Abstract
A body schema is a cortical representation of the spatial relations of body parts. It can be evaluated using the Image Marking Procedure (IMP). However, that instrument lacks information regarding its reliability and a standardized set of procedures. The aim of this study was to test the repeatability and intra-rater reproducibility of an adapted IMP. Methods: It consisted of two steps: (1) adaptation of the instrument; (2) verification of its reliability. Sixty-five young adult women were evaluated on two different days by a single rater, with a one-week interval between evaluations. Three consecutive measurements were performed on each day. Regarding repeatability, for all the variables (coordinates, distances and area), the ICC scores were classified as excellent, with low SEM (<4.5cm) and MDC (<8.5cm) values. Regarding intra-rater reproducibility, only the variables area and distance between the trochanters presented ICC> 0.6. The adapted IMP needs to be conducted only once. Regarding reproducibility, the variables apt for use are the area within the points and the distance between the trochanters. In contrast to the original IMP test, in this adapted version we do not recommend the use of the distances between the shoulders, the hip/waist or the top of the head in relation to the ground.
Key words
Evaluation of research programs and tools; Perception; Reproducibility of results
Resumo
O esquema corporal é uma representação cortical das relações espaciais das partes do corpo que pode ser avaliado pelo Image Marking Procedure (IMP), o qual carece de informações acerca da confiabilidade, bem como dos procedimentos de padronização do teste. Objetivou-se testar a repetibilidade e reprodutibilidade intra-avaliador do teste IMP adaptado. Estudo desenvolvido em duas etapas: (1) adaptação do instrumento; (2) verificação da confiabilidade. Participaram do estudo 65 mulheres adultas jovens, avaliadas em dois dias, por um único avaliador, com intervalo de sete dias. Em cada dia foram realizadas três medições consecutivas. Resultados: Em relação à repetibilidade, para todas as variáveis analisadas (coordenadas, distâncias e área), os escores ICC foram classificados como excelentes, com valores baixos de SEM (<4,5cm) e MDC (<8,5cm). Na reprodutibilidade intra-avaliador apenas as variáveis área e distância entre trocânteres apresentaram ICC>0,6. O IMP adaptado é um instrumento que necessita uma única execução do teste. Com relação a reprodutibilidade, as variáveis possíveis de serem utilizadas são a área e distância entre trocânteres. Contrariamente ao que é utilizado no teste IMP original, nesta versão adaptada não recomendamos o uso das distâncias entre os ombros, cinturas e o topo da cabeça em relação ao chão.
Palavras-chave
Avaliação de programas e instrumentos de pesquisa; Percepção; Reprodutibilidade dos testes
INTRODUCTION
The perceived dimensions of the body or body schema is a cortical representation of the spatial relations between parts of the body, which depends on multi-modal sensorial afferences and their connections with the motor system11 Pereira ES, Segueto KJ, Thurm BE, Gama EF. Body schema analysis between yogaand body combat practitioners. FIEP Bulletin 2010:80(1):494-98.,22 Segheto W, Segheto KJ, Silva CB, Gama EF. Esquema corporal e nível de atividadefísica em adultos jovens universitários. Rev Bras Ciênc Mov 2011;19(3):29-36.. Those perceived dimensions are based on two components: (1) the sensorial, which refers to visual responses and the integration of tactile and kinesthetic information, and (2) the non-sensorial, formed from cerebral information, which is cognitive and affective in nature, reflecting the beliefs and knowledge held by the individual regarding their own body33 Cash TF, Pruzinsky T. Body image: a handbook of theory, research and clinical practice. New York: Guilford Press, 2003.,44 McCabe MP, Ricciardelli LA, Sitaram G, Mikail K. Accuracy of body size estimation: Role of biopsychosocial variables. Body Image 2006;3(2):163-71..
