Abstract
OBJECTIVE: To translate, to perform a cultural adaptation of and to test the reproducibility of the Cochin Hand Functional Scale questionnaire for Brazil. METHODS: First, the Cochin Hand Functional Scale questionnaire was translated into Portuguese and was then back-translated into French. These translations were reviewed by a committee to establish a Brazilian version of the questionnaire to be tested. The validity and reproducibility of the Cochin Hand Functional Scale questionnaire was evaluated. Patients of both sexes, who were aged 18 to 60 years and presented with rheumatoid arthritis affecting their hands, were interviewed. The patients were initially interviewed by two observers and were later interviewed by a single rater. First, the Visual Analogue Scale for hand pain, the Arm, Shoulder and Hand Disability questionnaire and the Health Assessment Questionnaire were administered. The third administration of the Cochin Hand Functional Scale was performed fifteen days after the first administration. Ninety patients were assessed in the present study. RESULTS: Two questions were modified as a result of the assessment of cultural equivalence. The Cronbach's alpha value for this assessment was 0.93. The intraclass intraobserver and interobserver correlation coefficients were 0.76 and 0.96, respectively. The Spearman's coefficient indicated that there was a low level of correlation between the Cochin Hand Functional Scale and the Visual Analogue Scale for pain (0.46) and that there was a moderate level of correlation of the Cochin Scale with the Health Assessment Questionnaire (0.66) and with the Disability of the Arm, Shoulder and Hand questionnaire (0.63). The average administration time for the Cochin Scale was three minutes. CONCLUSION: The Brazilian version of the Cochin Hand Functional Scale was successfully translated and adapted, and this version exhibited good internal consistency, reliability and construct validity.
Validation Studies; Questionnaires; Hands; Rheumatoid Arthritis; Functional Disability Scale
CLINICAL SCIENCE
Translation, cultural adaptation and reproducibility of the Cochin Hand Functional Scale questionnaire for Brazil
Aline Chiari; Carla Caires de Souza Sardim; Jamil Natour
Division of Rheumatology, Escola Paulista de Medicina da Universidade Federal de São Paulo (UNIFESP), Sao Paulo, Brazil
ABSTRACT
OBJECTIVE: To translate, to perform a cultural adaptation of and to test the reproducibility of the Cochin Hand Functional Scale questionnaire for Brazil.
METHODS: First, the Cochin Hand Functional Scale questionnaire was translated into Portuguese and was then back-translated into French. These translations were reviewed by a committee to establish a Brazilian version of the questionnaire to be tested. The validity and reproducibility of the Cochin Hand Functional Scale questionnaire was evaluated. Patients of both sexes, who were aged 18 to 60 years and presented with rheumatoid arthritis affecting their hands, were interviewed. The patients were initially interviewed by two observers and were later interviewed by a single rater. First, the Visual Analogue Scale for hand pain, the Arm, Shoulder and Hand Disability questionnaire and the Health Assessment Questionnaire were administered. The third administration of the Cochin Hand Functional Scale was performed fifteen days after the first administration. Ninety patients were assessed in the present study.
RESULTS: Two questions were modified as a result of the assessment of cultural equivalence. The Cronbach's alpha value for this assessment was 0.93. The intraclass intraobserver and interobserver correlation coefficients were 0.76 and 0.96, respectively. The Spearman's coefficient indicated that there was a low level of correlation between the Cochin Hand Functional Scale and the Visual Analogue Scale for pain (0.46) and that there was a moderate level of correlation of the Cochin Scale with the Health Assessment Questionnaire (0.66) and with the Disability of the Arm, Shoulder and Hand questionnaire (0.63). The average administration time for the Cochin Scale was three minutes.
CONCLUSION: The Brazilian version of the Cochin Hand Functional Scale was successfully translated and adapted, and this version exhibited good internal consistency, reliability and construct validity.
Keywords: Validation Studies; Questionnaires; Hands; Rheumatoid Arthritis; Functional Disability Scale.
