Abstract
The end of a person’s life raises many ethical dilemmas. Recently, the Brazil’s Federal Council of Medicine approved and regulated the concept of “living will”; as a result, it is of considerable importance that doctors understand the issues that surround this matter. The aim of the present study was to evaluate the knowledge of medical students from the Pará State University, Brazil, of “living wills” and decisions involving the end of life. A cross-sectional study was performed with 238 students who answered a questionnaire of 10 questions. Only 8% of students demonstrated a clear understanding of the term “living will”. Nevertheless, when the definition of “living will” was explained to the participants of the study by the researchers, 92% of students declared that they would respect its provisions. Therefore it appears that while most respondents had a low level of understanding of the concept of “living will”, the vast majority positioned themselves in favor of accepting such a document.
Knowledge; Living wills; Patient rights-Right to die; Advance directives; Advance directive adherence; Students, Medical; Education
Resumo
A terminalidade da vida levanta cada vez mais dilemas éticos. Dada a importância do tema e a recente regulamentação do testamento vital pelo Conselho Federal de Medicina, é de grande valor o conhecimento dessa problemática por parte dos futuros médicos. Assim, buscou-se aferir a compreensão dos estudantes de medicina da Universidade do Estado do Pará acerca do testamento vital e das decisões envolvendo o final da vida. O estudo qualiquantitativo descritivo e transversal entrevistou 238 estudantes por meio de questionário com 10 questões. Apenas 8% dos estudantes demonstraram ter uma noção clara sobre o significado do termo “testamento vital”. Apesar disso, após ouvirem a definição das diretivas antecipadas de vontade fornecida pelos pesquisadores, 92% deles declararam que respeitariam o previsto no testamento vital. Portanto, conclui-se que, embora boa parte dos entrevistados tenha pouco entendimento sobre o tema “testamento vital”, a grande maioria posicionou-se a favor de sua aceitação.
Conhecimento; Testamentos quanto à vida; Direitos do paciente-direito a morrer; Diretivas antecipadas; Adesão a diretivas antecipadas; Estudantes de medicina; Educação
Resumen
La terminalidad de la vida levanta cada vez más dilemas éticos. Dada la importancia del tema y la reciente regulación del testamento vital por el Consejo Federal de Medicina del Brasil, es de gran valor el conocimiento de los futuros médicos acerca de este problema. Por lo tanto, tratamos de evaluar el conocimiento de los estudiantes de medicina de la Universidad del Estado del Pará, en Brasil, acerca del testamento vital y de las decisiones que involucran el final de la vida. La muestra del estudio cualitativo y cuantitativo descriptivo y transversal entrevistó 238 estudiantes y utilizó cuestionario con 10 preguntas. Sólo el 8% de los estudiantes han demostrado una clara comprensión sobre el término “testamento en vida”. Sin embargo, después de escuchar la definición de directrices anticipadas de voluntad proporcionada por los investigadores, el 92% del total declaró que respetarían las disposiciones del testamento vital. Por lo tanto, parece que la mayoría de los encuestados tienen un bajo nivel de comprensión del tema del “Testamento Vital”, pero la gran mayoría se ha posicionado a favor de la aceptación.
Conocimiento; Voluntad en vida; Derechos del paciente-derecho a morir; Directivas anticipadas; Adhesión a las directivas anticipadas; Estudiantes de medicina; Educación
The terminal phase of a disease raises a growing number of ethical dilemmas, generating conflicts among health professionals, patients and family members 11. Nogueira RMR. Ética no fim de vida: decisões médicas relacionadas com a abstenção e suspensão terapêuticas em doentes terminais [dissertação]. Porto: Universidade do Porto; 2009.. When an illness becomes terminal, therapeutic measures can no longer increase the patient’s chances of survival, and instead merely prolong the process of dying 22. Pereira CSA, Faria EO, Silva I, Bianco MM, Sides PM, Camargo VF. O fim da vida. São Paulo: Curso de Graduação em Enfermagem da Universidade Paulista; 2009. Mímeo.
In order to alleviate the pain inherent in the terminal phase of an illness, three approaches are usually defined: euthanasia, orthothanasia and dysthanasia. Euthanasia, or the “good death”, is a practice designed to prevent the suffering of the patient from extending to the end of his or her life 33. Garza MEM. La mejor calidad de vida posible: cuidados paliativos y derecho humano a la salud. [Internet]. Separata: del Periódico Oficial del Estado de Nuevo León. 2009 [acesso 30 set 2015];2(3):6-13. Disponível: http://www.nl.gob.mx/sites/default/files/separata_poe_nl_a01_n03.pdf
http://www.nl.gob.mx/sites/default/files...
. Dysthanasia is a form of therapeutic obstinacy, aimed at delaying an inevitable death. Orthothanasia, meanwhile, treats death as a natural process, in which patients receive treatment only to eliminate or lessen their pain and suffering 44. Morais IM. Autonomia pessoal e morte. Rev. bioét. (Impr.). 2010;18(2):289-309.,55. Yoshikawa DPP. Qual a diferença entre eutanásia, distanásia e ortotanásia? [Internet]. 2009 [acesso 2 nov 2012]. Disponível: http://lfg.jusbrasil.com.br/noticias/87732/qual-a-diferenca-entre-eutanasia-distanasia-e-ortotanasia
http://lfg.jusbrasil.com.br/noticias/877...
.