The Image Marking Procedure (IMP) is a test frequently used to evaluate the perceived dimension of the body, that is, the body schema55 Tavares MCGCF, Campana ANNB, Tavares Filho RF, Campana MB. Avaliaçãoperceptiva da imagem corporal: história, reconceituação e perspectivas para o Brasil. Psicol estud 2010;15(3):509-18.. It consists of a test in which blindfolded participants project the perceived location of body segments in relation to each other in response to tactile prompts (top of head, shoulders, waist, hip) on a sheet of paper fixed on the wall in front of them. It was developed in the 1970s to detect perceived distortions of body segments occasioned by eating disorders66 Askevold F. Measuring body image. Preliminary report on a new method. Psychother Psychosom 1975;26(2):71-77.. Currently, it is still used in clinical trials investigating eating disorders. However, its use has expanded to include the evaluation of healthy individuals and those with chronic pain, regardless of age77 Ferreira CC, Favero FM, Fontes SV, Quadros AAJ, Pereira SSR, Oliveira ASB, et al. Análise da imagem e esquema corporal em indivíduos com diagnóstico de síndrome pós-poliomielite. Revi Neuroc 2012;20(1):50-7.,88 Thurm EB, Matoso A, Diaz CA, Paschoalini C, Neves E, Tuunelis R, Kiyomoto HD, Gama EF. Chronic pain effect on body schema and neuropsychological performance in athletes: a pilot study. Percept Motor Skill 2013;116(2):544-53. or sedentary and active lifestyle88 Thurm EB, Matoso A, Diaz CA, Paschoalini C, Neves E, Tuunelis R, Kiyomoto HD, Gama EF. Chronic pain effect on body schema and neuropsychological performance in athletes: a pilot study. Percept Motor Skill 2013;116(2):544-53., as well as the collection of evidence regarding the effectiveness of exercises and therapies, mainly, associated to the body and mind, such as dance, yoga and pilates99 Fonseca CC, Thurm BE, Vecchi RL, Gama EF. Ballroom dance and body size perception. Percept Motor Skill 2014;119(2):495-503..
Although the IMP test has several evaluative functions11 Pereira ES, Segueto KJ, Thurm BE, Gama EF. Body schema analysis between yogaand body combat practitioners. FIEP Bulletin 2010:80(1):494-98.,88 Thurm EB, Matoso A, Diaz CA, Paschoalini C, Neves E, Tuunelis R, Kiyomoto HD, Gama EF. Chronic pain effect on body schema and neuropsychological performance in athletes: a pilot study. Percept Motor Skill 2013;116(2):544-53.-99 Fonseca CC, Thurm BE, Vecchi RL, Gama EF. Ballroom dance and body size perception. Percept Motor Skill 2014;119(2):495-503., our search of the literature found no references regarding its reliability. Thus, it is important to assess the repeatability and reproducibility of the test. Repeatability describes the degree of equality between the results obtained following consecutive measurements conducted by the same rater, using the same instrument and method1010 VIM. International vocabulary of metrology – Basic and general concepts and associated terms (3rd ed. ). Joint Committee for Guides in Metrology: 2012.. Confirmation of this feature allows, for example, the test to be conducted only once, with no need for repetition, thus saving the participants and professionals time. Intra-rater reproducibility describes the degree of equality between the results obtained in tests conducted by the same rater, using the same instrument and method, on different occasions, with a time difference1010 VIM. International vocabulary of metrology – Basic and general concepts and associated terms (3rd ed. ). Joint Committee for Guides in Metrology: 2012. at least 24 hours1111 Associação Brasileira de Normas Técnicas – ABNT. Norma Brasileira Registrada –NBR 10536 – Statistics: Vocabulary and Symbols. 1988; Available from: < https://onedrive. live. com/?cid=4E0D589D53BBEB5D&id=4E0D589D53BBEB5D!119&parId=4E0D589D53BBEB5D!118&o=OneUp> [2016 aug 10].
https://onedrive. live. com/?cid=4E0D589...
. Confirmation of this feature allows, for example, one to state that any differences in the results of tests conducted at distinct moments are derived from a specific intervention.
