Abstract
The aim of this study was to find correlations between haematological and rheological parameters in canine visceral leishmaniasis (CLV). Enrolled dogs with CVL (n=31) had a confirmed diagnosis using the rapid test Dual Path Platform (TR DPP®) kit and Polymerase Chain Reaction (PCR) assay. A control group (n=31) comprised healthy dogs with negative results for the TR DPP® kit and PCR assay. Haematological parameters and total protein, albumin, globulin, and antibody were assessed. The rheological properties of the blood samples were also determined. Erythrocytes, haematocrit and platelet values of dogs in the CVL group were found to be lower than those of the control group. The total protein, globulin and IgG concentrations were higher in serum samples from the CVL group. The blood flow curve demonstrated increased shear rates in the CVL group. The viscosity of the blood from the infected animals was lower than in the healthy dogs. A positive correlation was found between erythrocyte numbers and blood viscosity. These data suggest that changes in the flow curve and viscosity of blood as well as the erythrocyte values may be a viable low-cost alternative for the monitoring of dogs with visceral leishmaniasis.
Keywords:
Rheology; Leishmania chagasi; dogs; viscosity; erythrocytes
Resumo
O objetivo deste estudo foi encontrar correlações entre parâmetros hematológicos e reológicos na leishmaniose visceral canina (LVC). Cães com LVC (n=31) tiveram diagnóstico confirmado de LVC pelo teste rápido imunocromatográfico (TR DPP®) e o ensaio de Reação em Cadeia da Polimerase (PCR). Cães saudáveis negativos para o TR DPP® e PCR foram alocados no grupo controle (n=31). Foram avaliados parâmetros hematológicos, proteínas totais, albumina, globulina, anticorpos e as propriedades reológicas do sangue. Os valores de eritrócitos, hematócrito e plaquetas de cães do grupo LVC foram menores do que os encontrados no grupo controle. As concentrações de proteína total, globulina e imunoglobulina G (IgG) foram maiores em amostras de soro do grupo LVC. A curva do fluxo sanguíneo apresentou maior taxa de cisalhamento no grupo LVC. A viscosidade sanguínea dos animais infectados foi menor do que a viscosidade do sangue dos animais do grupo controle. Uma correlação positiva foi encontrada entre o número de eritrócitos e a viscosidade do sangue. Esses dados sugerem que as mudanças na curva de fluxo e viscosidade do sangue, bem como os valores de eritrócitos, podem ser uma alternativa viável e de baixo custo para o monitoramento de cães com leishmaniose visceral.
Palavras-chave:
Reologia; Leishmania chagasi; cães; viscosidade; eritrócitos
Introduction
Visceral leishmaniasis is a zoonotic parasitic disease caused by a protozoan of the family Trypanosomatidae, genus Leishmania. In Brazil, the disease is caused by the species Leishmania chagasi, which is transmitted to humans and animals primarily by Lutzomyia longipalpis ( MISSAWA & LIMA, 2006 Missawa NA, Lima GB. Spatial distribution of Lutzomyia longipalpis (Lutz & Neiva, 1912) and Lutzomyia cruzi (Mangabeira, 1938) in the State of Mato Grosso. Rev Soc Bras Med Trop 2006; 39(4): 337-340. http://dx.doi.org/10.1590/S0037-86822006000400004. PMid:17119747.
http://dx.doi.org/10.1590/S0037-8682200...
; MISSAWA et al., 2011 Missawa NA, Veloso MA, Maciel GB, Michalsky EM, Dias ES. Evidence of transmission of visceral leishmaniasis by Lutzomyia cruzi in the municipality of Jaciara, State of Mato Grosso, Brazil. Rev Soc Bras Med Trop 2011; 44(1): 76-78. http://dx.doi.org/10.1590/S0037-86822011000100017. PMid:21340413.
http://dx.doi.org/10.1590/S0037-8682201...
; FERREIRA et al., 2012 Ferreira GE, Santos BN, Dorval ME, Ramos TP, Porrozzi R, Peixoto AA, et al. The genetic structure of Leishmania infantum populations in Brazil and its possible association with the transmission cycle of visceral leishmaniasis. PLoS One 2012; 7(5): e36242. http://dx.doi.org/10.1371/journal.pone.0036242. PMid:22606248.
http://dx.doi.org/10.1371/journal.pone....
). Visceral leishmaniasis has been identified in all regions of Brazil and due to its high prevalence in dogs, it is believed that they are the primary reservoir in urban areas ( MARCHI et al., 2013 Marchi PGF, Mascarenhas LA, Lago NCMR. Levantamento sorológico de Leishmaniose Visceral Canina no município de Barra do Garças/MT. Rev Eletr Univar 2013; 2(10): 67-70. ).
Clinical signs vary from mild to severe. Lymphadenopathy and skin lesions are the most frequently observed symptoms ( LIMA et al., 2004 Lima WG, Michalick MS, Melo MN, Tafuri WL, Tafuri WL. Canine visceral leishmaniasis: a histopathological study of lymph nodes. Acta Trop 2004; 92(1): 43-53. http://dx.doi.org/10.1016/j.actatropica.2004.04.007. PMid:15301974.
http://dx.doi.org/10.1016/j.actatropica...
; ALMEIDA et al., 2012 Almeida AB, Sousa VR, Cruz FA, Dahroug MA, Figueiredo FB, Madeira MF. Canine visceral leishmaniasis: seroprevalence and risk factors in Cuiabá, Mato Grosso, Brazil. Rev Bras Parasitol Vet 2012; 21(4): 359-365. http://dx.doi.org/10.1590/S1984-29612012005000005. PMid:23184322.
http://dx.doi.org/10.1590/S1984-2961201...
). Studies have shown the presence of amastigotes in lymph nodes of dogs naturally infected with L. chagasi ( ALVES et al., 2009 Alves CF, Amorim IF, Moura EP, Ribeiro RR, Alves CF, Michalick MS, et al. Expression of IFN-γ, TNF-α, IL-10 and TGF-β in lymph nodes associates with parasite load and clinical form of disease in dogs naturally infected with Leishmania (Leishmania) chagasi.
Vet Immunol Immunopathol 2009; 128(4): 349-358. http://dx.doi.org/10.1016/j.vetimm.2008.11.020. PMid:19124159.
http://dx.doi.org/10.1016/j.vetimm.2008...
). Lymph node hypertrophy / hyperplasia occurs mainly in asymptomatic dogs, whereas atrophy is a predominant characteristic of symptomatic animals ( GIUNCHETTI et al., 2008 Giunchetti RC, Martins-Filho OA, Carneiro CM, Mayrink W, Marques MJ, Tafuri WL, et al. Histopathology, parasite density and cell phenotypes of the popliteal lymph node in canine visceral leishmaniasis. Vet Immunol Immunopathol 2008; 121(1-2): 23-33. http://dx.doi.org/10.1016/j.vetimm.2007.07.009. PMid:17723246.
http://dx.doi.org/10.1016/j.vetimm.2007...
). CVL dogs present lymphadenopathy ( LIMA et al., 2004 Lima WG, Michalick MS, Melo MN, Tafuri WL, Tafuri WL. Canine visceral leishmaniasis: a histopathological study of lymph nodes. Acta Trop 2004; 92(1): 43-53. http://dx.doi.org/10.1016/j.actatropica.2004.04.007. PMid:15301974.
http://dx.doi.org/10.1016/j.actatropica...
) with inflammatory infiltrates of macrophages and plasma cells, suggesting the importance of innate and humoral immunity ( MOREIRA et al., 2010 Moreira PR, Vieira LM, Andrade MM, Bandarra MB, Machado GF, Munari DP, et al. Immune response pattern of the popliteal lymph nodes of dogs with visceral leishmaniasis. Parasitol Res 2010; 107(3): 605-613. http://dx.doi.org/10.1007/s00436-010-1902-2. PMid:20499098.
http://dx.doi.org/10.1007/s00436-010-19...