However, until recently, people with terminal illnesses who found themselves in a vulnerable situation, with a loss of cognitive, mental and relationship capacity, could not decide what kind of medical treatment they would receive. In such cases, any decision regarding treatment was up to the legal representative of the patient. In order to preserve patient autonomy, a significant number of countries (Mexico, Argentina, Colombia, Bolivia and several states of the United States) have incorporated into legislation the concept of “advance healthcare directives”, previously called a “living will”. This is a document written by a person in full possession of their mental faculties, the purpose of which is to specify the care, treatment and procedures which they want, or do not want, to receive when affected by serious illness and are unable to freely express their will 66. Gusmão A. Testamento vital. Arquivos do CRM-PR. 2013 [acesso 24 jun 2015];30(118):1-2. Disponível: http://crmpr.org.br/publicacoes/cientificas/index.php/arquivos/article/view/437/427
http://crmpr.org.br/publicacoes/cientifi...
.
The living will was first proposed in 1967 by the then American Society of Euthanasia as a document relating to anticipated care. In this document, an individual could express in writing his or her desire to suspend medical procedures aimed at the maintenance of life. But it was only in 1991 that a legal provision on the subject was approved: the Patient Self Determination Act (PSDA), the first US federal law to recognize the right to the self-determination of the patient 77. United States General Accounting Office. Patient self-determination act: providers offer information on advance directives but effectiveness uncertain. [Internet]. Washington: HEHS; 1995 [acesso 22 jun 2015]. Disponível: http://www.gpo.gov/fdsys/pkg/GAOREPORTS-HEHS-95-135/pdf/GAOREPORTS-HEHS-95-135.pdf
http://www.gpo.gov/fdsys/pkg/GAOREPORTS-...
.
In Europe, the first country to legalize advance healthcare directives was Spain in 2002. In Portugal, official debate on the subject only began in 2006, based on the proposal of the Associação Portuguesa de Bioética (Portuguese Bioethics Association), which was submitted to the Comissão de Saúde da Assembleia da República (Health Commission of the Portuguese Parliament). According to Nunes 88. Nunes R. Testamento vital. Nascer e Crescer. 2012;21(4):250-5., a bill on informed consent was presented in 2009. While this bill originally proposed the legalization of advance healthcare directives, this topic has since been removed. It was only in July 2012 that the Portuguese Parliament enacted Law 25, which governs advance healthcare directives such as living wills and the appointment of a health care proxy and creates the Registro Nacional do Testamento Vital (National Living Will Registry)99. Portugal. Assembleia da República. Lei nº 25/2012, de 1º de junho 2012. Regula as directivas antecipadas de vontade, designadamente sob a forma de testamento vital, e a nomeação de procurador de cuidados de saúde e cria o Registo Nacional do Testamento Vital (RENTEV). [Internet]. Diário da República. 2012 [acesso 22 jun 2015]; nº 136, p. 3728-30. Disponível: http://www.portaldasaude.pt/NR/rdonlyres/0B43C2DF-C929-4914-A79A-E52C48D87AC5/0/TestamentoVital.pdf
http://www.portaldasaude.pt/NR/rdonlyres...
. In Argentina, where discussion of the topic remains on the political agenda, the first legislation on advance healthcare directives was Law 4263, in the province of Río Negro, enacted on December 19, 2007 1010. Río Negro. Ley nº 4.263, promulgada en el 19 de diciembre 2007. Voluntad anticipada. [Internet]. Boletín Oficial. 2007 [acesso 29 ago 2015]; nº 4.582. Disponível: http://www.notivida.com.ar/legprovincial/RIO_NEGRO_Ley%204263_Voluntad_anticipada.html
http://www.notivida.com.ar/legprovincial...
.
In Brazil, no individual is prevented from notarizing their will in relation to the medical care desired in case of incurable disease. However, with respect to the bioethical principle of autonomy, which expresses the individual’s free will, there is no legislation that requires medical practitioners to comply with the patient’s wishes in a terminal situation. As a result, this right is little known and observed by society. However, on August 31, 2012, the Conselho Federal de Medicina (CFM - Federal Council of Medicine) published Resolution 1995, which governs advance healthcare directives (living wills) 1111. Conselho Federal de Medicina. Resolução nº 1.995, de 9 de agosto de 2012. Dispõe sobre as diretivas antecipadas de vontade dos pacientes. [Internet]. Diário Oficial da União. 2012 [acesso 29 ago 2015]; Seção 1, p. 269-70. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2012/1995_2012.pdf
http://www.portalmedico.org.br/resolucoe...
,1212. Dadalto L. Reflexos jurídicos da Resolução CFM 1.995/12. Rev. bioét. (Impr.). 2013;21(1):106-12.. From this moment onwards, doctors have been obliged to respect the wishes of terminally ill patients, unless those desires (or the desires of their legal representatives) are in conflict with the precepts of the Código de Ética Médica (CEM - Code of Medical Ethics) 1313. Conselho Federal de Medicina. Resolução nº 1.931, de 17 de setembro de 2009. Aprova o Código de Ética Médica. [Internet]. Diário Oficial da União. 2009 [acesso 29 ago 2015]; Seção I, p. 90. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2009/1931_2009.pdf
http://www.portalmedico.org.br/resolucoe...
. According to this resolution, the advance healthcare directives of patients prevail over any other non-medical opinion, including the wishes of relatives 1111. Conselho Federal de Medicina. Resolução nº 1.995, de 9 de agosto de 2012. Dispõe sobre as diretivas antecipadas de vontade dos pacientes. [Internet]. Diário Oficial da União. 2012 [acesso 29 ago 2015]; Seção 1, p. 269-70. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2012/1995_2012.pdf
http://www.portalmedico.org.br/resolucoe...