In addition, as far as we know, the literature contains no clearly defined standardized procedure for performing the IMP test. For example, there is no mention of standardization of the distance at which that the individual should stand in relation to the location where they will mark the points. This may interfere in the results when many individuals are evaluated or when the same participant is reevaluated on different occasions. From the operational standpoint, the original IMP used materials like craft paper and a measuring tape66 Askevold F. Measuring body image. Preliminary report on a new method. Psychother Psychosom 1975;26(2):71-77.. Taking that into account, recording the evaluation using digital photography would facilitate the execution of the test and the storage of information, as well as allow more accurate modes of measurement. Slight changes in the originally proposed methodological procedures may make the test more practical and accurate, as well as more ecological.
From this perspective, seeking to fill this gap in the literature, the objectives of this study were: (1) to propose an adapted version of the IMP test; (2) to assess the repeatability and the intra-rater reproducibility of the adapted test. We believe that by modernizing and standardizing the procedures and applying rigorous methodological assessments, the adapted version of the IMP test will be faster to use and more reliable.
METHODOLOGICAL PROCEDURES
The methodology used to produce the adapted version of IMP, a test designed to assess body schema, consisted of two steps: (1) adaptation of the instrument based on the original IMP methodology; and (2) analysis of repeatability and intra-rater reproducibility of the adapted version. In order to corroborate and justify the adaptations, a brief description of the original IMP methodology, along with its analytical possibilities, is presented below.
The original IMP test
The IMP is considered a tactile-stimulation based projective test, which uses the following standard methodology: the blindfolded subjectis positioned in front of a sheet of craft paper (140cm high by 60cm wide) fixed to a wall at 40cm from the ground and is asked to imagine he/she is standing in front of a mirror. The evaluator then touches predetermined reference points on the subject’s body (top of head, right and left shoulders, waist curves and hips) and the subject should immediately mark the corresponding point on the paper with a marker pen. This procedure is repeated three times. For the purpose of analysis, the subject is placed against the paper and the same anatomical points are marked directly on the same sheet of paper in order to allow comparison between the real image and the perceived image based on the geometric figures obtained by joining the points, from the horizontal widths and the distance from the top of head to the ground6.
The adapted IMP test
In the first stage of the present study, some alterations were introduced to the IMP methodology, such as the use of a whiteboard. This alteration was based on the results of a pilot study conducted with two subjects of different heights (149cm and 195cm), in order to ensure that the test could be used to evaluate adults of various statures. Accordingly, the dimensions of the whiteboard were defined as height 160cm and width 100cm, and fixed 60cm above the ground. Also, a platform, measuring 70 in width, 100cm in length and 2cm in height, was used toposition the feet. To assist feet positioning, three 10cm wide stripes were marked in the center and outer edges of the platform. Considering comfort and balance, the subject was asked to place their feet between the stripes.
In addition, the subject’s position in relation to the white board was standardized based on the length of each individual’s arm, the distance from the right acromion to the styloid process of the right ulna. The following anatomical reference points were selected to be touched during the test: top of head (from the original IMP method), right and left acromion (substituting “shoulder” in the original IMP), a point immediately below the lowest right and left ribs (substituting “waist curves” in the original IMP) and right and left greater trochanter (substituting the “hips” in the original IMP). Following the identification of points with a dermographic pen, reflexive markers were fixed to the same locations and digital photographs of the body in the position adopted for the test were obtained,that is, with the subject’s back to the camera (DSC-W510 - 12.1 megapixels, Sony), which was positioned on a tripod 90cm from the ground and 350cm from the whiteboard.
Following this, the subject was blindfolded and physically prompted. Using the indicator and middle fingers, the researcher touched each reference mark for three seconds. At the same time, the subject was asked to immediately mark the corresponding location on the whiteboard using two marker pens, one in each hand, marking the point with the hand on the same side of the body that was touched, the corresponding mark of a touch in the right acromion was made with the marker in the right hand. Finally, a photographic image of the white board was obtained. Each sequence of points was repeated three consecutive times, without interval between sequences. The first reference point in each sequence was always the apex of the head as recommended in the original IMP test, when the subject was asked to take a deep breath, hold the breath, receive the prompt, mark the point on the white board, and only then exhale. The other prompts, executed in random order, were conducted without any link to breathing.
