outcome of Intermediate-Risk Pulmonary Embolism. J Am Coll Cardiol. 2017;69(12):1536-1544. https://doi.org/10.1016/j.jacc.2016.12.039
https://doi.org/10.1016/j.jacc.2016.12.0...
the incidences being comparable to those previously reported.3030 Hoeper MM, Humbert M, Souza R, Idrees M, Kawut SM, Sliwa-Hahnle K, et al. A global view of pulmonary hypertension. Lancet Respir Med. 2016;4(4):306-22. https://doi.org/10.1016/S2213-2600(15)00543-3
https://doi.org/10.1016/S2213-2600(15)00...
With modest short-term benefits, no long-term benefits, and a considerable risk of hemorrhage, the use of full-dose thrombolytic therapy in APTE is increasingly restricted to high-risk patients with hemodynamic instability. The current recommendation is close monitoring (preferably in the ICU) and, in case of instability, early implementation of thrombolysis.1313 Konstantinides SV. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(45):3145-6.,2222 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-352. https://doi.org/10.1016/j.chest.2015.11.026
https://doi.org/10.1016/j.chest.2015.11....
Alternative approaches to systemic thrombolysis in intermediate-high risk PTE, to minimize the risk of bleeding, have already been evaluated. In 2013, the Moderate Pulmonary Embolism Treated with Thrombolysis study3131 Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; "MOPETT" Investigators. Moderate pulmonary embolism treated with thrombolysis (from the "MOPETT" Trial). Am J Cardiol. 2013;111(2):273-7. https://doi.org/10.1016/j.amjcard.2012.09.027
https://doi.org/10.1016/j.amjcard.2012.0...
evaluated 121 patients randomized to receive alteplase (50 mg, corresponding to 50% of the usual dose) plus heparin, in comparison with patients receiving anticoagulation only. The reduced dose of the thrombolytic agent was found to be safe (no episodes of severe bleeding) and to reduce pulmonary artery pressure, not only acutely but also at six months after the initial event. However, that approach (using a reduced dose of a thrombolytic agent), albeit promising, cannot be routinely recommended until larger studies, with more robust outcomes, have been conducted.
ENDOVASCULAR APPROACH
Some patients with APTE and hemodynamic instability have an absolute contraindication to the administration of systemic fibrinolytic agents; for example, patients in the immediate postoperative period. In those situations, the endovascular approach to APTE is an alternative.3232 Kuo WT. Endovascular therapy for acute pulmonary embolism. J Vasc Interv Radiol. 2012;23(2):167-79 e4; quiz 179. The objective of this approach is to promote mechanical removal of the clot, reducing the RV afterload. In general, the vascular access for this procedure is via the femoral vein.
Important studies in the field of APTE have been carried out in recent years. One study evaluated 59 patients with intermediate-high-risk APTE randomized for conventional heparinization or ultrasound-assisted catheter-directed thrombolysis.3333 Kucher N, Boekstegers P, Müller OJ, Kupatt C, Beyer-Westendorf J, Heitzer T, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014;129(4):479-86. https://doi.org/10.1161/CIRCULATIONAHA.113.005544
https://doi.org/10.1161/CIRCULATIONAHA.1...
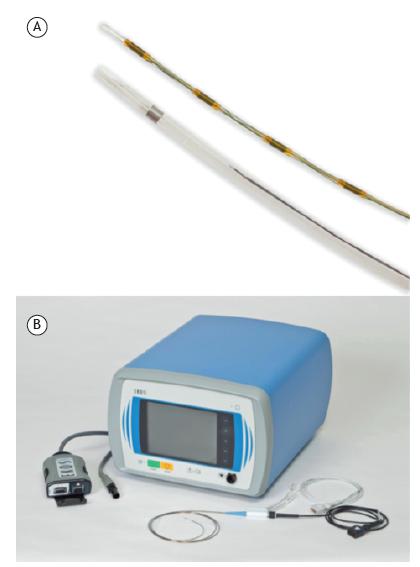
The catheter fragments the thrombus by ultrasound vibration (Figure 2), exposing more clot surface, thus enabling better action of the fibrinolytic agent at a lower dose (in that study, 10-20 mg of alteplase, over 15 h). With the endovascular approach, there was an improvement in the relationship between the areas of the RV and LV, indicating acute hemodynamic improvement. However, when patients were evaluated at the end of the study (90 days), there was no difference in terms of mortality. There was no significant bleeding with any of the approaches.