; MOREIRA et al., 2013 Moreira PRR, Bandarra MB, Magalhães GM, Munari DP, Machado GF, Prandini MM, et al. Influence of apoptosis on the cutaneous and peripheral lymph node inflammatory response in dogs with visceral leishmaniasis. Vet Parasitol 2013; 192(1-3): 149-157. http://dx.doi.org/10.1016/j.vetpar.2012.09.029. PMid:23084537.
http://dx.doi.org/10.1016/j.vetpar.2012...
).
Despite the clinical state, the skin and spleen are the main sites of high parasitic density during the course of CVL ( REIS et al., 2009 Reis AB, Martins-Filho OA, Teixeira-Carvalho A, Giunchetti RC, Carneiro CM, Mayrink W, et al. Systemic and compartmentalized immune response in canine visceral leishmaniasis. Vet Immunol Immunopathol 2009; 128(1-3): 87-95. http://dx.doi.org/10.1016/j.vetimm.2008.10.307. PMid:19054576.
http://dx.doi.org/10.1016/j.vetimm.2008...
). Anaemia, uraemia, hyperproteinaemia and hyperglobulinemia are common haematological and biochemical abnormalities observed in visceral leishmaniasis. Noteworthy clinical abnormalities include lymphadenopathy, skin changes, anorexia, onychogryphosis, emaciation, pale mucous membranes, ophthalmopathies, fever and diarrhoea ( FEITOSA et al., 2000 Feitosa MM, Ikeda FA, Luvizotto MCR, Perri SHV. Aspectos clínicos de cães com leishmaniose visceral no município de Araçatuba - São Paulo. Clín Vet 2000; 28: 36-44. ; MAGALHÃES et al., 2012 Magalhães LF, Wilson TM, Medeiros AA. Quadro clínico de cães com Leishmaniose visceral e sua correlação com a sensibilidade do teste parasitológico. Rev Vet Not 2012; 18(2): 67-72. ; MENDONÇA et al., 2015 Mendonça IL, Alves MMM, Batista JF, Rocha FSB, Silva EMC. Biochemical and hematological changes in dogs naturally infected by Leishmania (infantum) chagasi.
Clín Vet 2015; 20: 78-84. ).
Techniques that have been used for the diagnosis of leishmaniasis in dogs include the rapid screening test Dual Path Platform (DPP®), an ELISA test ( BRASIL, 2011 Brasil. Ministério da Saúde. Esclarecimentos sobre substituição do protocolo diagnóstico da leishmaniose visceral canina (LVC). Brasília: Coordenação Geral de Doenças Transmissíveis; Coordenação Geral de Laboratórios de Saúde Pública; Departamento de Vigilância das Doenças Transmissíveis; Secretaria de Vigilância em Saúde; 2011. (Nota Técnica Conjunta; no. 1). ), a Polymerase Chain Reaction (PCR) assay and flow cytometry. Although these diagnostic techniques are effective, the high costs of these tests limit their usefulness, thereby creating a need for new tools for the diagnosis and monitoring of this disease.
Laboratory findings such as biochemical and haematological abnormalities have been demonstrated to be of great prognostic value ( CIARAMELLA et al., 1997 Ciaramella P, Oliva G, Luna RD, Gradoni L, Ambrosio R, Cortese L, et al. A retrospective clinical study of canine leishmaniasis in 150 dogs naturally infected by Leishmania infantum.
Vet Rec 1997; 141(21): 539-543. http://dx.doi.org/10.1136/vr.141.21.539. PMid:9413121.
http://dx.doi.org/10.1136/vr.141.21.539...
; REIS et al., 2006 Reis AB, Teixeira-Carvalho A, Giunchetti RC, Guerra LL, Carvalho MG, Mayrink W, et al. Phenotypic features of circulating leucocytes as immunological markers for clinical status and bone marrow parasite density in dogs naturally infected by Leishmania chagasi.
Clin Exp Immunol 2006; 146(2): 303-311. http://dx.doi.org/10.1111/j.1365-2249.2006.03206.x. PMid:17034583.
http://dx.doi.org/10.1111/j.1365-2249.2...
). In visceral leishmaniasis, anaemia ( MENDONÇA et al., 2015 Mendonça IL, Alves MMM, Batista JF, Rocha FSB, Silva EMC. Biochemical and hematological changes in dogs naturally infected by Leishmania (infantum) chagasi.
Clín Vet 2015; 20: 78-84. ) can cause important erythrocytic alterations that likely cause changes in the adhesion and rheological properties of these cells.
It has been demonstrated that blood rheology can be influenced by the viscosity of the plasma, the erythrocytes, as well as factors affecting erythrocyte aggregation ( PIAGNERELLI et al., 2003 Piagnerelli M, Boudjeltia KZ, Vanhaeverbeek M, Vincent JL. Red blood cell rheology in sepsis. Intensive Care Med 2003; 29(7): 1052-1061. http://dx.doi.org/10.1007/s00134-003-1783-2. PMid:12802488.
http://dx.doi.org/10.1007/s00134-003-17...
). Infections such as malaria ( SCHERER et al., 2016 Scherer EF, Cantarini DG, Siqueira R, Ribeiro EB, Braga EM, Honório-França AC, et al. Cytokine modulation of human blood viscosity from vivax malaria patients. Acta Trop 2016; 158: 139-147. http://dx.doi.org/10.1016/j.actatropica.2016.03.001. PMid:26948901.
http://dx.doi.org/10.1016/j.actatropica...
) and diseases such as sickle cell anaemia ( HIGGINS et al., 2007 Higgins JM, Eddington DT, Bhatia SN, Mahadevan L. Sickle cell vasoocclusion and rescue in a microfluidic device. Proc Natl Acad Sci USA 2007; 104(51): 20496-20500. http://dx.doi.org/10.1073/pnas.0707122105. PMid:18077341.
http://dx.doi.org/10.1073/pnas.07071221...
) and diabetes mellitus ( FRANÇA et al., 2014 França EL, Ribeiro EB, Scherer EF, Cantarini DG, Pessôa RS, França FL, et al. Effects of Momordica charantia L. on the blood rheological properties in diabetic patients. BioMed Res Int 2014; 2014(1): 840379. http://dx.doi.org/10.1155/2014/840379. PMid:24672797.
http://dx.doi.org/10.1155/2014/840379 ...
) have been proposed as disorders in which alterations in blood viscosity may aid in clinical diagnosis.
The correlation between changes in haematological and rheological parameters may be useful as a new method for the diagnosis of visceral leishmaniasis. To investigate this possibility, the present study sought to correlate haematological and rheological parameters in canine visceral leishmaniasis.
Material and Methods
The procedures developed in this work were approved by the Ethics Committee on Use of Animals-CEUA/UFMT (Approval No23108.019567/14-1) and the disclosure of results was authorised by the animal owners, who signed an informed consent form.
Animals
This study was carried out over a 15 month period using 62 dogs of different ages, sexes and breeds, selected and evaluated in the Barra do Garças City, Mato Grosso State, Brazil (Latitude: -15.893, Longitude: 52.2599, 15° 53’ 35” South, 52° 15’ 36” West). The diagnosis of canine visceral leishmaniasis (n=31) was confirmed in each dog using the rapid test Dual Path Platform (RT DPP®) kit and a Polymerase Chain Reaction (PCR) assay. The control group (n=31) comprised healthy dogs without any typical clinical signs of leishmaniasis that had negative results on the RT DPP® kit and PCR assay.