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic autoimmune, systemic and symmetric inflammatory disease that affects synovial joints and often affects small joints, such as those in the hands and feet.1 When the joints in the hands are affected, their functional ability is compromised because this disease affects the strength, dexterity and mobility of the fingers and the wrist.2,3 The impact of chronic diseases such as AR has led to the development of tools for evaluating the physical, mental and social well-being aspects of a patient's quality of life.4,5 Because of the large number of existing tools and to the growing effort to use internationally standardized measures, the cultural adaptation of questionnaires has been widely used by researchers who do not have an assessment tool in their own language.5-7 The Cochin Hand Functional Scale (CHFS) is a scale that was initially developed in France to assess the level of functional disability in the hands of RA patients. This questionnaire consists of 18 questions about common daily activities. It is a valid and reliable scale that has been used in other languages and for other diseases.8-10
The aim of the present study was to translate, to perform a cultural adaptation of and to test the reproducibility of the CHFS for Brazil.
METHODS AND MATERIALS
The original CHFS was translated from French into Brazilian Portuguese by two independent translators, as recommended by Guillemin et al.5,6 The resulting translations were analyzed by a committee that was comprised of a rheumatologist and a physical therapist, who constructed a consensus version in Portuguese (V1). This version was translated into French by two other translators who were not familiar with the original questionnaire. These two versions were compared with the original questionnaire. This comparison demonstrated that there was a semantic equivalence between the two versions. Therefore, V1 (Appendix 1) was accepted as the version for testing as the CHFS-Portuguese.
The RA patients were selected according to the American College of Rheumatology (ACR) criteria.11 The subjects of the present study included RA patients of both sexes, who were aged between 18 and 60 years, with some impairment in the wrist or the hand. The exclusion criteria were the following: a range of motion restriction due to skin lesions or other autoimmune disorders; the presence of a neurological disease; the presence of another musculoskeletal disease in the upper limbs; a previous surgery on the wrist or the hand; trauma in the wrist or hand during the previous week and difficulty understanding the Portuguese language. The participants were consecutively selected at the outpatient clinics of the Division of Rheumatology at a university in São Paulo/Brazil.
The present study was approved by the Ethics Committee of the Universidade Federal de São Paulo, and all of the patients signed a free, prior informed consent statement. V1 of the questionnaire was administered to 30 patients. The items that were not understood by 20% or more of the respondents were analyzed and modified by the committee, and the revised questionnaire was then administered to a new group of 30 patients. The objective of this phase of the testing was to assess the questionnaire's cultural equivalence. After this phase, another group of 30 patients was selected. These patients were interviewed three times. For the first interview, the patients were interviewed twice by two raters to evaluate the interobserver reliability. The second interviews were performed 15 days after the first interview by one of the raters to evaluate the intraobserver reliability. The construct validity was tested during the first session when the Visual Analogue Scale (VAS) for hand pain, the Health Assessment Questionnaire (HAQ)12 and the Disability of the Arm, Shoulder and Hand (DASH) questionnaire13 were administered in addition to the CHFS.
Statistical Analysis
A descriptive analysis was performed using the mean, standard deviation and frequency distribution of the data. An analysis of the intraclass correlation coefficient (ICC), a scatter diagram and a Bland-Altman graph were performed to evaluate the interobserver and intraobserver reproducibility. Spearman's correlation test was used to verify the construct validity. Cronbach's alpha test was performed to assess the internal consistency of the CHFS.
RESULTS
Ninety patients with RA were interviewed. The demographic data are presented in table 1. During the cultural equivalence assessment, 60 patients were interviewed, and two questions were modified. In the initial instructions of the questionnaire, the phrase ''please answer the following questionswithout adapted equipment'' was changed to ''please answer the following questions without using any adaptation; for example, special pencil or special knife.'' In Question 4, the word ''shed was replaced with the word ''dump .
Questionnaire psychometric properties:
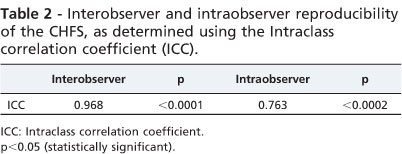
During this stage of the testing, 30 new patients were interviewed. We observed a strong correlation between the interobserver ratings, the scatter diagram (Figure 1a) and the Bland-Altman graph (Figure 1b), in which the majority of the data points were located close to the main diagonal and within the confidence interval (CI) of 95%. The ICC of this analysis was 0.968 (table 2).

Strong correlations were observed for the intraobserver ratings, the scatter diagram (Figure 2a) and the Bland-Altman graph (Figure 2b), in which the majority of the data points were located close to the main diagonal. The ICC of this analysis was 0.763 (table 2).