Catheter (in A) and Ekosonic Endovascular System (EKOS®; BTG Interventional Medicine, Bothell, WA, USA) device (in B) for endovascular reperfusion in acute pulmonary thromboembolism. The internal part of the catheter emits an ultrasonic pulse, vibrating and making the fibrin of the clot more porous, allowing the thrombus to be permeated by the fibrinolytic agent administered concomitantly at a low dose (images provided by the manufacturer).
Ultrasound-assisted catheter-directed thrombolysis was evaluated in another study,3434 Piazza G, Hohlfelder B, Jaff MR, Ouriel K, Engelhardt TC, Sterling KM, et al. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv. 2015;8(10):1382-92. https://doi.org/10.1016/j.jcin.2015.04.020
https://doi.org/10.1016/j.jcin.2015.04.0...
involving 150 patients with high-risk APTE (n = 31) or intermediate-high-risk APTE (n = 119). The fibrinolytic agent used was alteplase, which was administered at a dose of 24 mg, 1 mg/h, for 24 h with the use of unilateral catheters or for 12 h with the use of bilateral catheters. There was no control group in that study. The endovascular approach was effective in reducing the pulmonary artery pressure (51.4 mmHg vs. 36.9 mmHg; p < 0.0001) and improving the relationship between the areas of the RV and LV (1.55 vs. 1.13; p < 0.0001), 48 h after the acute event. In 10% of the patients, there was some type of moderate bleeding, although there was no intracranial bleeding.
A case series evaluating the combination of pharmacomechanical thrombolysis with a low-dose local fibrinolytic agent, published in 2015,3535 Kuo WT, Banerjee A, Kim PS, DeMarco FJ Jr, Levy JR, Facchini FR, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015;148(3):667-673. https://doi.org/10.1378/chest.15-0119
https://doi.org/10.1378/chest.15-0119...
involved 101 patients with intermediate-high-risk APTE (n = 73) or high-risk APTE (n = 28). Reperfusion was considered successful in 85.7% of the high-risk APTE cases and in 97.3% of the intermediate-high-risk APTE cases. The mean pulmonary artery pressure decreased from 51.17 ± 14.06 to 37.23 ± 15.81 mmHg (p < 0.0001).3535 Kuo WT, Banerjee A, Kim PS, DeMarco FJ Jr, Levy JR, Facchini FR, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015;148(3):667-673. https://doi.org/10.1378/chest.15-0119
https://doi.org/10.1378/chest.15-0119...
None of the patients evolved to major bleeding or intracranial bleeding.
Although evidence suggests some hemodynamic benefit of the vascular approach, current evidence does not justify its large-scale use in APTE. This approach should still be considered only for selected cases, at centers with expertise in this type of intervention. However, centers continue to gain experience, data of procedure records, such as those from the abovementioned study,3535 Kuo WT, Banerjee A, Kim PS, DeMarco FJ Jr, Levy JR, Facchini FR, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015;148(3):667-673. https://doi.org/10.1378/chest.15-0119
https://doi.org/10.1378/chest.15-0119...
are increasingly more available, and ongoing randomized trials should endorse the dissemination of this type of procedure in the near future.
