Abstract
The present study aimed to assess the influence of curing distance on the loss of irradiance and power density of four curing light devices. The behavior in terms of power density of four different dental curing devices was analyzed (Valo, Elipar 2, Radii-Cal, and Optilux-401) using three different distances of photopolymerization (0 mm, 4 mm, and 8 mm). All devices had their power density measured using a MARC simulator. Ten measurements were made per device at each distance. The total amount of energy delivered and the required curing time to achieve 16 J/cm2 of energy was also calculated. Data were statistically analyzed with one-way analysis of variance and Tukey’s tests (p < 0.05). The curing distance significantly interfered with the loss of power density for all curing light devices, with the farthest distance generating the lowest power density and consequently the longer time to achieve an energy density of 16 J/cm2 (p < 0.01). Comparison of devices showed that Valo, in extra power mode, showed the best results at all distances, followed by Valo in high power mode, Valo in standard mode, Elipar 2, Radii-Cal, and Optilux-401 halogen lamp (p < 0.01). These findings indicate that all curing lights induced a significant loss of irradiance and total energy when the light was emitted farther from the probe. The Valo device in extra power mode showed the highest power density and the shortest time to achieve an energy density of 16 J/cm2 at all curing distances.
Curing Lights, Dental; Composite Resins; Dentistry, Operative
Introduction
The development of modern dental composites with a higher proportion of loading filler particles per volume and improved mechanical properties has allowed its use not only on cavities of anterior teeth but also on posterior teeth.11 Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. The 5-year clinical performance of direct composite additions to correct tooth form and position II. Marginal qualities. Clin Oral Investig. 1997 Feb;1(1):19-26. , 22 Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. The 5-year clinical performance of direct composite additions to correct tooth form and position I. Esthetic qualities. Clin Oral Investig. 1997 Feb;1(1):12-8. A truly minimally invasive dentistry was achieved when photocurable materials were used.
A few techniques have strongly influenced dentistry, which includes photopolymerization that has revolutionized the field in the last century.33 Rueggeberg FA. State-of-the-art: dental photocuring- a review. Dent Mater. 2011 Jan;27(1):39-52. Nowadays, the majority of direct composite resins are dependent on this technique.
Unfortunately, on the basis of new findings and studies in the field, it seems that photopolymerization is a subject still being underestimated in both dental schools and offices.44 Price RB, McLeod ME, Felix CM. Quantifying light energy delivered to a Class I restoration. J Can Dent Assoc. 2010;76:a23. Apparently, the process is still being treated as something very simple. To be properly cured, the composite should be illuminated by a blue light for a pre-determined period of time. Power density, irradiance, and location and type of restoration are examples of factors that are also necessary to take into account when the desired outcome is the achievement of properly cured composite restorations.55 Torno V, Soares P, Martin JM, Mazur RF, Souza EM, Vieira S. Effects of irradiance, wavelength, and thermal emission of different light curing units on the Knoop and Vickers hardness of a composite resin. J Biomed Mater Res B Appl Biomater. 2008 Apr;85(1):166-71.
Achieving a high degree of conversion is one of the major concerns during photopolymerization because this is one of the conditions for the long-term success of composite restorations.66 Price RB, Felix CA. Effect of delivering light in specific narrow bandwidths from 394 to 515nm on the microhardness of resin composites. Dent Mater. 2009 Jul;25(7):899-908.However, even with all the improvements in the last years, only 43% out of the 100,000 composite resin restorations analyzed are still in a clinically acceptable situation,77 Burke T, Lucarotti S. Composite resin restoration longevity. J Esthet Restor Dent. 2007;19(4):183-4. a performance that the author compared “only to the worst performing amalgam restoration.”
Uncured restoration will certainly lead to problems, such as increased discoloration, increased marginal defects, decreased hardness, decreased flexural and fracture strengths, decreased dynamic elastic modulus, lower resistance to abrasive wear, decreased bond strength, and poorer biocompatibility of the restoration,88 Michaud PL, Price RB, Labrie D, Rueggeberg FA, Sullivan B. Localised irradiance distribution found in dental light curing units. J Dent. 2014 Feb;42(2):129-39. and as consequence of the latter, mild pulp inflammation. The evolution of this process can culminate in a weak tooth structure and ultimately, crown fracture.
Until recently, scientific literature presented discrepancies on the amount of energy necessary for proper curing of composite resins. Today, it is understood that there is not an absolute value because it varies from composite to composite,88 Michaud PL, Price RB, Labrie D, Rueggeberg FA, Sullivan B. Localised irradiance distribution found in dental light curing units. J Dent. 2014 Feb;42(2):129-39. depending mainly on the type, color, translucency, and the type of photoinitiators are present.
