
ABSTRACT
Objective: To describe the learning curve that shows the progress of a single neurosurgeon when performing single-level MI-TLIF. Methods: We included 99 consecutive patients who underwent single-level MI-TLIF by the same neurosurgeon (JASS). Patient’s demographic characteristics were analyzed. In addition, surgical time, intraoperative blood loss and hospital stay were evaluated. The learning curves were calculated with a piecewise regression model. Results: The mean age was 54.6 years. The learning curves showed an inverse relationship between the surgical experience and the variable analyzed, reaching an inflection point for surgical time in case 43 and for blood loss in case 48. The mean surgical time was 203.3 minutes (interquartile range [IQR] 150-240 minutes), intraoperative bleeding was 97.4ml (IQR 40-100ml) and hospital stay of four days (IQR 3-5 days). Conclusions: MI-TLIF is a very frequent surgical procedure due to its effectiveness and safety, which has shown similar results to open procedure. According to this study, the required learning curve is slightly higher than for open procedures, and is reached after about 45 cases.
Keywords:
Learning curve; Lumbar vertebrae; Spinal fusion; Minimally invasive surgical procedures; Intervertebral disc degeneration; Treatment outcome
RESUMO
Objetivo: Descrever a curva de aprendizagem que mostra o progresso de um único neurocirurgião na realização de MI-TLIF em um só nível. Métodos: Foram incluídos 99 pacientes consecutivos submetidos a MI-TLIF de um só nível pelo mesmo neurocirurgião (JASS). Foram analisadas as características demográficas dos pacientes. Além disso, avaliou-se o tempo operatório, a perda de sangue intraoperatória e o tempo de internação hospitalar. As curvas de aprendizagem foram realizadas com um modelo de regressão segmentada. Resultados: A média de idade foi 54,6 anos. As curvas de aprendizagem mostraram uma relação inversa entre a experiência cirúrgica e a variável analisada, atingindo um ponto de inflexão para o tempo de cirurgia no caso 43 e da perda sanguínea no caso 48. O tempo médio de cirurgia foi de 203,3 minutos (amplitude interquartil [IQR] 150 - 240 minutos), de sangramento intraoperatório foi 97,4 ml (IQR 40-100 ml) e de internação hospitalar foi de quatro dias (IQR 3-5 dias). Conclusões: O MI-TLIF é um procedimento realizado com muita frequência devido à sua eficácia e segurança, que tem mostrado resultados comparáveis com o procedimento aberto. De acordo com este estudo, a curva de aprendizagem necessária é ligeiramente maior do que para os procedimentos abertos, sendo que é atingida depois de cerca de 45 casos.
Descritores:
Curva de aprendizado; Vértebras Lombares; Fusão vertebral; Procedimentos cirúrgicos minimamente invasivos; Degeneração do disco intervertebral; Resultado do tratamento
RESUMEN
Objetivo: Describir la curva de aprendizaje que muestre el progreso de un sólo neurocirujano para la realización de MI-TLIF de un sólo nivel. Métodos: Se incluyeron 99 pacientes consecutivos sometidos a MI-TLIF en un solo nivel por un mismo neurocirujano (JASS). Se analizaron las características demográficas de los pacientes. Además se evaluó el tiempo quirúrgico, sangrado transoperatorio y tiempo de estancia hospitalaria. Las curvas de aprendizaje se realizaron con un modelo de regresión dividida en segmentos. Resultados: Se obtuvo un promedio de edad de 54,6 años. Las curvas de aprendizaje mostraron una relación inversa entre la experiencia quirúrgica y la variable analizada, alcanzando un punto de inflexión para tiempo quirúrgico en el caso 43 y para el sangrado en el caso 48. El promedio de tiempo quirúrgico fue de 203,3 minutos (amplitud intercuartil [IQR] 150 - 240 minutos), del sangrado transoperatorio fue 97,4 ml (IQR 40 - 100 ml) y de la estancia hospitalaria fue de cutro días (IQR 3 - 5 días). Conclusiones: El MI-TLIF es un procedimiento realizado con gran frecuencia debido a su efectividad y seguridad y que ha demostrado resultados equiparables con el procedimiento abierto. De acuerdo a este estudio la curva de aprendizaje requerida es discretamente mayor que para procedimientos abiertos, alcanzándola aproximadamente tras 45 casos.