SURGICAL EMBOLECTOMY
The surgical alternative, with the mechanical removal of the clot, reduction of the PVR, and recovery of the RV function, is another possible approach to high-risk APTE. In general, surgery is recommended when systemic thrombolysis is contraindicated and the center does not have the necessary infrastructure to apply the endovascular approach. Embolectomy is a major surgery, performed by median sternotomy, with extracorporeal circulation and deep hypothermia.3636 Lazar HL, Farber HW. Early pulmonary embolectomy for acute pulmonary embolus: an operation whose time has come. J Card Surg. 2010;25(3):259-60. https://doi.org/10.1111/j.1540-8191.2010.01012.x
https://doi.org/10.1111/j.1540-8191.2010...
The surgery produces the best results when the thrombus causing the hemodynamic instability has a central location and can therefore be removed more effectively. Consequently, the use of transesophageal echocardiography is recommended in order to locate the appropriate thrombus.3737 Le RD, Dewan NA. Pulmonary embolectomy: should it be offered earlier rather than later? Respir Care. 2009;54(3):390-2. The initial results of surgical embolectomy in APTE were very unsatisfactory, with high mortality rates, which in a certain way stigmatized the surgery. However, with the improvement of the surgical technique, of the knowledge of extracorporeal circulation, and of intensive care practices, together with the increase in experience at referral centers, significantly better results have been obtained.
In 2013, Aymard et al.3838 Aymard T, Kadner A, Widmer A, Basciani R, Tevaearai H, Weber A, et al. Massive pulmonary embolism: surgical embolectomy versus thrombolytic therapy--should surgical indications be revisited? Eur J Cardiothorac Surg. 2013;43(1):90-4; discussion 94. https://doi.org/10.1093/ejcts/ezs123
https://doi.org/10.1093/ejcts/ezs123...
retrospectively evaluated 80 consecutive patients with high-risk APTE who were subjected to reperfusion via embolectomy (35%) or systemic fibrinolytic agent administration (65%) at a single center in Bern, Switzerland.3838 Aymard T, Kadner A, Widmer A, Basciani R, Tevaearai H, Weber A, et al. Massive pulmonary embolism: surgical embolectomy versus thrombolytic therapy--should surgical indications be revisited? Eur J Cardiothorac Surg. 2013;43(1):90-4; discussion 94. https://doi.org/10.1093/ejcts/ezs123
https://doi.org/10.1093/ejcts/ezs123...
Of the patients who received the fibrinolytic agent, 21% required rescue embolectomy, because of persistent shock. Early mortality did not differ significantly between the embolectomy and thrombolysis groups (3.6% vs. 13.5%; p = 0.25). Early mortality was significantly higher in the thrombolysis group patients who underwent rescue embolectomy (26.5%, p = 0.02). The rates of severe bleeding after treatment were significantly higher in the thrombolysis group than in the embolectomy group (26.5% vs. 3.6%, p = 0.013). In the long-term follow-up (63 ± 21 months), the mortality rate was similar in both groups (17.9% in the embolectomy group vs. 23.1% in the thrombolysis group, p = 0.6).
Another relevant study in this field, published in 2017, was conducted by Lehnert et al.3939 Lehnert P, Moller CH, Mortensen J, Kjaergaard J, Olsen PS, Carlsen J. Surgical embolectomy compared to thrombolysis in acute pulmonary embolism: morbidity and mortality. Eur J Cardiothorac Surg. 2017;51(2):354-361. In a prospective cohort study, the authors evaluated 136 patients with APTE (64 with high-risk APTE and 72 with intermediate-high-risk APTE), treated with surgical embolectomy or systemic thrombolysis at a single center in Copenhagen, Denmark. In the high-risk group, there was no statistical difference between those treated with embolectomy and those treated with thrombolysis in terms of 30-day mortality (14% vs. 31%; p = 0.16) or five-year mortality (32% vs. 49%; p = 0.53). Similar results were found in the intermediate-high-risk group, with no difference between the two treatments. Secondary vascular outcomes, such as the extent of perfusion defect in lung scintigraphy and the reduction in diffusion, were evaluated, suggesting a smaller quantity of residual thrombus in the embolectomy group.