.
Medicine is currently undergoing a period in which a sensible balance in the doctor-patient relationship is sought. Traditional medical ethics were marked by a strong paternalistic instinct, where the patient would simply comply with the medical decisions made for him or her. Thus, until the first half of the twentieth century, any medical act was judged by taking into account only the morality of the agent, without considering the values and beliefs of patients. It was only in the 1960s that professional codes of ethics came to recognize the patient as an autonomous agent 1414. Junges JR, Cremonese C, Oliveira EA, Souza LL, Backes V. Reflexões legais e éticas sobre o final da vida: uma discussão sobre a ortotanásia. Rev. bioét. (Impr.). 2010;18(2):275-88..
Whether because of the significance of the decisions of the patient regarding the healing process and diagnostic and therapeutic actions, particularly with regard to future medical conduct, or by the regulating of this issue by the CFM 1111. Conselho Federal de Medicina. Resolução nº 1.995, de 9 de agosto de 2012. Dispõe sobre as diretivas antecipadas de vontade dos pacientes. [Internet]. Diário Oficial da União. 2012 [acesso 29 ago 2015]; Seção 1, p. 269-70. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2012/1995_2012.pdf
http://www.portalmedico.org.br/resolucoe...
,1515. Conselho Federal de Medicina. Resolução nº 1.805, de 9 de novembro de 2006. Na fase terminal de enfermidades graves e incuráveis é permitido ao médico limitar ou suspender procedimentos e tratamentos que prolonguem a vida do doente, garantindo-lhe os cuidados necessários para aliviar os sintomas que levam ao sofrimento, na perspectiva de uma assistência integral, respeitada a vontade do paciente ou de seu representante legal. [Internet]. Diário Oficial da União. 2006 [acesso 29 ago 2015]; Seção 1, p. 169. Disponível: http://www.portalmedico.org.br/resolucoes/cfm/2006/1805_2006.htm
http://www.portalmedico.org.br/resolucoe...
, knowledge of advance healthcare directives and their consequences for the patient is now of vital importance to medical students,. The issue is therefore of great relevance to both professionals and patients, manifesting itself both as a concern for the autonomy of patients and part of any consideration of the future of the medical profession and its relationship with the attitudes and aspirations of society. The aim of this study was therefore to determine the level of knowledge of medical students regarding the subject of living wills.
