Abstract
A model of an anthropometric record to be used in the Núcleos de Apoio à Saúde da Família (Centers for Family Health Support) in Brazil has been proposed in the literature, showing the logistics of use. The aim of this study was to discuss the anthropometric record, showing the potential and obstacles of its use. It was observed that, for adults, the screening measures (body mass index and waist circumference) for the determination of the risk of cardiovascular and metabolic diseases can be considered promising, although the Basic Health Care network already uses these measures. Nevertheless, the supplementary assessment (skinfold thickness and body circumferences) could be another potential possibility, except for the time spent to perform this assessment and the lack of studies of the cost-benefit of these anthropometric techniques. It was concluded that the anthropometric record proposed is an important instrument for improving the quality of the service provided to users of the Basic Health Care System; however, some adjustments, such as the removal of skinfold measurements as part of primary care, should be taken into consideration.
Key words:
Anthropometry; Physical activity; Primary health care
Resumo
Um modelo de ficha antropométrica foi proposto na literatura para ser usado no Núcleo de Apoio à Saúde da Família (NASF), apresentando a logística de utilização. O estudo objetivou discutir tal proposta, apresentando as potencialidades e os obstáculos no seu uso. Assim, pôde-se observar que, para adultos, a medida de triagem (Índice de Massa Corporal e o Perímetro da Cintura) para determinar o risco para desenvolvimento de doenças cardiovasculares e metabólicas pode ser considerado um potencial do estudo, entretanto, esta mensuração já ocorre na Atenção Básica à Saúde. Já a avaliação complementar (Dobras Cutâneas e Perímetros) seria outra potencialidade, se não fosse pelo tempo despendido pelo profissional em realizar esta avaliação e pela ausência de estudos sobre o custo-benefício dessas técnicas antropométricas. De tal modo, a ficha antropométrica proposta é um instrumento importante, de vanguarda, para melhorar a qualidade dos serviços prestados aos usuários do SUS, entretanto, alguns reajustes, como a retirada das dobras cutâneas na Atenção Primária, podem ser levados em consideração.
Palavras-chave:
Antropometria; Atenção primária à saúde; Atividade física
INTRODUCTION
Anthropometry is a set of procedures used both for the assessment of nutritional status and for the identification of cardiovascular and metabolic risk as a simple, low-cost, noninvasive method that provides easily obtained and immediately available results. However, although its accuracy has been extensively evaluated1Huxley R, Mendis S, Zheleznyakov E, Reddy S, Chan J. Body mass index, waist circumference and waist:hip ratio as predictors of cardiovascular risk - a review of the literature. Eur J Clin Nutr 2010;64(1):16-22., there is controversy in the literature regarding its specificity. For example, de Onis2Onis M. Measuring nutritional status in relation to mortality. Bull World Health Organ 2000;78(10):1271-4.reported the low specificity of this method as its main disadvantage.
Nevertheless, anthropometry has been widely used for individual evaluations throughout the life cycle or to determine health status in relation to the socioeconomic conditions of a population3Brasil, Ministério da Saúde. Sistema de vigilância alimentar e nutricional - Sisvan: orientações básicas para a coleta, processamento, análise de dados e informação em serviços de saúde. Brasília: Ministério da Saúde; 2004.,4de Onis M, Habicht JP. Anthropometric reference data for international use: recommendations from a World Health Organization Expert Committee. Am J Clin Nutr 1996;64(4):650-8..
On this basis, the Brazilian Health Ministry has indicated the use of the body mass index (BMI, for all age ranges) and waist circumference (WC, for adults) as anthropometric indicators to evaluate nutritional profile, to monitor child growth and development and, in the case of adults, to evaluate the risk of developing cardiovascular and metabolic diseases2Onis M. Measuring nutritional status in relation to mortality. Bull World Health Organ 2000;78(10):1271-4.,5Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Secretaria de Gestão Estratégica e Participativa. Vigitel Brasil 2010: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2011..
In Primary Health Care (PHC), the family health teams are responsible for the execution of these evaluations and for monitoring the nutritional profile of the subjects covered by the system on a day-to-day health care basis. Thus, when considering all actions and services that can be offered by PHC, and those that are effectively part of the routine of the professionals who work in Family Health Strategy (FHS), the Health Ministry created the "Núcleos de Apoio à Saúde da Família" (Centers for Family Health Support, NASF in the Portuguese acronym) in order to insert FHS in the health service network and to expand the actions of PHC (expansion and reinforcement of resolvability and of the processes of health territorialization and regionalization).
