Abstract
INTRODUCTION: This study aimed to investigate a number of demographic characteristics in males with osteoporosis (OP) treated with bisphosphonate and determine whether any of these measures could act as an effective indicator of medication persistence and compliance. MATERIAL AND METHOD: Among the patients with OP who applied to our clinic and were prescribed weekly oral bisphosphonate treatment, 89 patients over 50 years of age were included in this study. The demographic characteristics of these patients were evaluated. The number of medications used by the patients over the past 1 and 3 years were counted, and the persistence and compliance with bisphosphonate treatment was estimated. The patients were divided into two groups: fully compliant and noncompliant subjects. The two groups of patients were compared separately for 1 and 3 years while considering their demographic characteristics. RESULTS: The mean age of the 89 patients included in the study was 62.43 + 9.41 years. Comparisons among the studied demographic characteristics during the 1-year period of medication use indicated that the educational status of the fully compliant patients was higher. During the 3-year period of medication use, educational status was the only demographic characteristic that was determined to be significantly lower in the noncompliant patients than in the fully compliant group. CONCLUSION: Although deficiencies in medication persistence and compliance during osteoporosis treatment can lead to serious health and social problems in both genders, the causes of these deficiencies have not been thoroughly clarified. We suggest that the educational status of the patient may contribute to these deficiencies.
Osteoporosis; Bisphosphonates; Medication adherence; Medication persistence; Treatment effectivenes
CLINICAL SCIENCE
IMinistry of Health Ankara Diskapi Yildirim Beyazit Training and Research Hospital, Physical Medicine and Rehabilitation Clinic, Ankara, Turkey
IIAnkara Diskapi Yildirim Beyazit Training and Research Hospital, Clinic of Physical Medicine and Rehabilitation, Ankara, Turkey.
ABSTRACT
INTRODUCTION: This study aimed to investigate a number of demographic characteristics in males with osteoporosis (OP) treated with bisphosphonate and determine whether any of these measures could act as an effective indicator of medication persistence and compliance.
MATERIAL AND METHOD: Among the patients with OP who applied to our clinic and were prescribed weekly oral bisphosphonate treatment, 89 patients over 50 years of age were included in this study. The demographic characteristics of these patients were evaluated. The number of medications used by the patients over the past 1 and 3 years were counted, and the persistence and compliance with bisphosphonate treatment was estimated. The patients were divided into two groups: fully compliant and noncompliant subjects. The two groups of patients were compared separately for 1 and 3 years while considering their demographic characteristics.
RESULTS: The mean age of the 89 patients included in the study was 62.43 + 9.41 years. Comparisons among the studied demographic characteristics during the 1-year period of medication use indicated that the educational status of the fully compliant patients was higher. During the 3-year period of medication use, educational status was the only demographic characteristic that was determined to be significantly lower in the noncompliant patients than in the fully compliant group.
CONCLUSION: Although deficiencies in medication persistence and compliance during osteoporosis treatment can lead to serious health and social problems in both genders, the causes of these deficiencies have not been thoroughly clarified. We suggest that the educational status of the patient may contribute to these deficiencies.
Keywords: Osteoporosis; Bisphosphonates; Medication adherence; Medication persistence; Treatment effectivenes.
INTRODUCTION
Osteoporosis (OP) is a structural insufficiency of the bones that is characterized by low bone mass and the impairment of the micro-architectural structure of the bony tissue, leading to increased bone fragility.1,2 Because the increase in bone fragility also increases morbidity and mortality, an accurate early diagnosis and the initiation of an effective mode of treatment are the basic aims of OP treatment.3
Bisphosphonates are commonly used to treat and prevent OP because of their low number of side effects and their ability to inhibit bone resorption.4 They are stable pyropho-sphate analogs that decrease bone destruction by binding to hydroxyapatite crystals in the bone.5 It has been demonstrated in the literature that these medications decrease the formation of new fractures and increase the bone mineral density (BMD).6,7
Despite the reported effectiveness of bisphosphonates for the treatment of OP, studies have shown that regular use and medication compliance are much lower than expected.8,9 Noncompliance reduces the effectiveness of medication treatment, increases the risk of fractures and hospitalization, and creates a serious socioeconomic burden.10 Although the results are controversial, possible factors affecting medication compliance have been reviewed in the literature and include individual demographic characteristics such as the continuity of the medication treatment, patient gender, educational status, diseases accompanying OP, additional medications being taken, timing of medication administration (daily or weekly) and the presence of side effects.11-13
The aim of this study was to investigate a number of demographic characteristics to determine whether any was an effective indicator of persistent medication use and compliance in males with OP who were being treated with bisphosphonate.