Interpretation of the adapted IMP test
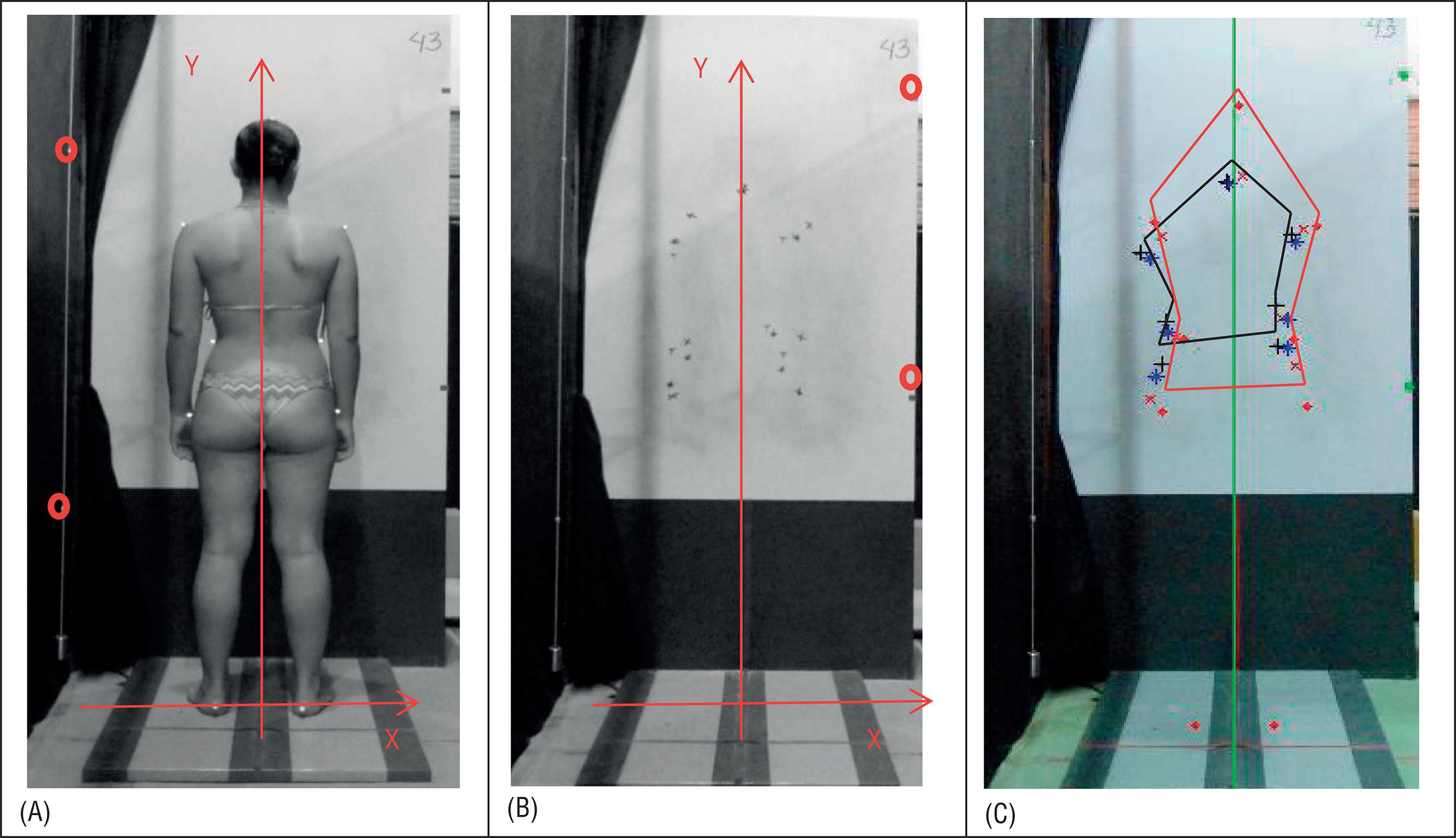
In the interpretation of the adapted instrument, each point, whether of the real image or the perceived image, was represented by x and y coordinates. As there were two distinct planes, one closer (real image) and the other further from the camera (perceived image), two reference systems were constructed, based on two plumb lines, one mobile, which was adjusted according to the standardized distance of the subject from the white board, and the other fixed to the white board. Both of which had two markers 100cm apart. The origin of the reference system adopted in the real image was a point midway between the subject`s heels, ascending vertical axis (y) and the horizontal axis (x) increasing to the right (Figure 1A). As the position of the camera remained unaltered and neither the zoom nor the focus were altered, the origin of the reference system in the perceived image was maintained (Figure 1B). The horizontal reference was assumed to be perpendicular to the plumb line in both cases. Thus, all the values referring to the represented points, both in the real and perceived image had positive ordinates (y values), positive abscissas (x values) when the points were on the right side of the central reference, and negative abscissas when the points were on the left side.