The studies cited above have shown reasonable results, given the severity of patients with PTE and hemodynamic instability, with an early mortality rate of 3.6%, underscoring the role of embolectomy in the treatment of this condition, especially at centers with experience in this type of surgery. We emphasize that the worst result occurred in the patients who underwent surgery because of refractory shock after administration of the thrombolytic agent. Therefore, if embolectomy can be performed, perhaps it should be an early option, rather than a rescue measure.
FINAL CONSIDERATIONS
APTE is a highly prevalent condition and is potentially fatal. Approximately 20% of patients with APTE are hypotensive, being considered at high risk of death. In such patients, immediate lung reperfusion is necessary in order to reduce RV afterload and to restore hemodynamic stability. Reperfusion can be performed in various ways (Figure 3): via the use of systemic thrombolytic agents (the most widely used method); with endovascular treatment (a method that is increasingly more widely used); or with surgical embolectomy (the most complex strategy; Figure 3). For the population of patients with intermediate-high-risk APTE (who maintain arterial pressure but show signs of RV injury, as well as radiological and biochemical signs), the benefit of reperfusion with thrombolytic agents is limited in the short term, whereas it is nonexistent in the long term, and there is a significant rate of intracranial bleeding. In order to define the best individualized approach and to improve the evaluation of the risk/benefit ratio of reperfusion therapies versus the risks of bleeding, some institutions have opted for the model of multidisciplinary, rapid-response teams, with encouraging results.
REFERENCES
-
1Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol. 2015;12(8):464-74. https://doi.org/10.1038/nrcardio.2015.83
» https://doi.org/10.1038/nrcardio.2015.83 -
2Heit JA. The epidemiology of venous thromboembolism in the community. Arterioscler Thromb Vasc Biol. 2008;28(3):370-2. https://doi.org/10.1161/ATVBAHA.108.162545
» https://doi.org/10.1161/ATVBAHA.108.162545 -
3Cohen AT, Agnelli G, Anderson FA, Arcelus JI, Bergqvist D, Brecht JG, et al. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007;98(4):756-64.
-
4ISTH Steering Committee for World Thrombosis Day. Thrombosis: a major contributor to the global disease burden. J Thromb Haemost. 2014;12(10):1580-90. https://doi.org/10.1111/jth.12698
» https://doi.org/10.1111/jth.12698 -
5Darze ES, Casqueiro JB, Ciuffo LA, Santos JM, Magalhães IR, Latado AL. Pulmonary Embolism Mortality in Brazil from 1989 to 2010: Gender and Regional Disparities. Arq Bras Cardiol. 2016;106(1):4-12. https://doi.org/10.5935/abc.20160001
» https://doi.org/10.5935/abc.20160001 -
6Oger E. Incidence of venous thromboembolism: a community-based study in Western France. EPI-GETBP Study Group. Groupe d'Etude de la Thrombose de Bretagne Occidentale. Thromb Haemost. 2000;83(5):657-60. https://doi.org/10.1055/s-0037-1613887
» https://doi.org/10.1055/s-0037-1613887 -
7Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002;121(3):877-905. https://doi.org/10.1378/chest.121.3.877
» https://doi.org/10.1378/chest.121.3.877 -
8Hoette S, Jardim C, Souza Rd. Diagnosis and treatment of pulmonary hypertension: an update. J Bras Pneumol. 2010;36(6):795-811. https://doi.org/10.1590/S1806-37132010000600018
» https://doi.org/10.1590/S1806-37132010000600018 -
9Torbicki A. Acute and long term management of pulmonary embolism. Heart. 2010;96(17):1418-24. https://doi.org/10.1136/hrt.2008.153957
» https://doi.org/10.1136/hrt.2008.153957 -
10Sequeira V, van der Velden J. Historical perspective on heart function: the Frank-Starling Law. Biophys Rev. 2015;7(4):421-447. https://doi.org/10.1007/s12551-015-0184-4
» https://doi.org/10.1007/s12551-015-0184-4 -
11Konstantinides S, Torbicki A. Management of venous thrombo-embolism: an update. Eur Heart J. 2014;35(41):2855-63. https://doi.org/10.1093/eurheartj/ehu243
» https://doi.org/10.1093/eurheartj/ehu243 -
12Kasper W, Konstantinides S, Geibel A, Tiede N, Krause T, Just H. Prognostic significance of right ventricular afterload stress detected by echocardiography in patients with clinically suspected pulmonary embolism. Heart. 1997;77(4):346-9. https://doi.org/10.1136/hrt.77.4.346
» https://doi.org/10.1136/hrt.77.4.346 -
13Konstantinides SV. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(45):3145-6.
