ABSTRACT
Objective:
To evaluate the trends in smoking prevalence in all Brazilian capitals between 2006 and 2017.
Methods:
This was a study of temporal trends in smoking, based on information from the Telephone-based System for the Surveillance of Risk and Protective Factors for Chronic Diseases. The trends in smoking prevalence were stratified by gender, age, level of education, and capital of residence. We used linear regression analysis with a significance level of 5%.
Results:
From 2006 to 2017, the overall prevalence of smoking in the Brazilian capitals declined from 19.3% to 13.2% among men and from 12.4% to 7.5% among women (p < 0.05 for both). Despite the overall decline in the prevalence of smoking in all of the capitals, the rate of decline was lower in the more recent years. There was also a reduction in the prevalence of former smoking (22.2% in 2006 to 20.3% in 2017). In contrast, there was an upward trend in the prevalence of former smoking among individuals with a lower level of education (from 27.9% in 2006 to 30.0% in 2017). In 2017, the prevalence of smoking among men was highest in the cities of Curitiba, São Paulo, and Porto Alegre, whereas it was highest among women in the cities of Curitiba, São Paulo, and Florianópolis.
Conclusions:
There have been improvements in smoking prevalence in Brazil. Annual monitoring of smoking prevalence can assist in the battle against chronic noncommunicable diseases.
Keywords:
Smoking; Tobacco use disorder; Health surveys
RESUMO
Objetivo:
Avaliar a tendência de indicadores relacionados ao tabagismo nas capitais brasileiras entre os anos de 2006 e 2017.
Métodos:
Estudo de tendência temporal a partir de informações do Sistema de Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico. Os indicadores do tabagismo foram estratificados por sexo, idade, escolaridade e capitais. Utilizou-se análise de regressão linear com nível de significância de 5%.
Resultados:
Considerando-se toda a série, a prevalência de tabagismo caiu de 19,3% (2006) para 13,2% (2017) no sexo masculino e de 12,4% para 7,5% no sexo feminino (p < 0,05 para ambos). Todas as capitais apresentaram um declínio na prevalência de tabagismo para ambos os sexos; entretanto, a velocidade desse declínio foi menor nos últimos anos. Ocorreu uma redução da proporção de ex-fumantes (de 22,2% em 2006 para 20,3% em 2017). Em contrapartida, houve uma tendência de aumento entre os ex-fumantes que tinham escolaridade de 0-8 anos (de 27,9% em 2006 para 30,0% em 2017). Em 2017, as maiores prevalências de tabagismo do sexo masculino foram em Curitiba, São Paulo e Porto Alegre; em relação ao sexo feminino, essas foram em Curitiba, São Paulo e Florianópolis.
Conclusões:
Houve melhoria dos indicadores relacionados ao tabagismo no Brasil. O monitoramento anual dos indicadores de tabagismo auxilia no enfrentamento das doenças crônicas não transmissíveis.
Descritores:
Fumar; Tabagismo; Inquéritos epidemiológicos
INTRODUCTION
Smoking is a major risk factor for chronic respiratory disease, cardiovascular disease, and various cancers.11 Instituto Nacional de Câncer [homepage on the Internet]. Rio de Janeiro: INCA [cited 2018 Nov 18]. Programa Nacional de Controle do Tabagismo-Tratamento do Tabagismo. [Adobe Acrobat document, 18p.] Available from: http://www1.inca.gov.br/inca/Arquivos/tire_duvidas_pnct_2014.pdf
http://www1.inca.gov.br/inca/Arquivos/ti...
Approximately 1.1 billion smokers (i.e., 80% of all smokers) live in low- or middle-income countries, where the burden of smoking-related diseases is highest.22 World Health Organization (WHO) [homepage on the Internet]. Geneva: WHO; 2018 [cited 2018 Nov 18]. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. [Adobe Acrobat document, 135p.]. Available from: http://apps.who.int/iris/bitstream/handle/10665/255874/9789241512824-eng.pdf?sequence=1
http://apps.who.int/iris/bitstream/handl...
Tobacco use represents a major health care system problem because of increased socioeconomic and health care costs.33 Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; 2015 [cited 2018 Nov 18]. Estratégias para o cuidado da pessoa com doença crônica: o cuidado da pessoa tabagista [Adobe Acrobat document, 154p.]; Available from: http://189.28.128.100/dab/docs/portaldab/publicacoes/caderno_40.pdf
http://189.28.128.100/dab/docs/portaldab...
The total cost of smoking has been estimated at US$ 1,436 billion, which is equivalent to 1.8% of the world’s annual gross domestic product.44 Goodchild M, Nargis N, Tursan d’Espaignet E. Global economic cost of smoking-attributable diseases. Tob Control. 2018;27(1):58-64. http://tobaccocontrol.bmj.com/lookup/doi/10.1136/tobaccocontrol-2016-053305
http://tobaccocontrol.bmj.com/lookup/doi...
Approximately 40% of this cost occurs in low- and middle-income countries, reflecting substantial losses caused by smoking.44 Goodchild M, Nargis N, Tursan d’Espaignet E. Global economic cost of smoking-attributable diseases. Tob Control. 2018;27(1):58-64. http://tobaccocontrol.bmj.com/lookup/doi/10.1136/tobaccocontrol-2016-053305
http://tobaccocontrol.bmj.com/lookup/doi...
In addition, the indirect cost of smoking-attributable diseases is estimated at US$ 1,014 billion.44 Goodchild M, Nargis N, Tursan d’Espaignet E. Global economic cost of smoking-attributable diseases. Tob Control. 2018;27(1):58-64. http://tobaccocontrol.bmj.com/lookup/doi/10.1136/tobaccocontrol-2016-053305
http://tobaccocontrol.bmj.com/lookup/doi...
More than 7 million deaths per year are due to smoking, and approximately 890,000 are due to exposure to secondhand smoke.55 World Health Organization (WHO) [homepage on the Internet]. Geneva: WHO; 2018 [cited 2018 Nov 18]. Tobacco. Available from: http://www.who.int/news-room/fact-sheets/detail/tobacco
http://www.who.int/news-room/fact-sheets...
In 2015, smoking accounted for the loss of 150 million disability-adjusted life years.66 GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906. https://linkinghub.elsevier.com/retrieve/pii/S014067361730819X
https://linkinghub.elsevier.com/retrieve...