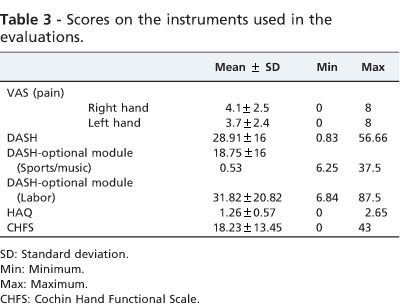
The scores for the instruments that were used during the evaluations are shown in table 3.
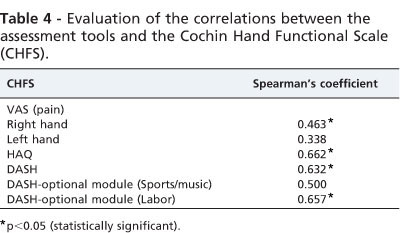
A weak correlation between the CHFS and the VAS for hand pain was observed, and a moderate correlation was observed between the questionnaire and the other tools (HAQ and DASH) (table 4). Cronbach s alpha was 0.933 (95% CI, 0.925 to 0.941), indicating that the questionnaire had internal consistency.
The average time for the administration of the CHFS was 3 minutes.
DISCUSSION
Aspects of quality of life have been evaluated in previous assessments of RA patients. These aspects are generally assessed using questionnaires because the traditional assessment methods, such as the number of painful and swollen joints, the patient s muscle strength and the patient's range of motion (ROM), have been shown to be weak functional and physiological health indicators.15,16 In Brazil, the instruments that have been used and validated for the functional assessment of the hand are skill tests, which require training and special equipment to administer.15 We decided against constructing a new questionnaire to assess hand laterality because several high-quality questionnaires are available in the international literature and are used in other cultures.
The CHFS was chosen for the present study because of its validity and reliability, which have already been established in the international literature.9,17 We also chose the CHFS because this questionnaire includes questions that are similar to other hand function questionnaires that are longer and require a longer administration time.18-20
The average time that was needed to administer the CHFS was 3 minutes, which was similar to the time that was required to administer the original French version. This length of time is reasonable compared with the time that is required to administer the other questionnaires that are frequently used in Brazil, such as the DASH (16.5 minutes) and the SF-36 (seven minutes, on average).13,21
We decided to use the interview method with our patients because of the low educational level of the majority of the patients who seek healthcare at the public health institutions in our country. In addition, this type of assessment was used by Guermazi et al. (2004) during the CHFS validation process for the Arab population, in which the illiteracy level among the study volunteers was 60%.
For the CHFS cultural equivalence assessment, 60 patients were interviewed on two occasions. This number of patients is comparable with the 60 patients that were interviewed during the validation process for the Body Dysmorphic Disorder Examination (BDDE) for Brazil.22 This number is also similar to the number used for validation of the Brazilian version of SF-36 21 and the Arabic and Italian version of the CHFS.9,10
The maximum possible score on the CHFS is 90 points, which is obtained by adding the number of points that are assigned for each question. During the reproducibility process, the average scores that were obtained during the assessments were 18.2 points (obtained by the first interviewer) and 17.9 points (obtained by the second interviewer). These results exhibited a strong correlation of 0.968 for the interobserver reproducibility analysis, both observer evaluation were performed on the same day after an hour-long break. In the original study, this value was 0.96, with a three-hour interval between assessments. For the intraobserver reproducibility, the ICC was 0.763 and indicated a moderate correlation. This result, although relatively strong, does not correspond with the findings of other studies (0.97 and 0.96).8-10 This discrepancy is likely due to the changes that may have occurred in the patients health statuses during the 15-day interval.
The internal consistency of the questionnaire was 0.933, which was measured using the Cronbach s alpha value. This result indicates that although several questions were changed, they retained their concepts and did not lose their original meanings.
The questionnaire's construct validity was based on validated questionnaires in Brazil that are used for this type of patient. The correlation between the VAS and the CHFS for pain was low (0.463), and was similar to the correlation that was observed in the original study (0.52).8 The correlation between the HAQ and the CHFS was moderate (0.662). In patients with systemic sclerosis, the correlation between the CHFS and the HAQ was 0.81.9
The correlation of the CHFS with the DASH was 0.632. A previous review article reported that the DASH questionnaire is appropriate for evaluating the wrist and hand.23 The correlation of the DASH with the other tools was moderate. When the DASH was correlated with the Patient-Rated Wrist Evaluation (PRWE), which is a validated wrist assessment, the DASH was considered valid; it had a strong correlation score (0.796) for patients undergoing surgical treatment for chronic wrist diseases.24,25 These weak-to-moderate correlations can be explained by the fact that the rheumatoid arthritis can affect many parts of the body in addition to the hand. Because the DASH questionnaire evaluates the upper limbs, this assessment may detect differences that include other parts of the arm.