The NASF are staffed by multiprofessional teams that should be involved in the transformation of the activity and attitudes of family health professionals, including intersectorial and interdisciplinary actions for the promotion and rehabilitation of health and the achievement of a cure, and for the prevention of disease, as well as actions devoted to humanization of the services, continued education and the promotion of integrality.
This context has generated a demand for the formulation of proposals that will guide the intervention of physical education professionals in PHC in order to legitimize this discipline in the health field and to direct the actions of NASF professionals to the real health necessities of the population and to the requirements and characteristics of the Brazilian public health system. In this respect, Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.have proposed a model of an anthropometric record for the NASF and have demonstrated how the logistics of its application would be, since the inclusion of the anthropometric record will permit a more effective evaluation by the physical education professional regarding the detection of health risk factors and health education.
Within this context, the objective of the present study was to discuss the proposal of Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53., presenting its potential and the obstacles to be overcome so that the proposal can be effectively implemented.
The NASF and the role of physical education professionals
The NASF was created by an ordinance of the Health Ministry in order to support the activities performed by the FHS for regionalized and quality care in PHC throughout the national territory7Gomes MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir?. Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.. The Centers consist of three modalities according to the number of health teams involved, the number of health professionals hired, and the minimum workload of the staff as a whole and of each professional8Brasil. Ministério da Saúde. Portaria nº 154, de 24 de janeiro de 2008. Cria os Núcleos de Apoio à Saúde da Família - NASF. Available at: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2008/prt0154_24_01_2008.html> [2013 Dec 05].
http://bvsms.saude.gov.br/bvs/saudelegis...
.
Each modality can count on health professionals from various occupations depending on the interest of the region, such as a clinician, physical education professional, nutritionist, physiotherapist, psychologist, and social assistant9Brasil. Ministério da Saúde. Portaria nº 3.124, de 28 de dezembro de 2012. Redefine os parâmetros de vinculação dos Núcleos de Apoio à Saúde da Família (NASF) Modalidades 1 e 2 às Equipes Saúde da Família e/ou Equipes de Atenção Básica para populações específicas, cria a Modalidade NASF 3, e dá outras providências. Available at: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2012/prt3124_28_12_2012.html> [2013 Dec 05].
http://bvsms.saude.gov.br/bvs/saudelegis...
.
These professionals engage in various established strategies of action, among them physical activity, one of the areas of activity of physical education professionals. In this case, according to the directives of the NASF, physical education professionals should deal with elements of the culture of body movement, not only within the physiological area, but also considering aspects of sociology and psychology. On this basis, the body should be seen in its historical moment in a respected and singular manner in order to promote health and to prevent and treat the diseases that most affect the Brazilian population10Brasil. Ministério da Saúde. Portaria nº 256, de 11 de março de 2013. Estabelece novas regras para o cadastramento das equipes que farão parte dos Núcleos de Apoio à Saúde da Família (NASF) Sistema de Cadastro Nacional de Estabelecimentos de Saúde (SCNES). Available at: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2013/prt0256_11_03_2013.html [2014 Jan 16].
http://bvsms.saude.gov.br/bvs/saudelegis...
. From this viewpoint, the intention is to show to society that, beyond the well-known 30-minute walks without supervision, there are more effective forms of physical exercise for the improvement of health under the monitoring of a professional regarding intensity, duration and frequency. Thus, it is the task of physical education professionals to propose, in partnership, the construction of groups that will permit collective activities, popular and sports games, reasoning games, folk dances, and playful games, regardless of age range, gender or socioeconomic level.
It is clear that this a greater challenge than one may think since physical education professionals will have to deal with the treatment of chronic-degenerative diseases, increase the level of physical activity of the population in general, and also offer activities focusing on elements of the culture of body movement as a whole.
In view of this diversity of work in the NASF, the physical education professional will determine the effectiveness of the activity he is developing only by performing one evaluation. In this case, anthropometric evaluation is a method extensively used in the area of physical education to monitor the physical/physiological patterns before and after the activity of the professional. In view of the importance of such evaluation, Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.have proposed a model of an anthropometric record to be used by NASF professionals, and physical education teachers in particular.
Anthropometric record proposed by Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.: potential and obstacles
The proposal of the anthropometric record is to use an evaluation chart at two time points defined according to the site of evaluation (seeFigure 1). The first evaluation will be performed in the subject's residence by a Community Health Agent (CHA)6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.. This step is denoted by the authors as screening and its purpose is to define the profile of users of the Unified Health System (SUS in the Portuguese acronym) regarding the risk of development of cardiovascular and metabolic diseases. In this case, the CHA himself will be responsible for the measurement of weight and height for the calculation of BMI and for the measurement of WC. With this information, it will be possible to determine immediately the risk of the user associated with excess weight and fat distribution.