Smoking is associated with high morbidity and mortality; although the prevalence of smoking has steadily declined worldwide, it remains high in some regions and vulnerable groups.33 Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; 2015 [cited 2018 Nov 18]. Estratégias para o cuidado da pessoa com doença crônica: o cuidado da pessoa tabagista [Adobe Acrobat document, 154p.]; Available from: http://189.28.128.100/dab/docs/portaldab/publicacoes/caderno_40.pdf
http://189.28.128.100/dab/docs/portaldab...
The reduction in smoking prevalence was primarily due to a substantial expansion and strengthening of tobacco control initiatives worldwide.66 GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906. https://linkinghub.elsevier.com/retrieve/pii/S014067361730819X
https://linkinghub.elsevier.com/retrieve...
In Brazil, studies using data from the 1989 Brazilian National Survey on Health and Nutrition, the 2003 Pesquisa Especial de Tabagismo (PETab, Global Adult Tobacco Survey), the 2008 Brazilian National Household Sample Survey, and the 2013 Pesquisa Nacional de Saúde (PNS, Brazilian National Health Survey) have shown a reduction in tobacco use in the country.77 Szklo AS, de Almeida LM, Figueiredo VC, Autran M, Malta D, Caixeta R, et al. A snapshot of the striking decrease in cigarette smoking prevalence in Brazil between 1989 and 2008. Prev Med. 2012;54(2):162-7. https://linkinghub.elsevier.com/retrieve/pii/S009174351100483X
https://linkinghub.elsevier.com/retrieve...
,88 Malta DC, Vieira ML, Szwarcwald CL, Caixeta R, Brito SM, Dos Reis AA. Smoking Trends among Brazilian population - National Household Survey, 2008 and the National Health Survey, 2013. Rev Bras Epidemiol. 2015;18 Suppl 2:45-56. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2015000600045&lng=pt&tlng=pt
http://www.scielo.br/scielo.php?script=s...
Regulatory measures to reduce smoking in Brazil include the implementation of the Framework Convention on Tobacco Control in 2006 and the enactment of the Smoke-Free Law in 2014.99 Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; 2011 [cited 2018 Nov 18]. Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis (DCNT) no Brasil 2011-2022. [Adobe Acrobat document, 160p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf
http://bvsms.saude.gov.br/bvs/publicacoe...
The 2011-2022 Strategic Action Plan to Combat Chronic Noncommunicable Diseases (NCDs) set a goal of reducing tobacco use and implementing surveillance of smoking.99 Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; 2011 [cited 2018 Nov 18]. Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis (DCNT) no Brasil 2011-2022. [Adobe Acrobat document, 160p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf
http://bvsms.saude.gov.br/bvs/publicacoe...
,1010 Malta DC, Silva Jr JB. Brazilian Strategic Action Plan to Combat Chronic Non-communicable Diseases and the global targets set to confront these diseases by 2025: a review [Article in Portuguese]. Epidemiol Serv Saude. 2013;22(1):151-64. http://scielo.iec.gov.br/scielo.php?script=sci_arttext&pid=S1679-49742013000100016
http://scielo.iec.gov.br/scielo.php?scri...
The Sistema de Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico (VIGITEL, Telephone-based System for the Surveillance of Risk and Protective Factors for Chronic Diseases) is an essential tool for monitoring the frequency and distribution of major determinants of chronic NCDs and their risk factors, including smoking.1111 Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Vigitel Brasil 2017: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2018.
The objective of the present study was to evaluate the trends in smoking prevalence in all Brazilian capitals between 2006 and 2017.
METHODS
This was a study of temporal trends in smoking between 2006 and 2017, based on data from the VIGITEL. The VIGITEL is a cross-sectional population-based study that annually assesses adults (≥ 18 years of age) residing in any of the 26 Brazilian state capitals or in the Federal District of Brasília. Between 2006 and 2017, 12 telephone-based surveys were conducted, a total of 54,000 interviews being conducted each year (i.e., approximately 2,000 interviews in each capital city). Details regarding the sampling and data collection process are provided elsewhere.1111 Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Vigitel Brasil 2017: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2018.
In the present study, smoking prevalence was analyzed as follows:
-
Prevalence of current smoking: number of smokers/number of individuals interviewed. Those who answered “yes” to the question “Do you smoke?” were considered to be smokers regardless of the number of cigarettes smoked per day, frequency of smoking, or duration of smoking.
-
Prevalence of former smoking: number of former smokers/number of individuals interviewed. Nonsmokers who answered “yes” to the question “Have you ever smoked?” were considered to be former smokers regardless of the number of cigarettes smoked or the duration of smoking.
-
Prevalence of smoking ≥ 20 cigarettes per day: number of individuals smoking ≥ 20 cigarettes per day/number of individuals interviewed, the number of individuals smoking ≥ 20 cigarettes per day being assessed by the question “How many cigarettes do you smoke per day?”.
As of 2009, smoking prevalence analysis included the following:
-
d. Prevalence of passive smoking at home: number of nonsmokers who reported living with at least one smoker who smoked inside the household/number of individuals interviewed, the number of nonsmokers who reported living with at least one smoker who smoked inside the household being assessed by the question “Do any of the people who live with you usually smoke inside the household?”.
-
e. Prevalence of passive smoking at work: number of nonsmokers who reported having at least one coworker who smoked indoors at work/number of individuals interviewed, the number of nonsmokers who reported having at least one coworker who smoked indoors at work being assessed by the question “Do any of your coworkers usually smoke indoors at work?”.
The temporal trends in smoking prevalence were stratified by gender, age group (18-24, 25-34, 35-44, 45-54, 55-64, and ≥ 65 years), level of education (0-8, 9-11, and ≥ 12 years of schooling), and capital of residence.
A linear regression model was used for trend analysis, the response variable (Yi) being the prevalence of smoking and the explanatory variable (Xi) being the year of study. A negative slope coefficient (β) indicated a reduction in smoking prevalence over the years, whereas a positive slope coefficient indicated an annual increase in prevalence. Analysis of residuals was performed in order to assess the goodness of fit of the model. The level of significance was set at 5%. The Stata statistical software package, version 14 (StataCorp LP, College Station, TX, USA) was used for data processing and statistical analysis.
The VIGITEL was approved by the Brazilian National Research Ethics Committee (Ruling no. 355,590/2013). All participants gave verbal informed consent during the telephone interview.