One limitation of our study was the underrepresentation of male patients. However, this underrepresentation does not prevent the measure s use in RA patients because the CHFS was developed to be used for both sexes.
It was concluded that the Brazilian version of the CHFS questionnaire was successfully translated and adapted, with good internal consistency, reliability and construct validity.
ACKNOWLEDGMENTS
We thank Mr. Michel Revel and Mr. Serge Poiraudeau, Hospital Cochin/ Paris, France for authorizing the use of the questionnaire and for answering questions about the questionnaire.
Received for publication on October 15, 2010; First review completed on December 25, 2010; Accepted for publication on January 31, 2011
E-mail: jnatour@unifesp.br Tel.: 55 11 5576-4239
Appendix 1 - Brazilian version of the Cochin Hand Functional Scale (Cochin/Brasil).
Respostas as questões:
0 = sem dificuldade
1 = pouquíssima dificuldade
2 = alguma dificuldade
3 = com muita dificuldade
4 = quase impossível
5 = impossível
Queira responder às perguntas a seguir, sem o uso de adaptacao. Por exemplo, lápis especial, faca especial. As respostas são baseadas na experiência do último mês.
Você consegue.
Na cozinha
1. Segurar uma tigela?
2. Pegar uma garrafa cheia e levantá-la?
3. Segurar um prato cheio?
4. Despejar o líquido de uma garrafa num copo?
5. Desenroscar a tampa de um pote que já foi aberto?
6. Cortar carne com uma faca?
7. Pegar de forma eficaz com o garfo?
8. Descascar uma fruta?
Roupa
9. Abotoar uma camisa?
10. Abrir e fechar zíperes?
Higiene pessoal
11. Apertar um tubo de creme dental?
12. Segurar sua escova de dente de forma eficaz?
No escritório
13. Escrever uma frase curta com um lápis ou uma caneta normal?
14. Escrever uma carta com um laípis ou uma caneta normal?
Diversos
15. Girar uma macçaneta redonda?
16. Utilizar tesouras para cortar um pedacço de papel?
17. Pegar moedas sobre a mesa?
18. Girar uma chave na fechadura?
ERRATA
CLINICS 2011;66(5):731-736
Page 736 Appendix 1 - Brazilian version of the Cochin Hand Functional Scale (Cochin/Brasil). Include: Você consegue.
6. Cortar carne com uma faca?
- 1. Trieb K. Treatment of the wrist in rheumatoid arthritis. J Hand Surg. 2008;33:113-23, doi: 10.1016/j.jhsa.2007.09.011.
- 2. O'Dell JR. Rheumatoid Arthritis: The Disease - Diagnosis and Clinical Features. In: Current Rheumatology Diagnosis & Treatment, 2ďż˝ ed 2007; pp. 161.
- 3. Poole JL, Cordova KJ, Brower LM. Reliabilitiy and validity of a sef-report of hand function in persons with rheumatoid arthritis. J Hand Ther. 2006;19:12-7, doi: 10.1197/j.jht.2005.10.001.
- 4. Bell MJ, Bombardier C, Turgwell P. Measurement of functional status, quality of life, and utility in rheumatoid arthritis. Arthritis and Rheumatism. 1990;3:591-601, doi: 10.1002/art.1780330420.
- 5. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol.1993;46:1417-32, doi: 10.1016/0895-4356(93)90142-N.
- 6. Guillemin F. Cross-cultural adaptation and validation of health status measures - Editorial review. Scand J Rheumatol. 1995;24:61-3, doi: 10. 3109/03009749509099285.
- 7. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25:3186-91, doi: 10.1097/00007632-200012150-00014.
- 8. Duruoz MT, Poiraudeau S, Fermanian J, Menkes CJ Amor B, Dougados M, et al. Development and validation of a rheumatoid hand functional disability scale that assess functional handicap. J Rheumatol. 1996;23:1167-72.
- 9. Ingegnoli F, Galbiati V, Boracchi P, Comi D, Gualtierotti R, Zeni S, et al. Realibility and validity of the Italian version of the hand functional disability scale in patients with Systemic Sclerosis. Clin Rheumatol. 2008;27:743-49, doi: 10.1007/s10067-007-0785-9.