According to previous studies,99 Benetti AR, Asmussen E, Peutzfeldt A. Influence of curing rate of resin composite on the bond strength to dentin. Oper Dent. 2007 Mar-Apr;32(2):144-8. , 1010 Pfeifer CS, Ferracane JL, Sakaguchi RL, Braga RR. Photoinitiator content in restorative composites: influence on degree of conversion, reaction kinetics, volumetric shrinkage and polymerization stress. Am J Dent. 2009 Aug;22(4):206-10. , 1111 Bortolotto T, Dagon C, Krejci I. Light polymerization during cavity filling: effect of exposure reciprocity law and the resulted shrinkage forces on restoration margins. Acta Odontol Scand. 2013 Sep;71(5):1296-302. , 1212 Peutzfeldt A, Asmussen E. Resin composite properties and energy density of light cure. J Dent Res. 2005 Jul;84(7):659-62. , 1313 Gritsch K, Souvannasot S, Schembri C, Farge P, Grosgogeat B. Influence of light energy and power density on the microhardness of two nanohybrid composites. Eur J Oral Sci. 2008 Feb;116(1):77-82. , 1414 Vandewalle KS, Ferracane JL, Hilton TJ, Erickson RL, Sakaguchi RL. Effect of energy density on properties and marginal integrity of posterior resin composite restorations. Dent Mater. 2004 Jan;20(1):96-106. an energy value of 16 J/cm2 was the minimum requirement for adequate mechanical properties of the restorative composite and was considered as the required dose necessary to fully polymerize an increment of 2 mm of composite.
When it comes to photocuring lamps, one important topic is power density,i.e., how much light is emitted in a given area.1515 Park SH, Krejci I, Lutz F. Microhardness of resin composites polymerized by plasma arc or conventional visible light curing. Oper Dent. 2002 Jan-Feb;27(1):30-7. , 1616 Millar BJ, Nicholson JW. Effect of curing with a plasma light on the properties of polymerizable dental restorative materials. J Oral Rehabil. 2001 Jun;28(6):549-52. Power density can also be referred to as irradiance or light intensity and is expressed as mW/cm2. This parameter will determine the amount of energy received by the composite, and ultimately, if the composite will be sufficiently cured or not.
Regrettably, not all light produced reaches the target, particularly when the distance from the tip to the composite increases because of the light dispersion. This energy loss means that there is a risk of the composite not being properly cured1717 Rode KM, Kawano Y, Turbino ML. Evaluation of curing light distance on resin composite microhardness and polymerization. Oper Dent. 2007 Nov-Dec;32(6):571-8. and to make matters even more complicated, emitted light can significantly vary from one lamp to another. However, almost all information shared by manufacturers about their device’s power output refers only to the light emitted at the very tip.44 Price RB, McLeod ME, Felix CM. Quantifying light energy delivered to a Class I restoration. J Can Dent Assoc. 2010;76:a23. It is important to understand how the light beam behaves as the distance from the bottom of the restoration and the tip increases, i.e., the device’s light collimation behavior.
In the present study, the experimental hypothesis was that all curing lights would present a loss of power density (irradiance) of the light being delivered into the composite as the distance between the light tip and composite increased. To test this hypothesis, the amount of irradiance time necessary to achieve 16 J/cm2 of energy density received from different photopolymerization devices at three different distances was evaluated, simulating conditions commonly found in clinical practice.
Thus, the aim of this study was to evaluate the changes in irradiance and energy density related to different curing distances.
Methodology
The behavior in terms of power density of four different dental curing devices was analyzed at three different distances of photopolymerization commonly found in the clinical practice: 0 mm, which serves as parameter to a regular anterior restoration; 4 mm, which relates to the deepest surface of a regular class I restoration; and 8 mm, simulating the deepest surface of a regular class II restoration.1818 Price RB, Fahey J, Felix CM. Knoop microhardness mapping used to compare the efficacy of LED, QTH and PAC curing lights. Oper Dent. 2010 Jan-Feb;35(1):58-68. , 1919 Price RB, Fahey J, Felix CM. Knoop hardness of five composites cured with single-peak and polywave LED curing lights. Quintessence Int. 2010 Nov-Dec;41(10):e181-91.
Four different dental curing lights were tested. Three were light emitting diodes (LED) devices: Elipar Freelight 2 (3M ESPE, Saint Paul, USA); Radii-cal (SDI Limited, Victoria, Australia), and Valo (Ultradent Products, South Jordan, USA). The last device was also tested for its three modes of operation (standard, high, and extra power). The fourth device used as a control group, was a halogen lamp, the Optilux 401 (Demetron/Kerr, Danbury, USA).
According to the manufacturer, Radii-cal presents a power density of 1,200 mW/cm2. During the first 5 s, the emitted light of this device gradually increased and was emitted in pulses. It presented only one high energy LED, which emitted a blue light within the range of 430–480 nm.