Method
The present work took the form of a descriptive qualitative and quantitative cross-sectional study. A total of 238 medical students from the Universidade do Estado do Pará (UEPA - Pará State University), in the 1st to the 8th semester of study, were surveyed during the month of September 2013. All medical students in this group were included in this study, subject to the exclusion criteria, which were: (1) students under 18; (2) students who refused to participate in the interview or to sign the “termo de consentimento livre e esclarecido” (TCLE - free and informed consent form), which described in detail the objectives of the study.
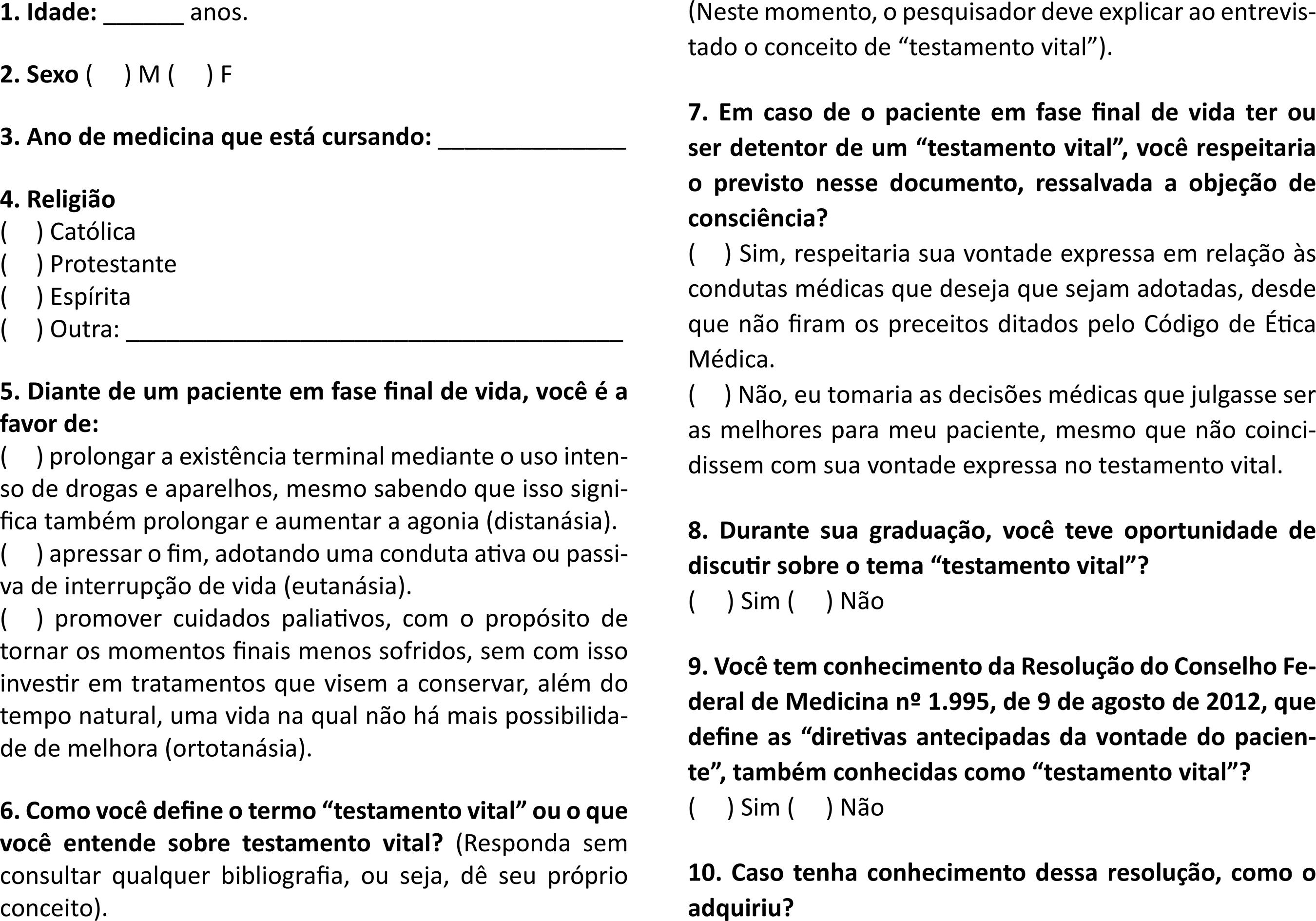
The research instrument was a questionnaire designed specifically for the study (Appendix 1 Appendix 1 Questionnaire ). This consisted of ten questions, four to classify the respondents into groups (age, gender, current semester of course, religion), an objective question on behavior when treating a terminally ill patient (dysthanasia, euthanasia or orthothanasia) and an open question in which the interviewee talked about what he or she understood by the term “living will”. After this question the interviewees were given a definition of “living will” before answering the 7th question, which was whether they would or would not accept the living will of a patient in the final phase of life. The three last questions asked about: whether the student had come into contact with the term “living will” during his or her university course (8th); knowledge of the existence of Resolution 1.995 (9th), and the source of this knowledge (10th).
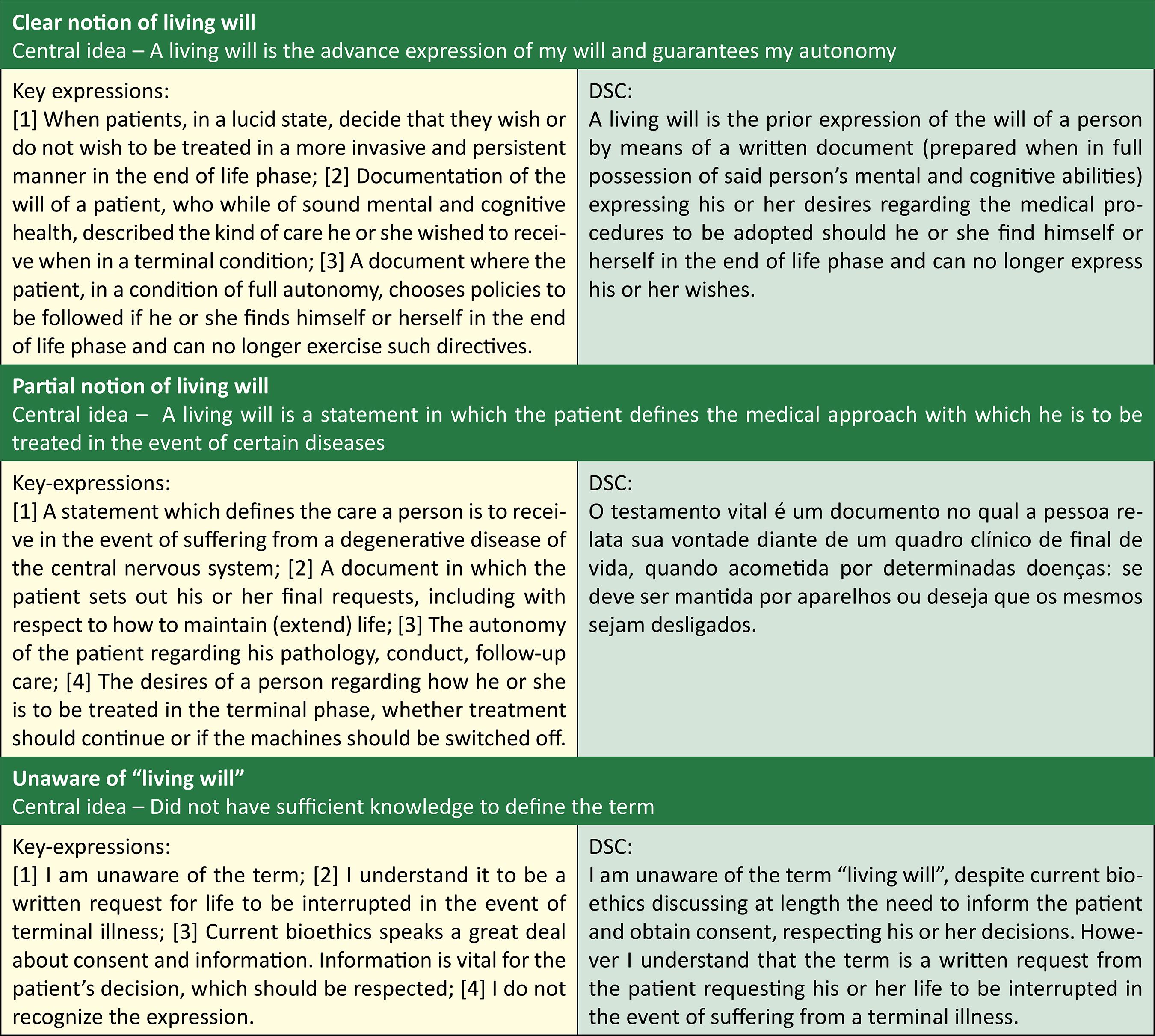
The question in which the student discussed the living will was analyzed using the “discurso do sujeito coletivo” (discourse of the collective subject - DSC), which sought to ascertain whether the respondent had a clear or partial notion of, or was not aware of, the theme. When applying the questionnaires to the students, the researchers provided instructions collectively, in the classroom, explaining the objectives and the form of the participation of individuals in the study. At this time, the TCLE was provided and the optional nature of participation in the study was stressed, together with a reminder that the questionnaire should be filled out individually and without consulting external bibliographic references.