- 10. Guermazi M, Kessomtini W, Poiraudeaus S, Elleuchi M, Fermarian J, Elleuch MH, et al. Development and validation on an Arabic rheumatoid hand disability scale. Disability and Rehabilitation. 2004;26:655-61, doi: 10.1080/09638280410001683164.
- 11. Arnett FC, Edworthy SM, Block DA, McShane DJ, Fries JF, Cooper NS,et al. The American rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis and Rheumatism.1988;31:315-24, doi: 10.1002/art.1780310302.
- 12. Ferraz MB, Oliveira LM, Araujo PMP, Atra E, Tugwell P. Cross cultural reability of the physical ability dimension of the health assessment questionnaire. J Rheumatol. 1990;17:813-7.
- 13. Orfale AG, Araujo PMP, Ferraz MB, Natour J. Translation into Brazilian Portuguese, cultural adaptation and avaluation of the reliability of the Disabiliaty of the Arm, Shoulder and Hand questionnaire. Brazilian Journal of Medical and Biological Research. 2005;38:293-302, doi: 10.1590/S0100-879X2005000200018.
- 14. Falcao DM, Ciconelli RM, Ferraz MB. Translation and cultural adaptation of quality of life questionnaires: An evaluation of methodology.J Rheumatol. 2003;30:379-85.
- 15. Kirkley A, Sharon G. Development of disease-specific quality of life measurement tools. Arthroscopy. 2003;19:1121-28, doi: 10.1016/j.arthro.2003.10.028.
- 16. Oku EC, Pinheiro G da R, Araujo PMP. Instrumentos de avaliaçao functional da mao em pacientes com artrite reumatoide. Fisioterapia Mov. 2009;22:221-28.
- 17. Baillet A, Payraud E, Niderprim V, Nissen M, Allenet B, Francois P, et al. A dynamic exercise programme to improve patients' disability in rheumatoid arthritis: a prospective randomized controlled trial. Rheumatology. 2009;48:410-15, doi: 10.1093/rheumatology/ken511.
- 18. Birtane M, Kabayel DD, Uzunca K, Unlu E, Tastekin N. The relation of hand functions with radiological damage and disease activity in rheumatoid arthritis. Rheumatol Int. 2008;28:407-12, doi: 10.1007/ s00296-007-0461-z.
- 19. Leeb BF, Sautner J, Andel I, Rintelen B. SACRAH: a score for assessment and quantification of chronic rheumatic affections of the hands. Rheumatoloy (Oxford). 2003;42:1173-8, doi: 10.1093/rheumatology/keg319.
- 20. Chung KC, Pillsbury MS, Walters MR, Hayward RA, Arbor A. Reliability and validity testing of the Michigan Hand Outcomes Questionnaire. J Hand Surg. 1998;23A:575-87.
- 21. Ciconelli RM, Ferraz MB, Santos WF, Meinao IM, Quaresma MR. Traduçao para a lingual portuguesa e validaçao do questionario generico de avaliaçao de qualidade de vida SF-36. Rev Bras Reumatol. 1999;39: 143-50.
- 22. Jorge RTB, Sabino Neto M, Natour J, Veiga DF, Jones A, Ferreira LM. Brazilian version of the body dysmorphic disordes examination. Sao Paulo Med J. 2008;126:87-95, doi: 10.1590/S1516-31802008000200005.
- 23. De Semet L. The DASH questionnaire and score in the evaluation of hand and wrist disorders. Acta Orthop Belg. 2008;74:575-81.
- 24. MacDermind JC, Turgeon T, Richards RS, Beadle M, Roth JH. Patients rating of wrist pain and disability: a reliable and valid measurement tool. J Orthop. Trauma. 1998; 12:577-86, doi: 10.1097/00005131-19981100000009.
- 25. Lefevre-Colau MM, Poiraudeau S, Fermanian J, Etchepare F, Alnot JY, Le Viet D, et al. Responsiveness of the Cochin rheumatoid hand disability scale after surgey. Rheumatology. 2001;40:843-50, doi: 10.1093/rheuma tology/40.8.843.
Publication Dates
-
Publication in this collection
14 July 2011 -
Date of issue
2011
History
-
Reviewed
25 Dec 2010 -
Received
15 Oct 2010 -
Accepted
31 Jan 2011