Elipar Freelight 2 delivered a power density of approximately 1,000 mW/cm2, according to the manufacturer’s instructions and presented a single high energy LED that emitted a blue light also in the range of 430–480 nm.
Both Radii-cal and Elipar Freelight 2 are battery-operated; the device’s battery was fully charged before initiating the study.
Valo lamp was tested in its three available power modes: standard, high, and extra power (1,000, 1,400, and 3,200 mW/cm2, respectively, according to the manufacturer). Of the four different LEDs, Valo is the only LED device that produces different wavelengths at this emission. Two identical LEDs produce blue light at a wavelength of 465 nm, another at 400 nm, and finally, the last one at 445 nm.
Optilux 401 was used as a comparator to an older method of curing, the halogen lamp. According to the manufacturer, it delivers approximately 600 mW/cm2 of power density within a spectral range of 400 nm–525 nm
Valo and Optilux 401 were connected to a surge protector to protect the lamps from voltage spikes and any power peak during photopolymerization.
Elipar Freelight 2, Radii-cal, Optilux 401, and Valo in standard mode were tested for 20 s. Valo on high power mode was tested for 4 s and on extra power mode for 3 s, following the lamp’s default program. Data for mean irradiance (mW/cm2) and energy (J) were gathered 10 times for each lamp and/or lamp power mode at each distance.
For the measurements at all three distances (0, 4, and 8 mm), all lamps were attached to a device, responsible not only for stabilizing the curing lamp but also to control the distance from the tip to the sensor. The device comprised a movable perpendicular axis with proper articulation. The movement of the axis was precisely controlled by a handle. The irradiance data was collected with a MARC simulator (BlueLight analytics Inc., Halifax, Canada). The device presented a cosine-corrector optical fiber irradiance probe capable of capturing all emitted light, which in turn was guided into a spectral calibrated radiometer. The MARC simulator was attached to a dedicated computer running the software (version 3.0.4.0) responsible for the data analysis of mean irradiance in mW/cm2. On the basis of that value, the program calculates the time required to achieve an energy density of 16 J/cm2 based on the Irradiance required for such a value.
