Abstracts
INTRODUCTION:
Language acquisition and development require an understanding of physical and psychosocial aspects during diagnosis and treatment. At this point, a partnership between phoniatric physicians and other health professionals is often a determinant for favorable prognosis.
OBJECTIVE:
To identify the clinical and epidemiological characteristics of a pediatric population attending a phoniatric clinical practice.
METHODS:
Study design: Cross-sectional cohort. Retrospective, epidemiological study of 297 children, seen in phoniatric appointments between 1976 and 2005. Outcome variables were referral origin, gender, age, mean age, diagnosis, and treatment approach.
RESULTS:
66% were male and 34% were female, with a mean age of 6.4 years. The largest number of referrals for phoniatric treatments came from speech therapists (38%). The predominant complaint was alteration in speech (35%); the diagnostics in speech, language, and fluency (49.5%) are noteworthy. Considering the total of the patients analyzed, 28.2% were referred for speech therapy and 11.8% for psychotherapy.
CONCLUSION:
The studied population is predominantly male, the diagnosis points to a higher incidence in cases of impairment in speech, language, and fluency; the most common treatment was speech therapy.
Child language; Language development; Speech disorders; Epidemiology
INTRODUÇÃO:
Aquisição e desenvolvimento da linguagem demandam cuidados exigindo compreensão dos aspectos orgânicos e psíquicos no diagnóstico e tratamento. Assim, parceria entre foniatra e outros profissionais é, muitas vezes, determinante de um prognóstico favorável.
OBJETIVO:
Caracterizar clínica e epidemiologicamente os distúrbios de comunicação em crianças na prática clínica.
MÉTODO:
Coorte transversal histórica. Estudo epidemiológico retrospectivo de 297 prontuários de crianças atendidas em consulta foniátrica no período entre 1976 a 2005. Variáveis: origem do encaminhamento, gênero, média da idade, diagnóstico e conduta para tratamento.
RESULTADOS:
66% foram do gênero masculino e 34% do feminino com média de idade de 6,4 anos. Maior número de encaminhamentos foi realizado por fonoaudiólogos (38%). A queixa predominante era de alterações na fala 35% e ressaltam-se os diagnósticos na área da fala, linguagem e fluência (49,5%). Do total destacaram-se os encaminhamentos para: 28,2% fonoterapia e 11,8% psicoterapia.
CONCLUSÃO:
A população atendida foi predominantemente masculina, o diagnóstico aponta maior incidência em quadros de comprometimento na fala, linguagem e fluência e o tratamento mais indicado foi fonoterapia.
Linguagem infantil; Desenvolvimento da linguagem; Distúrbios da fala; Epidemiologia
Introduction
For the establishment of proper diagnosis and appropriate treatment, children with language disorders require the services of a coordinated medical and phoniatric team capable of considering that organic, psychological, and social factors can be part of the genesis of this problem.11 Union Europeenne des medecins specialists (UEMS/Union of the European Phoniatricians (UEP). Training logbook of phoniatrics. Versao October 1st, 2010. Available from: http://www.orluems.com/gestor/upload/file/7%20Logbook%20Phoniatrics [accessed 31.01.13].
http://www.orluems.com/gestor/upload/fil...
Even in cases where there is an obvious functional abnormality of an organ or system, e.g., in cases of hearing loss, cleft palate, and encephalopathy, it is critical to understand that the problems that arise in patients with communication difficulties are complex and sometimes difficult to understand. Affected children and their families, when seeking help for communication difficulties look for clinical responses that appreciate the biopsychic foundations of their language disorder.22 Spinelli M. O diagnóstico foniátrico nos transtornos da lin guagem. Distúrbios Comun, Sao Paulo. 2003;15:143-9.
The otorhinolaryngologist involved in phoniatrics plays a key role in this complex process of human communication, not only at the time of diagnosis, but also during his/her communication with the team helping to formulate the best conduct and the most appropriate intervention for each patient.33 Tabith A Jr. Distúrbios do desenvolvimento da linguagem: aspec- tos foniátricos. Fórum: INES, Rio de Janeiro. 2005;12:16-27.