Descriptores:
Curva de aprendizaje; Vértebras lumbares; Fusión vertebral; Procedimientos quirúrgicos mínimamente invasivos; Degeneración del disco intervertebral; Resultado del tratamiento
INTRODUCTION
When a new procedure is being learned, performance tends to improve with experience; however, in medicine there are no accurate measurements to monitor said improvement. This is why learning curves have been adopted, first described in 1936 by TP Wright, an aeronautical engineer, and widely used in industry where performance measurement is very clear. This type of curve has been adopted in clinical practice, although the results are not as compelling as in industry since they involve a greater number of factors.1,21. Hopper AN, Jamison MH, Lewis WG. Learning curves in surgical practice. Postgraduate Medical Journal. 2007;83(986):777-9. To be able to measure learning in a surgical procedure, the procedural factors (surgical time, blood loss, among others) and those related to patient outcome (analgesia requirements, blood transfusions, type of hospitalization, hospital stay, morbidity, mortality, and survival, among others) can be evaluated. It is important to mention that not all the variables are suitable for evaluating all procedures. For example, mortality is not a good factor in the evaluation of procedures with a low risk of mortality.11. Hopper AN, Jamison MH, Lewis WG. Learning curves in surgical practice. Postgraduate Medical Journal. 2007;83(986):777-9.
Transforaminal lumbar interbody fusion (TLIF) is one of the most frequently performed procedures in the field of neurosurgery.33. Zhang Q, Yuan Z, Zhou M, Liu H, Xu Y, Ren Y. A comparison of posterior lumbar interbody fusion and transforaminal lumbar interbody fusion: a literature review and meta-analysis. BMC Musculoskelet Disord. 2014;15:367. In recent years, at the global level, numerous minimally invasive procedures have been developed and implemented and there is increasingly more evidence of their benefits as compared to open surgical procedures, particularly in the case of minimally invasive TLIF (MI-TLIF).4-94. Schizas C, Tzinieris N, Tsiridis E, Kosmopoulos V. Minimally invasive versus open transforaminal lumbar interbody fusion: evaluating initial experience. Int Orthop. 2009;33(6):1683-8. Recently, numerous published articles highlight the major advantages of MI-TLIF, including less blood loss, lower postoperative pain intensity, shorter perioperative hospitalization time, and shorter recovery periods (Oswestry Disability Index).5-75. Lin Y, Chen W, Chen A, Li F. Comparison between minimally invasive and open transforaminal lumbar interbody fusion: a meta-analysis of clinical results and safety outcomes. J Neurol Surg A Cent Eur Neurosurg. 2016;77(1):2-10. Recent review articles suggest that long term MI-TLIF outcomes are comparable to open techniques in terms of fusion and complication percentages.8-108. Seng C, Siddiqui MA, Wong KP, Zhang K, Yeo W, Tan SB, et al. Five-year outcomes of minimally invasive versus open transforaminal lumbar interbody fusion: a matched-pair comparison study. Spine (Phila Pa 1976). 2013;38(23):2049-55. In contrast, exposure to ionizing radiation is one of the main arguments against MI-TLIF.1111. Kim CH, Lee CH, Kim KP. How high are radiation-related risks in minimally invasive transforaminal lumbar interbody fusion compared with traditional open surgery?: a meta-analysis and dose estimates of ionizing radiation. Clin Spine Surg. 2016;29(2):52-9. Likewise, longer surgical times have been reported for MI, at least during the first cases, which could be a reflection of technical differences, but some authors associate this with a significant learning curve.12-1812. Silva PS, Pereira P, Monteiro P, Silva PA, Vaz R. Learning curve and complications of minimally invasive transforaminal lumbar interbody fusion. Neurosurg Focus. 2013;35(2):E7.
The objective of this study was to present and analyze the single level MI-TLIF learning curve for a single neurosurgeon (JASS). To this end, we evaluated various parameters, such as surgical time, amount of bleeding, and days of hospitalization.