The following formulas were used to calculate the time of irradiance required for achieving a value of 16 J/cm2 of energy density:
Irradiance required for 16 J/cm2(mW/cm2) = mean irradiance (mW/cm2) x 16 (J)/total energy delivered (J)
Time required to achieve 16 J/cm2(s) = Irradiance required for 16 J (mW/cm2) x time of irradiant exposure (s)/mean irradiance (mW/cm2)
Statistical analysis
All data was tabulated and statistically analyzed. First, the normality of the data was verified using the Kolmogorov–Smirnov test. After that, the groups were compared using analysis of variance (ANOVA) and complemented by Tukey’s test (p < 0.05).
Results
The behavior of the curing lights tested is expressed in Table 1. One-way ANOVA compared the curing lights at the same emission distance and after that, the same light at different emission distances. Tukey’s post-hoc test verified the possible significant differences. After the possible comparisons, it was noted that all of them showed significant statistical differences (p < 0.01).
Means and standard deviations of irradiance (mW/cm2), total energy (J) and time necessary to achieve 16J (s).
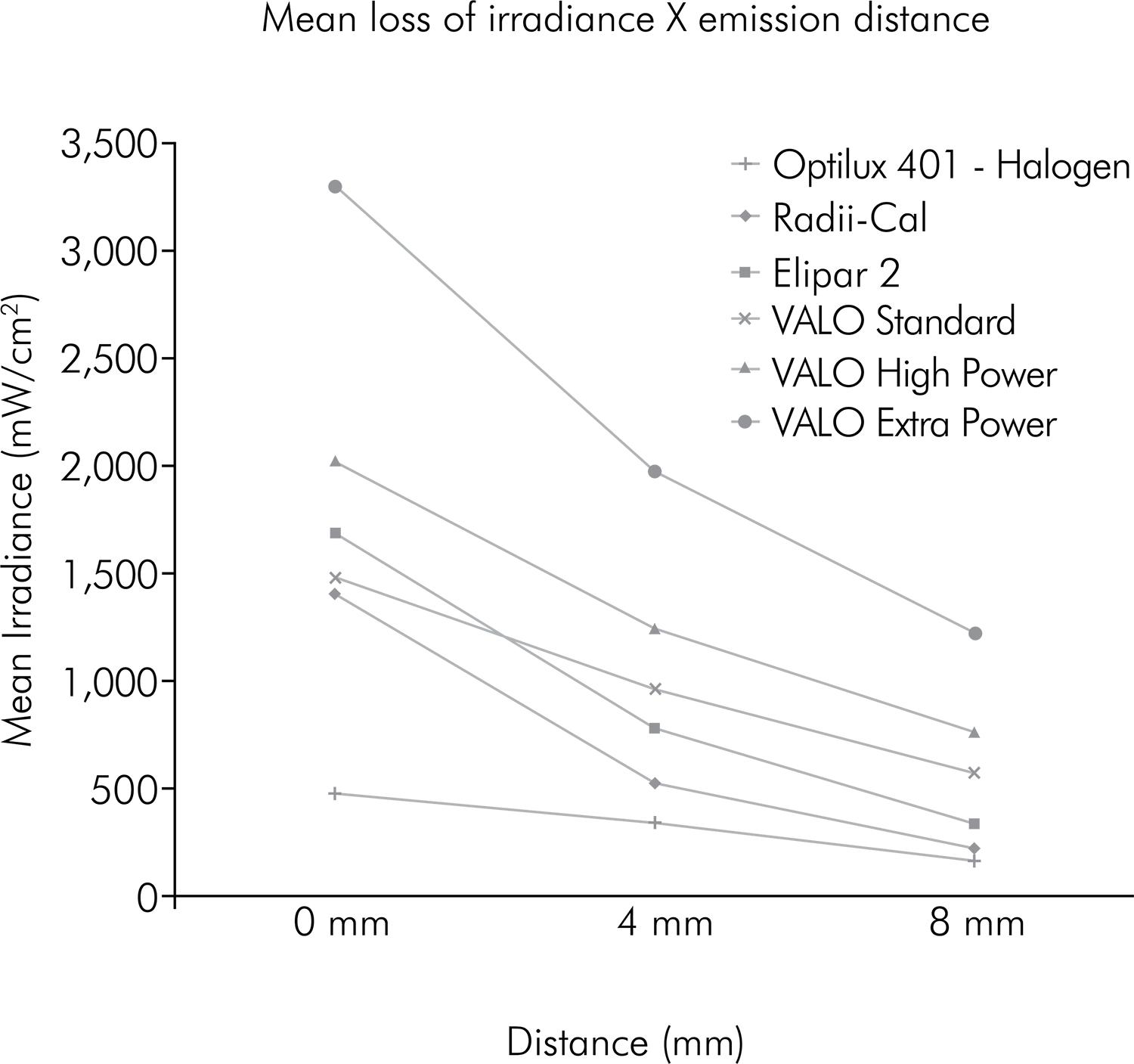
Figure 1 illustrates the mean loss of irradiance (mW/cm2) in relation to the curing light emission distance. It was noted that all curing lights had a significant loss when the emission distance increased.
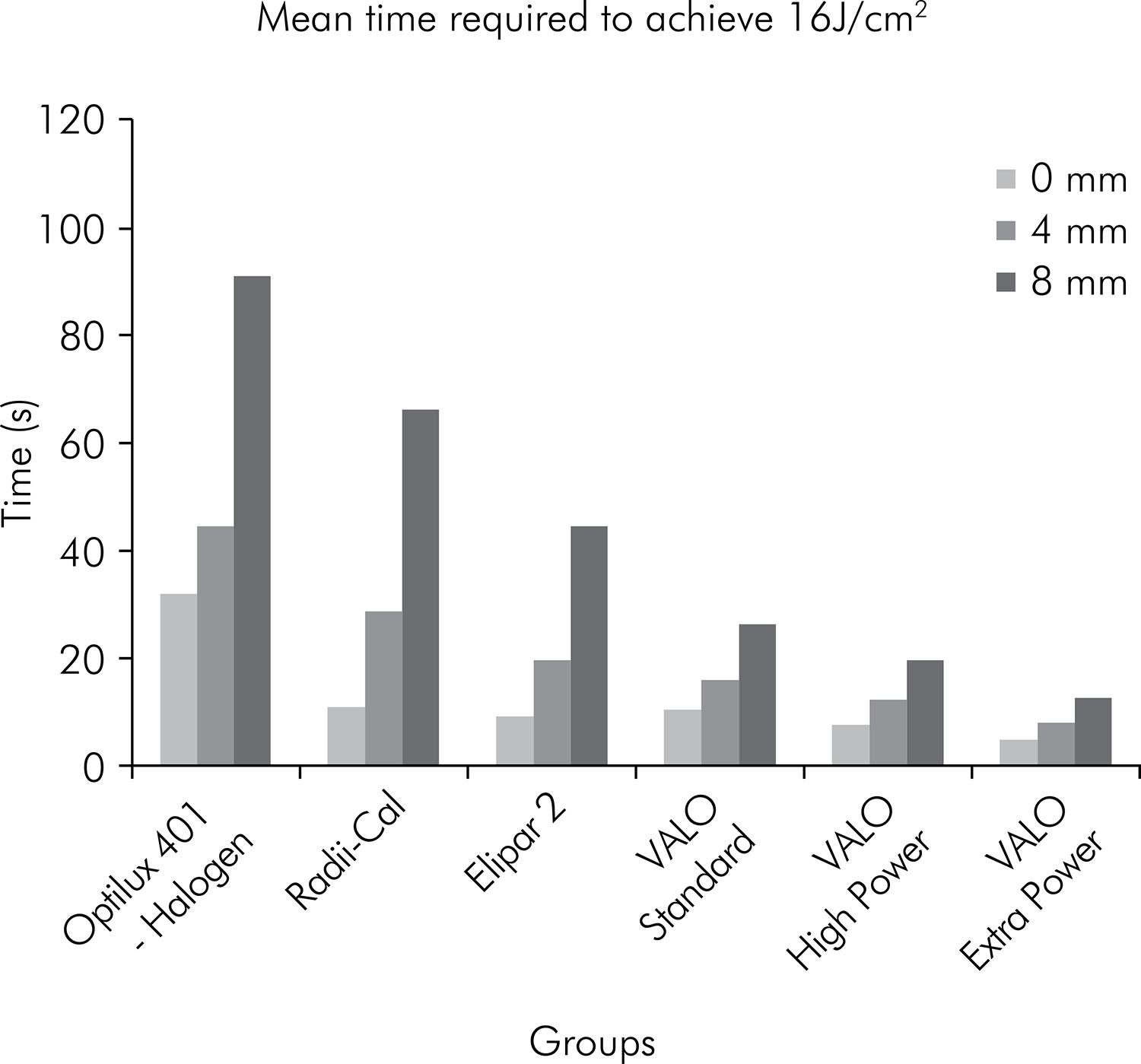
Figure 2 illustrates the mean time required to achieve the energy amount of 16 J/cm2 in relation to the curing light emission distance. It was noted that the greater the emission distance, more time was necessary to achieve a total energy of 16 J/cm2.
Mean time required to achieve an energy density of 16 J/cm2 at each emission distance from the tip to the sensor.
As previously stated, the significant statistical differences between all curing light devices and curing modes were observed. In addition, the significant statistical difference between the curing distances for the same curing light device and/or curing mode was detected. Valo in extra power mode showed the best irradiance results at all distances, followed by Valo in high power mode, Valo in standard mode, Elipar 2, Radii-Cal, and the Optilux-401 halogen lamp (p < 0.01).
Discussion