Similarly, due to the large number of potential diagnoses for a child with a language disorder - for example, specific language impairment, language delay, and articulation disorders, we believe that epidemiological studies are useful to help in selecting the composition of the team necessary to care for these children. In this sense, the aim of this study was to epidemiologically characterize the practice and the referrals made to a phoniatric clinic for communication disorders occurring in childhood
Methods
The study design was approved by the Ethics Committee of Pontifícia Universidade Católica de São Paulo, according to Declaration no. 06919712.6.0000.5482.
A retrospective study of a historical cross-sectional cohort was conducted. From a total of 843 patients with complaints of a disorder of communication submitted to phoniatric assessment and treatment in a private clinic in the city of São Paulo between June of 1976 and January of 2005 half, were analyzed (those registered with an even number). From these medical records, only children of both genders of between ages 1 year and 11 years and 11 months were included, totaling 422 records.
Exclusion criteria: incomplete or illegible records
During the phoniatric consultation, one semi-open interview took place, where data were collected on the complaint, previous history of the complaint, family history, schooling, family routine, feeding habits, neuropsychomotor development, and social and family relationships.
In addition to an otorhinolaryngological examination, the phoniatrist used games and symbolic play, drawing, and writing (depending on the child's age) to investigate aspects related to global and oral motor functions, auditory and visual perceptual functions, static and dynamic balance, and spatial orientation at body and graphic levels. The examinations provided by the child's parents during the consultation were also considered, and the physician ordered other appropriate tests to complement the data for evaluation.
For the analysis, the following variables were used: gender, mean age, referral source, family complaint, diagnosis, and conduct.
The statistical analysis was performed using an ANOVA parametric test (quantitative and continuous data) and the equality of two proportions nonparametric test (qualitative data). A significance level of p = 0.05 (5%) with a 95% confidence interval was established. 44 Vieira S. Bio Estatistica Tópicos Avançados. 2nd ed. Rio de Janeiro: Ed. Campus; 2004.
Results
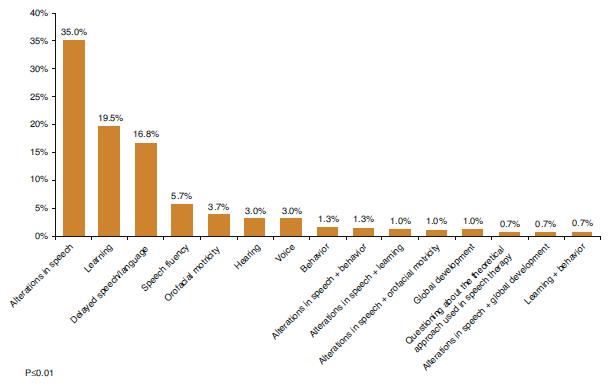
Of 422 medical records, 22 were excluded for incompleteness and 103 for being outside the stipulated age. Thus, 297 medical records were evaluated. Of this sample, most children were male (n = 196; 66%) compared to females (n = 101; 34%; p < 0.001) and the mean age was 6.3 ± 0.3 years. Most of the patients came from the city of São Paulo, i.e., 65.32% of cases (p < 0.01%). Most referrals to phoniatric consultation were made by speech therapists, 38% ( Fig. 1). The main family complaint was a change in speech (p ≤ 0.01; Fig. 2), and the most frequent diagnosis was established in the speech/language/fluency area (49.5%; p ≤ 0.01; Fig. 3).
according to main disorders found. * Speech/language/fluency - language deviations, language deviations delay, speech disorders, specific language disorder, dyspraxia, and disfluency. ** Articulation disorders, alterations in chewing, swallowing, and respiration, sigmatism, malocclusion, and tone deficit of OFA (O.M. = oral motricity). *** Inhibition, clinical pictures of psychosis, autism, psychic imbalance, and depression.
In the analysis of the gender and diagnostic variables, no statistically significant differences were found between the two genders with respect to "hearing," "neurological picture," and "voice" diagnoses (and also in "no diagnosis" cases). A statistically significant difference was found in those diagnoses related to speech/language/fluency areas, with a prevalence of 63.9% in boys and 36.1% in girls (p < 0.001) ( Table 1).