METHODS
This was a retrospective study that included all patients who underwent single level MI-TLIF at a single institution and by the same neurosurgeon (JASS), during the time period from September 2005 through August 2014. We conducted a retrospective review of all the clinical files in order to report and evaluate surgical time, transoperative bleeding, and hospitalization time. It is important to mention that all the procedures were performed after the proper signing of the informed consent form and the study was duly accepted by the institutional review board of the medical center where it was conducted.
The data evaluated was described in terms of percentages or ratios, arithmetic averages with standard deviation, or medians and interquartile ranges (IQR) when appropriate. The learning curve for each surgical variable was extracted via piecewise regression analysis in order to determine the inflection point of the curve. Statistical analysis was conducted using the SigmaPlot Statistical Software (version 12.3) and the Stata program (Stata Corporation, College Station, TX, USA).
The surgical procedure was performed following the previously published congenital technique described for MI-TLIF.1919. Quillo-Olvera J, Soriano-Solis S, Ortiz-Leyva RU, Gutiérrez-Partida CF, Rodríguez-García M, Soriano-Sánchez JA. Microsurgical landmarks in minimally invasive transforaminal lumbar interbody fusion. Coluna/Columna. 2015;14(4):317-9. Based on radiological planning, an incision of approximately 2.5 cm was made, and the 20 mm tubular retractor (METRx®, Medtronic, USA) was placed in the sulcus between the longissimus and illiocostalis muscles. The lateral facet joint and the anatomical landmarks were thus identified. The lateral facet was milled, always maintaining the approach within the Kambin triangle, and the radical discectomy and preparation of the superior and inferior terminal plates were performed, and then, after the placement of bone chips and morphogenetic bone protein (OMC®, Bioteck, Italy), the bullet-tip interbody cage was put in place (Forza®, Orthofix, USA). Subsequently, a review was conducted under microscopic vision to resect disc segments that might have protruded. Then, the cannulated transpedicle screws were put in place, guided by imaging, through the incision already used in the tubular approach.
RESULTS
This study included 99 patients with an average age at the time of surgery of 54.6 years ± 13.9 (range 21 - 84 years), during the time period discussed in the Methods section, comprising 41 men (41%) and 58 women (59%). (Table 1) The indications for MI-TLIF included degenerative spondylolisthesis, degenerative disc disease, (Figure 1) adjacent disc disease, and segmental instability. There is a clear tendency towards an increase in the annual number of surgical procedures, starting with one case in the first year and reaching 19 procedures in the last two years, with more than 50 procedures performed in the last three years. (Figure 2) It should be noted that during the fifth and sixth years there was a decrease in the number of cases because of less availability of the surgical material due to official regulations in Mexico.
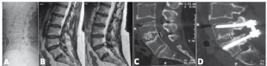
Illustrative case of a patient with degenerative L4-L5 disc disease who underwent MI-TLIF at one level (L4-L5). Preoperative radiography (A). Preoperative T2 Magnetic resonance of the lumbar spine (B) showing L4-L5 radicular compression. In the 1-year postoperative tomography fusion in the midline (C) and proper placement of the screws and rods (D) can be observed.

We recorded a median surgical time of 203.3 minutes (IQR 150 - 240 min), (Figure 3), median transoperative bleeding of 97.4 mL (IQR 40 - 1000 mL) (Figure 4), and a median in-hospital stay of four days (IQR 3 - 5 days). (Figure 5)



The learning curves with respect to surgical time and transoperative bleeding showed a progressive decrease in both variables as the number of consecutively operated procedures increased, until a point of inflection was reached in each curve marking the proportion of cases corresponding to the initial experience with MI-TLIF and the patients in whom the procedure was performed with sufficient experience to keep the surgical time and the quantity of bleeding constant. In Figure 6, we can see the learning curve for surgical time and identify the inflection point as occurring in case 43. Similarly, in Figure 7, we can see the learning curve for transoperative bleeding, with the inflection point identified in case 48.