An important element that should be considered in photocuring lamps is the power density (mW/cm2), also called irradiance or light intensity. The total energy concept2020 Halvorson RH, Erickson RL, Davidson CL. Energy dependent polymerization of resin-based composite. Dent Mater. 2002 Sep;18(6):463-9. , 2121 Koran P, Kurschner R. Effect of sequential versus continuous irradiation of a light-cured resin composite on shrinkage, viscosity, adhesion, and degree of polymerization. Am J Dent. 1998 Feb;11(1):17-22. attests that the photopolymerization process depends on the energy absorbed by the resin and can be summarized by the multiplication of light intensity by the time of exposure (for example, 20 s under a light intensity of 800 mW/cm2 = 20 s x 800 mW/cm2 = 16,000 mWs/cm2 or 16 J/cm2).
In the past, scientific literature reported discrepancies in the amount of energy necessary for the proper curing of composite resins. For example, one study2222 Fróes-Salgado NR, Francci C, Kawano Y. Influência do modo de fotoativação e da distância de irradiação no grau de conversão de um compósito. Perspect Oral Sci 2009 Ago;1(1):11-17. declared that the minimum dose required to achieve good mechanical properties in a cured composite should be at least 24 J/cm2. However, it is better understood that this is not an absolute value and varies from composite to composite,88 Michaud PL, Price RB, Labrie D, Rueggeberg FA, Sullivan B. Localised irradiance distribution found in dental light curing units. J Dent. 2014 Feb;42(2):129-39. depending mainly on the type, color, translucency, and kind of photoinitiators present.
It has been reported that 12 J/cm2 was required to adequately polymerize a 2-mm increment of Z100 (3M ESPE) composite.2323 Yap AU, Seneviratne C. Influence of light energy density on effectiveness of composite cure. Oper Dent. 2001 Sep-Oct;26(5):460-6. However, another work2424 Fan PL, Schumacher RM, Azzolin K, Geary R, Eichmiller FC. Curing-light intensity and depth of cure of resin-based composites tested according to international standards. J Am Dent Assoc. 2002 Apr;133(4):429-34; quiz 491-3. reported that while an energy density of 6–12 J/cm2 cured most composite resins to a depth of 1.5 mm, some composites required more than 18 J/cm2 to achieve an acceptable cure. The manufacturers of Aelite LS and Tetric EvoCeram recommended1313 Gritsch K, Souvannasot S, Schembri C, Farge P, Grosgogeat B. Influence of light energy and power density on the microhardness of two nanohybrid composites. Eur J Oral Sci. 2008 Feb;116(1):77-82. that their composites should receive an energy density of 10–11 J/cm2.