The phoniatric diagnosis was analyzed considering three age groups, distributed as follows: 0-5 years, >5 and ≤10 years, and >10 years. In the first two age groups, speech/language/fluency was the most common diagnosis. However, in the group of children over 10 years of age, the most frequent diagnosis was established in the reading/writing/learning area, with 33.3%, but there was no statistical difference vs. the diagnoses established for speech/language/fluency and emotional disturbance (30.3% and 15.2%, respectively; Table 2).
The phoniatrist returned 46.7% of these patients to the professionals responsible for the patient's referral: 28.2% for speech therapy, 11.8% for psychotherapy, and 3% for educational psychology, as shown in Fig. 4. The remaining patients (10.3%) were to return to the phoniatrist for monitoring.
Discussion
Phoniatrics is an area of otorhinolaryngology which treats human communication disorders, focusing on voice, speech, language, hearing, and swallowing functions.11 Union Europeenne des medecins specialists (UEMS/Union of the European Phoniatricians (UEP). Training logbook of phoniatrics. Versao October 1st, 2010. Available from: http://www.orluems.com/gestor/upload/file/7%20Logbook%20Phoniatrics [accessed 31.01.13].
http://www.orluems.com/gestor/upload/fil...
As a function of the complexity of the process of human communication and of the enormous range of possible diagnoses, it is believed that the success of the treatment for communication disorders in childhood is intimately linked to an interdisciplinary strategy and to an effective interlocution among the team members.
The analysis of the population represented by the 297 successfully evaluated medical records reflects the findings in the literature. A significant majority of families seeking speech therapy services bring their boys to the medical appointment with a complaint of speech disorder (Fig. 2).55 Lima BPS, Guimaraes JATI, Rocha MCG. Caracteristicas epidemiológicas das alterações de linguagem em um centro fonoaudiológico do primeiro setor. Rev Soc Bras Fonoaudiol. 2008;13:376-80. However, when analyzing the phoniatric diagnosis (divided into broad areas, as a result of statistical adjustments), it can be noted that male gender represents a significant majority of alterations both in the speech/language/fluency area, the most frequent diagnosis group (Fig. 3) that includes language deviations, delays in language acquisition, speech disorders, specific language disturbance, dyspraxias, and dysfluency, as well as in the reading and writing alterations, oral motricity problems, emotional disorders, and otorhinolaryngological disorders (Table 1). This could be explained by hormonal issues in boys and their slower neurological maturity, and, according to some studies, also by the social demands that are incurred in these children, when, by cultural imposition, they are called upon to speak correctly. There are several explanations for the male predominance in the literature, but there is no definitive consensus.66 Choudhury N, Benasich AA. A family aggregation study: the influence of family history and other risk factors on language development. J Speech Lang Hear Res. 2003;46:261-72. , 77 Fávero ML, Higino TC, Pires AP, Burke PR, Silva FL, Tabith Júnior A. Pediatric phoniatry outpatient ward: clinical and epidemiological characteristics. Braz J Otorhinolaryngol. 2013;79:1-5. and 88 Spinelli M, Tabith A. Distúrbios Especifico de linguagem aspectos conceituais, fundamentos biológicos e dados clinicos. In: Massari IC, Spinelli M, Goro A, Sollero DC, Penido JCA, editors. Quando a inteligência nao encontra palavras - Distúrbio Especifico de Linguagem. Sao Paulo: LCTE; 2014. p. 13-23.
The age of children at the time of the phoniatric assessment was around 6 years, with a mean age of 6.4 ± 0.4 years, which may coincide with their entrance into elementary school. In this context, the child is inserted into the social group, interacting with peers and teachers; thus, there is a greater demand for communication, and this may highlight the existing differences in the group,99 Bergès JB. Porque cinco vezes mais meninos nao aprendem? In: Bergès J, Bergès-Bounes M, Calmettes-Jaean S, editors. O que aprendemos com crianças que nao aprendem? Porto Alegre: CMC Ed.; 2008. p. 69-72. and 1010 Vygotsky L. SA pré-história da linguagem escrita. In: A formaçao social da mente. Sao Paulo: Martins Fontes; 1984. p. 117-34. stimulating the child's referral and the search for a phoniatric evaluation.