RESULTS
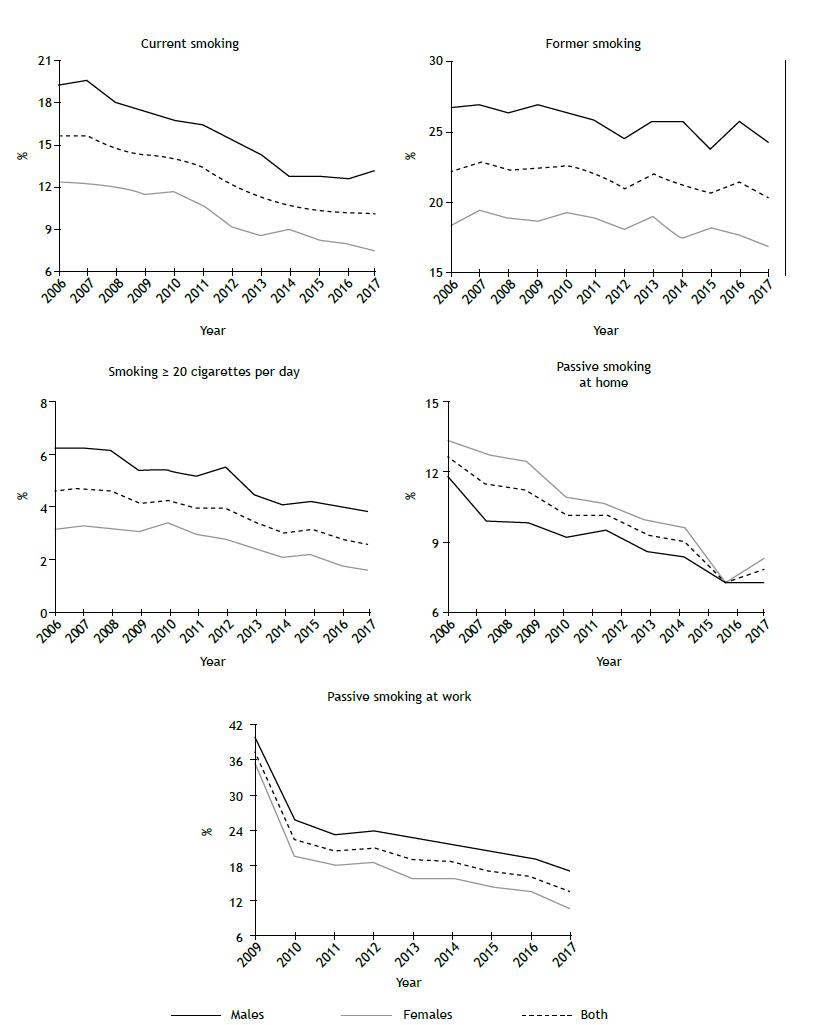
Figure 1 shows the trends in smoking prevalence in Brazil, by gender. There was a trend toward a reduction in smoking prevalence (p < 0.001). The prevalence of current smoking was found to be higher in males than in females (19.3% in 2006 and 13.2% in 2017 vs. 12.4% in 2006 and 7.5% in 2017). This was also true for the prevalence of former smoking, smoking ≥ 20 cigarettes per day, and passive smoking at work. In the 2015-2017 period, there was a reduction in the rate of decline in the prevalence of smoking in the general population and in males. There were reductions in the prevalence of former smoking (from 22.2% in 2006 to 20.3% in 2017; p < 0.001), smoking ≥ 20 cigarettes per day (from 4.6% in 2006 to 2.6% in 2017; p < 0.001), passive smoking at home (from 12.7% in 2006 to 7.9% in 2017; p < 0.001), and passive smoking at work (from 12.1% in 2006 to 6.7% in 2017; p < 0.001) among males and females.
Trends in smoking prevalence in all Brazilian capitals, by gender. VIGITEL, 2006-2017. VIGITEL: Sistema de Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico (Telephone-based System for the Surveillance of Risk and Protective Factors for Chronic Diseases).
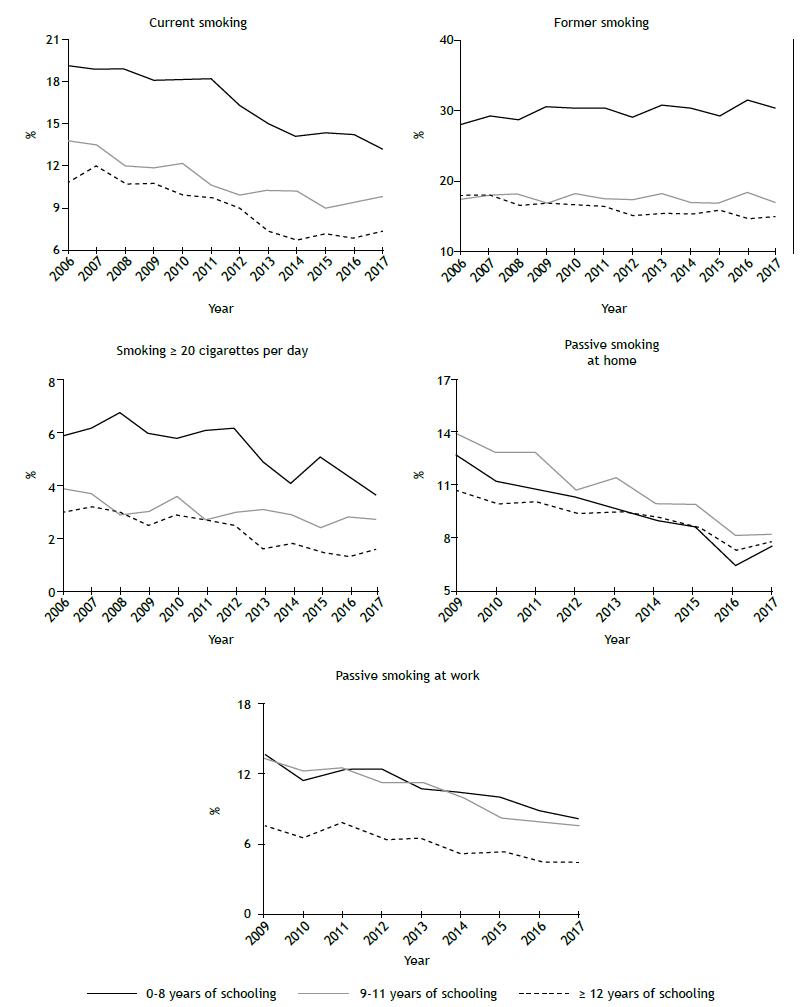
The trends in smoking prevalence in Brazil were also stratified by level of education. There was a trend toward an increase in the prevalence of former smoking among individuals who had had 0-8 years of schooling (from 27.9% in 2006 to 30.0% in 2017; p = 0.0435; slope = 0.159); among those who had had 9-11 years of schooling, there was no significant variation (p = 0.527; β = −0.035); and there was a decrease in the number of former smokers among individuals who had had ≥ 12 years of schooling (p < 0.001; β = −0.270). There was a trend toward a reduction in the prevalence of current smoking, smoking ≥ 20 cigarettes per day, passive smoking at home, and passive smoking at work for all levels of education. The decrease in the prevalence of current smoking and smoking ≥ 20 cigarettes per day was most pronounced among individuals who had had 0-8 years of schooling (p < 0.001; β = −0.591 and p < 0.001; β = −0.232, respectively). The decrease in the prevalence of passive smoking at home and passive smoking at work was most pronounced among individuals who had had 9-11 years of schooling (p < 0.001; β = −0.725), followed by those who had had 0-8 years of schooling (p < 0.001; β = −0.675) and those who had had ≥ 12 years of schooling (p < 0.001; β = −0.373; Figure 2).