Following previous and more up-to-date studies,99 Benetti AR, Asmussen E, Peutzfeldt A. Influence of curing rate of resin composite on the bond strength to dentin. Oper Dent. 2007 Mar-Apr;32(2):144-8. , 1010 Pfeifer CS, Ferracane JL, Sakaguchi RL, Braga RR. Photoinitiator content in restorative composites: influence on degree of conversion, reaction kinetics, volumetric shrinkage and polymerization stress. Am J Dent. 2009 Aug;22(4):206-10. , 1111 Bortolotto T, Dagon C, Krejci I. Light polymerization during cavity filling: effect of exposure reciprocity law and the resulted shrinkage forces on restoration margins. Acta Odontol Scand. 2013 Sep;71(5):1296-302. , 1212 Peutzfeldt A, Asmussen E. Resin composite properties and energy density of light cure. J Dent Res. 2005 Jul;84(7):659-62. , 1313 Gritsch K, Souvannasot S, Schembri C, Farge P, Grosgogeat B. Influence of light energy and power density on the microhardness of two nanohybrid composites. Eur J Oral Sci. 2008 Feb;116(1):77-82. , 1414 Vandewalle KS, Ferracane JL, Hilton TJ, Erickson RL, Sakaguchi RL. Effect of energy density on properties and marginal integrity of posterior resin composite restorations. Dent Mater. 2004 Jan;20(1):96-106. a value of 16 J/cm2 (16,000 mWs/cm2, according to the concept above) was used as the required dose to completely polymerize an increment of 2 mm composite.
Having that in mind and the knowledge of both the clinical and commercial trend for procedures that requires less chair time,2525 Rueggeberg FA, Cole MA, Looney SW, Vickers A, Swift EJ. Comparison of manufacturer recommended exposure durations with those determined using biaxial flexure strength and scraped composite thickness among a variety of light-curing units. J Esthet Restor Dent. 2009;21(1):43-61. it is important to acknowledge that the manufacturers of dental photocuring lamps suggest curing times not taking into account important composite characteristics, such as the distance from the tip to restoration.33 Rueggeberg FA. State-of-the-art: dental photocuring- a review. Dent Mater. 2011 Jan;27(1):39-52.
The distance from the end of the light guide to the pulpal floor has been reported to be ≥ 4.0 mm, and it can be > 7 mm to the gingival floor of deep preparations.2626 Price RB, Dérand T, Sedarous M, Andreou P, Loney RW. Effect of distance on the power density from two light guides. J Esthet Dent. 2000;12(6):320-7. , 2727 Yearn JA. Factors affecting cure of visible light activated composites. Int Dent J. 1985 Sep;35(3):218-25. Because the light-curing times recommended by dental manufacturers are usually based on placing the tip end of the curing light as close as possible to the surface of the resin, it is clear that this positioning is often difficult or impossible to clinically achieve.2525 Rueggeberg FA, Cole MA, Looney SW, Vickers A, Swift EJ. Comparison of manufacturer recommended exposure durations with those determined using biaxial flexure strength and scraped composite thickness among a variety of light-curing units. J Esthet Restor Dent. 2009;21(1):43-61. , 2828 Price RB, Labrie D, Whalen M, Felix CM. Effect of distance on irradiance and beam homogeneity from 4 light-emitting diode curing units. J Can Dent Assoc. 2011;77:b9. Therefore, it is relevant that the performance of dental curing lights should not be tested only at 0 mm from the end of the light guide; instead, they should be tested at other clinically relevant distances. Previous studies have used 4 mm to represent an average distance, such as a class I restoration, and 8 mm to represent an extreme situation, such as a deep class II restoration.1818 Price RB, Fahey J, Felix CM. Knoop microhardness mapping used to compare the efficacy of LED, QTH and PAC curing lights. Oper Dent. 2010 Jan-Feb;35(1):58-68. , 2222 Fróes-Salgado NR, Francci C, Kawano Y. Influência do modo de fotoativação e da distância de irradiação no grau de conversão de um compósito. Perspect Oral Sci 2009 Ago;1(1):11-17.