-
14Jiménez D, Aujesky D, Moores L, Gómez V, Lobo JL, Uresandi F, et al. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med. 2010;170(15):1383-9. https://doi.org/10.1001/archinternmed.2010.199
» https://doi.org/10.1001/archinternmed.2010.199 -
15Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353(9162):1386-9. https://doi.org/10.1016/S0140-6736(98)07534-5
» https://doi.org/10.1016/S0140-6736(98)07534-5 -
16Fernandes CJ, Alves Júnior JL, Gavilanes F, Prada LF, Morinaga LK, Souza R. New anticoagulants for the treatment of venous thromboembolism. J Bras Pneumol. 2016;42(2):146-54. https://doi.org/10.1590/S1806-37562016042020068
» https://doi.org/10.1590/S1806-37562016042020068 -
17Miller GA, Sutton GC, Kerr IH, Gibson RV, Honey M. Comparison of streptokinase and heparin in treatment of isolated acute massive pulmonary embolism. Br Heart J. 1971;33(4):616. https://doi.org/10.1136/bmj.2.5763.681
» https://doi.org/10.1136/bmj.2.5763.681 -
18Bell WR, Simon TL, Stengle JM, Sherry S. The urokinase-streptokinase pulmonary embolism trial (phase II) results. Circulation. 1974;50(6):1070-1. https://doi.org/10.1161/01.CIR.50.6.1070
» https://doi.org/10.1161/01.CIR.50.6.1070 -
19Dalen JE, Alpert JS, Hirsh J. Thrombolytic therapy for pulmonary embolism: is it effective? Is it safe? When is it indicated? Arch Intern Med. 1997;157(22):2550-6. https://doi.org/10.1001/archinte.1997.00440430026003
» https://doi.org/10.1001/archinte.1997.00440430026003 -
20Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110(6):744-9. https://doi.org/10.1161/01.CIR.0000137826.09715.9C
» https://doi.org/10.1161/01.CIR.0000137826.09715.9C -
21Stein PD, Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465-70. https://doi.org/10.1016/j.amjmed.2011.10.015
» https://doi.org/10.1016/j.amjmed.2011.10.015 -
22Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-352. https://doi.org/10.1016/j.chest.2015.11.026
» https://doi.org/10.1016/j.chest.2015.11.026 -
23Goldhaber SZ. Thrombolytic therapy. Adv Intern Med. 1999;44:311-25.