MATERIALS AND METHODS
Among the patients who applied to our clinic with OP and who were prescribed weekly oral bisphosphonate treatment, a total of 89 patients over 50 years of age were included in this study. OP treatment was given to patients who had a vertebra/femur BMD of2.5 or below, along with risk factors and/or the presence of clinic symptoms such as extreme kyphosis, back pain, height loss, and so forth. The files of these patients were examined retrospectively. Patients under 50 years of age with secondary OP or those who first presented with OP during the previous 3 years were not included in the study.
The demographic characteristics of the patients included the following details: age; educational level; smoking habits; alcohol consumption; a history of previous fractures; the presence of gastrointestinal system diseases (GIS), such as gastritis or peptic ulcers; the presence of accompanying diseases, such as hypertension or diabetes mellitus; and the presence of additional prescribed medications other than those for OP.
In the evaluation of the demographic characteristics, age is indicated by the year of birth and education level is indicated as one of the following: illiterate, literate, elementary school, junior high school, high school, higher education vocational school or university. Smoking habits, alcohol consumption, history of previous fractures, the presence of GIS disorders, the presence of comorbidities and the use of additional medications are indicated by the numbers of patients.
At an interval of every three months, the patients were called to the hospital to detect medication levels and were followed for three years.
The amounts of medications used by the patients for 1 and 3 years were measured and the persistence and compliance with bisphosphonate treatment were estimated.
The persistence of medication use was estimated by calculating the number of medications taken relative to the number of medications prescribed for 1 and 3 years. Medication compliance was defined as the full administration of medications without skipping any doses and without reducing or increasing the dosage. According to this definition, ''full medication compliance'' was considered as a persistence rating of the medication for 1 and 3 years that was equivalent to 1.
The eighty-nine patients were divided into two groups: fully compliant and noncompliant patients. Fully compliant and noncompliant patients were compared separately after 1 year (n = 44 and n = 45, respectively) and after 3 years (n = 16 and n = 73, respectively) according to their demographic characteristics.
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS) for Windows 11.0. The results are presented as the mean + standard deviation and the number of observations (%) using a chi-square test. Significant differences between the rates of persistence and medication compliance, as well as differences in the demographic characteristics of fully compliant and noncompliant patients, were analyzed with a Pearson chisquare correlation test. Logistic regression analysis was performed for the correlations that were found to be significant. Results were considered to be significant for values of p<0.05.
RESULTS
The mean age of the 89 patients included in the study was 62.43 + 9.41 years and the majority of these patients had completed elementary school. The demographic characteristics of these patients are given in Table 1.
More than 50% of the patients were smokers and nearly 50% presented another disease in addition to OP.
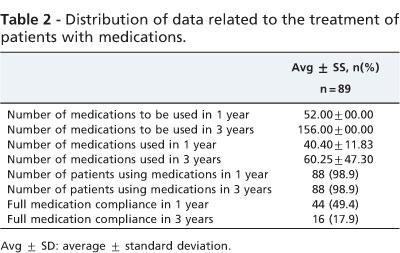
All of the patients were receiving alendronate treatment administered weekly and the number of medication tablets prescribed at 1 year was 52 and the number at 3 years was 156 tablets. One patient (1.1%) had not used the medication at all at the 1-year and 3-year follow-ups. The number of medications used during the treatment period and the distribution of data for full medication compliance are given in Table 2.
A total of 44 patients were in full compliance during the 1-year follow-up, whereas fewer remained in this group at the 3-year follow-up (n = 16, 17.9%).
The rate of persistence at the 1-year follow-up was 0.77+ 0.23 0.57 (0.0-1.0) and the persistence rate at the 3-year follow-up was 0.38 + 0.30 0.19 (0.0-1.0). Upon comparing the medication persistence rates, it was observed that the rate of persistence decreased with long-term use (r= 0.660, p = 0.001).
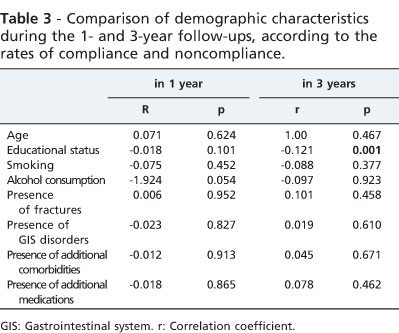
Upon comparing the full compliance rates for the 1- and 3-year periods (49.4% and 17.9%, respectively), it was observed that compliance decreased with long-term use (r= 0.491, p=0.005). A comparison of the demographic characteristics of patients at the 1- and 3-year follow-up periods according to rates of compliance and noncompliance is indicated in Table 3.