Trends in smoking prevalence in all Brazilian capitals, by level of education (number of years of schooling). VIGITEL, 2006-2017. VIGITEL: Sistema de Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico (Telephone-based System for the Surveillance of Risk and Protective Factors for Chronic Diseases).
Table 1 shows the trends in smoking prevalence in Brazil, by age group. There was a trend toward a reduction in the prevalence of current smoking, smoking ≥ 20 cigarettes per day, passive smoking at home, and passive smoking at work in all age groups. The prevalence of smoking was highest in individuals in the 45- to 54-year age bracket between 2006 and 2014, and, as of 2015, in those in the 55- to 64-year age bracket. In all years studied, smoking prevalence was lowest in those ≥ 65 years of age. There was a trend toward an increase in the prevalence of former smoking in individuals in the 55- to 64-year age bracket (p = 0.013; β = 0.390). The prevalence of smoking ≥ 20 cigarettes per day was highest in those in the 45- to 54-year age bracket (p < 0.001; β = −0.507), the rate of increase in the prevalence of smoking ≥ 20 cigarettes per day being highest in individuals in the 55- to 64-year bracket (p = 0.003; β = −0.271). Although the prevalence of passive smoking at home was found to have decreased over the years, it was highest in individuals in the 18- to 24-year age bracket (p < 0.001; β = −0.972). The prevalence of passive smoking at work was highest in individuals in the 35- to 44-year age bracket (p < 0.001; β = −0.975) and in those in the 25- 34-year age bracket (p < 0.001; β = −0.803). Although the prevalence of passive smoking at work was lowest in individuals in the 18-24 year age bracket, the β coefficient was −0.828 in that age group, and there was no significant variation in individuals > 55 years of age.
The prevalence of smoking in males was found to have decreased in all Brazilian capitals. In 2017, smoking prevalence in males was highest in the cities of Curitiba, São Paulo, and Porto Alegre (Table 2). The prevalence of smoking in females was also found to have decreased in all Brazilian capitals. In 2017, smoking prevalence in females was highest in the cities of Curitiba, São Paulo, and Florianópolis (Table 3).
DISCUSSION
The present study showed a reduction in the prevalence of smoking between 2006 and 2017, as well as improvements in the prevalence of former smoking, smoking ≥ 20 cigarettes per day, passive smoking at home, and passive smoking at work. In the 2015-2017 period, there was a reduction in the rate of decline in smoking prevalence in Brazil as a whole and in some of the Brazilian capitals. The prevalence of smoking was highest in males, individuals with a lower level of education, and individuals in the 35- to 64-year age bracket. The prevalence of smoking in 2017 was highest in the capital cities of Curitiba, São Paulo, Porto Alegre, and Florianópolis.
The 2011-2022 Strategic Action Plan to Combat Chronic NCDs set a goal of reducing the prevalence of smoking by 30%.99 Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; 2011 [cited 2018 Nov 18]. Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis (DCNT) no Brasil 2011-2022. [Adobe Acrobat document, 160p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf
http://bvsms.saude.gov.br/bvs/publicacoe...
,1010 Malta DC, Silva Jr JB. Brazilian Strategic Action Plan to Combat Chronic Non-communicable Diseases and the global targets set to confront these diseases by 2025: a review [Article in Portuguese]. Epidemiol Serv Saude. 2013;22(1):151-64. http://scielo.iec.gov.br/scielo.php?script=sci_arttext&pid=S1679-49742013000100016
http://scielo.iec.gov.br/scielo.php?scri...
The World Health Organization Global Action Plan for the Prevention and Control of NCDs and the United Nations 2030 Agenda for Sustainable Development have also set goals of reducing the prevalence of smoking.1212 World Health Organization (WHO) [homepage on the Internet]. Geneva: WHO; 2013 [cited 2018 Nov 18]. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013-2020. [Adobe Acrobat document, 55p.]. Available from: http://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf?sequence=1
http://apps.who.int/iris/bitstream/handl...
,1313 United Nations [homepage on the Internet]. New York: United Nations; 2015 [cited 2018 Nov 18]. Transforming our World: The 2030 Agenda for Sustainable Development. [Adobe Acrobat document, 41p.]. Available from: https://sustainabledevelopment.un.org/content/documents/21252030 Agenda for Sustainable Development web.pdf
https://sustainabledevelopment.un.org/co...
Data from the 1989 Brazilian National Survey on Health and Nutrition showed that the prevalence of tobacco use among adults was 34.8%.1414 Monteiro C, Cavalcante TM, Moura EC, Claro RM, Szwarcwald CL. Population-based evidence of a strong decline in the prevalence of smokers in Brazil (1989-2003). Bull World Health Organ. 2007;85(7):527-34. http://www.who.int/bulletin/volumes/85/7/06-039073.pdf
http://www.who.int/bulletin/volumes/85/7...
Data from the 2003 World Health Survey showed a reduction in smoking prevalence (to 22.4%).1414 Monteiro C, Cavalcante TM, Moura EC, Claro RM, Szwarcwald CL. Population-based evidence of a strong decline in the prevalence of smokers in Brazil (1989-2003). Bull World Health Organ. 2007;85(7):527-34. http://www.who.int/bulletin/volumes/85/7/06-039073.pdf
http://www.who.int/bulletin/volumes/85/7...