Evaluating the body schema, (A) real image, (B) perceived image (points marked on the board), and (C) figure formed by joining the points: in red, joining the points from the real image, in black, joining the points from the third repetition of the perceived image. The red circles in images (A) and (B) identify the reference points used to construct the scale in each of the coordinate systems.
The same derived measurements used in the original IMP were calculated: the area within the linked points, the distance between the corresponding right and left points and the distance from the top of head to the ground. In addition, the distance between top of head to the point midway between the trochanters and the specific individual coordinate values of each point were evaluated. All calculations were obtained using routines elaborated in Matlab software (version 7.9).
Analysis of repeatability and intra-rater reproducibility
The second stage consisted in the analysis of repeatability and intra-rater reproducibility of the adapted version of the instrument. The sample size was calculated according to Walter, Eliasziw and Donner1414 Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliabilitystudies. Stat Med 1998;17(1):101-10., assuming: the null hypothesis value of the Intraclass Correlation Coefficient - ICC to be 0.40 (on the basis that any value lower than .40 might be considered clinically “unacceptable”); 80% of power; three replicated measurements per subject; and a significance level of 95% to detect an ICC value of 0.6, a minimum number of 52 participants was determined (rounding up from 51.5). Considering any possible losses due to the fact that evaluations would be conducted on two different days, 65 participants were selected (age 28.6±4.0years; weight 60.2±8.0kg; height 165.9±11.0cm; BMI 21.9±1.9Kg/ m2). Given the possibility of gender differences regarding the expression of the body schema, for convenience, only young women, aged between 21 and 35 years, who were part of the university community where this research was conducted, were selected. To be included, participants were required to be healthy and physically active (IPAQ ≤150 minutes of moderate and vigorous weekly physical activity), not to be pregnant, nor present psychological and/or neurological disorders that could interfere with the test. Participants would also be excluded in the case of dizziness or difficulty in maintaining the orthostatic position during the test period. The participants received information regarding the evaluation procedures and agreed to participate voluntarily by signing a free informed consent term in accordance with the requirements of National Health Council. The research was approved by the Research Ethics Committee of the university where the study was conducted.
The evaluations were carried out in a controlled environment, with ambient temperature maintained at 23ºC, stable lighting conditions, and external interferences, including noise, restricted to a minimum. The circadian rhythm of the subjects was obeyed, with the test and re-test being performed preferably at the same time of the day, during day time. First, the subject’s medical history was taken to collect information regarding depressed states and personal data (name and age). After, the IPAQ questionnaire was applied to verify the level of physical activity, and the body mass and height were measured. Then, the subject was instructed to don swimwear (bikini) to perform the test.