Blood sampling
Blood samples (3 mL) were collected by cephalic or jugular venipuncture. Portions of each blood sample were placed into tubes without anti-coagulant for obtaining serum as well as into anti-coagulant (Ethylene diamine tetra acetic Acid- EDTA) tubes. The total blood samples were used for rheological and haematological analysis. The serum samples were obtained after centrifugation of the blood sample at 300 x g for 10 min and then transferred to 2 mL microtubes that were stored at –80°C for subsequent measurement of biochemical and immunological parameters.
Immunochromatographic rapid test-TR DPP® kit
The rapid immunochromatographic tests for detection of anti-Leishmania chagasi antibodies (DPP® - Leishmaniosis-visceral-canine-BioManguinhos/FIOCRUZ, Rio de Janeiro, Brazil) were performed according to the manufacturer's protocol.
Polymerase Chain Reaction – PCR Assay
DNA extraction from blood samples was performed by the phenol-chloroform method ( SAMBROOK et al., 1989 Sambrook J, Fritsch EF, Maniatis T. Molecular clonig: a laboratory manual. Nova York: Cold Spring Harbor Laboratory Press; 1989. ). The polymerase chain reaction assay was performed using primers RV1(sense) 5’-CTT TTC TGG TCCCGC GGG TAG G-3’ and RV2(anti-sense) 5’-CCA CCT GGC TAT TTT ACA CCA-3’ '( LACHAUD et al., 2002 Lachaud L, Marchergui-Hammami S, Chabbert E, Dereure J, Dedet JP, Bastien P. Comparison of six PCR methods using peripheral blood for detection of canine visceral leishmaniasis. J Clin Microbiol 2002; 40(1): 210-215. http://dx.doi.org/10.1128/JCM.40.1.210-215.2002. PMid:11773118.
http://dx.doi.org/10.1128/JCM.40.1.210-...
), which amplifies a DNA fragment from a 145bp region of the conserved kDNA present in L. chagasi. The amplification utilized 200mM dNTP, 1 pM of each primer, a buffer solution (10 mMof Tris-HCl and 50 mMofKCl, pH 8.3), 2 mMof MgCl2, 1.5 U of Taq DNA polymerase and 2μl of the DNA sample in a final volume of 25μl. The assays were run for one cycle at 94°C for 4 min, followed by 30 cycles at 94°C for 30s, 60°C for 30s, 72 °C for 30s, and a one-cycle final step extension at 72 °C for 10 minutes. The amplification product was fractionated by 2.0% agarose gel electrophoresis, stained with Gel Red stain and visualized in a transilluminator (UV-300nm).
Haematological parameters
Erythrocytes, total leukocytes and platelet counts were performed as described by Anthony & Sirois (2007) Anthony E, Sirois M. Hematology and hemostasis. In: Hendrix CM, Sirois M. Laboratory procedures for veterinary technicians. 5th ed. St. Louis: Elsevier Mosby; 2007. p. 27-73. . The haemoglobin level was measured by the cyanmethemoglobin method and the haematocrit was determined by the microhaematocrit method. The evaluation criteria and reference values used were those established by Feldman et al. (2000) Feldman BF, Zinkl JG, Jain NC. Schalm’s veterinary hematology. 5th ed. Oxford: Blackwell Publishing Ltda; 2000. .
Albumin, total protein and globulin determination
The serum biochemistry was assessed with a semiautomatic analyser (Celm SB-190® , São Paulo, Brazil) and commercial kits (Gold Analisa® , Belo Horizonte, Brazil) were used to determine the levels of albumin. Serum total protein was determined by refractometry. The globulin levels were calculated as the difference between the serum total protein and albumin concentrations ( THRALL, 2015 Thrall MA. Classificação e abordagem diagnostica da anemia. In: Trhall MA, Weiser G, Allison RW, Campbell TW. Hematologia e bioquímica clínica veterinária. São Paulo: Ed. Roca; 2015. p. 65-68. ).
Immunoglobulin determination
The immunoglobulin (IgM and IgG) concentrations in the sera were determined by the turbidimetric method. For IgM at 1:11 (v/v) and for IgG at 1:15 (v/v), the antibody concentrations were determined using IgM (Bioclin®, Brazil, Ref K063) and IgG (Bioclin®, Brazil, Ref K062) antisera diluted at 1:12 (v/v). A calibration curve obtained from the Multical (Bioclin®, Brazil, Ref K064) calibrator was used to determine the standard curve for each immunoglobulin. Samples of sera, standards, and positive and negative control sera were placed in 500μL of buffer solution (sodium chloride 0.15 mol/L, Tris 50 mmol / L, 6.0000 PEG 50 g/L, and sodium azide15.38 nmol/L). The suspensions were mixed and incubated at 37oC for 10 min. The reactions were read on a spectrophotometer at 340 nm.
Blood rheological parameters
The rheological parameters were measured using the Modular Compact Rheometer – MCR 102 [Anton Paar® GmbH, Ostfildern, Germany] as described by França et al. (2014) França EL, Ribeiro EB, Scherer EF, Cantarini DG, Pessôa RS, França FL, et al. Effects of Momordica charantia L. on the blood rheological properties in diabetic patients. BioMed Res Int 2014; 2014(1): 840379. http://dx.doi.org/10.1155/2014/840379. PMid:24672797.
http://dx.doi.org/10.1155/2014/840379 ...
. In all experiments, 600 µL of blood was placed on the surface of a plate reader, followed by the removal of excess sample. The readings were obtained with a permanent control of gap measurements using TruGap™ in 0.099-mm increments and Toolmaster™ CP 50; precise temperature control was achieved using T-Ready™ and Rheoplus V3.61 software. Rheoplus software was also used for the graphics. For the flow curves and viscosity, established parameters were based on the control of shear stress [τ] to 0–5 Pa for the upsweep and 5–0 Pa for downward curves. The tests were conducted under isothermal conditions at 37°C with an analysis of 75 readings.
Statistical analysis
The data are expressed as the mean ± standard error [SE]. Statistically significant differences between groups were evaluated using Student’s t-test. The correlation between immunohaematological parameters and blood viscosity in leishmaniasis was evaluated using the Pearson's linear correlation. Statistical significance was set for p-values lower than 0.05 (P<0.05).
Results
Among the animals selected for this study, 48.39% were female and 51.61% were male. For the CVL dogs, there was a higher prevalence of males (61.29%) than females (38.71%). The dogs’ ages ranged from 1.4 to 8 years in the control group and 1 to 11 years in the CVL group.
Clinical symptoms in seropositive animals (CVL) included lymphadenopathy (77.42%), cutaneous ulcers (58.06%), ear ulceration (51.61%), onychogryphosis (48.39%), desquamation (48.39%), muscular atrophy (35.48%), ophthalmia (35.48%), alopecia (29.03%), splenomegaly (29.03%), lethargy (19.35%), cachexia (30.71%), periocular alopecia (19.35%), hepatomegaly (16.13%), hyperkeratosis (16.13%) and cutaneous nodules (12.90%).
The haematological results are shown in ( Table 1 ). The erythrocytes, haematocrit and platelet values of dogs in the CVL group were found to be lower (p <0.05) than the values for animals in the control group. There were no differences in haemoglobin concentrations or leukocyte counts between the groups studied.
Mean and standard error of erythrocytes, haemoglobin levels, haematocrit, leukocytes and platelets of dogs with canine visceral leishmaniasis (CVL) and control group.
Total protein concentrations and globulin concentrations were higher in the CVL group than in the respective samples from the control group ( Table 2 ). IgG antibody levels were higher in the serum from the CVL group than the control group. Albumin and IgM concentrations were similar between the control and CVL groups.
Mean and standard error of total protein, albumin, globulin and immunoglobulin (IgG and IgM) levels in the sera of dogs with canine visceral leishmaniasis (CVL) and control group.