All the subjects in the study were treated in accordance with the precepts of the Declaration of Helsinki 1616. Associação Médica Mundial. Declaração de Helsinque da Associação Médica Mundial: princípios éticos para pesquisa médica envolvendo seres humanos. Jorge MR, tradutor. [Internet]. [s.d.] [acesso 22 jun 2015]. Disponível: http://www.amb.org.br/_arquivos/_downloads/491535001395167888_DoHBrazilianPortugueseVersionRev.pdf
http://www.amb.org.br/_arquivos/_downloa...
and the Nuremburg Code 1717. Tribunal Internacional de Nuremberg. Código de Nuremberg. [Internet]. Nüremberg; 1947 [acesso 29 ago 2015]. Disponível: http://www.ufrgs.br/bioetica/nuremcod.htm
http://www.ufrgs.br/bioetica/nuremcod.ht...
, and the guidelines and directives governing research involving humans expressed in Resolution 466/2012 of the Federal Council of Medicine were respected 1818. Conselho Nacional de Saúde. Resolução nº 466, de 12 de dezembro de 2012. Aprova as seguintes diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. [Internet]. Diário Oficial da União. 2012 [acesso 22 jun 2015]; Seção 1, p. 59. Disponível: http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf
http://conselho.saude.gov.br/resolucoes/...
. The study was approved by the Núcleo de Pesquisa e Extensão de Medicina (NUPEM - Center for Medical Research and Extension Studies) and the research supervisor of the work.
The Excel 2007 software program was used to process the quantitative data, and from a qualitative perspective, the table from the study by Piccini et al 1919. Piccini CF, Steffani JA, Bonamigo EL, Bortoluzzi MC, Schlemper BR Jr. Testamento vital na perspectiva de médicos, advogados e estudantes. Bioethikos. 2011;5(4):384-91. (Appendix 2 Appendix 2 Analytical framework of discourse of the collective subject (DSC) ) was used to analyze the DSC. The Word 2007 software program was used to prepare the text. Descriptive statistical analysis was performed, based on the absolute and percentage values studied.
Results
Of the 238 students interviewed, 108 were men (45.3%) and 130 were women (54.7%). Of these, 45 (19%) were in the first two semesters of their course; 63 (26%), in the 3th or 4th semester; 68 (29%), in the 5th or 6th semester, and 62 (26%), in the 7th or 8th semester.
The age of the students varied between 17 and 28 years. In the first two semesters, the majority (82%) were between 17 and 20 years. In the 3rd and 4th semesters, 57% were aged between 17 and 20 years. In the 5th and 6th, the age groups 17 to 20 years (48%) and 21 to 24 years (44%) were almost equal. In the last two semesters, the majority of respondents (79%) were aged between 21 and 24 years.
In terms of understanding of the term “living will”, only 6% of respondents demonstrated a clear notion, while 33.1% of respondents had a partial notion, 11% were unaware of the theme and the great majority (50%) refrained from answering the question (Table 1).
Understanding of UEPA medicine students in the 1st to the 8th semester of study, in September 2013, of the term “living will”
When asked about the possibility of treating a terminally ill patient with a living will, 43 of students (95%) from the 1st and the 2nd semesters, 62 (98%) from the 3rd and 4th, 64 (94%) from the 5th and the 6th and 60 (97%) from the 7th and 8th semesters, stated that they would respect the wishes of the patient (Table 2).
Position of UEPA medicine students in the 1st to the 8th semester of study, in September 2013, regarding the possibility of treating a terminally ill patient with a living will
In terms of the knowledge of the respondents about CFM Resolution 1.995/2012, the great majority (29%) said that they were unaware of such resolution. Only six (15%) students from the 1st and the 2nd semesters, 21 (33%) from the 3rd and 4th semesters, 24 (35%) from the 5th and 6th and 20 (32%) from the 7th and 8th semesters possessed some knowledge of the subject. All those who declared they knew about the resolution said in the questionnaire that they had obtained their information from the university itself.
Only a small number (18%) of students from the first two semesters said they had had the opportunity to discuss the theme of “living will” during their course. This percentage varied in subsequent semesters, with 66% of students in the 3rd and 4th semesters, 53% from the 5th and 6th and 45% from the 7th and 8th having had such a discussion (Table 3).