However, in many cases - and depending on the severity of this delay - seeking specialized care and/or a phoniatric diagnosis only when the child reaches 6 years of age may have negative developmental consequences since good communication is essential for physical and mental development While 60% of children with language delay at the age of 2 years achieve language development similar to that of their normal peers in 12 months without treatment, the persistence of their symptoms brings adverse effects on learning, behavior, social skills, and mental health in adulthood; therefore, they should not be overlooked.1111 Boyle J. Speech and language delays in preschool children. BMJ. 2011:343 [Editorials].
It must also be considered that at the age of 6, the child begins to learn how to read and write, both necessary for developing literacy. A child who has not consolidated oral language may have lower chances of advancing in the written language at the same pace of other children, considering that part of oral skills are used in the writing process.1212 Nicolieto AP, Fernendes GB, Garcia VL, Hage SRV. Desempenho escolar de crianças com Distúrbio Especifico de Linguagem: relações com habilidades metafonológicas e memória de curto prazo. Rev Bras Fonoaudiol. 2008;13:246-50.
Table 2 documents how speech and language delays can be long-lasting throughout childhood; this is the most frequent diagnosis under 5 years of age and between 5 and 10 years of age, and is almost as common as the reading/writing/learning alterations in children over 10 years.
We believe that an interdisciplinary approach in the phoniatrics clinic is critical to a good prognosis for communication disorders. Fig. 4 presents a good example of the interdisciplinary nature and, especially, of the composition of the team, since most of the patients returned to their original care providers at the conclusion of their phoniatric assessment, to proceed with the treatment.
In the formation of this team, a partnership between the phoniatrist and the speech therapist is of fundamental importance, whether in the treatment of clinically complex cases, in longitudinal follow-up pursuing a diagnosis, or interpreting specific data stemming from the language assessment.
The speech therapist stands out as the professional who often directs patients to phoniatric evaluation (Fig. 1); furthermore, he/she is the professional who receives the greatest number of indications of patients based on the phoniatrist's clinical conduct (Fig. 4). It must be emphasized that well-coordinated work between these specialties - phonoaudiology and phoniatrics - can contribute to greater efficacy in the treatment of children with speech and language disorders.1313 Spinelli M. Distúrbios no Desenvolvimento da Linguagem. In: Assumpçao FB Jr, editor. Psiquiatria da Infância e da Adolescência. Sao Paulo: Santos; 1994. p. 171-9. and 1414 Jerusalinsky A, Coriat E. Aspectos estruturais e instrumentos do desenvolvimento infantil. Escritos da criança, vol. 4. Porto Alegre: Centro Lydia Coriat; 1996.
The importance of the psychologist as a member of the interdisciplinary team for treating communication disorders is worth mentioning. In this series, 11.8% of patients were referred by the speech specialist for a psychological evaluation (Fig. 4). Considering that psychological disorders and suffering are directly related to language problems,1515 Gupta AR, State MW. Autism: genetics. Rev Bras Psiquiatr. 2006;28:S29-38. , 1616 Spinelli M. Distúrbios Severos de Linguagem na criança. Termi nologia e aspectos clinicos. In: Paiva AF, Spinelli M, Vieira S, editors. Distúrbios de Comunicaçao: Estudos Interdisciplinares. Sao Paulo: Cortez; 1981. p. 15-31. and 1717 Spinelli M. Os problemas de comunicaçao na clinica dos distúr bios do desenvolvimento infantil. Estilo da Clinica, Instituto de Psicologia da USP; 1997, ano II, n.3: 21-9. and are frequently the primary cause of the delay, an intervention that considers the child's psychic and language constitution will provide more specific therapeutic results.
Conclusion
The population studied comprised predominantly males, and the diagnosis points to a higher occurrence of problems in the speech, language and fluency area. The most commonly recommended treatment was speech therapy.
References
-
1Union Europeenne des medecins specialists (UEMS/Union of the European Phoniatricians (UEP). Training logbook of phoniatrics. Versao October 1st, 2010. Available from: http://www.orluems.com/gestor/upload/file/7%20Logbook%20Phoniatrics [accessed 31.01.13].