Learning curve of patients submitted to MI-TLIF (n=99) by surgical time. Inflection point in patient number 43

Learning curve of patients submitted to MI-TLIF (n=99) by transoperative bleeding. Inflection point in patient number 48
DISCUSSION
MI spine surgery techniques have been gaining increasingly better diffusion and acceptance, since the benefits offered by this type of technique as compared with open procedures have been reported with greater frequency. Among the advantages reported are less intense postoperative pain, less surgical trauma to the paravertebral musculature and adjacent neural tissues, as well as shorter recovery times.4-99. Wu RH, Fraser JF, Härtl R. Minimal access versus open transforaminal lumbar interbody fusion: meta-analysis of fusion rates. Spine (Phila Pa 1976). 2010;35(26):2273-81. However, despite the advantages cited, there are several disadvantages that must be taken into account. One of the principle disadvantages is the learning curve that this type of procedure requires to be able to perform them safely and with results comparable to the literature. This is one factor that has led many spine surgeons not to be attracted to make the change from classical open procedures, which have good outcomes and few complications, to the new MI techniques. Another disadvantage that has been reported is the elevated cost incurred at the beginning of the implementation of MI procedures due to the materials and teams required to execute them. However, there have already been reports in the literature showing that, in the long run, the costs are similar or even lower than in open procedures, since shorter hospitalization and recovery times permit earlier reintegration to daily life, among other factors. Economic savings, both direct and indirect, of up to 49% as compared to open procedures have been reported.7,127. Goldstein CL, Phillips FM, Rampersaud YR. Comparative effectiveness and economic evaluations of open versus minimally invasive posterior or transforaminal lumbar interbody fusion: a systematic review. Spine (Phila Pa 1976). 2016;41 Suppl 8:S74-89.
As previously mentioned, to date there is no ideal statistical method to assess learning in medicine and in surgical procedures in particular. For this reason, there are several calculations that have been adapted to this end. In this case, we chose piecewise type curves for the calculation of the learning curve, in which the form of the curve corresponds to an exponential regression model where the curve drops dramatically at the onset and, as the cases advance consecutively, approaches an asymptote. The piecewise model allows us to obtain a more accurate inflection point, both statistically and visually, so it proved to be the best model for the planned objective. Using this type of curve, we see that the asymptote was reached in case 43 of this series for surgical time and in case 48 for transoperative bleeding. The median surgical time was 203.3 minutes and the median transoperative bleeding was 97.4 mL. This information reflects the number of cases that were necessary to reach the point where the surgeon managed to complete his learning curve. The data presented are in agreement with previous publications in which surgical time range from 104 to 389.7 minutes are reported and the learning curves are reached around case 40.12,2012. Silva PS, Pereira P, Monteiro P, Silva PA, Vaz R. Learning curve and complications of minimally invasive transforaminal lumbar interbody fusion. Neurosurg Focus. 2013;35(2):E7.
CONCLUSIONS
As observed in this article, MI-TLIF is a safe and effective technique for achieving lumbar arthrodesis with results comparable to those of open techniques. As evidenced in the previously published literature, as well and in this article, it is important to take the learning curve necessary for this technique into account, which can be reached after about 45 days.
REFERENCES
-
1Hopper AN, Jamison MH, Lewis WG. Learning curves in surgical practice. Postgraduate Medical Journal. 2007;83(986):777-9.
- 2. Aoun SG, Bendok BR, Mocoo JD, Levy EI. Simulation in vascular neurosurgery. Congress Quartertly: The Future of Neurosurgical Education. 2011;12(3):9-11. Disponível em: https://www.cns.org/system/files/congress_quarterly/CNSQ_11summer_0.pdf
-
3Zhang Q, Yuan Z, Zhou M, Liu H, Xu Y, Ren Y. A comparison of posterior lumbar interbody fusion and transforaminal lumbar interbody fusion: a literature review and meta-analysis. BMC Musculoskelet Disord. 2014;15:367.
-
4Schizas C, Tzinieris N, Tsiridis E, Kosmopoulos V. Minimally invasive versus open transforaminal lumbar interbody fusion: evaluating initial experience. Int Orthop. 2009;33(6):1683-8.
-
5Lin Y, Chen W, Chen A, Li F. Comparison between minimally invasive and open transforaminal lumbar interbody fusion: a meta-analysis of clinical results and safety outcomes. J Neurol Surg A Cent Eur Neurosurg. 2016;77(1):2-10.
-
6Guan J, Bisson EF, Dailey AT, Hood RS, Schmidt MH. Comparison of clinical outcomes in the national neurosurgery quality and outcomes database for open versus minimally invasive transforaminal lumbar interbody fusion. Spine (Phila Pa 1976). 2016;41(7):E416-21.