In the case of measuring the emitted light from a light source, such as dental curing lights, several previous studies rely on validity devices called “hand-held curing radiometers”.33 Rueggeberg FA. State-of-the-art: dental photocuring- a review. Dent Mater. 2011 Jan;27(1):39-52. Unfortunately, significant discrepancies among the measurement of light unit output have been reported using such hand-held dental curing radiometers; thus, validating that they are not considered reliable indicators in ranking the potential for depths of cure among lights.33 Rueggeberg FA. State-of-the-art: dental photocuring- a review. Dent Mater. 2011 Jan;27(1):39-52. , 2929 Hansen EK, Asmussen E. Reliability of three dental radiometers. Scand J Dent Res. 1993 Apr;101(2):115-9. , 3030 Rueggeberg FA. Precision of hand-held dental radiometers. Quintessence Int. 1993 Jun;24(6):391-6.
The device used in the present study was a cosine-corrector fiber optic irradiance probe capable of capturing all emitted light, which in turn was guided into a spectral calibrated radiometer. This is relevant because it presents a very precise measurement of the energy actually received and not only the energy emitted from the light tip. This device is highly efficient in capturing the emitted light as well as measuring the critical energy required to cure dental composites adequately.33 Rueggeberg FA. State-of-the-art: dental photocuring- a review. Dent Mater. 2011 Jan;27(1):39-52.
Table 1 shows the extensive discrepancies among the tested devices. While for 0 mm, the values for most LED devices were somewhat similar regarding irradiance, differences were observed as the distance of the tip to the sensor increased and/or when lamps were used in more powerful modes. For example, Radii-cal, Elipar 2, and Valo in standard mode were able to deliver sufficient light energies to reach 16 J/cm2 at similar times of 11.28 ± 0.33 s; 9.43 ± 0.05 s, and 10.77 ± 0.4 s, respectively. Optilux-401 halogen lamp required a clinically significant longer time, as shown by the results: 33.22 ± 0.23; and Valo on high power and extra power required less time: 7.83 ± 0.07 and 4.84 ± 0.07, respectively.
However, when the distance between the tip and the sensor increased, the time to achieve 16 J/cm2 also increased; i.e., from 11.28 ± 0.33 s at 0 mm, Radii-cal required 69.07 ± 1.25 s at 8 mm, which was a significantly longer duration than those recommended by most manufacturers. Similarly, Elipar increased from 9.43 ± 0.05 to 46.48 ± 0.43 s. Valo in both standard and high power modes increased from 10.77 ± 0.4 s to 27.62 ± 0.08 s and from 7.83 ± 0.07 s to 20.74 ± 0.16 s, respectively. The least time was achieved by Valo in the extra power mode (13.03 ± 0.09 s) and the highest time by Optilux-401 halogen lamp (94.96 ± 1.47 s).
Figure 1 displays the mean irradiance loss versus the distance from the tip to the sensor. It can be noted that all devices lost power as the distance from the light emitting tip and the sensor increased.
Figure 2 illustrates the time required to achieve an energy density of 16 J/cm2 at each emission distance from the tip to the sensor. All devices required a proportionally longer exposure time to achieve a 16 J/cm2 delivered energy.
This information is relevant in clinical practice because it differs from the guidelines of light exposure time suggested by the manufacturers of various lamps in the dental market.
Conclusions
Within the limitations of the present study, it was concluded that all curing lights had a significant loss of irradiance and total energy when the light was emitted farther from the probe. Consequently, the mean time to achieve the total energy density of 16 J/cm2 significantly increased as the distance from the tip to the sensor increased.
On comparing devices, it was observed that Valo in the extra power mode showed the best irradiance results at all distances, followed by Valo in high power mode, Valo in standard mode, Elipar 2, Radii-Cal, and Optilux-401 halogen lamp (p < 0.01).
References
-
1Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. The 5-year clinical performance of direct composite additions to correct tooth form and position II. Marginal qualities. Clin Oral Investig. 1997 Feb;1(1):19-26.
-
2Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. The 5-year clinical performance of direct composite additions to correct tooth form and position I. Esthetic qualities. Clin Oral Investig. 1997 Feb;1(1):12-8.
-
3Rueggeberg FA. State-of-the-art: dental photocuring- a review. Dent Mater. 2011 Jan;27(1):39-52.
-
4Price RB, McLeod ME, Felix CM. Quantifying light energy delivered to a Class I restoration. J Can Dent Assoc. 2010;76:a23.
-
5Torno V, Soares P, Martin JM, Mazur RF, Souza EM, Vieira S. Effects of irradiance, wavelength, and thermal emission of different light curing units on the Knoop and Vickers hardness of a composite resin. J Biomed Mater Res B Appl Biomater. 2008 Apr;85(1):166-71.
-
6Price RB, Felix CA. Effect of delivering light in specific narrow bandwidths from 394 to 515nm on the microhardness of resin composites. Dent Mater. 2009 Jul;25(7):899-908.
-
7Burke T, Lucarotti S. Composite resin restoration longevity. J Esthet Restor Dent. 2007;19(4):183-4.