We evaluated possible correlations between the clinical signs with the haemogram (erythrocytes, haematocrit and platelets). For dogs with CVL, a correlation was observed between erythrocyte numbers and clinical signs of alopecia (r = 0.6762 ; p = 0.0455), splenomegaly (r = 0.9479; p = 0.0001), hepatomegaly (r = 0.8928; p = 0.0414), hyperkeratosis (r = -0.9442; p = 0.0157) and cutaneous nodules (r = -0.9549; p = 0.0114).
The rheological profiles of the blood from dogs with leishmaniasis and from dogs in the control group are shown in ( Figure 1 ). The blood flow curve for both groups begins at the origin, increases, and is nonlinear. An increase in shear rates demonstrated in the blood flow curve of the CVL group ( Figure 1 ).

Blood flow curves of animals with canine visceral leishmaniasis (CVL) and a control group. These data represent the mean of 31 animals in each group. The data were evaluated by Student’s t-test. *indicates intergroup differences.
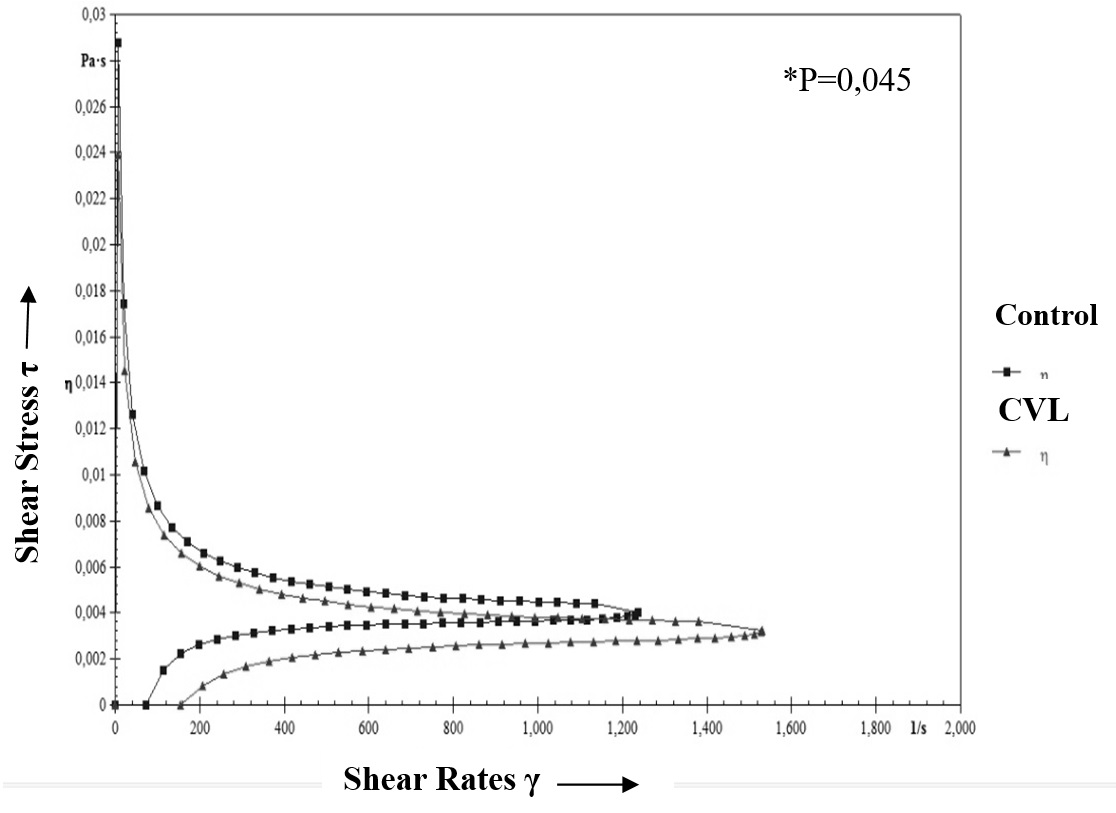
An analysis of blood viscosity as a function of the shear rates is presented in ( Figure 2 ). The viscosity of the blood from infected animals was observed to be significantly (p = 0.045) lower than for the non-infected animals.

Blood viscosity curve as a function of shear rates from dogs with canine visceral leishmaniasis (CVL) and a control group. These data represent the mean of 31 animals in each group. The data were evaluated by Student’s t-test. *indicates intergroup differences.
The blood viscosity and rheological parameters were examined for correlations with haematological parameters using the Pearson test ( Table 3 ). A positive correlation (p<0.05) was observed between erythrocyte numbers and blood viscosity. However, no correlation (p>0.05) was found between blood viscosity and the haematocrit, leukocytes, platelets, total protein concentrations, globulin levels or antibody concentrations.
Correlations between blood viscosity with haematological parameters, proteins and antibody concentrations in the blood of dogs with canine visceral leishmaniasis (CVL) and control group.
Discussion
The findings of the present study indicate that animals with visceral leishmaniasis exhibit changes in their blood flow curves and blood viscosity and that the alterations of these rheological parameters are correlated with haematological abnormalities.
Visceral leishmaniasis, which is the most severe form of leishmaniasis, is endemic in more than 80 countries ( WHO, 2016 World Health Organization – WHO. Leishmaniasis: epidemiological situation. Geneva: WHO; 2016. (Fact sheet). ). Transmission of leishmaniasis is believed to be increasing in Brazil, with 43% of the population at risk for developing the disease. The high prevalence of infected dogs is an important factor that contributes to the maintenance and transmission of this parasite in urban areas ( MARCHI et al., 2013 Marchi PGF, Mascarenhas LA, Lago NCMR. Levantamento sorológico de Leishmaniose Visceral Canina no município de Barra do Garças/MT. Rev Eletr Univar 2013; 2(10): 67-70. ).
In this study, animals with visceral leishmaniasis demonstrated clinical signs of this disease such as lymphadenopathy, skin ulcers, ulcerated ears, and peeling, onychogryphosisas described in previous studies ( FEITOSA et al., 2000 Feitosa MM, Ikeda FA, Luvizotto MCR, Perri SHV. Aspectos clínicos de cães com leishmaniose visceral no município de Araçatuba - São Paulo. Clín Vet 2000; 28: 36-44. ; MATTOS et al., 2004 Mattos DG Jr, Pinheiro JM, Menezes RC, Costa DA. Clinical and laboratorial aspects of seropositive dogs to leishmaniosis. Arq Bras Med Vet Zootec 2004; 56(1): 119-122. ; MAGALHÃES et al., 2012 Magalhães LF, Wilson TM, Medeiros AA. Quadro clínico de cães com Leishmaniose visceral e sua correlação com a sensibilidade do teste parasitológico. Rev Vet Not 2012; 18(2): 67-72. ; ALMEIDA et al., 2012 Almeida AB, Sousa VR, Cruz FA, Dahroug MA, Figueiredo FB, Madeira MF. Canine visceral leishmaniasis: seroprevalence and risk factors in Cuiabá, Mato Grosso, Brazil. Rev Bras Parasitol Vet 2012; 21(4): 359-365. http://dx.doi.org/10.1590/S1984-29612012005000005. PMid:23184322.
http://dx.doi.org/10.1590/S1984-2961201...
).
Structural changes in erythrocytes and alterations in viscosity have been reported in other diseases ( HIGGINS et al., 2007 Higgins JM, Eddington DT, Bhatia SN, Mahadevan L. Sickle cell vasoocclusion and rescue in a microfluidic device. Proc Natl Acad Sci USA 2007; 104(51): 20496-20500. http://dx.doi.org/10.1073/pnas.0707122105. PMid:18077341.
http://dx.doi.org/10.1073/pnas.07071221...
; FRANÇA et al., 2014 França EL, Ribeiro EB, Scherer EF, Cantarini DG, Pessôa RS, França FL, et al. Effects of Momordica charantia L. on the blood rheological properties in diabetic patients. BioMed Res Int 2014; 2014(1): 840379. http://dx.doi.org/10.1155/2014/840379. PMid:24672797.
http://dx.doi.org/10.1155/2014/840379 ...