The 2008 PETab showed a smoking prevalence of 17.2%,1515 Instituto Nacional de Câncer [homepage on the Internet]. Rio de Janeiro: INCA; 2011 [cited 2018 May 5]. Pesquisa especial de tabagismo PETab: Relatório Brasil. [Adobe Acrobat document, 199p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/pesquisa_especial_tabagismo_petab.pdf
http://bvsms.saude.gov.br/bvs/publicacoe...
and the 2013 PNS showed a smoking prevalence of 14.7%.88 Malta DC, Vieira ML, Szwarcwald CL, Caixeta R, Brito SM, Dos Reis AA. Smoking Trends among Brazilian population - National Household Survey, 2008 and the National Health Survey, 2013. Rev Bras Epidemiol. 2015;18 Suppl 2:45-56. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2015000600045&lng=pt&tlng=pt
http://www.scielo.br/scielo.php?script=s...
,1616 Instituto Brasileiro de Geografia e Estatística (IBGE) [homepage on the Internet]. Rio de Janeiro: IBGE; 2014 [cited 2018 Nov 18]. Pesquisa Nacional de Saúde 2013. [Adobe Acrobat document, 181p.]. Available from: ftp://ftp.ibge.gov.br/PNS/2013/pns2013.pdf These results show that Brazil has made progress in reducing the prevalence of smoking.
Brazil has set a global example on reducing smoking prevalence, and these advances have been attributed to the regulatory measures put forth by the World Health Organization Framework Convention on Tobacco Control, which came into force in 2005. Several measures have been implemented in the country, such as monitoring tobacco use and raising taxes on tobacco products.1717 The Lancet. Slow burn: tobacco control in the Americas. Lancet. 2018;392(10150):796. https://linkinghub.elsevier.com/retrieve/pii/S014067361832066X
https://linkinghub.elsevier.com/retrieve...
,1818 World Health Organization [homepage on the Internet]. Geneva: World Health Organization [cited 2018 Nov 18]. WHO Framework Convention on Tobacco Control 2003. [Adobe Acrobat document, 44p.]. Available from: https://apps.who.int/iris/bitstream/handle/10665/42811/9241591013.pdf;jsessionid=4F94D484511BBA31FD279E97EACAB595?sequence=1
https://apps.who.int/iris/bitstream/hand...
Other measures include Decree no. 5,658, which was issued in 2006 and enacted the Framework Convention on Tobacco Control, banning the advertising of tobacco products1919 Brasil. Presidência da República. Ministério das Relações Exteriores. Decreto no 5.658, de 2 de janeiro de 2006. Promulga a Convenção-Quadro sobre Controle do Uso do Tabaco, adotada pelos países membros da Organização Mundial de Saúde em 21 de maio de 2003 e assinada pelo Brasil em 16 de junho de 2003. Brasília:o Ministério; 2006.; Law no. 12,546, which was issued in 2011 and established smoke-free environments2020 Brasil. Presidência da República. Ministério da Casa Civil. Subchefia para Assuntos Jurídicos [homepage on the Internet]. Lei no. 12.546, de 14 de dezembro de 2011; [about 140 screens]. Available from: http://www.planalto.gov.br/CCIVIL_03/_Ato2011-2014/2011/Lei/L12546.htm
http://www.planalto.gov.br/CCIVIL_03/_At...
; and Decree no. 8,262/2014, which regulated smoke-free environments, increased the size of text and graphic warnings on the packages of tobacco products and other smoking products, prohibited the sale of tobacco products and other smoking products to minors (individuals under 18 years of age), established a minimum price for tobacco products and other smoking products, and banned smoking advertisements in the media, among other measures.2121 Brasil. Presidência da República. Ministério da Casa Civil. Decreto No 8.262, de 31 de Maio de 2014. Altera o Decreto no 2.018, de 1o de outubro de 1996, que regulamenta a Lei no 9.294, de 15 de julho de 1996. Brasília: o Ministério; 2014.
In recent years, there has been a reduction in the rate of decline in smoking prevalence, a longer observation period being required in order to determine whether this trend will change. This draws attention to the need for new regulatory measures, including the use of plain packaging, enforcement of the law regulating smoke-free environments and point-of-sale advertising, control of illicit tobacco trade, and provision of support to small-scale tobacco farmers for crop diversification.2222 World Health Organization (WHO) [homepage on the Internet]. Geneva: World Health Organization; 2017 [cited 2018 Nov 18]. “Best Buys” and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases. [Adobe Acrobat document, 18p.]. Available from: http://who.int/ncds/management/WHO_Appendix_BestBuys.pdf
http://who.int/ncds/management/WHO_Appen...
Other relevant issues include the impact of the current economic crisis in Brazil, the implementation of fiscal austerity measures, cuts in public spending on social welfare and health care, and the diminishing regulatory role of the Brazilian government.2323 Rasella D, Basu S, Hone T, Paes-Sousa R, Ocké-Reis CO, Millett C. Child morbidity and mortality associated with alternative policy responses to the economic crisis in Brazil: A nationwide microsimulation study. Persson LÅ, editor. PLOS Med. 2018;15(5):e1002570. https://dx.plos.org/10.1371/journal.pmed.1002570
https://dx.plos.org/10.1371/journal.pmed...
24 Schramm JM, Paes-Sousa R ML. Políticas de austeridade e seus impactos na saúde: um debate em tempos de crises. 1st ed. Rio de Janeiro: Fiocruz; 2018.-2525 Malta DC, Duncan BB, Barros MBA, Katikireddi SV, Souza FM, Silva AGD, et al. Fiscal austerity measures hamper noncommunicable disease control goals in Brazil. Cien Saude Colet. 2018;23(10):3115-3122. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232018001003115&lng=pt&tlng=pt
http://www.scielo.br/scielo.php?script=s...
Because of historical, economic, cultural, and social issues, being male is still a determinant of smoking.2626 Paes NL. Economic factors and gender differences in the prevalence of smoking among adults [Article in Portuguese]. Cien Saude Colet. 2016;21(1):53-61. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232016000100053&lng=pt&tlng=pt
http://www.scielo.br/scielo.php?script=s...
In addition, tobacco companies created a brand image that promoted the ideals of prestige, wealth, glamour, masculinity, athleticism, and health.2727 Campaign for Tobacco-Free Kids [homepage on the Internet]. Washington DC: Campaign for Tobacco-Free Kids; 2016 [cited 2018 Oct 20]. Rótulos de advertência de saúde [about 3 screens]. Available from: https://www.tobaccofreekids.org/assets/global/pdfs/pt/HWL_essential_components_pt.pdf
https://www.tobaccofreekids.org/assets/g...