Logistics in NASF for anthropometric evaluation. Adapted from Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53..
The authors suggest that users with no associated risks be invited to participate in health education sessions in Basic Health Units (BHU). In contrast, users with associated risks will be referred to BHU where they will be submitted to a complementary anthropometric evaluation (second step of the anthropometric record) for which the authors propose the determination of skinfolds (subscapular, triceps, suprailiac, midaxillary, mid-thigh, mid-calf) and circumferences (arm, gluteus, thigh, calf). The purpose of this complementary evaluation is to perform a more efficient intervention regarding the necessities of the user.
In view of this logistics, an important potential is the anthropometric evaluation for screening, which is applied to the entire community covered by the FHS. However, two important obstacles arise regarding the complementary evaluation which deserve consideration: 1) time to be spent by the physical education professional to perform the complementary evaluations, and 2) absence of a cost-effectiveness study regarding the implementation of new anthropometric techniques in the SUS.
Regarding the first obstacle, we shall use a hypothetical example to clarify how much time will be necessary to perform the evaluations. Imagine a modality 1 NASF covering a total of 8 FHS, with each FHS covering 1000 families and each family consisting of approximately 3.5 adults, 28.7% of them being women11Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Diretrizes do NASF: Núcleo de Apoio a Saúde da Família. Brasília: Ministério da Saúde, 2010.. Part of these women will have a BMI above ≥ 30 kg/m2 together with a WC of more than 88 cm, a condition associated with a very high and an extremely high risk of developing cardiovascular and metabolic diseases12Instituto Brasileiro de Geografia e Estatística. Censo Demográfico. 2010. Available at: http://censo2010.ibge.gov.br/. [2014 Jan 16].
http://censo2010.ibge.gov.br/...
. Studies conducted on women from the city of São Leopoldo (RS) have shown that 17.4% had a BMI above ≥ 30 g/m213World Health Organization. Waist circumference and waist-hip ratio: report of a WHO expert consultation. Genebra: WHO; 2008.and 23.3% had a WC of more than 88 cm14Masson CR, Dias-da-Costa JS, Olinto MTA, da Costa CC, Bairros F, Hallal WC. Prevalência de sedentarismo nas mulheres adultas da cidade de São Leopoldo, Rio Grande do Sul, Brasil. Cad. Saúde Pública 2005;21(6):1685-94., leading to the conclusion that 4% of all women from São Leopoldo (RS) have conditions involving high and extremely high health risks.
If a physical education professional working 40 hours per week in a NASF evaluated the skinfolds and circumferences proposed by Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.in each woman in this 4% group, he would spend on average 4 minutes to explain the test and to mark the 8 anatomical points (4 skinfolds and 4 perimeters), plus 10 minutes to collect the data in duplicate. Thus, if this procedure were applied to all São Leopoldo women in the 4% group (about 333 women), the physical education professional would have to devote
44.47 hours of work to this activity. Considering a workload of 40 hours per week, the professional would need more than one week to conclude this evaluation, without taking into consideration the group of women in the remaining risk groups or the men, which would require additional time.
On this basis, it can be seen that the time spent to perform the complementary evaluations is very great, hampering the execution of the remaining activities established by the Directives of NASF10Brasil. Ministério da Saúde. Portaria nº 256, de 11 de março de 2013. Estabelece novas regras para o cadastramento das equipes que farão parte dos Núcleos de Apoio à Saúde da Família (NASF) Sistema de Cadastro Nacional de Estabelecimentos de Saúde (SCNES). Available at: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2013/prt0256_11_03_2013.html [2014 Jan 16].
http://bvsms.saude.gov.br/bvs/saudelegis...
for the physical education professional.
The second obstacle is the absence of studies in Brazil regarding the cost-effectiveness of health care in the NASF, specifically of anthropometric evaluations. In this case, before proposing the inclusion of a new anthropometric instrument in the SUS, two questions should be asked: Is it really necessary to implant two additional anthropometric evaluations (i.e., skinfolds and circumferences) if existing evaluations (BMI and WC) already determine the risk of users to develop cardiovascular and metabolic diseases? Would this inclusion be advantageous from a cost-effectiveness viewpoint?