; SCHERER et al., 2016 Scherer EF, Cantarini DG, Siqueira R, Ribeiro EB, Braga EM, Honório-França AC, et al. Cytokine modulation of human blood viscosity from vivax malaria patients. Acta Trop 2016; 158: 139-147. http://dx.doi.org/10.1016/j.actatropica.2016.03.001. PMid:26948901.
http://dx.doi.org/10.1016/j.actatropica...
). In this study, there was a reduction in erythrocyte numbers, the haematocrit and platelet numbers in the blood of dogs with visceral leishmaniasis, indicating mild anaemia ( MATTOS et al., 2004 Mattos DG Jr, Pinheiro JM, Menezes RC, Costa DA. Clinical and laboratorial aspects of seropositive dogs to leishmaniosis. Arq Bras Med Vet Zootec 2004; 56(1): 119-122. ; IKEDA-GARCIA & FEITOSA, 2006 Ikeda-Garcia FA, Feitosa MM. Métodos de diagnóstico da leishmaniose visceral canina. Clín Vet 2006; 11: 32-38. ; MEDEIROS et al., 2008 Medeiros CMO, Melo AGC, Lima AKF, Silva ING, Oliveira LC, Silva MC. Haematological profile of dogs with visceral leishmaniasis in the city of Fortaleza, Ceará. Ciênc Anim 2008; 18(1): 43-50. ; MENDONÇA et al., 2015 Mendonça IL, Alves MMM, Batista JF, Rocha FSB, Silva EMC. Biochemical and hematological changes in dogs naturally infected by Leishmania (infantum) chagasi.
Clín Vet 2015; 20: 78-84. ) and the likely presence of immunoglobulins capable of binding platelets ( TERRAZZANO et al., 2006 Terrazzano G, Cortese L, Piantedosi D, Zappacosta S, Di Loria A, Santoro D, et al. Presence of anti-platelet IgM and IgG antibodies in dogs naturally infected by Leishmania infantum. Vet Immunol Immunopathol 2006; 110(3-4): 331-337. http://dx.doi.org/10.1016/j.vetimm.2005.11.001. PMid:16406554.
http://dx.doi.org/10.1016/j.vetimm.2005...
; CORTESE et al., 2009 Cortese L, Piantedosi D, Ciaramella P, Pero ME, Sica M, Ruggiero G, et al. Secondary immune-mediated thrombocytopenia in dogs naturally infected by Leishmania infantum.
Vet Rec 2009; 164(25): 778-782. http://dx.doi.org/10.1136/vr.164.25.778. PMid:19542552.
http://dx.doi.org/10.1136/vr.164.25.778...
). Erythropoiesis may occur due to chronic character, blood loss and lysis of erythrocytes by production of autoantibodies leading to splenic sequestration ( TERRAZZANO et al., 2006 Terrazzano G, Cortese L, Piantedosi D, Zappacosta S, Di Loria A, Santoro D, et al. Presence of anti-platelet IgM and IgG antibodies in dogs naturally infected by Leishmania infantum. Vet Immunol Immunopathol 2006; 110(3-4): 331-337. http://dx.doi.org/10.1016/j.vetimm.2005.11.001. PMid:16406554.
http://dx.doi.org/10.1016/j.vetimm.2005...
; IKEDA-GARCIA & FEITOSA, 2006 Ikeda-Garcia FA, Feitosa MM. Métodos de diagnóstico da leishmaniose visceral canina. Clín Vet 2006; 11: 32-38. ). Thrombocytopenia of infected animals may be associated with the clinical stage of the disease and the presence of IgM and IgG anti-platelet antibodies ( CIARAMELLA et al., 2005 Ciaramella P, Pelagalli A, Cortese L, Pero ME, Corona M, Lombardi P, et al. Altered platelet aggregation and coagulation disorders related to clinical findings in 30 dogs naturally infected by Leishmania infantum. Vet J 2005; 169(3): 465-467. http://dx.doi.org/10.1016/j.tvjl.2004.03.009. PMid:15848791.
http://dx.doi.org/10.1016/j.tvjl.2004.0...
; TERRAZZANO et al., 2006 Terrazzano G, Cortese L, Piantedosi D, Zappacosta S, Di Loria A, Santoro D, et al. Presence of anti-platelet IgM and IgG antibodies in dogs naturally infected by Leishmania infantum. Vet Immunol Immunopathol 2006; 110(3-4): 331-337. http://dx.doi.org/10.1016/j.vetimm.2005.11.001. PMid:16406554.
http://dx.doi.org/10.1016/j.vetimm.2005...
; CORTESE et al., 2009 Cortese L, Piantedosi D, Ciaramella P, Pero ME, Sica M, Ruggiero G, et al. Secondary immune-mediated thrombocytopenia in dogs naturally infected by Leishmania infantum.
Vet Rec 2009; 164(25): 778-782. http://dx.doi.org/10.1136/vr.164.25.778. PMid:19542552.
http://dx.doi.org/10.1136/vr.164.25.778...
).
The response to natural infection of L. infantum is associated with the presence of IgG ( QUINNELL et al., 2003 Quinnell RJ, Courtenay O, Garcez LM, Kaye PM, Shaw MA, Dye C, et al. IgG subclass responses in a longitudinal study of canine visceral leishmaniasis. Vet Immunol Immunopathol 2003; 91(3-4): 161-168. http://dx.doi.org/10.1016/S0165-2427(02)00311-2. PMid:12586479.
http://dx.doi.org/10.1016/S0165-2427(02...
) and IgM specific for Leishmania ( RODRÍGUEZ et al., 2006 Rodríguez A, Solano-Gallego L, Ojeda A, Quintana J, Riera C, Gállego M, et al. Dynamics of Leishmania-specific immunoglobulin isotypes in dogs with clinical leishmaniasis before and after treatment. J Vet Intern Med 2006; 20(3): 495-498. http://dx.doi.org/10.1111/j.1939-1676.2006.tb02887.x. PMid:16734080.
http://dx.doi.org/10.1111/j.1939-1676.2...
). Some studies have reported that an increase in total protein occurs frequently in dogs infected with visceral leishmaniasis due to the increased production of antibodies ( CIARAMELLA et al., 1997 Ciaramella P, Oliva G, Luna RD, Gradoni L, Ambrosio R, Cortese L, et al. A retrospective clinical study of canine leishmaniasis in 150 dogs naturally infected by Leishmania infantum.
Vet Rec 1997; 141(21): 539-543. http://dx.doi.org/10.1136/vr.141.21.539. PMid:9413121.
http://dx.doi.org/10.1136/vr.141.21.539...
; MEDEIROS et al., 2008 Medeiros CMO, Melo AGC, Lima AKF, Silva ING, Oliveira LC, Silva MC. Haematological profile of dogs with visceral leishmaniasis in the city of Fortaleza, Ceará. Ciênc Anim 2008; 18(1): 43-50. ). This study reinforces the hypothesis that increases in total protein and the globulin fraction in the serum of dogs with visceral leishmaniasis is likely associated with higher concentrations of IgG.
Serum albumin concentrations were similar between the two groups of dogs. Studies report that hypoalbuminemia and hyperglobulinemia ( FREITAS et al., 2012 Freitas JCC, Nunes-Pinheiro DC, Lopes BE No, Santos GJL, Abreu CRA, Braga RR, et al. Clinical and laboratory alterations in dogs naturally infected by Leishmania chagasi.
Rev Soc Bras Med Trop 2012; 45(1): 24-29. http://dx.doi.org/10.1590/S0037-86822012000100006. PMid:22370824.
http://dx.doi.org/10.1590/S0037-8682201...