Distribution of students in the 1st to the 8th semester of the UEPA medicine course, in September 2013, who had had the opportunity to discuss the subject of the “living will” as part of their degree
Discussion
In the medicine course at UEPA, the first (and only) curricular contact of students with themes of bioethics occurs in the 3rd or 4th semester, in the discipline of Medical Ethics and Human Rights. Despite the fact that issues relating to bioethics are an essential part of medical practice, it can be seen that this area is largely absent from the training of future medical professionals.
When questioned, only 8% of students demonstrated a clear notion of the meaning of the term “living will”. Of these, 74% were in at least their 3rd semester. In contrast, 64% of those interviewed from the 3rd to the 8th semester chose the option “Nothing to declare” or revealed that they were not aware of the term. As Hossne and Hossne have observed, medicine courses, in general, deal with the subject of bioethics before students have experienced clinical situations, meaning that they are unable to recognize the importance of the theme 2020. Hossne WS, Hossne RS. Opinião do estudante de medicina sobre algumas questões bioéticas. Bioética. 1998;6(2):127-33.. Moreover, the authors point out that, in most cases, the approach to these topics is considered only from an ethical angle, from the perspective of the Código de Ética Médica (CEM - Code of Medical Ethics). There is therefore the sense of a need for a greater stimulus for discussion of these issues in order to enable the construction of ideas among students and improve their personal training.
In a similar study, conducted with students in their final year of medical school, Piccini et al 1919. Piccini CF, Steffani JA, Bonamigo EL, Bortoluzzi MC, Schlemper BR Jr. Testamento vital na perspectiva de médicos, advogados e estudantes. Bioethikos. 2011;5(4):384-91. also found a low level of knowledge regarding living wills, with only 29% of respondents demonstrating a clear understanding of the subject. In this study, both professionals and students of medicine and law were analyzed, and a critical panorama of a lack of knowledge of a subject of importance to both disciplines was revealed. Such results may be partly explained however, by the fact that CFM Resolution 1.995/2012, which led to the subject of living wills being more widely discussed, was published only in the year after the study 2121. Pessini L. Distanásia: até quando investir sem agredir? Bioética. 1996;4(1):31-43..
Despite the large number of students who were unfamiliar with the topic, after a brief explanation of the subject, performed by researchers at time of interview, 92% said they would respect the wishes previously recorded in the living will of a patient at the end of life, against 8% who said they would make the medical decisions they deemed to be best for the patient, even if they contradicted those expressed in the document.
Such a position follows CFM Resolution 1.995/2012, which governs the subject in relation the practice of medicine in Brazil. Article 2 of the Resolution states: In decisions about the care and treatment of patients who are unable to communicate their will or to express their desires freely and independently, the doctor shall consider the advance healthcare directives [living will] 1111. Conselho Federal de Medicina. Resolução nº 1.995, de 9 de agosto de 2012. Dispõe sobre as diretivas antecipadas de vontade dos pacientes. [Internet]. Diário Oficial da União. 2012 [acesso 29 ago 2015]; Seção 1, p. 269-70. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2012/1995_2012.pdf
http://www.portalmedico.org.br/resolucoe...
. And, as stated by Gusmão 66. Gusmão A. Testamento vital. Arquivos do CRM-PR. 2013 [acesso 24 jun 2015];30(118):1-2. Disponível: http://crmpr.org.br/publicacoes/cientificas/index.php/arquivos/article/view/437/427
http://crmpr.org.br/publicacoes/cientifi...
, the CFM Resolutions, while not legally binding, are considered to be mandatory for doctors. To disobey them can be interpreted as a breach of the Code of Medical Ethics, which can cause serious problems and even revocation of the permission to practice medicine. It is therefore imperative that medical students from this and future generations are aware of this professional duty, as well as the serious implications of non-compliance with the advance healthcare directives of terminal patients 2222. Brasil. Ministério da Saúde. Instituto Nacional de Câncer. Cuidados paliativos oncológicos: controle da dor. [Internet]. Rio de Janeiro: Inca; 2001 [acesso 29 ago 2015]. (Manuais Técnicos). Disponível: http://www.inca.gov.br/publicacoes/manual_dor.pdf
http://www.inca.gov.br/publicacoes/manua...
,2323. Bomtempo TV. A ortotanásia e o direito de viver com dignidade: uma análise constitucional. Âmbito Jurídico. 2011 [acesso 24 jun 2015];14(89):[s/p.]. Disponível: http://www.ambito-juridico.com.br/site/?n_link=revista_artigos_leitura&artigo_id=9645&revista_caderno=9
http://www.ambito-juridico.com.br/site/?...
.
Due to the importance given to themes of the terminal phases of illness, various religious institutions have reflected on and debated the subject. According to the Confederação Nacional dos Bispos do Brasil (CNBB - National Confederation of Bishops of Brazil), a doctor should accept his or her patient’s desire to receive only palliative care 2424. Conselho Federal de Medicina. Entrevista ao CFM: CNBB apoia ortotanásia. [Internet]. 24 set 2012 [acesso 29 ago 2015]. Disponível: http://portal.cfm.org.br/index.php?option=com_content&view=article&id=23257:entrevista-ao-cfm-cnbb-apoia-ortotanasia&catid=3
http://portal.cfm.org.br/index.php?optio...
