Introduction
Sialolithiasis is one of the most common diseases of the salivary glands. 11. Gupta A, Rattan D, Gupta R. Giant sialoliths of submandibular gland duct: report of two cases with unusual shape. Contemp Clin Dent. 2013;4:78-80.and22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4. It is a condition characterized by an obstructive phenomenon in a salivary gland or in its excretory duct due to a calculus. 11. Gupta A, Rattan D, Gupta R. Giant sialoliths of submandibular gland duct: report of two cases with unusual shape. Contemp Clin Dent. 2013;4:78-80. The clinical presentation is usually characterized by local swelling, pain, infection of the affected area, and dilation of the salivary duct. 11. Gupta A, Rattan D, Gupta R. Giant sialoliths of submandibular gland duct: report of two cases with unusual shape. Contemp Clin Dent. 2013;4:78-80. Sialolithiasis usually affects adults between the third and fourth decades of life, with a frequency of 12:1000. 33. Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3. The number of cases in male patients is about twice that of female patients. 33. Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3. It is estimated that 80-90% of cases occur in the submandibular gland, while 10-20% occur in the parotid gland. 33. Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3. The size of the calculi varies from <1 mm to a few centimeters. Although the frequency of sialolithiasis is relatively high, the occurrence of giant sialoliths, larger than 1.5 cm in any diameter, is rare. For this reason few studies are found in the pertinent medical literature. 11. Gupta A, Rattan D, Gupta R. Giant sialoliths of submandibular gland duct: report of two cases with unusual shape. Contemp Clin Dent. 2013;4:78-80.and44. Dalal S, Jain S, Agarwal S, Vyas N. Surgical management of an unusually large sialolith of Wharton's duct: a case report. King Saud Univ J Dent Sci. 2013;4:33-5.
This report describes a case of giant sialolith in a 42-years-old male, addressing the clinical features, the diagnosis, and the ductal repair surgery performed to restore salivary flow.
Case report
The patient, a 42-year-old black man, attended a dental appointment in March of 2014. After routine radiographic examination, he was referred for a consultation with an oral and maxillofacial surgeon, in April of 2014. During anamnesis the patient denied any previous diseases. He reported only an uneventful surgery on the right leg. The physical examination showed an ankyloglossia and, during palpation, a hardness in the right submandibular salivary gland. To further investigate the case, imaging exams were requested ( Fig. 1A ). A provisional diagnosis of sialolithiasis in the right submandibular gland duct was suggested.
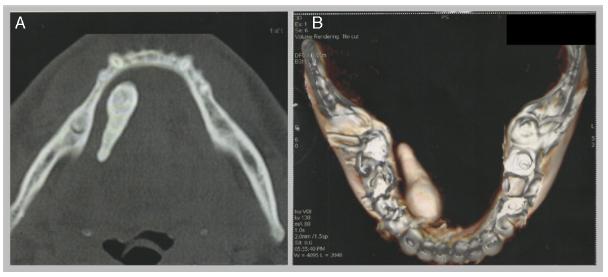
(A) Computed tomography scan (axial aspect) revealing a mineralized tissue with heterogeneous density and dimensions of 3.0 × 1.0 cm, approximately. (B) Three-dimensional image of the sialolith and the mandible.
Since the sialolith had exuberant dimensions, an excision followed by the reconstruction of the submandibular gland duct was proposed. Blood tests and surgical risk exams were requested for the patient.
On May 21, 2014, the surgical procedure was conducted by an intra-oral approach. The sialolith was removed by curettage after direct incision of the duct. A partial mineralization favored the fragmentation of the distal portion of the calculus. A true salivary gland cyst was removed in association with the calculus ( Fig. 2 ).
(A) The fragmented stone is seen on the left. On the right side, there is a tissue corresponding to the salivary cyst. (B) Histological section of the cyst showing oncocytic epithelium compatible with ductal epithelium (hematoxylin and eosin stain, 400×).
For the treatment of ankyloglossia, a tongue frenectomy was performed. To restore the salivary flow, a No. 8 urethral catheter was placed in the residual duct path. The mucosa was sutured around the catheter using a Vicryl 3-0 suture in order to repair the duct of the submandibular gland.
The other tissues were sutured in anatomical planes and there were no complications during the surgical procedure.
Two days after the surgery, an ultrasound showed that the catheter was inside the submandibular gland duct ( Fig. 3 ). After milking of the gland, the presence of crystalline liquid flowing from within the tube was noted ( Fig. 4 ). Eight days after the surgery, the patient reported an increase in salivary volume and the occurrence of contractions in the submandibular gland region.
The sutures and the drain were removed fourteen days after the surgery. A gland milking maneuver showed copious salivation, indicating that the performed surgical technique succeeded in reconstructing the ductal structure. The follow-up appointments within two months of the surgery showed no complications or complaints.