) and albumin/globulin inversion ( MENDONÇA et al., 2015 Mendonça IL, Alves MMM, Batista JF, Rocha FSB, Silva EMC. Biochemical and hematological changes in dogs naturally infected by Leishmania (infantum) chagasi.
Clín Vet 2015; 20: 78-84. ) are frequent changes in dogs with visceral leishmaniasis and suggest that the inversion of these proteins may occur due to the increase in the production of antibodies to Leishmania spp. ( SILVA et al., 2008 Silva EB, Fioravanti MCS, Silva LAF, Araújo EG, Menezes LB, Miguel MP, et al. Característica leucocitária, relação albumina/globulina, proteína plasmática e fibrinogênio de bovinos da raça Nelore, confinados e terminados a pasto. Cienc Rural 2008; 38(8): 2191-2196. http://dx.doi.org/10.1590/S0103-84782008000800016.
http://dx.doi.org/10.1590/S0103-8478200...
).
Alterations in erythrocytes, inhibition of normal erythrocyte aggregation ( PIAGNERELLI et al., 2003 Piagnerelli M, Boudjeltia KZ, Vanhaeverbeek M, Vincent JL. Red blood cell rheology in sepsis. Intensive Care Med 2003; 29(7): 1052-1061. http://dx.doi.org/10.1007/s00134-003-1783-2. PMid:12802488.
http://dx.doi.org/10.1007/s00134-003-17...
), increases in glucose levels ( FRANÇA et al., 2014 França EL, Ribeiro EB, Scherer EF, Cantarini DG, Pessôa RS, França FL, et al. Effects of Momordica charantia L. on the blood rheological properties in diabetic patients. BioMed Res Int 2014; 2014(1): 840379. http://dx.doi.org/10.1155/2014/840379. PMid:24672797.
http://dx.doi.org/10.1155/2014/840379 ...
), protein levels ( FORESTO et al., 2005 Foresto P, D’Arrigo M, Filippini F, Gallo R, Barberena L, Racca L, et al. Evaluación de alteraciones hemorreológicas en pacientes hipertensos. Medicina (B Aires) 2005; 65(2): 121-125. PMid:16075805. ) and infections ( SCHERER et al., 2016 Scherer EF, Cantarini DG, Siqueira R, Ribeiro EB, Braga EM, Honório-França AC, et al. Cytokine modulation of human blood viscosity from vivax malaria patients. Acta Trop 2016; 158: 139-147. http://dx.doi.org/10.1016/j.actatropica.2016.03.001. PMid:26948901.
http://dx.doi.org/10.1016/j.actatropica...
) may influence blood viscosity.
The rheological properties of erythrocytes are important gauges, as they may indicate increased destruction of these cells, leading to anaemia ( MOHANDAS & AN, 2012 Mohandas N, An X. Malaria and human red blood cells. Med Microbiol Immunol (Berl) 2012; 201(4): 593-598. http://dx.doi.org/10.1007/s00430-012-0272-z. PMid:22965173.
http://dx.doi.org/10.1007/s00430-012-02...
). In this study, dogs with visceral leishmaniasis had lower blood viscosities and lower percentages of erythrocytes and haematocrits than the controls, suggesting that anaemia may be associated with rheological alterations. Studies report that haematocrit values above 50% cause an increase in viscosity, while values below 35% lead to a reduction in blood viscosity (MARTINS & SILVA, 1983 Martins e Silva J. Principles of blood rheology. Acta Med Port 1983; 4(Suppl): 5-7. PMid:6880837. ). It should be noted that the viscosity is directly associated with resistance to blood flow and the shear stress rates in the vascular wall ( YEOM et al., 2014 Yeom J, Hwang BW, Yang DJ, Shin HI, Hahn SK. Effect of osteoconductive hyaluronate hydrogels on calvarial bone regeneration. Biomater Res 2014; 18(1): 8. http://dx.doi.org/10.1186/2055-7124-18-8. PMid:26331059.
http://dx.doi.org/10.1186/2055-7124-18-...
).
The rheological profile of the blood flow, independent of infection, demonstrates a blood flow curve that begins at the origin. Ascending and non-linear behaviour that starts at the origin characterizes non-Newtonian and pseudoplastic fluids under these shear conditions ( ROSENCRANZ & BOGEN, 2006 Rosencranz R, Bogen SA. Clinical laboratory measurement of serum, plasma, and blood viscosity. Am J Clin Pathol 2006; 125(Suppl): S78-S86. PMid:16830959. ; VERDIER et al., 2009 Verdier C, Etienne J, Duperray A, Preziosi L. Rheological properties of biological materials. C R Phys 2009; 10(8): 790-811. http://dx.doi.org/10.1016/j.crhy.2009.10.003.
http://dx.doi.org/10.1016/j.crhy.2009.1...
).
In the ascending and descending flows, the upper curve is not superimposed on the lower curve; between them is an area of hysteresis, which defines the magnitude of the property of thixotropy ( FRANÇA et al., 2014 França EL, Ribeiro EB, Scherer EF, Cantarini DG, Pessôa RS, França FL, et al. Effects of Momordica charantia L. on the blood rheological properties in diabetic patients. BioMed Res Int 2014; 2014(1): 840379. http://dx.doi.org/10.1155/2014/840379. PMid:24672797.
http://dx.doi.org/10.1155/2014/840379 ...
). The presence of a hysteresis area was observed in our study, suggesting that thixotropic properties are present in the blood stream of animals infected with Leishmania chagasi . However, the blood flow curve in this group demonstrated an increase in the shear rate, creating a deviation of the flow curve to the right.
The rheological behaviour of blood is influenced by the properties and interactions of the cellular components and plasma (MARTINS & SILVA, 1983 Martins e Silva J. Principles of blood rheology. Acta Med Port 1983; 4(Suppl): 5-7. PMid:6880837. ). Leishmania spp. are obligatory intracellular organisms of the mononuclear phagocytic system ( CORTES et al., 2012 Cortes S, Vaz Y, Neves R, Maia C, Cardoso L, Campino L. Risk factors for canine leishmaniasis in an endemic Mediterranean region. Vet Parasitol 2012; 189(2-4): 189-196. http://dx.doi.org/10.1016/j.vetpar.2012.04.028. PMid:22575278.
http://dx.doi.org/10.1016/j.vetpar.2012...
). Leukocytes are also rheologically important for flow at the microcirculation level ( ERNST & BERGMANN, 1989 Ernst E, Bergmann H. Influence of cilazapril on blood rheology in healthy subjects: a pilot study. Am J Med 1989; 87(6B): 70S-71S. PMid:2532464. ).
In high concentrations, leukocytes and platelets may become physical obstacles to erythrocyte microcirculation. Temporary or permanent occlusions of the bloodstream may occur if there is reduced deformability of the red blood cells or blood pressure (MARTINS & SILVA, 1983 Martins e Silva J. Principles of blood rheology. Acta Med Port 1983; 4(Suppl): 5-7. PMid:6880837. ). Although in this study no leukocyte alterations were observed, further studies should be performed to demonstrate the role of these cells during Leishmania chagasi infection.
The rheological changes caused by viscosity reduction and increased shear rates associated with decreased erythrocytes and haematocrit levels may be useful as a new tool for the monitoring of animals with visceral leishmaniasis.
Interestingly, blood viscosity and erythrocyte numbers were positively correlated. These findings demonstrate that a reduction in erythrocytes also reduces viscosity and confirm the importance of erythrocytes and blood viscosity changes in leishmaniasis infection.
These data suggest that the effects of leishmaniasis on the flow curve and viscosity of blood in association with erythrocyte values may be considered to be a viable, low-cost alternative for monitoring of dogs with visceral leishmaniasis.
Acknowledgements
This research received grants from Fundação de Amparo à Pesquisa de Mato Grosso (FAPEMAT No 299032/2010) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq No 447218/2014-0 No: 308600/2015-0), Brazil.