. In Portugal, while the Catholic Church was not initially in favor of accepting the living will, after several debates, it now supports the legalization of this device 2525. Cabral LM. Entra em vigor lei que permite o testamento vital. Diário de Notícias. [Internet]. Lisboa, 16 ago 2012 [acesso 29 ago 2015]. Disponível: http://www.dn.pt/inicio/portugal/interior.aspx?content_id=2722143&page=-1
http://www.dn.pt/inicio/portugal/interio...
.
Final considerations
It can be seen that, despite the publicity given to the theme of the terminal phase of illness by the media, many of the students interviewed were unaware of the basic concepts of the subject. Given its relevance for future doctors and for patient autonomy, the need to intensify this discussion during medical training is therefore apparent.
Most respondents had only a partial notion of the meaning of the term “living will”. When asked whether they would or would not accept the patient’s choice, most said they would accept. It was not verified whether this decision was influenced by religious or family issues. Other studies, which could, for example, expand the survey to other environments such as private universities or specific age groups, are required in order to answer the questions posed by this work.
The data of the present study can contribute to the ethical education of medical students and thus improve patient care, which involves the promotion of psychosocial care and support when hospitalized, conduct that also extends to the family members of a terminally ill patient. Medical schools should develop teaching and learning strategies based on the humanities, including issues of bioethics and medical ethics, in order to train doctors with a critical, ethical and reflexive vision.
The information gathered by this study may contribute to improving health services, providing guidance to healthcare managers and teams as they try to improve the care offered in terminal phase of a disease, especially with regard to the urgent need to promote discussions about the theme during training and training courses.
Finally, there is an urgent requirement to extend the discussion of the topic to wider society, informing people about the meaning and scope of advance healthcare directives, as well as making them aware of the understanding that the patient’s decision should be discussed in all its complexity, and respected by health professionals.
Referências
-
1Nogueira RMR. Ética no fim de vida: decisões médicas relacionadas com a abstenção e suspensão terapêuticas em doentes terminais [dissertação]. Porto: Universidade do Porto; 2009.
-
2Pereira CSA, Faria EO, Silva I, Bianco MM, Sides PM, Camargo VF. O fim da vida. São Paulo: Curso de Graduação em Enfermagem da Universidade Paulista; 2009. Mímeo
-
3Garza MEM. La mejor calidad de vida posible: cuidados paliativos y derecho humano a la salud. [Internet]. Separata: del Periódico Oficial del Estado de Nuevo León. 2009 [acesso 30 set 2015];2(3):6-13. Disponível: http://www.nl.gob.mx/sites/default/files/separata_poe_nl_a01_n03.pdf
» http://www.nl.gob.mx/sites/default/files/separata_poe_nl_a01_n03.pdf -
4Morais IM. Autonomia pessoal e morte. Rev. bioét. (Impr.). 2010;18(2):289-309.
-
5Yoshikawa DPP. Qual a diferença entre eutanásia, distanásia e ortotanásia? [Internet]. 2009 [acesso 2 nov 2012]. Disponível: http://lfg.jusbrasil.com.br/noticias/87732/qual-a-diferenca-entre-eutanasia-distanasia-e-ortotanasia
» http://lfg.jusbrasil.com.br/noticias/87732/qual-a-diferenca-entre-eutanasia-distanasia-e-ortotanasia -
6Gusmão A. Testamento vital. Arquivos do CRM-PR. 2013 [acesso 24 jun 2015];30(118):1-2. Disponível: http://crmpr.org.br/publicacoes/cientificas/index.php/arquivos/article/view/437/427
» http://crmpr.org.br/publicacoes/cientificas/index.php/arquivos/article/view/437/427 -
7United States General Accounting Office. Patient self-determination act: providers offer information on advance directives but effectiveness uncertain. [Internet]. Washington: HEHS; 1995 [acesso 22 jun 2015]. Disponível: http://www.gpo.gov/fdsys/pkg/GAOREPORTS-HEHS-95-135/pdf/GAOREPORTS-HEHS-95-135.pdf
» http://www.gpo.gov/fdsys/pkg/GAOREPORTS-HEHS-95-135/pdf/GAOREPORTS-HEHS-95-135.pdf -
8Nunes R. Testamento vital. Nascer e Crescer. 2012;21(4):250-5.
-
9Portugal. Assembleia da República. Lei nº 25/2012, de 1º de junho 2012. Regula as directivas antecipadas de vontade, designadamente sob a forma de testamento vital, e a nomeação de procurador de cuidados de saúde e cria o Registo Nacional do Testamento Vital (RENTEV). [Internet]. Diário da República. 2012 [acesso 22 jun 2015]; nº 136, p. 3728-30. Disponível: http://www.portaldasaude.pt/NR/rdonlyres/0B43C2DF-C929-4914-A79A-E52C48D87AC5/0/TestamentoVital.pdf
» http://www.portaldasaude.pt/NR/rdonlyres/0B43C2DF-C929-4914-A79A-E52C48D87AC5/0/TestamentoVital.pdf -
10Río Negro. Ley nº 4.263, promulgada en el 19 de diciembre 2007. Voluntad anticipada. [Internet]. Boletín Oficial. 2007 [acesso 29 ago 2015]; nº 4.582. Disponível: http://www.notivida.com.ar/legprovincial/RIO_NEGRO_Ley%204263_Voluntad_anticipada.html
» http://www.notivida.com.ar/legprovincial/RIO_NEGRO_Ley%204263_Voluntad_anticipada.html -
11Conselho Federal de Medicina. Resolução nº 1.995, de 9 de agosto de 2012. Dispõe sobre as diretivas antecipadas de vontade dos pacientes. [Internet]. Diário Oficial da União. 2012 [acesso 29 ago 2015]; Seção 1, p. 269-70. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2012/1995_2012.pdf
» http://www.portalmedico.org.br/resolucoes/CFM/2012/1995_2012.pdf -
12Dadalto L. Reflexos jurídicos da Resolução CFM 1.995/12. Rev. bioét. (Impr.). 2013;21(1):106-12.