Discussion
Sialolithiasis is a disease that can affect any age group, with a higher prevalence in male adults. 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4.and55. Filho MAO, Almeida LE, Pereira JA. Sialolito gigante associado à fístula cutânea. Rev Cir Traumatol Buco-Maxilo-Fac. 2008;8:35-8. It mainly affects the submandibular gland. 66. Branco BLC, Cardoso AB, Caubi AF, Pena GN. Sialolitíase: relato de um caso. Rev Cir Traumatol Buco-Maxilo-Fac. 2003;3: 9-14. Despite being a common disease, the presence of giant calculus is extremely rare and most sialoliths do not exceed 1.5 cm. 33. Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3.and55. Filho MAO, Almeida LE, Pereira JA. Sialolito gigante associado à fístula cutânea. Rev Cir Traumatol Buco-Maxilo-Fac. 2008;8:35-8. The calculus in the present case had dimensions of approximately 3.0 cm × 1.0 cm, thus considered a giant sialolith. 11. Gupta A, Rattan D, Gupta R. Giant sialoliths of submandibular gland duct: report of two cases with unusual shape. Contemp Clin Dent. 2013;4:78-80.
The reported symptoms usually are pain and swelling in the gland, which worsen during the meal time ( Table 1 ). 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4.,33. Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3.,44. Dalal S, Jain S, Agarwal S, Vyas N. Surgical management of an unusually large sialolith of Wharton's duct: a case report. King Saud Univ J Dent Sci. 2013;4:33-5.,66. Branco BLC, Cardoso AB, Caubi AF, Pena GN. Sialolitíase: relato de um caso. Rev Cir Traumatol Buco-Maxilo-Fac. 2003;3: 9-14.and77. Cawson RA, Odell EW, Porter SR. Neoplastic and non-neoplastic diseases of salivary glands. In: Cawson's essentials of oral pathology and oral medicine. 7th ed. Edinburgh: Churchill Livingstone; 2002. p. 291-3. In the current report, the patient remained asymptomatic despite the exuberant dimensions of the stone.
According to Jensen 88. Jensen JL. Idiopathic diseases. In: Ellis GL, Auclair PL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: W.B. Saunders; 1991. p. 60-82. and Cawson et al., 77. Cawson RA, Odell EW, Porter SR. Neoplastic and non-neoplastic diseases of salivary glands. In: Cawson's essentials of oral pathology and oral medicine. 7th ed. Edinburgh: Churchill Livingstone; 2002. p. 291-3. salivary stones can be associated with the presence of true salivary gland cysts. Such lesions occur due to the obstruction of the salivary flow, followed by a proliferation of the duct epithelium that surrounds the stone. The present specimen presented a squamous and oncocytic differentiation in accord with the literature. 88. Jensen JL. Idiopathic diseases. In: Ellis GL, Auclair PL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: W.B. Saunders; 1991. p. 60-82.
The pathophysiology of the stone formation is still poorly understood. 33. Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3. However, it is believed that the sialolith is formed after the deposition of calcium salts around a "niche" of organic material. 77. Cawson RA, Odell EW, Porter SR. Neoplastic and non-neoplastic diseases of salivary glands. In: Cawson's essentials of oral pathology and oral medicine. 7th ed. Edinburgh: Churchill Livingstone; 2002. p. 291-3.
In 80% of cases the submandibular gland is affected 77. Cawson RA, Odell EW, Porter SR. Neoplastic and non-neoplastic diseases of salivary glands. In: Cawson's essentials of oral pathology and oral medicine. 7th ed. Edinburgh: Churchill Livingstone; 2002. p. 291-3. due to a number of synergistic factors, such as: (a) the composition of the saliva produced by the gland, which is more alkaline and with a major concentration of calcium 66. Branco BLC, Cardoso AB, Caubi AF, Pena GN. Sialolitíase: relato de um caso. Rev Cir Traumatol Buco-Maxilo-Fac. 2003;3: 9-14. ; (b) the salivary flow occurs against gravity 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4.and99. Krishnan B, Gehani RE, Shehumi MI. Submandibular giant sialoliths - 2 case reports and review of the literature. Indian J Otolaryngol Head Neck Surg. 2009;61:55-8. ; and (c) the long and tortuous anatomy of the duct of the submandibular gland. 66. Branco BLC, Cardoso AB, Caubi AF, Pena GN. Sialolitíase: relato de um caso. Rev Cir Traumatol Buco-Maxilo-Fac. 2003;3: 9-14.and99. Krishnan B, Gehani RE, Shehumi MI. Submandibular giant sialoliths - 2 case reports and review of the literature. Indian J Otolaryngol Head Neck Surg. 2009;61:55-8. All these factors work together in the formation of the calculus in the submandibular gland. 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4.,66. Branco BLC, Cardoso AB, Caubi AF, Pena GN. Sialolitíase: relato de um caso. Rev Cir Traumatol Buco-Maxilo-Fac. 2003;3: 9-14.and99. Krishnan B, Gehani RE, Shehumi MI. Submandibular giant sialoliths - 2 case reports and review of the literature. Indian J Otolaryngol Head Neck Surg. 2009;61:55-8. In the authors' opinion, the occurrence of the sialoliths presented in the consulted literature is in line with their understanding.