Data from the Global Burden of Disease 2015 study showed that, worldwide, the prevalence of smoking in 2015 was 25.0% among males and 5.4% among females.66 GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906. https://linkinghub.elsevier.com/retrieve/pii/S014067361730819X
https://linkinghub.elsevier.com/retrieve...
Data from two Brazilian national surveys also showed a higher prevalence of smoking in males (18.9% and 21.6%) than in females (11.0% and 13.1%).88 Malta DC, Vieira ML, Szwarcwald CL, Caixeta R, Brito SM, Dos Reis AA. Smoking Trends among Brazilian population - National Household Survey, 2008 and the National Health Survey, 2013. Rev Bras Epidemiol. 2015;18 Suppl 2:45-56. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2015000600045&lng=pt&tlng=pt
http://www.scielo.br/scielo.php?script=s...
,1515 Instituto Nacional de Câncer [homepage on the Internet]. Rio de Janeiro: INCA; 2011 [cited 2018 May 5]. Pesquisa especial de tabagismo PETab: Relatório Brasil. [Adobe Acrobat document, 199p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/pesquisa_especial_tabagismo_petab.pdf
http://bvsms.saude.gov.br/bvs/publicacoe...
The present study showed an upward trend in smoking cessation among individuals with a lower level of education and an increase in the rate of decline in the prevalence of smoking ≥ 20 cigarettes per day, both of which can be attributed to increased tobacco taxation and pricing. Price increases constitute the most cost-effective strategy to reduce the number of smokers and daily tobacco use, especially among younger and lower-income individuals.2828 Organização Mundial da Saúde. Organização Pan-Americana da Saúde [homepage on the Internet]. Washington DC: the organization [cited 2019 Feb 4]. MPOWER--Um plano de medidas para reverter a epidemia de tabagismo [Adobe Acrobat document, 39p.]. Available from: https://www.paho.org/bra/index.php?option=com_docman&view=download&alias=375-mpower-um-plano-para-reverter-a-epidemia-tabagismo-5&category_slug=tabagismo-132&Itemid=965
https://www.paho.org/bra/index.php?optio...
A tax increase resulting in a 10% increase in tobacco prices can reduce tobacco use by approximately 4% in high-income countries and approximately 8% in low- and middle-income countries.2828 Organização Mundial da Saúde. Organização Pan-Americana da Saúde [homepage on the Internet]. Washington DC: the organization [cited 2019 Feb 4]. MPOWER--Um plano de medidas para reverter a epidemia de tabagismo [Adobe Acrobat document, 39p.]. Available from: https://www.paho.org/bra/index.php?option=com_docman&view=download&alias=375-mpower-um-plano-para-reverter-a-epidemia-tabagismo-5&category_slug=tabagismo-132&Itemid=965
https://www.paho.org/bra/index.php?optio...
Another strategy is the Protocol to Eliminate Illicit Trade in Tobacco Products,2929 Brasil. Presidência da República. Decreto Nº 9.516, de 1º de Outubro de 2018. Promulga o Protocolo para Eliminar o Comércio Ilícito de Produtos de Tabaco, de 12 de novembro de 2012. Brasília: a Presidência; 2012. the objective of which is to recoup lost taxes and reduce access to low-priced tobacco products available on the black market. Yet another strategy is the provision of universal access to smoking cessation treatment in the Brazilian Unified Health Care System, primarily at primary care clinics.3030 Brasil. Presidência da República. Portaria Nº 571, de 5 de Abril de 2013. Atualiza as diretrizes de cuidado à pessoa tabagista no âmbito da Rede de Atenção à Saúde das Pessoas com Doenças Crônicas do Sistema Único de Saúde (SUS) e dá outras providências. Brasília: a Presidência; 2013.
With regard to the prevalence of smoking among different age groups, our results are similar to those of a study in which the prevalence of smoking was lowest in individuals in the 18- to 24-year age bracket (10.7%) and highest in those in the 40- to 59-year age bracket (19.4%).1414 Monteiro C, Cavalcante TM, Moura EC, Claro RM, Szwarcwald CL. Population-based evidence of a strong decline in the prevalence of smokers in Brazil (1989-2003). Bull World Health Organ. 2007;85(7):527-34. http://www.who.int/bulletin/volumes/85/7/06-039073.pdf
http://www.who.int/bulletin/volumes/85/7...
In a study using data from the 2008 Brazilian National Household Sample Survey, the prevalence of smoking was found to increase with age up to the age of 59 years, decreasing among the elderly.3131 Parmar D, Stavropoulou C, Ioannidis JP. Health outcomes during the 2008 financial crisis in Europe: systematic literature review. BMJ. 2016;354:i4588. http://www.bmj.com/lookup/doi/10.1136/bmj.i4588
http://www.bmj.com/lookup/doi/10.1136/bm...
Brazil is characterized by great cultural diversity, and there are large socioeconomic differences across individuals in the country, all of which can have an impact on tobacco use patterns.3232 Barros AJ, Cascaes AM, Wehrmeister FC, Martínez-Mesa J, Menezes AM. Tobacco smoking in Brazil: regional inequalities and prevalence according to occupational characteristics [Article in Portuguese]. Cien Saude Colet. 2011;16(9):3707-16. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232011001000008&lng=pt&tlng=pt
http://www.scielo.br/scielo.php?script=s...
The fact that the southern region of Brazil is the largest tobacco producer in the country can have a social, political, economic, and cultural impact on tobacco acceptance and use there, and might explain why smoking prevalence was highest in that region.3333 Secretaria de Estado da Agricultura e do Abastecimento do Paraná [homepage on the Internet]. Curitiba: a Secretaria; 2017 [cited 2018 Nov 18]. Prognóstico Fumo. [Adobe Acrobat document, 16p.]. Available from: http://www.agricultura.pr.gov.br/arquivos/File/deral/Prognosticos/2018/Fumo_2017_18.pdf
http://www.agricultura.pr.gov.br/arquivo...
Data from the PETab and the PNS also show that smoking prevalence is highest in southern Brazil and in the state of São Paulo.1515 Instituto Nacional de Câncer [homepage on the Internet]. Rio de Janeiro: INCA; 2011 [cited 2018 May 5]. Pesquisa especial de tabagismo PETab: Relatório Brasil. [Adobe Acrobat document, 199p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/pesquisa_especial_tabagismo_petab.pdf
http://bvsms.saude.gov.br/bvs/publicacoe...