Statistic procedures
The data were analyzed using SPSS software, version 20.0. The mean and standard deviation were used in the descriptive analysis. To determine the repeatability and the intra-rater reproducibility, the intra-class coefficient (ICC), the standard error of measurement (SEM) and the minimum detectable change (MDC) were calculated. Where, ICCs>0.80 indicate high reliability, between 0.60-0.79 moderately high reliability, from 0.40-0.59 moderate reliability and <0.40 low reliability1717 Katz JN, Larson MG, Phillips CB, Fossel AH, Liang MH. Comparative measurement sensitivity of short and longer health status instruments. Med Care 1992;30(10):917-25.. Thus, only those ICC values greater than 0.6 were considered relevant. To evaluate the degree to which measurements that may have varied due to errors in the measurement process, the standard error of measurement (SEM) was calculated using the following formula: SEM=SD, where SD is the standard deviation of the measurements1818 Denegar CR, Donald WB. Assessing reliability and precision of measurement: an introduction to intraclass and standard error of measurement. J Sport Rehabil 1993;2(1):35-42.. To evaluate the degree of change necessary to determine whether there was a real change or merely a measurement error, minimum detectable change (MDC) was used based with a 95% confidence interval, where MDC=1.96 * SEM1919 Hicks GE, George SZ, Nevitt MA, Cauley JA, Vogt MT. Measurement of lumbarlordosis: inter-rater reliability, minimum detectable change and longitudinal variation. J Spinal Disord Tech 2006;19(7):501-506.. In all the analyses α<0.05 was adopted.
To analyze repeatability, the three replicates of the first test were considered (tests performed in sequence on the same day). To analyze intra-rater reproducibility, the first replicate, performed on day one, was compared with the first replicate performed after a minimum interval of seven days following the first1515 Staes F, Stappaerts K, Vertommen H, Everaert D, Coppieters M. Reproducibility of a survey questionnaire for the investigation of low back problems in adolescents. Acta Paediatr 1999;88(11):1269-73.,1616 Pedhazur EJ, Schmelkin LP. Measurement, design and analysis: an integrated approach. Hillsdale, NJ: Lawrence Erlbaum Associates, 2013..
RESULTS
In relation to repeatability, for all the analyzed variables (coordinates, distances and area) the ICC scores were classified as excellent, with SEM values less than 4.5cm and MDC values less than 8.5cm (Table 1). By contrast, in the analyzes of reproducibility only two variables, the distance between trochanters and the area within the points, were shown to be relevant (ICC>0.6). None of the coordinates, nor the other distances, had ICC scores greater than 0.6, with SEM values almost doubled and MDC values above 30 cm (Table 2).
DISCUSSION
The repeatability of the adapted instrument was supported by the high ICC values obtained for all the variables (Table 1), which suggests it is unnecessary to conduct three consecutive repetitions. Thus, the method can be adapted to include just one point-marking session. The reduction in the number of repetitions makes the procedure simpler and quicker, with no loss of information quality.
In relation to intra-rater reproducibility (Table 2), given that the ICC classification should be at least high moderate, only the distance between the trochanters and the area within the points should be used in a comparative analysis at two distinct moments (24-hour minimum interval), since only these variables reliably reproduce the perceived body dimensions. The horizontal distances between the acromions and the waist curves, as well as the height from the top of head, measures used in the original version of IMP, were found not to present reproducibility. Therefore, they should not be used.
According to Tavares et al.55 Tavares MCGCF, Campana ANNB, Tavares Filho RF, Campana MB. Avaliaçãoperceptiva da imagem corporal: história, reconceituação e perspectivas para o Brasil. Psicol estud 2010;15(3):509-18., the factors influencing body perception may be either environmental, which are independent of the subject, or subjective, which are intrinsic to the evaluated individual. The environmental factors are created by the test conditions, and include the instruction protocol, the lighting in the evaluation room, the color of clothes, the repetition of the test and the presence of marks on the face. Considering these factors, in the present study, great care was taken in its execution, when instructing the subject and in the choice of location (physical environment and lighting). As the subject remained blindfolded during the evaluation, visual aspects were deemed to have no influence. Regarding to repetitions of the test, this factor had no apparent influence since the measures were repeatable.