The answer goes beyond the results of clinical and meta-analysis studies demonstrating that one technology is better than the other, i.e., in the case of anthropometry, that skinfold evaluation would be more effective than BMI and WC. This because it is also necessary to consider the cost-effectiveness (cost-utility) of the techniques15Olinto MTA, da Costa JSD, Kac G, Pattussi MP. Epidemiologia da obesidade abdominal em mulheres adultas residentes no sul do Brasil. Arch Latinoam Nutr 2007;57(4):349-56.. In this case, in addition to determining which choice would be more effective for the health of the Brazilian population, it is important to consider the difference in cost between the various techniques15Olinto MTA, da Costa JSD, Kac G, Pattussi MP. Epidemiologia da obesidade abdominal em mulheres adultas residentes no sul do Brasil. Arch Latinoam Nutr 2007;57(4):349-56.. On this basis, the equipment showing greater effectiveness and a lower cost would be adopted15Olinto MTA, da Costa JSD, Kac G, Pattussi MP. Epidemiologia da obesidade abdominal em mulheres adultas residentes no sul do Brasil. Arch Latinoam Nutr 2007;57(4):349-56.. In this respect, the ideal would be to carry out a study to determine whether the insertion of skinfolds and WC would actually have a greater cost-benefit than the measurement of BMI and WC. We may then conclude that this would be a new field of investigation in the area of anthropometry.
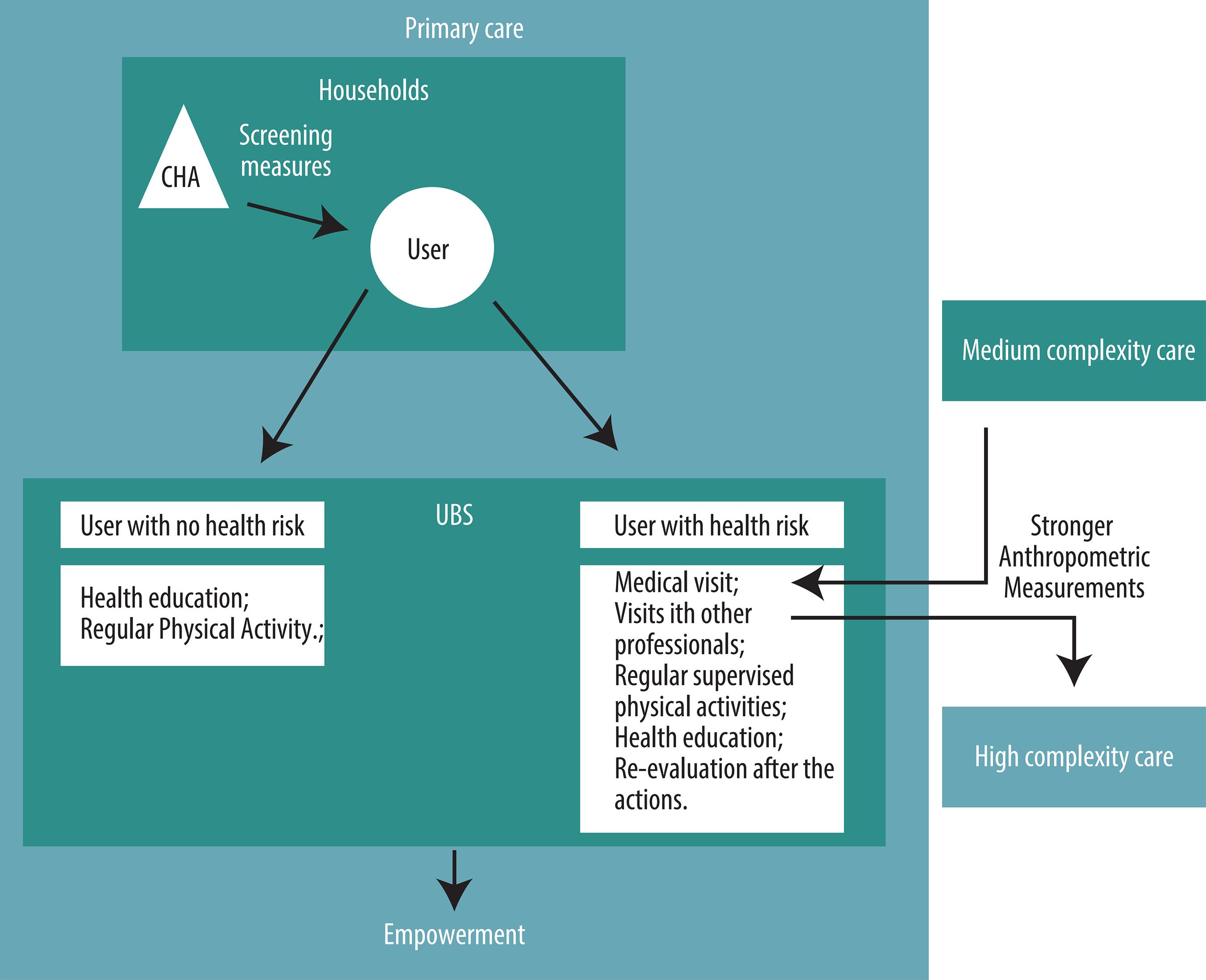
In view of the potential and difficulties described here regarding the proposal of Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.,Figure 2shows a new logistics for anthropometric evaluation in the NASF.