Reference
- Almeida AB, Sousa VR, Cruz FA, Dahroug MA, Figueiredo FB, Madeira MF. Canine visceral leishmaniasis: seroprevalence and risk factors in Cuiabá, Mato Grosso, Brazil. Rev Bras Parasitol Vet 2012; 21(4): 359-365. http://dx.doi.org/10.1590/S1984-29612012005000005. PMid:23184322.
» http://dx.doi.org/10.1590/S1984-29612012005000005 - Alves CF, Amorim IF, Moura EP, Ribeiro RR, Alves CF, Michalick MS, et al. Expression of IFN-γ, TNF-α, IL-10 and TGF-β in lymph nodes associates with parasite load and clinical form of disease in dogs naturally infected with Leishmania (Leishmania) chagasi. Vet Immunol Immunopathol 2009; 128(4): 349-358. http://dx.doi.org/10.1016/j.vetimm.2008.11.020. PMid:19124159.
» http://dx.doi.org/10.1016/j.vetimm.2008.11.020 - Anthony E, Sirois M. Hematology and hemostasis. In: Hendrix CM, Sirois M. Laboratory procedures for veterinary technicians. 5th ed. St. Louis: Elsevier Mosby; 2007. p. 27-73.
- Brasil. Ministério da Saúde. Esclarecimentos sobre substituição do protocolo diagnóstico da leishmaniose visceral canina (LVC). Brasília: Coordenação Geral de Doenças Transmissíveis; Coordenação Geral de Laboratórios de Saúde Pública; Departamento de Vigilância das Doenças Transmissíveis; Secretaria de Vigilância em Saúde; 2011. (Nota Técnica Conjunta; no. 1).
- Ciaramella P, Oliva G, Luna RD, Gradoni L, Ambrosio R, Cortese L, et al. A retrospective clinical study of canine leishmaniasis in 150 dogs naturally infected by Leishmania infantum. Vet Rec 1997; 141(21): 539-543. http://dx.doi.org/10.1136/vr.141.21.539. PMid:9413121.
» http://dx.doi.org/10.1136/vr.141.21.539 - Ciaramella P, Pelagalli A, Cortese L, Pero ME, Corona M, Lombardi P, et al. Altered platelet aggregation and coagulation disorders related to clinical findings in 30 dogs naturally infected by Leishmania infantum. Vet J 2005; 169(3): 465-467. http://dx.doi.org/10.1016/j.tvjl.2004.03.009. PMid:15848791.
» http://dx.doi.org/10.1016/j.tvjl.2004.03.009 - Cortes S, Vaz Y, Neves R, Maia C, Cardoso L, Campino L. Risk factors for canine leishmaniasis in an endemic Mediterranean region. Vet Parasitol 2012; 189(2-4): 189-196. http://dx.doi.org/10.1016/j.vetpar.2012.04.028. PMid:22575278.
» http://dx.doi.org/10.1016/j.vetpar.2012.04.028 - Cortese L, Piantedosi D, Ciaramella P, Pero ME, Sica M, Ruggiero G, et al. Secondary immune-mediated thrombocytopenia in dogs naturally infected by Leishmania infantum. Vet Rec 2009; 164(25): 778-782. http://dx.doi.org/10.1136/vr.164.25.778. PMid:19542552.
» http://dx.doi.org/10.1136/vr.164.25.778 - Ernst E, Bergmann H. Influence of cilazapril on blood rheology in healthy subjects: a pilot study. Am J Med 1989; 87(6B): 70S-71S. PMid:2532464.
- Feitosa MM, Ikeda FA, Luvizotto MCR, Perri SHV. Aspectos clínicos de cães com leishmaniose visceral no município de Araçatuba - São Paulo. Clín Vet 2000; 28: 36-44.
- Feldman BF, Zinkl JG, Jain NC. Schalm’s veterinary hematology. 5th ed. Oxford: Blackwell Publishing Ltda; 2000.
- Ferreira GE, Santos BN, Dorval ME, Ramos TP, Porrozzi R, Peixoto AA, et al. The genetic structure of Leishmania infantum populations in Brazil and its possible association with the transmission cycle of visceral leishmaniasis. PLoS One 2012; 7(5): e36242. http://dx.doi.org/10.1371/journal.pone.0036242. PMid:22606248.
» http://dx.doi.org/10.1371/journal.pone.0036242 - Foresto P, D’Arrigo M, Filippini F, Gallo R, Barberena L, Racca L, et al. Evaluación de alteraciones hemorreológicas en pacientes hipertensos. Medicina (B Aires) 2005; 65(2): 121-125. PMid:16075805.
- França EL, Ribeiro EB, Scherer EF, Cantarini DG, Pessôa RS, França FL, et al. Effects of Momordica charantia L. on the blood rheological properties in diabetic patients. BioMed Res Int 2014; 2014(1): 840379. http://dx.doi.org/10.1155/2014/840379. PMid:24672797.
» http://dx.doi.org/10.1155/2014/840379 - Freitas JCC, Nunes-Pinheiro DC, Lopes BE No, Santos GJL, Abreu CRA, Braga RR, et al. Clinical and laboratory alterations in dogs naturally infected by Leishmania chagasi. Rev Soc Bras Med Trop 2012; 45(1): 24-29. http://dx.doi.org/10.1590/S0037-86822012000100006. PMid:22370824.
» http://dx.doi.org/10.1590/S0037-86822012000100006 - Giunchetti RC, Martins-Filho OA, Carneiro CM, Mayrink W, Marques MJ, Tafuri WL, et al. Histopathology, parasite density and cell phenotypes of the popliteal lymph node in canine visceral leishmaniasis. Vet Immunol Immunopathol 2008; 121(1-2): 23-33. http://dx.doi.org/10.1016/j.vetimm.2007.07.009. PMid:17723246.
» http://dx.doi.org/10.1016/j.vetimm.2007.07.009 - Higgins JM, Eddington DT, Bhatia SN, Mahadevan L. Sickle cell vasoocclusion and rescue in a microfluidic device. Proc Natl Acad Sci USA 2007; 104(51): 20496-20500. http://dx.doi.org/10.1073/pnas.0707122105. PMid:18077341.
» http://dx.doi.org/10.1073/pnas.0707122105 - Ikeda-Garcia FA, Feitosa MM. Métodos de diagnóstico da leishmaniose visceral canina. Clín Vet 2006; 11: 32-38.
- Lachaud L, Marchergui-Hammami S, Chabbert E, Dereure J, Dedet JP, Bastien P. Comparison of six PCR methods using peripheral blood for detection of canine visceral leishmaniasis. J Clin Microbiol 2002; 40(1): 210-215. http://dx.doi.org/10.1128/JCM.40.1.210-215.2002. PMid:11773118.
» http://dx.doi.org/10.1128/JCM.40.1.210-215.2002 - Lima WG, Michalick MS, Melo MN, Tafuri WL, Tafuri WL. Canine visceral leishmaniasis: a histopathological study of lymph nodes. Acta Trop 2004; 92(1): 43-53. http://dx.doi.org/10.1016/j.actatropica.2004.04.007. PMid:15301974.
» http://dx.doi.org/10.1016/j.actatropica.2004.04.007 - Magalhães LF, Wilson TM, Medeiros AA. Quadro clínico de cães com Leishmaniose visceral e sua correlação com a sensibilidade do teste parasitológico. Rev Vet Not 2012; 18(2): 67-72.
- Marchi PGF, Mascarenhas LA, Lago NCMR. Levantamento sorológico de Leishmaniose Visceral Canina no município de Barra do Garças/MT. Rev Eletr Univar 2013; 2(10): 67-70.
- Martins e Silva J. Principles of blood rheology. Acta Med Port 1983; 4(Suppl): 5-7. PMid:6880837.