On the other hand, the subjective factors are related to individual characteristics55 Tavares MCGCF, Campana ANNB, Tavares Filho RF, Campana MB. Avaliaçãoperceptiva da imagem corporal: história, reconceituação e perspectivas para o Brasil. Psicol estud 2010;15(3):509-18., such as the period of the menstrual cycle, which was not controlled in present study; the body mass index, which did not vary beyond the limits of normality (18.5–24.9kg/m2); depressed states, which were self-reported when taking the medical history and considered an inclusion criterion; the cultural value attributed to certain parts of body, which we were unable to control; and the practice of physical activity. In view of the above, it is believed that subjective factors, even though controlled as far as possible, may have directly influenced the measures and psychometric indexes obtained.
According to Button, Francellaand Slade2121 Button EJ, Francella F, Slade PD. A reappraisal of body perception disturbance in anorexia nervosa. Psychol Med 1977;7(2):235-243. there is no homogeneous perception regarding the body among healthy women, since aspects such as weight changes, concerns about slimness and anxiety appear to mediate body perception differently in each person. This fact corroborates the findings of the present study regarding the area of the body schema, since the area encompasses a larger body dimension, and is more susceptible to perceptive distortions.
The advantages of the adapted IMP include its ease-of-use, the low cost of the materials, the relatively small physical space required, and the short data collection period, since the test needs to be performed only once. Together these features make the instrument feasible for use in evaluating the body schema. It should be noted that although this study was conducted to evaluate only the reliability of the adapted IMP test, future users of this adapted test will also be able to calculate the body perception index, created by Slade and Russel2222 Slade PD, Russell GFM. Awareness of body dimensions in anorexia nervosa:cross-sectional and longitudinal studies. Psychol Med 1973;3(2):188-99., which categorizes the body schema2222 Slade PD, Russell GFM. Awareness of body dimensions in anorexia nervosa:cross-sectional and longitudinal studies. Psychol Med 1973;3(2):188-99.. By determining the ratio between the perceived size and actual size multiplied by 100, the index expresses scores such as underestimation (<100%), normal estimation (=100%) and overestimation (>100%). Thus, it is emphasized that the adapted IMP can be adopted for use in educational and clinical routines, as well as in research, while always respecting ethical and methodological issues1313 Neves AN, Morgado FFR, Tavares MCGCF. Body image assessment: essential notes for a good research practice. Psic: Teor Pesq 2015;31(3):375-80..
The present study has some limitations, including the fact the sample is exclusively composed of young females, which inhibits the extrapolation of the results. Moreover, there are significant limitations regarding inter-rater reproducibility and inter-location reproducibility. Therefore, to overcome these limitations, further studies should be conducted among subjects from both genres, from different age groups, and involving different evaluators and locations.
CONCLUSION
The adapted IMP it is an instrument with excellent repeatability. Therefore, it is suggested that in future evaluations only one test run be performed. With regard to reproducibility, this is restricted to the area within the points and the distance between the trochanters, since these variables represent the perceptual dimension of the body in the same way at different times. In contrast to the original IMP test, when applying this adapted version, we do not recommend the use of the distances between the shoulders, waist curvesor the top of the head in relation to the ground.
REFERENCES
-
1Pereira ES, Segueto KJ, Thurm BE, Gama EF. Body schema analysis between yogaand body combat practitioners. FIEP Bulletin 2010:80(1):494-98.
-
2Segheto W, Segheto KJ, Silva CB, Gama EF. Esquema corporal e nível de atividadefísica em adultos jovens universitários. Rev Bras Ciênc Mov 2011;19(3):29-36.
-
3Cash TF, Pruzinsky T. Body image: a handbook of theory, research and clinical practice. New York: Guilford Press, 2003.
-
4McCabe MP, Ricciardelli LA, Sitaram G, Mikail K. Accuracy of body size estimation: Role of biopsychosocial variables. Body Image 2006;3(2):163-71.