In this model, the screening measurements would be the same as those proposed byGomes et al. (2009)Gomes MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir?. Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53. 6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53., whereas the next step, regarding referral, would change.
In this respect, health education activities would be maintained for users showing no associated risks, with the addition of regular physical activities in order to promote health and to prevent disease, without overlooking the objective stated in the Directives of NASF10Brasil. Ministério da Saúde. Portaria nº 256, de 11 de março de 2013. Estabelece novas regras para o cadastramento das equipes que farão parte dos Núcleos de Apoio à Saúde da Família (NASF) Sistema de Cadastro Nacional de Estabelecimentos de Saúde (SCNES). Available at: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2013/prt0256_11_03_2013.html [2014 Jan 16].
http://bvsms.saude.gov.br/bvs/saudelegis...
, which is to offer to the community the elements of the culture of body movement.
In contrast, users showing associated risks would first be referred for a medical visit to the NASF, which would then make two different referrals: 1) to another level of care depending on the condition of the user (medium- or high-complexity care). The idea is that, at these other levels of care, more reliable anthropometric indicators would be adopted to identify health problems. It is in this phase that the following procedures would be included: skinfold measurements, densitometry and dual-energy X-ray absorptiometry, among others, depending on the resources available in the region. 2) Referral to the remaining professionals of NASF (e.g., physical education professional, nutritionist, psychologist) for the adoption of treatment measures such as regular physical activity monitored by the physical education professional. Health education activities would also be proposed for this group and, at the end of a given period of time established by NASF professionals, these users would be re-evaluated.
Finally, in this new proposal, the anthropometric evaluations determined in basic care for the determination of the risk to develop cardiovascular and metabolic diseases in adults would be only the BMI and WC, as is already the case in Brazil in the Food and Nutrition Surveillance System (SISVAN in the Portuguese acronym)2Onis M. Measuring nutritional status in relation to mortality. Bull World Health Organ 2000;78(10):1271-4.. The complementary evaluations suggested by Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.would then be performed at a higher level in the health care hierarchy.
FINAL CONSIDERATIONS
The intention of the present study was to establish a dialogue with the study of Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.in order to improve the quality of the services rendered to SUS users. The vanguard characteristic of the study by Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.should be highlighted, since their proposal led to the present reflection and will probably lead to future reflections, as proposed by this category of publication of the journal.
It should be pointed out that this discussion was motivated by some points that were not clear in the study by Gomes et al.6MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.. For example, if the objective is to screen for cardiovascular and metabolic risk, what is the need to measure skinfolds and circumferences and to calculate fat percentage? In addition to this doubt, the logistics for these evaluations and the cost-effectiveness analysis were additional points originating from the cited study.
The suggestion of adding skinfold measurements is a potential demonstrated in the proposal which, however, is limited by the time to be spent by the professional to perform this evaluation and by the absence of a cost-benefit study. Conversely, the proposal of BMI and WC determination, in addition to involving a low-cost method for determining the risk of developing cardiovascular and metabolic diseases, is an anthropometric technique already used in the SISVAN2Onis M. Measuring nutritional status in relation to mortality. Bull World Health Organ 2000;78(10):1271-4..
It should also be mentioned that the physical education professional will perform other activities in the PHC, such as offering specific physical exercises to hypertensive, obese and diabetic subjects, pregnant women, elderly subjects and others. Thus, although the need to create anthropometric protocols and parameters for professional activity within the context of Brazilian health is recognized, it is also necessary to determine the time devoted to this activity and its cost.