Comparison of the studied demographic characteristics during the 1-year period of medication use demonstrated that educational status was higher in the fully compliant patients. In contrast, smoking habits, alcohol consumption, fracture history and the presence of additional diseases and medications were lower in the fully compliant group relative to the noncompliant patients. Although the presence of diseases accompanying OP and the use of additional medications were observed less frequently in the fully compliant patients, these differences were not significant (p>0.05). During the 3-year period of medication use, only educational status was significantly lower in the noncompliant patients when compared with the fully compliant group (p<0.05). According to the regression analysis, educational status effectively influenced the long-term compliance rate among males treated for OP (odds ratio = 0.34, p = 0.001).
DISCUSSION
Until recently, OP has been discussed as a ''woman's disease'' in the literature and studies frequently involve only females. In 2007, OP was reported as an important health issue in males as well and was described as a serious socioeconomic burden.14 Although OP is recognized as occurring less frequently in males, the morbidity and mortality rates in males are higher than in females.15 Although this difference is attributed to the more advanced age of onset in males, the cause has not been fully elucidated. In a study by Kamatari et al.,16 which included 1274 patients with OP, it was reported that medication compliance in males was lower than in females; however, the cause of this noncompliance was not investigated in their study.
In our study, we aimed to determine whether any of the investigated demographic characteristics were effective indicators of medication persistence and compliance in males with OP. On the basis of the results of this study, it was determined that educational status was associated with medication compliance in the long term and with medication persistence. In addition, medication compliance diminished as the treatment period progressed. Medication compliance was not affected by age, smoking habits, alcohol consumption, fracture history, the presence of gastrointestinal diseases, accompanying diseases and additional medications.
There is only one study in the literature investigating the factors affecting medication compliance among males with OP. Hansen et al.17 studied 198 males with OP and examined age, race, body weight, smoking and alcohol habits, fracture history, additional medications and the presence of side effects related to the medication. They reported that compliance was better in the younger patients (mean age of 69) and in the non-smokers after 1 year of medication use. After 2 years of medication use, compliance was better in non-smokers and in those who experienced fewer side effects related to the medication. In that study, full compliance with the medication was reported to be 59% during the first year and 54% at the end of the second year.
Our study differs from that study because the mean age of our patients was lower and because we also evaluated the presence of gastrointestinal disease, compliance after a 3-year treatment period, educational status and the presence of accompanying diseases. Although Hansen's study17 is not directly comparable to ours, when the 1-year results were compared with those of our study, factors such as alcohol consumption, fracture history and additional medications did not affect compliance during a 1-year treatment period; although, medication compliance did decrease by 50% over the 1-year treatment period.
In our study, we determined that smoking habits did not affect compliance with treatment. Although the smoking rate was 53.9% in our study, the same rate was 33% in the study by Hansen et al.17 This difference may be due to the differences in the study groups and health policies of the respective countries. The study by Hansen et al.17 was performed among United States veterans and we believe that this difference may reflect the lower rates of smokers in the U.S. as compared with Turkey or the higher educational status of those individuals compared with the participants in our study.
In addition, despite the results of Hansen et al.17 that indicate that the presence of side effects from the medication are effective indicators, the results of these two studies cannot be compared because the current study aimed only to evaluate whether or not certain demographic characteristics of patients were associated with medication persistence and compliance. However, we did not evaluate medication side effects in the current study.
To the best of our knowledge, there are no other studies on medication persistence and medication compliance in males with OP. However, according to studies in the literature performed among postmenopausal females with OP, medication persistence and medication compliance were better in females with a higher education, which is similar to the results of our study.18 We think that this finding may be attributed to the fact that such patients better comprehend the severity of OP, the necessity of an effective treatment and acknowledge the optimal means of using the medication.
CONCLUSION
Although deficiencies in medication persistence and medication compliance during OP treatment can lead to serious health and social problems in both genders, the causes of these deficiencies are not fully understood. Although the side effects of these medications are frequently reported as effective indicators of persistence and compliance, clinicians should note that factors specific to each patient can also play a role, particularly with respect to long-term use. Education may be the factor that most affects the outcome of long-term treatments. Even if the initiation of a medication does not seem very important, compliance during treatment and follow-up is extremely important. Furthermore, to understand the importance of education level on medication compliance, large-scale and comprehensive studies evaluating the effects of demographic characteristics on medication compliance are required.
Received for publication on October 3, 2010; First review completed on December 6, 2010; Accepted for publication on January 4, 2011
E-mail: ebruumay@gmail.com Tel.: 90 3125962000
- 1. Consensus development conference: prophylaxis and treatment of osteoporosis. Br Med J. 1987;295:914-15, doi: 10.1136/bmj.295.6603.914.