-
5Tavares MCGCF, Campana ANNB, Tavares Filho RF, Campana MB. Avaliaçãoperceptiva da imagem corporal: história, reconceituação e perspectivas para o Brasil. Psicol estud 2010;15(3):509-18.
-
6Askevold F. Measuring body image. Preliminary report on a new method. Psychother Psychosom 1975;26(2):71-77.
-
7Ferreira CC, Favero FM, Fontes SV, Quadros AAJ, Pereira SSR, Oliveira ASB, et al. Análise da imagem e esquema corporal em indivíduos com diagnóstico de síndrome pós-poliomielite. Revi Neuroc 2012;20(1):50-7.
-
8Thurm EB, Matoso A, Diaz CA, Paschoalini C, Neves E, Tuunelis R, Kiyomoto HD, Gama EF. Chronic pain effect on body schema and neuropsychological performance in athletes: a pilot study. Percept Motor Skill 2013;116(2):544-53.
-
9Fonseca CC, Thurm BE, Vecchi RL, Gama EF. Ballroom dance and body size perception. Percept Motor Skill 2014;119(2):495-503.
-
10VIM. International vocabulary of metrology – Basic and general concepts and associated terms (3rd ed. ). Joint Committee for Guides in Metrology: 2012.
-
11Associação Brasileira de Normas Técnicas – ABNT. Norma Brasileira Registrada –NBR 10536 – Statistics: Vocabulary and Symbols. 1988; Available from: < https://onedrive. live. com/?cid=4E0D589D53BBEB5D&id=4E0D589D53BBEB5D!119&parId=4E0D589D53BBEB5D!118&o=OneUp> [2016 aug 10].
» https://onedrive. live. com/?cid=4E0D589D53BBEB5D&id=4E0D589D53BBEB5D!119&parId=4E0D589D53BBEB5D!118&o=OneUp -
12Ferrer-García M, Gutiérrez-Maldonado J. Body Image Assessment Software:psychometric data. Behav Res Methods 2008;40(2):394-407.
-
13Neves AN, Morgado FFR, Tavares MCGCF. Body image assessment: essential notes for a good research practice. Psic: Teor Pesq 2015;31(3):375-80.
-
14Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliabilitystudies. Stat Med 1998;17(1):101-10.
-
15Staes F, Stappaerts K, Vertommen H, Everaert D, Coppieters M. Reproducibility of a survey questionnaire for the investigation of low back problems in adolescents. Acta Paediatr 1999;88(11):1269-73.
-
16Pedhazur EJ, Schmelkin LP. Measurement, design and analysis: an integrated approach. Hillsdale, NJ: Lawrence Erlbaum Associates, 2013.
-
17Katz JN, Larson MG, Phillips CB, Fossel AH, Liang MH. Comparative measurement sensitivity of short and longer health status instruments. Med Care 1992;30(10):917-25.
-
18Denegar CR, Donald WB. Assessing reliability and precision of measurement: an introduction to intraclass and standard error of measurement. J Sport Rehabil 1993;2(1):35-42.
-
19Hicks GE, George SZ, Nevitt MA, Cauley JA, Vogt MT. Measurement of lumbarlordosis: inter-rater reliability, minimum detectable change and longitudinal variation. J Spinal Disord Tech 2006;19(7):501-506.
-
20Gaya A, Garlipp DC, Silva MF, Moreira RB. Ciências do movimento humano: introdução à metodologia da pesquisa. Porto Alegre: Artmed, 2008.
-
21Button EJ, Francella F, Slade PD. A reappraisal of body perception disturbance in anorexia nervosa. Psychol Med 1977;7(2):235-243.
-
22Slade PD, Russell GFM. Awareness of body dimensions in anorexia nervosa:cross-sectional and longitudinal studies. Psychol Med 1973;3(2):188-99.
Publication Dates
-
Publication in this collection
Mar-Apr 2017
History
-
Received
09 Oct 2016 -
Accepted
08 Apr 2017