-
7Goldstein CL, Phillips FM, Rampersaud YR. Comparative effectiveness and economic evaluations of open versus minimally invasive posterior or transforaminal lumbar interbody fusion: a systematic review. Spine (Phila Pa 1976). 2016;41 Suppl 8:S74-89.
-
8Seng C, Siddiqui MA, Wong KP, Zhang K, Yeo W, Tan SB, et al. Five-year outcomes of minimally invasive versus open transforaminal lumbar interbody fusion: a matched-pair comparison study. Spine (Phila Pa 1976). 2013;38(23):2049-55.
-
9Wu RH, Fraser JF, Härtl R. Minimal access versus open transforaminal lumbar interbody fusion: meta-analysis of fusion rates. Spine (Phila Pa 1976). 2010;35(26):2273-81.
-
10Wong AP, Smith ZA, Stadler JA 3rd, Hu XY, Yan JZ, Li XF, et al. Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF): surgical technique, long-term 4-year prospective outcomes, and complications compared with an open TLIF cohort. Neurosurg Clin N Am. 2014;25(2):279-304.
-
11Kim CH, Lee CH, Kim KP. How high are radiation-related risks in minimally invasive transforaminal lumbar interbody fusion compared with traditional open surgery?: a meta-analysis and dose estimates of ionizing radiation. Clin Spine Surg. 2016;29(2):52-9.
-
12Silva PS, Pereira P, Monteiro P, Silva PA, Vaz R. Learning curve and complications of minimally invasive transforaminal lumbar interbody fusion. Neurosurg Focus. 2013;35(2):E7.
-
13Nandyala SV, Fineberg SJ, Pelton M, Singh K. Minimally invasive transforaminal lumbar interbody fusion: one surgeon's learning curve. Spine J. 2014;14(8):1460-5.
-
14Ryang YM, Villard J, Obermüller T, Friedrich B, Wolf P, Gempt J, et al. Learning curve of 3D fluoroscopy image-guided pedicle screw placement in the thoracolumbar spine. Spine J. 2015;15(3):467-76.
-
15Wang B, Lü G, Patel AA, Ren P, Cheng I. An evaluation of the learning curve for a complex surgical technique: the full endoscopic interlaminar approach for lumbar disc herniations. Spine J. 2011;11(2):122-30.
-
16Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, et al. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013;115(10):1987-91.
-
17Park Y, Lee SB, Seok SO, Jo BW, Ha JW. Perioperative surgical complications and learning curve associated with minimally invasive transforaminal lumbar interbody fusion: a single-institute experience. Clin Orthop Surg. 2015;7(1):91-6.
-
18Ng CL, Pang BC, Medina PJ, Tan KA, Dahshaini S, Liu LZ. The learning curve of lateral access lumbar interbody fusion in an Asian population: a prospective study. Eur Spine J. 2015;24 Suppl 3:361-8.
-
19Quillo-Olvera J, Soriano-Solis S, Ortiz-Leyva RU, Gutiérrez-Partida CF, Rodríguez-García M, Soriano-Sánchez JA. Microsurgical landmarks in minimally invasive transforaminal lumbar interbody fusion. Coluna/Columna. 2015;14(4):317-9.
-
20Tian NF, Wu YS, Zhang XL, Xu HZ, Chi YL, Mao FM. Minimally invasive versus open transforaminal lumbar interbody fusion: a meta-analysis based on the current evidence. Eur Spine J. 2013;22(8):1741-9.
-
2
Study conducted at the Centro Médico ABC, Santa Fe, Cuajimalpa, Ciudad de México.
-
CONTRIBUTION OF THE AUTHORS:
Each author made significant individual contributions to this manuscript. SRF (ORCID: 0000-0001-8089- 6684) coordinated, wrote, and reviewed the article. JASS is the surgeon who performed the surgical procedures and was responsible for the final approval of the manuscript. SSS, JCZR, CFGP, MRG, and HASS all contributed equally to the review, retrospective analysis, and collection of the data.
Publication Dates
-
Publication in this collection
Oct-Dec 2017
History
-
Received
29 June 2017 -
Accepted
04 Aug 2017