-
24Moorjani N, Price S. Massive pulmonary embolism. Cardiol Clin. 2013;31(4):503-18, vii. https://doi.org/10.1016/j.ccl.2013.07.005
» https://doi.org/10.1016/j.ccl.2013.07.005 -
25Kabrhel C, Rosovsky R, Channick R, Jaff MR, Weinberg I, Sundt T, et al. A Multidisciplinary Pulmonary Embolism Response Team: Initial 30-Month Experience With a Novel Approach to Delivery of Care to Patients With Submassive and Massive Pulmonary Embolism. Chest. 2016;150(2):384-93. https://doi.org/10.1016/j.chest.2016.03.011
» https://doi.org/10.1016/j.chest.2016.03.011 -
26Dalla-Volta S, Palla A, Santolicandro A, Giuntini C, Pengo V, Visioli O, et al. PAIMS 2: alteplase combined with heparin versus heparin in the treatment of acute pulmonary embolism. Plasminogen activator Italian multicenter study 2. J Am Coll Cardiol. 1992;20(3):520-6. https://doi.org/10.1016/0735-1097(92)90002-5
» https://doi.org/10.1016/0735-1097(92)90002-5 -
27Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W; Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002;347(15):1143-50. https://doi.org/10.1056/NEJMoa021274
» https://doi.org/10.1056/NEJMoa021274 -
28Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-11. https://doi.org/10.1056/NEJMoa1302097
» https://doi.org/10.1056/NEJMoa1302097 -
29Konstantinides SV, Vicaut E, Danays T, Becattini C, Bertoletti L, Beyer-Westendorf J, et al. Impact of Thrombolytic Therapy on the Long-Term Outcome of Intermediate-Risk Pulmonary Embolism. J Am Coll Cardiol. 2017;69(12):1536-1544. https://doi.org/10.1016/j.jacc.2016.12.039
» https://doi.org/10.1016/j.jacc.2016.12.039 -
30Hoeper MM, Humbert M, Souza R, Idrees M, Kawut SM, Sliwa-Hahnle K, et al. A global view of pulmonary hypertension. Lancet Respir Med. 2016;4(4):306-22. https://doi.org/10.1016/S2213-2600(15)00543-3
» https://doi.org/10.1016/S2213-2600(15)00543-3 -
31Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; "MOPETT" Investigators. Moderate pulmonary embolism treated with thrombolysis (from the "MOPETT" Trial). Am J Cardiol. 2013;111(2):273-7. https://doi.org/10.1016/j.amjcard.2012.09.027
» https://doi.org/10.1016/j.amjcard.2012.09.027 -
32Kuo WT. Endovascular therapy for acute pulmonary embolism. J Vasc Interv Radiol. 2012;23(2):167-79 e4; quiz 179.
-
33Kucher N, Boekstegers P, Müller OJ, Kupatt C, Beyer-Westendorf J, Heitzer T, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014;129(4):479-86. https://doi.org/10.1161/CIRCULATIONAHA.113.005544
» https://doi.org/10.1161/CIRCULATIONAHA.113.005544 -
34Piazza G, Hohlfelder B, Jaff MR, Ouriel K, Engelhardt TC, Sterling KM, et al. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv. 2015;8(10):1382-92. https://doi.org/10.1016/j.jcin.2015.04.020
» https://doi.org/10.1016/j.jcin.2015.04.020 -
35Kuo WT, Banerjee A, Kim PS, DeMarco FJ Jr, Levy JR, Facchini FR, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015;148(3):667-673. https://doi.org/10.1378/chest.15-0119
» https://doi.org/10.1378/chest.15-0119 -
36Lazar HL, Farber HW. Early pulmonary embolectomy for acute pulmonary embolus: an operation whose time has come. J Card Surg. 2010;25(3):259-60. https://doi.org/10.1111/j.1540-8191.2010.01012.x
» https://doi.org/10.1111/j.1540-8191.2010.01012.x -
37Le RD, Dewan NA. Pulmonary embolectomy: should it be offered earlier rather than later? Respir Care. 2009;54(3):390-2.
-
38Aymard T, Kadner A, Widmer A, Basciani R, Tevaearai H, Weber A, et al. Massive pulmonary embolism: surgical embolectomy versus thrombolytic therapy--should surgical indications be revisited? Eur J Cardiothorac Surg. 2013;43(1):90-4; discussion 94. https://doi.org/10.1093/ejcts/ezs123
» https://doi.org/10.1093/ejcts/ezs123 -
39Lehnert P, Moller CH, Mortensen J, Kjaergaard J, Olsen PS, Carlsen J. Surgical embolectomy compared to thrombolysis in acute pulmonary embolism: morbidity and mortality. Eur J Cardiothorac Surg. 2017;51(2):354-361.
-
1
Study carried out at the Unidade de Circulação Pulmonar, Disciplina de Pneumologia, Instituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
-
Financial support:
None.
Publication Dates
-
Publication in this collection
May-Jun 2018
History
-
Received
12 July 2017 -
Accepted
19 Jan 2018