- Mattos DG Jr, Pinheiro JM, Menezes RC, Costa DA. Clinical and laboratorial aspects of seropositive dogs to leishmaniosis. Arq Bras Med Vet Zootec 2004; 56(1): 119-122.
- Medeiros CMO, Melo AGC, Lima AKF, Silva ING, Oliveira LC, Silva MC. Haematological profile of dogs with visceral leishmaniasis in the city of Fortaleza, Ceará. Ciênc Anim 2008; 18(1): 43-50.
- Mendonça IL, Alves MMM, Batista JF, Rocha FSB, Silva EMC. Biochemical and hematological changes in dogs naturally infected by Leishmania (infantum) chagasi. Clín Vet 2015; 20: 78-84.
- Missawa NA, Lima GB. Spatial distribution of Lutzomyia longipalpis (Lutz & Neiva, 1912) and Lutzomyia cruzi (Mangabeira, 1938) in the State of Mato Grosso. Rev Soc Bras Med Trop 2006; 39(4): 337-340. http://dx.doi.org/10.1590/S0037-86822006000400004. PMid:17119747.
» http://dx.doi.org/10.1590/S0037-86822006000400004 - Missawa NA, Veloso MA, Maciel GB, Michalsky EM, Dias ES. Evidence of transmission of visceral leishmaniasis by Lutzomyia cruzi in the municipality of Jaciara, State of Mato Grosso, Brazil. Rev Soc Bras Med Trop 2011; 44(1): 76-78. http://dx.doi.org/10.1590/S0037-86822011000100017. PMid:21340413.
» http://dx.doi.org/10.1590/S0037-86822011000100017 - Mohandas N, An X. Malaria and human red blood cells. Med Microbiol Immunol (Berl) 2012; 201(4): 593-598. http://dx.doi.org/10.1007/s00430-012-0272-z. PMid:22965173.
» http://dx.doi.org/10.1007/s00430-012-0272-z - Moreira PR, Vieira LM, Andrade MM, Bandarra MB, Machado GF, Munari DP, et al. Immune response pattern of the popliteal lymph nodes of dogs with visceral leishmaniasis. Parasitol Res 2010; 107(3): 605-613. http://dx.doi.org/10.1007/s00436-010-1902-2. PMid:20499098.
» http://dx.doi.org/10.1007/s00436-010-1902-2 - Moreira PRR, Bandarra MB, Magalhães GM, Munari DP, Machado GF, Prandini MM, et al. Influence of apoptosis on the cutaneous and peripheral lymph node inflammatory response in dogs with visceral leishmaniasis. Vet Parasitol 2013; 192(1-3): 149-157. http://dx.doi.org/10.1016/j.vetpar.2012.09.029. PMid:23084537.
» http://dx.doi.org/10.1016/j.vetpar.2012.09.029 - Piagnerelli M, Boudjeltia KZ, Vanhaeverbeek M, Vincent JL. Red blood cell rheology in sepsis. Intensive Care Med 2003; 29(7): 1052-1061. http://dx.doi.org/10.1007/s00134-003-1783-2. PMid:12802488.
» http://dx.doi.org/10.1007/s00134-003-1783-2 - Quinnell RJ, Courtenay O, Garcez LM, Kaye PM, Shaw MA, Dye C, et al. IgG subclass responses in a longitudinal study of canine visceral leishmaniasis. Vet Immunol Immunopathol 2003; 91(3-4): 161-168. http://dx.doi.org/10.1016/S0165-2427(02)00311-2. PMid:12586479.
» http://dx.doi.org/10.1016/S0165-2427(02)00311-2 - Reis AB, Martins-Filho OA, Teixeira-Carvalho A, Giunchetti RC, Carneiro CM, Mayrink W, et al. Systemic and compartmentalized immune response in canine visceral leishmaniasis. Vet Immunol Immunopathol 2009; 128(1-3): 87-95. http://dx.doi.org/10.1016/j.vetimm.2008.10.307. PMid:19054576.
» http://dx.doi.org/10.1016/j.vetimm.2008.10.307 - Reis AB, Teixeira-Carvalho A, Giunchetti RC, Guerra LL, Carvalho MG, Mayrink W, et al. Phenotypic features of circulating leucocytes as immunological markers for clinical status and bone marrow parasite density in dogs naturally infected by Leishmania chagasi. Clin Exp Immunol 2006; 146(2): 303-311. http://dx.doi.org/10.1111/j.1365-2249.2006.03206.x. PMid:17034583.
» http://dx.doi.org/10.1111/j.1365-2249.2006.03206.x - Rodríguez A, Solano-Gallego L, Ojeda A, Quintana J, Riera C, Gállego M, et al. Dynamics of Leishmania-specific immunoglobulin isotypes in dogs with clinical leishmaniasis before and after treatment. J Vet Intern Med 2006; 20(3): 495-498. http://dx.doi.org/10.1111/j.1939-1676.2006.tb02887.x. PMid:16734080.
» http://dx.doi.org/10.1111/j.1939-1676.2006.tb02887.x - Rosencranz R, Bogen SA. Clinical laboratory measurement of serum, plasma, and blood viscosity. Am J Clin Pathol 2006; 125(Suppl): S78-S86. PMid:16830959.
- Sambrook J, Fritsch EF, Maniatis T. Molecular clonig: a laboratory manual. Nova York: Cold Spring Harbor Laboratory Press; 1989.
- Scherer EF, Cantarini DG, Siqueira R, Ribeiro EB, Braga EM, Honório-França AC, et al. Cytokine modulation of human blood viscosity from vivax malaria patients. Acta Trop 2016; 158: 139-147. http://dx.doi.org/10.1016/j.actatropica.2016.03.001. PMid:26948901.
» http://dx.doi.org/10.1016/j.actatropica.2016.03.001 - Silva EB, Fioravanti MCS, Silva LAF, Araújo EG, Menezes LB, Miguel MP, et al. Característica leucocitária, relação albumina/globulina, proteína plasmática e fibrinogênio de bovinos da raça Nelore, confinados e terminados a pasto. Cienc Rural 2008; 38(8): 2191-2196. http://dx.doi.org/10.1590/S0103-84782008000800016.
» http://dx.doi.org/10.1590/S0103-84782008000800016 - Terrazzano G, Cortese L, Piantedosi D, Zappacosta S, Di Loria A, Santoro D, et al. Presence of anti-platelet IgM and IgG antibodies in dogs naturally infected by Leishmania infantum. Vet Immunol Immunopathol 2006; 110(3-4): 331-337. http://dx.doi.org/10.1016/j.vetimm.2005.11.001. PMid:16406554.
» http://dx.doi.org/10.1016/j.vetimm.2005.11.001 - Thrall MA. Classificação e abordagem diagnostica da anemia. In: Trhall MA, Weiser G, Allison RW, Campbell TW. Hematologia e bioquímica clínica veterinária. São Paulo: Ed. Roca; 2015. p. 65-68.
- Verdier C, Etienne J, Duperray A, Preziosi L. Rheological properties of biological materials. C R Phys 2009; 10(8): 790-811. http://dx.doi.org/10.1016/j.crhy.2009.10.003.
» http://dx.doi.org/10.1016/j.crhy.2009.10.003 - World Health Organization – WHO. Leishmaniasis: epidemiological situation. Geneva: WHO; 2016. (Fact sheet).
- Yeom J, Hwang BW, Yang DJ, Shin HI, Hahn SK. Effect of osteoconductive hyaluronate hydrogels on calvarial bone regeneration. Biomater Res 2014; 18(1): 8. http://dx.doi.org/10.1186/2055-7124-18-8. PMid:26331059.
» http://dx.doi.org/10.1186/2055-7124-18-8
Publication Dates
-
Publication in this collection
24 May 2018 -
Date of issue
Apr-Jun 2018
History
-
Received
27 Nov 2017 -
Accepted
07 Mar 2018