In order to advance in the fight against chronic NCDs and their risk factors (particularly smoking), policy decisions and new regulatory measures conflicting with the interests of the tobacco industry are needed so that the goals of reducing the prevalence of smoking set by the Strategic Action Plan to Combat Chronic NCDs, the World Health Organization Global Action Plan for the Prevention and Control of NCDs, and the United Nations 2030 Agenda for Sustainable Development can be achieved.
ACKNOWLEDGMENTS
We would like to thank the Brazilian National Ministry of Health Department of Health Surveillance technicians who participated in the implementation and operationalization of the VIGITEL.
REFERENCES
-
1Instituto Nacional de Câncer [homepage on the Internet]. Rio de Janeiro: INCA [cited 2018 Nov 18]. Programa Nacional de Controle do Tabagismo-Tratamento do Tabagismo. [Adobe Acrobat document, 18p.] Available from: http://www1.inca.gov.br/inca/Arquivos/tire_duvidas_pnct_2014.pdf
» http://www1.inca.gov.br/inca/Arquivos/tire_duvidas_pnct_2014.pdf -
2World Health Organization (WHO) [homepage on the Internet]. Geneva: WHO; 2018 [cited 2018 Nov 18]. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. [Adobe Acrobat document, 135p.]. Available from: http://apps.who.int/iris/bitstream/handle/10665/255874/9789241512824-eng.pdf?sequence=1
» http://apps.who.int/iris/bitstream/handle/10665/255874/9789241512824-eng.pdf?sequence=1 -
3Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; 2015 [cited 2018 Nov 18]. Estratégias para o cuidado da pessoa com doença crônica: o cuidado da pessoa tabagista [Adobe Acrobat document, 154p.]; Available from: http://189.28.128.100/dab/docs/portaldab/publicacoes/caderno_40.pdf
» http://189.28.128.100/dab/docs/portaldab/publicacoes/caderno_40.pdf -
4Goodchild M, Nargis N, Tursan d’Espaignet E. Global economic cost of smoking-attributable diseases. Tob Control. 2018;27(1):58-64. http://tobaccocontrol.bmj.com/lookup/doi/10.1136/tobaccocontrol-2016-053305
» http://tobaccocontrol.bmj.com/lookup/doi/10.1136/tobaccocontrol-2016-053305 -
5World Health Organization (WHO) [homepage on the Internet]. Geneva: WHO; 2018 [cited 2018 Nov 18]. Tobacco. Available from: http://www.who.int/news-room/fact-sheets/detail/tobacco
» http://www.who.int/news-room/fact-sheets/detail/tobacco -
6GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906. https://linkinghub.elsevier.com/retrieve/pii/S014067361730819X
» https://linkinghub.elsevier.com/retrieve/pii/S014067361730819X -
7Szklo AS, de Almeida LM, Figueiredo VC, Autran M, Malta D, Caixeta R, et al. A snapshot of the striking decrease in cigarette smoking prevalence in Brazil between 1989 and 2008. Prev Med. 2012;54(2):162-7. https://linkinghub.elsevier.com/retrieve/pii/S009174351100483X
» https://linkinghub.elsevier.com/retrieve/pii/S009174351100483X -
8Malta DC, Vieira ML, Szwarcwald CL, Caixeta R, Brito SM, Dos Reis AA. Smoking Trends among Brazilian population - National Household Survey, 2008 and the National Health Survey, 2013. Rev Bras Epidemiol. 2015;18 Suppl 2:45-56. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2015000600045&lng=pt&tlng=pt
» http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2015000600045&lng=pt&tlng=pt -
9Brasil. Ministério da Saúde [homepage on the Internet]. Brasília: Ministério da Saúde; 2011 [cited 2018 Nov 18]. Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis (DCNT) no Brasil 2011-2022. [Adobe Acrobat document, 160p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf
» http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf -
10Malta DC, Silva Jr JB. Brazilian Strategic Action Plan to Combat Chronic Non-communicable Diseases and the global targets set to confront these diseases by 2025: a review [Article in Portuguese]. Epidemiol Serv Saude. 2013;22(1):151-64. http://scielo.iec.gov.br/scielo.php?script=sci_arttext&pid=S1679-49742013000100016
» http://scielo.iec.gov.br/scielo.php?script=sci_arttext&pid=S1679-49742013000100016 -
11Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Vigitel Brasil 2017: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2018.
-
12World Health Organization (WHO) [homepage on the Internet]. Geneva: WHO; 2013 [cited 2018 Nov 18]. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013-2020. [Adobe Acrobat document, 55p.]. Available from: http://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf?sequence=1
» http://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf?sequence=1 -
13United Nations [homepage on the Internet]. New York: United Nations; 2015 [cited 2018 Nov 18]. Transforming our World: The 2030 Agenda for Sustainable Development. [Adobe Acrobat document, 41p.]. Available from: https://sustainabledevelopment.un.org/content/documents/21252030 Agenda for Sustainable Development web.pdf
» https://sustainabledevelopment.un.org/content/documents/21252030 Agenda for Sustainable Development web.pdf -
14Monteiro C, Cavalcante TM, Moura EC, Claro RM, Szwarcwald CL. Population-based evidence of a strong decline in the prevalence of smokers in Brazil (1989-2003). Bull World Health Organ. 2007;85(7):527-34. http://www.who.int/bulletin/volumes/85/7/06-039073.pdf
» http://www.who.int/bulletin/volumes/85/7/06-039073.pdf -
15Instituto Nacional de Câncer [homepage on the Internet]. Rio de Janeiro: INCA; 2011 [cited 2018 May 5]. Pesquisa especial de tabagismo PETab: Relatório Brasil. [Adobe Acrobat document, 199p.]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/pesquisa_especial_tabagismo_petab.pdf
» http://bvsms.saude.gov.br/bvs/publicacoes/pesquisa_especial_tabagismo_petab.pdf -
16Instituto Brasileiro de Geografia e Estatística (IBGE) [homepage on the Internet]. Rio de Janeiro: IBGE; 2014 [cited 2018 Nov 18]. Pesquisa Nacional de Saúde 2013. [Adobe Acrobat document, 181p.]. Available from: ftp://ftp.ibge.gov.br/PNS/2013/pns2013.pdf
-
17The Lancet. Slow burn: tobacco control in the Americas. Lancet. 2018;392(10150):796. https://linkinghub.elsevier.com/retrieve/pii/S014067361832066X
» https://linkinghub.elsevier.com/retrieve/pii/S014067361832066X -
18World Health Organization [homepage on the Internet]. Geneva: World Health Organization [cited 2018 Nov 18]. WHO Framework Convention on Tobacco Control 2003. [Adobe Acrobat document, 44p.]. Available from: https://apps.who.int/iris/bitstream/handle/10665/42811/9241591013.pdf;jsessionid=4F94D484511BBA31FD279E97EACAB595?sequence=1
» https://apps.who.int/iris/bitstream/handle/10665/42811/9241591013.pdf;jsessionid=4F94D484511BBA31FD279E97EACAB595?sequence=1 -
19Brasil. Presidência da República. Ministério das Relações Exteriores. Decreto no 5.658, de 2 de janeiro de 2006. Promulga a Convenção-Quadro sobre Controle do Uso do Tabaco, adotada pelos países membros da Organização Mundial de Saúde em 21 de maio de 2003 e assinada pelo Brasil em 16 de junho de 2003. Brasília:o Ministério; 2006.