-
13Conselho Federal de Medicina. Resolução nº 1.931, de 17 de setembro de 2009. Aprova o Código de Ética Médica. [Internet]. Diário Oficial da União. 2009 [acesso 29 ago 2015]; Seção I, p. 90. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2009/1931_2009.pdf
» http://www.portalmedico.org.br/resolucoes/CFM/2009/1931_2009.pdf -
14Junges JR, Cremonese C, Oliveira EA, Souza LL, Backes V. Reflexões legais e éticas sobre o final da vida: uma discussão sobre a ortotanásia. Rev. bioét. (Impr.). 2010;18(2):275-88.
-
15Conselho Federal de Medicina. Resolução nº 1.805, de 9 de novembro de 2006. Na fase terminal de enfermidades graves e incuráveis é permitido ao médico limitar ou suspender procedimentos e tratamentos que prolonguem a vida do doente, garantindo-lhe os cuidados necessários para aliviar os sintomas que levam ao sofrimento, na perspectiva de uma assistência integral, respeitada a vontade do paciente ou de seu representante legal. [Internet]. Diário Oficial da União. 2006 [acesso 29 ago 2015]; Seção 1, p. 169. Disponível: http://www.portalmedico.org.br/resolucoes/cfm/2006/1805_2006.htm
» http://www.portalmedico.org.br/resolucoes/cfm/2006/1805_2006.htm -
16Associação Médica Mundial. Declaração de Helsinque da Associação Médica Mundial: princípios éticos para pesquisa médica envolvendo seres humanos. Jorge MR, tradutor. [Internet]. [s.d.] [acesso 22 jun 2015]. Disponível: http://www.amb.org.br/_arquivos/_downloads/491535001395167888_DoHBrazilianPortugueseVersionRev.pdf
» http://www.amb.org.br/_arquivos/_downloads/491535001395167888_DoHBrazilianPortugueseVersionRev.pdf -
17Tribunal Internacional de Nuremberg. Código de Nuremberg. [Internet]. Nüremberg; 1947 [acesso 29 ago 2015]. Disponível: http://www.ufrgs.br/bioetica/nuremcod.htm
» http://www.ufrgs.br/bioetica/nuremcod.htm -
18Conselho Nacional de Saúde. Resolução nº 466, de 12 de dezembro de 2012. Aprova as seguintes diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. [Internet]. Diário Oficial da União. 2012 [acesso 22 jun 2015]; Seção 1, p. 59. Disponível: http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf
» http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf -
19Piccini CF, Steffani JA, Bonamigo EL, Bortoluzzi MC, Schlemper BR Jr. Testamento vital na perspectiva de médicos, advogados e estudantes. Bioethikos. 2011;5(4):384-91.
-
20Hossne WS, Hossne RS. Opinião do estudante de medicina sobre algumas questões bioéticas. Bioética. 1998;6(2):127-33.
-
21Pessini L. Distanásia: até quando investir sem agredir? Bioética. 1996;4(1):31-43.
-
22Brasil. Ministério da Saúde. Instituto Nacional de Câncer. Cuidados paliativos oncológicos: controle da dor. [Internet]. Rio de Janeiro: Inca; 2001 [acesso 29 ago 2015]. (Manuais Técnicos). Disponível: http://www.inca.gov.br/publicacoes/manual_dor.pdf
» http://www.inca.gov.br/publicacoes/manual_dor.pdf -
23Bomtempo TV. A ortotanásia e o direito de viver com dignidade: uma análise constitucional. Âmbito Jurídico. 2011 [acesso 24 jun 2015];14(89):[s/p.]. Disponível: http://www.ambito-juridico.com.br/site/?n_link=revista_artigos_leitura&artigo_id=9645&revista_caderno=9
» http://www.ambito-juridico.com.br/site/?n_link=revista_artigos_leitura&artigo_id=9645&revista_caderno=9 -
24Conselho Federal de Medicina. Entrevista ao CFM: CNBB apoia ortotanásia. [Internet]. 24 set 2012 [acesso 29 ago 2015]. Disponível: http://portal.cfm.org.br/index.php?option=com_content&view=article&id=23257:entrevista-ao-cfm-cnbb-apoia-ortotanasia&catid=3
» http://portal.cfm.org.br/index.php?option=com_content&view=article&id=23257:entrevista-ao-cfm-cnbb-apoia-ortotanasia&catid=3 -
25Cabral LM. Entra em vigor lei que permite o testamento vital. Diário de Notícias. [Internet]. Lisboa, 16 ago 2012 [acesso 29 ago 2015]. Disponível: http://www.dn.pt/inicio/portugal/interior.aspx?content_id=2722143&page=-1
» http://www.dn.pt/inicio/portugal/interior.aspx?content_id=2722143&page=-1
-
Aprovação CEP/Uepa (Plataforma Brasil) 229.711
Publication Dates
-
Publication in this collection
Sep-Dec 2015
History
-
Received
17 Mar 2015 -
Reviewed
17 Aug 2015 -
Accepted
25 Aug 2015