» http://www.orluems.com/gestor/upload/file/7%20Logbook%20Phoniatrics -
2Spinelli M. O diagnóstico foniátrico nos transtornos da lin guagem. Distúrbios Comun, Sao Paulo. 2003;15:143-9.
-
3Tabith A Jr. Distúrbios do desenvolvimento da linguagem: aspec- tos foniátricos. Fórum: INES, Rio de Janeiro. 2005;12:16-27.
-
4Vieira S. Bio Estatistica Tópicos Avançados. 2nd ed. Rio de Janeiro: Ed. Campus; 2004.
-
5Lima BPS, Guimaraes JATI, Rocha MCG. Caracteristicas epidemiológicas das alterações de linguagem em um centro fonoaudiológico do primeiro setor. Rev Soc Bras Fonoaudiol. 2008;13:376-80.
-
6Choudhury N, Benasich AA. A family aggregation study: the influence of family history and other risk factors on language development. J Speech Lang Hear Res. 2003;46:261-72.
-
7Fávero ML, Higino TC, Pires AP, Burke PR, Silva FL, Tabith Júnior A. Pediatric phoniatry outpatient ward: clinical and epidemiological characteristics. Braz J Otorhinolaryngol. 2013;79:1-5.
-
8Spinelli M, Tabith A. Distúrbios Especifico de linguagem aspectos conceituais, fundamentos biológicos e dados clinicos. In: Massari IC, Spinelli M, Goro A, Sollero DC, Penido JCA, editors. Quando a inteligência nao encontra palavras - Distúrbio Especifico de Linguagem. Sao Paulo: LCTE; 2014. p. 13-23.
-
9Bergès JB. Porque cinco vezes mais meninos nao aprendem? In: Bergès J, Bergès-Bounes M, Calmettes-Jaean S, editors. O que aprendemos com crianças que nao aprendem? Porto Alegre: CMC Ed.; 2008. p. 69-72.
-
10Vygotsky L. SA pré-história da linguagem escrita. In: A formaçao social da mente. Sao Paulo: Martins Fontes; 1984. p. 117-34.
-
11Boyle J. Speech and language delays in preschool children. BMJ. 2011:343 [Editorials].
-
12Nicolieto AP, Fernendes GB, Garcia VL, Hage SRV. Desempenho escolar de crianças com Distúrbio Especifico de Linguagem: relações com habilidades metafonológicas e memória de curto prazo. Rev Bras Fonoaudiol. 2008;13:246-50.
-
13Spinelli M. Distúrbios no Desenvolvimento da Linguagem. In: Assumpçao FB Jr, editor. Psiquiatria da Infância e da Adolescência. Sao Paulo: Santos; 1994. p. 171-9.
-
14Jerusalinsky A, Coriat E. Aspectos estruturais e instrumentos do desenvolvimento infantil. Escritos da criança, vol. 4. Porto Alegre: Centro Lydia Coriat; 1996.
-
15Gupta AR, State MW. Autism: genetics. Rev Bras Psiquiatr. 2006;28:S29-38.
-
16Spinelli M. Distúrbios Severos de Linguagem na criança. Termi nologia e aspectos clinicos. In: Paiva AF, Spinelli M, Vieira S, editors. Distúrbios de Comunicaçao: Estudos Interdisciplinares. Sao Paulo: Cortez; 1981. p. 15-31.
-
17Spinelli M. Os problemas de comunicaçao na clinica dos distúr bios do desenvolvimento infantil. Estilo da Clinica, Instituto de Psicologia da USP; 1997, ano II, n.3: 21-9.
-
FundingThis study was supported by CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior).
-
☆
Please cite this article as: Baptista MGG, Caiuby Novaes BCA, Favero ML. Epidemiology of communication disorders in childhood phoniatric clinical practice. Braz J Otorhinolaryngol. 2015;81:368-73.
-
☆☆
Institution: Pontifícia Universidade de São Paulo (PUC-SP), São Paulo, SP, Brazil.
Publication Dates
-
Publication in this collection
Jul-Aug 2015
History
-
Received
16 Jan 2014 -
Accepted
06 Jan 2015