It has also been very clear that care should be taken with users who have a strong risk to develop cardiovascular and metabolic diseases. However, it should also be remembered that the family is the focus of basic care and as such it should act jointly in the entire process. Thus, participating in health education activities or even in regular physical activities may be a way for the family to incorporate the treatment of the member at risk and also to start a process of disease prevention or of health promotion.
Acknowledgments
The authors acknowledge the financial support of Fundação de Amparo à Pesquisa do Estado da Bahia (Fapesb), Coordenação de Aperfeiçoamento de Pessoa de Ensino Superior (Capes), and Universidade Estadual do Sudoeste da Bahia (fellowship program).
REFERENCES
- Huxley R, Mendis S, Zheleznyakov E, Reddy S, Chan J. Body mass index, waist circumference and waist:hip ratio as predictors of cardiovascular risk - a review of the literature. Eur J Clin Nutr 2010;64(1):16-22.
- Onis M. Measuring nutritional status in relation to mortality. Bull World Health Organ 2000;78(10):1271-4.
- Brasil, Ministério da Saúde. Sistema de vigilância alimentar e nutricional - Sisvan: orientações básicas para a coleta, processamento, análise de dados e informação em serviços de saúde. Brasília: Ministério da Saúde; 2004.
- de Onis M, Habicht JP. Anthropometric reference data for international use: recommendations from a World Health Organization Expert Committee. Am J Clin Nutr 1996;64(4):650-8.
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Secretaria de Gestão Estratégica e Participativa. Vigitel Brasil 2010: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2011.
- MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir? Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.
- Gomes MA, Beck CC, Duarte MFS, Petroski EL. Ficha antropométrica no Núcleo de Apoio a Saúde da Família: o que medir e para que medir?. Rev Bras Cineantropom Desempenho Hum 2009;11(2):243-53.
- Brasil. Ministério da Saúde. Portaria nº 154, de 24 de janeiro de 2008. Cria os Núcleos de Apoio à Saúde da Família - NASF. Available at: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2008/prt0154_24_01_2008.html> [2013 Dec 05].
» http://bvsms.saude.gov.br/bvs/saudelegis/gm/2008/prt0154_24_01_2008.html - Brasil. Ministério da Saúde. Portaria nº 3.124, de 28 de dezembro de 2012. Redefine os parâmetros de vinculação dos Núcleos de Apoio à Saúde da Família (NASF) Modalidades 1 e 2 às Equipes Saúde da Família e/ou Equipes de Atenção Básica para populações específicas, cria a Modalidade NASF 3, e dá outras providências. Available at: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2012/prt3124_28_12_2012.html> [2013 Dec 05].
» http://bvsms.saude.gov.br/bvs/saudelegis/gm/2012/prt3124_28_12_2012.html - Brasil. Ministério da Saúde. Portaria nº 256, de 11 de março de 2013. Estabelece novas regras para o cadastramento das equipes que farão parte dos Núcleos de Apoio à Saúde da Família (NASF) Sistema de Cadastro Nacional de Estabelecimentos de Saúde (SCNES). Available at: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2013/prt0256_11_03_2013.html [2014 Jan 16].
» http://bvsms.saude.gov.br/bvs/saudelegis/sas/2013/prt0256_11_03_2013.html - Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Diretrizes do NASF: Núcleo de Apoio a Saúde da Família. Brasília: Ministério da Saúde, 2010.
- Instituto Brasileiro de Geografia e Estatística. Censo Demográfico. 2010. Available at: http://censo2010.ibge.gov.br/. [2014 Jan 16].
» http://censo2010.ibge.gov.br/ - World Health Organization. Waist circumference and waist-hip ratio: report of a WHO expert consultation. Genebra: WHO; 2008.
- Masson CR, Dias-da-Costa JS, Olinto MTA, da Costa CC, Bairros F, Hallal WC. Prevalência de sedentarismo nas mulheres adultas da cidade de São Leopoldo, Rio Grande do Sul, Brasil. Cad. Saúde Pública 2005;21(6):1685-94.
- Olinto MTA, da Costa JSD, Kac G, Pattussi MP. Epidemiologia da obesidade abdominal em mulheres adultas residentes no sul do Brasil. Arch Latinoam Nutr 2007;57(4):349-56.
- Silva LK. Avaliação tecnológica e análise custo-efetividade em saúde: a incorporação de tecnologias e a produção de diretrizes clínicas para o SUS. Ciênc Saúde Colet 2003;8(2):501-520.
Publication Dates
-
Publication in this collection
Mar-Apr 2015
History
-
Received
29 Jan 2014 -
Accepted
22 July 2014