-
8Michaud PL, Price RB, Labrie D, Rueggeberg FA, Sullivan B. Localised irradiance distribution found in dental light curing units. J Dent. 2014 Feb;42(2):129-39.
-
9Benetti AR, Asmussen E, Peutzfeldt A. Influence of curing rate of resin composite on the bond strength to dentin. Oper Dent. 2007 Mar-Apr;32(2):144-8.
-
10Pfeifer CS, Ferracane JL, Sakaguchi RL, Braga RR. Photoinitiator content in restorative composites: influence on degree of conversion, reaction kinetics, volumetric shrinkage and polymerization stress. Am J Dent. 2009 Aug;22(4):206-10.
-
11Bortolotto T, Dagon C, Krejci I. Light polymerization during cavity filling: effect of exposure reciprocity law and the resulted shrinkage forces on restoration margins. Acta Odontol Scand. 2013 Sep;71(5):1296-302.
-
12Peutzfeldt A, Asmussen E. Resin composite properties and energy density of light cure. J Dent Res. 2005 Jul;84(7):659-62.
-
13Gritsch K, Souvannasot S, Schembri C, Farge P, Grosgogeat B. Influence of light energy and power density on the microhardness of two nanohybrid composites. Eur J Oral Sci. 2008 Feb;116(1):77-82.
-
14Vandewalle KS, Ferracane JL, Hilton TJ, Erickson RL, Sakaguchi RL. Effect of energy density on properties and marginal integrity of posterior resin composite restorations. Dent Mater. 2004 Jan;20(1):96-106.
-
15Park SH, Krejci I, Lutz F. Microhardness of resin composites polymerized by plasma arc or conventional visible light curing. Oper Dent. 2002 Jan-Feb;27(1):30-7.
-
16Millar BJ, Nicholson JW. Effect of curing with a plasma light on the properties of polymerizable dental restorative materials. J Oral Rehabil. 2001 Jun;28(6):549-52.
-
17Rode KM, Kawano Y, Turbino ML. Evaluation of curing light distance on resin composite microhardness and polymerization. Oper Dent. 2007 Nov-Dec;32(6):571-8.
-
18Price RB, Fahey J, Felix CM. Knoop microhardness mapping used to compare the efficacy of LED, QTH and PAC curing lights. Oper Dent. 2010 Jan-Feb;35(1):58-68.
-
19Price RB, Fahey J, Felix CM. Knoop hardness of five composites cured with single-peak and polywave LED curing lights. Quintessence Int. 2010 Nov-Dec;41(10):e181-91.
-
20Halvorson RH, Erickson RL, Davidson CL. Energy dependent polymerization of resin-based composite. Dent Mater. 2002 Sep;18(6):463-9.
-
21Koran P, Kurschner R. Effect of sequential versus continuous irradiation of a light-cured resin composite on shrinkage, viscosity, adhesion, and degree of polymerization. Am J Dent. 1998 Feb;11(1):17-22.
-
22Fróes-Salgado NR, Francci C, Kawano Y. Influência do modo de fotoativação e da distância de irradiação no grau de conversão de um compósito. Perspect Oral Sci 2009 Ago;1(1):11-17.
-
23Yap AU, Seneviratne C. Influence of light energy density on effectiveness of composite cure. Oper Dent. 2001 Sep-Oct;26(5):460-6.
-
24Fan PL, Schumacher RM, Azzolin K, Geary R, Eichmiller FC. Curing-light intensity and depth of cure of resin-based composites tested according to international standards. J Am Dent Assoc. 2002 Apr;133(4):429-34; quiz 491-3.
-
25Rueggeberg FA, Cole MA, Looney SW, Vickers A, Swift EJ. Comparison of manufacturer recommended exposure durations with those determined using biaxial flexure strength and scraped composite thickness among a variety of light-curing units. J Esthet Restor Dent. 2009;21(1):43-61.
-
26Price RB, Dérand T, Sedarous M, Andreou P, Loney RW. Effect of distance on the power density from two light guides. J Esthet Dent. 2000;12(6):320-7.
-
27Yearn JA. Factors affecting cure of visible light activated composites. Int Dent J. 1985 Sep;35(3):218-25.
-
28Price RB, Labrie D, Whalen M, Felix CM. Effect of distance on irradiance and beam homogeneity from 4 light-emitting diode curing units. J Can Dent Assoc. 2011;77:b9.
-
29Hansen EK, Asmussen E. Reliability of three dental radiometers. Scand J Dent Res. 1993 Apr;101(2):115-9.
-
30Rueggeberg FA. Precision of hand-held dental radiometers. Quintessence Int. 1993 Jun;24(6):391-6.
Publication Dates
-
Publication in this collection
2015
History
-
Received
07 Nov 2014 -
Accepted
15 Jan 2015 -
Reviewed
16 Apr 2015