-
20Brasil. Presidência da República. Ministério da Casa Civil. Subchefia para Assuntos Jurídicos [homepage on the Internet]. Lei no. 12.546, de 14 de dezembro de 2011; [about 140 screens]. Available from: http://www.planalto.gov.br/CCIVIL_03/_Ato2011-2014/2011/Lei/L12546.htm
» http://www.planalto.gov.br/CCIVIL_03/_Ato2011-2014/2011/Lei/L12546.htm -
21Brasil. Presidência da República. Ministério da Casa Civil. Decreto No 8.262, de 31 de Maio de 2014. Altera o Decreto no 2.018, de 1o de outubro de 1996, que regulamenta a Lei no 9.294, de 15 de julho de 1996. Brasília: o Ministério; 2014.
-
22World Health Organization (WHO) [homepage on the Internet]. Geneva: World Health Organization; 2017 [cited 2018 Nov 18]. “Best Buys” and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases. [Adobe Acrobat document, 18p.]. Available from: http://who.int/ncds/management/WHO_Appendix_BestBuys.pdf
» http://who.int/ncds/management/WHO_Appendix_BestBuys.pdf -
23Rasella D, Basu S, Hone T, Paes-Sousa R, Ocké-Reis CO, Millett C. Child morbidity and mortality associated with alternative policy responses to the economic crisis in Brazil: A nationwide microsimulation study. Persson LÅ, editor. PLOS Med. 2018;15(5):e1002570. https://dx.plos.org/10.1371/journal.pmed.1002570
» https://dx.plos.org/10.1371/journal.pmed.1002570 -
24Schramm JM, Paes-Sousa R ML. Políticas de austeridade e seus impactos na saúde: um debate em tempos de crises. 1st ed. Rio de Janeiro: Fiocruz; 2018.
-
25Malta DC, Duncan BB, Barros MBA, Katikireddi SV, Souza FM, Silva AGD, et al. Fiscal austerity measures hamper noncommunicable disease control goals in Brazil. Cien Saude Colet. 2018;23(10):3115-3122. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232018001003115&lng=pt&tlng=pt
» http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232018001003115&lng=pt&tlng=pt -
26Paes NL. Economic factors and gender differences in the prevalence of smoking among adults [Article in Portuguese]. Cien Saude Colet. 2016;21(1):53-61. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232016000100053&lng=pt&tlng=pt
» http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232016000100053&lng=pt&tlng=pt -
27Campaign for Tobacco-Free Kids [homepage on the Internet]. Washington DC: Campaign for Tobacco-Free Kids; 2016 [cited 2018 Oct 20]. Rótulos de advertência de saúde [about 3 screens]. Available from: https://www.tobaccofreekids.org/assets/global/pdfs/pt/HWL_essential_components_pt.pdf
» https://www.tobaccofreekids.org/assets/global/pdfs/pt/HWL_essential_components_pt.pdf -
28Organização Mundial da Saúde. Organização Pan-Americana da Saúde [homepage on the Internet]. Washington DC: the organization [cited 2019 Feb 4]. MPOWER--Um plano de medidas para reverter a epidemia de tabagismo [Adobe Acrobat document, 39p.]. Available from: https://www.paho.org/bra/index.php?option=com_docman&view=download&alias=375-mpower-um-plano-para-reverter-a-epidemia-tabagismo-5&category_slug=tabagismo-132&Itemid=965
» https://www.paho.org/bra/index.php?option=com_docman&view=download&alias=375-mpower-um-plano-para-reverter-a-epidemia-tabagismo-5&category_slug=tabagismo-132&Itemid=965 -
29Brasil. Presidência da República. Decreto Nº 9.516, de 1º de Outubro de 2018. Promulga o Protocolo para Eliminar o Comércio Ilícito de Produtos de Tabaco, de 12 de novembro de 2012. Brasília: a Presidência; 2012.
-
30Brasil. Presidência da República. Portaria Nº 571, de 5 de Abril de 2013. Atualiza as diretrizes de cuidado à pessoa tabagista no âmbito da Rede de Atenção à Saúde das Pessoas com Doenças Crônicas do Sistema Único de Saúde (SUS) e dá outras providências. Brasília: a Presidência; 2013.
-
31Parmar D, Stavropoulou C, Ioannidis JP. Health outcomes during the 2008 financial crisis in Europe: systematic literature review. BMJ. 2016;354:i4588. http://www.bmj.com/lookup/doi/10.1136/bmj.i4588
» http://www.bmj.com/lookup/doi/10.1136/bmj.i4588 -
32Barros AJ, Cascaes AM, Wehrmeister FC, Martínez-Mesa J, Menezes AM. Tobacco smoking in Brazil: regional inequalities and prevalence according to occupational characteristics [Article in Portuguese]. Cien Saude Colet. 2011;16(9):3707-16. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232011001000008&lng=pt&tlng=pt
» http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232011001000008&lng=pt&tlng=pt -
33Secretaria de Estado da Agricultura e do Abastecimento do Paraná [homepage on the Internet]. Curitiba: a Secretaria; 2017 [cited 2018 Nov 18]. Prognóstico Fumo. [Adobe Acrobat document, 16p.]. Available from: http://www.agricultura.pr.gov.br/arquivos/File/deral/Prognosticos/2018/Fumo_2017_18.pdf
» http://www.agricultura.pr.gov.br/arquivos/File/deral/Prognosticos/2018/Fumo_2017_18.pdf
-
Financial support:
None. -
2
Study carried out at the Escola de Enfermagem, Universidade Federal de Minas Gerais, Belo Horizonte (MG) Brasil.
Publication Dates
-
Publication in this collection
11 Nov 2019 -
Date of issue
2019
History
-
Received
04 Dec 2018 -
Accepted
18 Feb 2019