Regarding the treatment, a less invasive procedure is of utmost importance in order to preserve the gland's function. 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4.,44. Dalal S, Jain S, Agarwal S, Vyas N. Surgical management of an unusually large sialolith of Wharton's duct: a case report. King Saud Univ J Dent Sci. 2013;4:33-5.,77. Cawson RA, Odell EW, Porter SR. Neoplastic and non-neoplastic diseases of salivary glands. In: Cawson's essentials of oral pathology and oral medicine. 7th ed. Edinburgh: Churchill Livingstone; 2002. p. 291-3.and99. Krishnan B, Gehani RE, Shehumi MI. Submandibular giant sialoliths - 2 case reports and review of the literature. Indian J Otolaryngol Head Neck Surg. 2009;61:55-8. The pertinent literature indicated some surgical procedures such as trans-oral sialolithotomy, sialoendoscopy, extracorporeal shockwave lithotripsy, and resection of the gland. 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4.and33. Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3. For small sialoliths, conservative treatments using sialogogues and massage of the gland are also possible. 77. Cawson RA, Odell EW, Porter SR. Neoplastic and non-neoplastic diseases of salivary glands. In: Cawson's essentials of oral pathology and oral medicine. 7th ed. Edinburgh: Churchill Livingstone; 2002. p. 291-3. The current case showed the treatment of an exuberant calculus through an intra-oral approach associated with a ductal repair. Although Fowell et al. 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4. concluded that sialoplasty is one of the main treatments for giant sialoliths, this technique has not been described or used by the authors consulted. They performed the removal of the sialolith with closure by secondary intention.
Among the possible surgical complications, one is injury of the mandibular nerve, 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4. another is Wharton's duct stenosis. 22. Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4. There was no evidence of any of these complications in the present case. The ductal repair maintained salivary flow between the gland and the oral cavity.
The surgical removal of sialolith varies between surgeons. The preferred approach is mostly performed through intra-oral intervention ( Table 1 ).
Conclusion
The present case report described the removal of a giant sialolith. To the best of the authors' knowledge, this case is unique with regard to the surgical ductal repair after the excision of a salivary stone.
References
-
1Gupta A, Rattan D, Gupta R. Giant sialoliths of submandibular gland duct: report of two cases with unusual shape. Contemp Clin Dent. 2013;4:78-80.
-
2Fowell C, Macbean A. Giant salivary calculi of the submandibular gland. J Surg Case Rep. 2012;9:1-4.
-
3Iqbal A, Gupta AK, Natu SS, Gupta AK. Unusually large sialolith of Wharton's duct. Ann Maxillofac Surg. 2012;2:70-3.
-
4Dalal S, Jain S, Agarwal S, Vyas N. Surgical management of an unusually large sialolith of Wharton's duct: a case report. King Saud Univ J Dent Sci. 2013;4:33-5.
-
5Filho MAO, Almeida LE, Pereira JA. Sialolito gigante associado à fístula cutânea. Rev Cir Traumatol Buco-Maxilo-Fac. 2008;8:35-8.
-
6Branco BLC, Cardoso AB, Caubi AF, Pena GN. Sialolitíase: relato de um caso. Rev Cir Traumatol Buco-Maxilo-Fac. 2003;3: 9-14.
-
7Cawson RA, Odell EW, Porter SR. Neoplastic and non-neoplastic diseases of salivary glands. In: Cawson's essentials of oral pathology and oral medicine. 7th ed. Edinburgh: Churchill Livingstone; 2002. p. 291-3.
-
8Jensen JL. Idiopathic diseases. In: Ellis GL, Auclair PL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: W.B. Saunders; 1991. p. 60-82.
-
9Krishnan B, Gehani RE, Shehumi MI. Submandibular giant sialoliths - 2 case reports and review of the literature. Indian J Otolaryngol Head Neck Surg. 2009;61:55-8.
-
☆
Please cite this article as: Oliveira TP, Oliveira INF, Pinheiro ECP, Gomes RCF, Mainenti P. Giant sialolith of submandibular gland duct treated by excision and ductal repair: case report. Braz J Otorhinolaryngol. 2016;82:112-5.
-
☆☆
Institution: Faculdade de Medicina de Juiz de Fora, Universidade Presidente Antônio Carlos, Juiz de Fora, MG, Brazil.
Publication Dates
-
Publication in this collection
Jan-Fev 2016
History
-
Received
11 Mar 2015 -
Accepted
27 Mar 2015