- 2. Dawson-Hughes B Prevention. In: Riggs BL, Melton III LJ (eds.). Osteoporosis: Etiology, Diagnosis, and Management. 2nd ed. Philadelphia: Lippincott-Raven; 1995. p. 335-50.
- 3. Kanis JA, Delmas P, Burckhardt P, Cooper C, Torgerson D. Guidelines for diagnosis and management of osteoporosis. The European Foundation for Osteoporosis and Bone Disease. Osteoporos Int. 1997;7:390-406.
- 4. Fleisch H. Bisphosphonates in osteoporosis: an introduction. Osteoporosis Int. 1993;3:3-5, doi: 10.1007/BF01623000.
- 5. Bartl R. Biologic half-life of bisphosphonates. Dtsch Med Wochenschr. 2009;134:651-2, doi: 10.1055/s-0029-1208102.
- 6. Bone HG, Hosking D, Devogelaer JP, Tucci JR, Emkey RD, Tonino RP et al. Alendronate Phase III Osteoporosis Treatment Study Group. Ten years' experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med. 2004;350:1189-99.
- 7. Hochberg MC, Greenspan S, Wasnich RD, Miller P, Thompson DE, Ross PD. Changes in bone density and turnover explain the reductions in incidence of nonvertebral fractures that occur during treatment with antiresorptive agents. J Clin Endocrinol Metab. 2002;87:1586-92, doi: 10. 1210/jc.87.4.1586.
- 8. Cramer JA, Amonkar MM, Hebborn A, Altman R. Compliance and persistence with bisphosphonate dosing regimens among women with postmenopausal osteoporosis. Curr Med Res Opin. 2005;21:1453-60, doi: 10.1185 / 030079905X61875.
- 9. Curtis JR, Westfall AO, Allison JJ, Freman A, Saag KG. Channeling and adherence with alendronate and risedronate among chronic glucocorticoid users. Osteoporos Int. 2006;17:1268-74, doi: 10.1007/s00198-006-0136-8.
- 10. Huybrechts KF, Ishak KJ, Caro JJ. Assessment of compliance with osteoporosis treatment and its consequences in a managed care population. Bone. 2006;38:922-8, doi: 10.1016/j.bone.2005.10.022.
- 11. Weycker D, Macarios D, Edelsberg J, Oster G. Compliance with medication therapy for postmenopausal osteoporosis. Osteoporos Int.2006;17:1645-52, doi: 10.1007/s00198-006-0179-x.
- 12. Rossini M, Bianchi G, Di Munno O, Giannini S, Minisola S, Sinigaglia L et al. Treatment of Osteoporosis in Clinical Practice (TOP) Study Group. Determinants of adherence to osteoporosis treatment in clinical practice. Osteoporos Int. 2006;17:914-21.
- 13. Lo JC, Pressman AR, Omar MA, Ettinger B. Persistence with weekly alendronate therapy among postmenopausal women. Osteoporos Int.2006;17:922-8, doi: 10.1007/s00198-006-0085-2.
- 14. Schousboe JT, Taylor BC, Fink HA, Kane RL, Cummings SR, Orwoll ES, et al. Cost-effectiveness of bone densitometry followed by treatment of osteoporosis in older men. JAMA. 2007;298:629-37, doi: 10.1001/jama. 298.6.629.
- 15. Gennari L, Bilezikian JP. Osteoporosis in men. Endocrinol Metab Clin North Am. 2007;36(2):399-419, doi: 10.1016/j.ecl.2007.03.008.
- 16. Kamatari M, Koto S, Ozawa N, Urao C, Suzuki Y, Akasaka E, et al. Factors affecting long-term compliance of osteoporotic patients with bisphosphonate treatment and QOL assessment in actual practice: alendronate and risedronate. J Bone Miner Metab. 2007;25:302-9, doi:10.1007/s00774-007-0768-6.
- 17. Hansen KE, Swenson ED, Baltz B, Schuna AA, Jones AN, Elliott ME. Adherence to alendronate in male veterans. Osteoporos Int. 2008;19:349-56, doi: 10.1007/s00198-007-0471-4.
- 18. Barrett-Connor E, Ensrud K, Tosteson AN, Varon SF, Anthony M, Daizadeh N, et al. Design of the POSSIBLE UStrade mark Study: postmenopausal women's compliance and persistence with osteoporosis medications. Osteoporos Int. 2009;20:463-72, doi: 10.1007/s00198-008-0674-3.
The relationship between bisphosphonate use and demographic characteristics of male osteoporosis patients
Publication Dates
-
Publication in this collection
21 Oct 2011 -
Date of issue
2011
History
-
Accepted
04 Jan 2011 -
Reviewed
06 Dec 2010 -
Received
03 Oct 2010