Abstracts
PURPOSE: To verify the applicability of the protocol Overall Assessment of the Speaker's Experience of Stuttering - Adults (OASES-A), translated into Brazilian Portuguese, in a sample of adults who stutter. METHODS: The Brazilian Portuguese version of the OASES-A protocol was individually applied to 18 people who stutter. The classification of stuttering severity was based on the Stuttering Severity Instrument for Children and Adults (SSI-3) protocol. Translation and back-translation processes were carried out by specialists, considering semantic, conceptual, cultural, and idiomatic equivalences. RESULTS: There was no correlation between the severity degrees of stuttering assessed by the SSI-3 protocol and the self-assessment performed using the OASES-A. Subjects reported impairments in perceived fluency; speech ability; level of knowledge about stuttering and treatment options; use of confrontational techniques; quality of life. They also mentioned having difficulty coping with emotional states such as anxiety and embarrassment, and with communication in daily situations. CONCLUSION: The OASES-A protocol is useful in the assessment and treatment of stutterers, as it provides specialized speech-language pathologists with sutterers' self-perception regarding their communication difficulties and the impact of stuttering on their quality of life.
Stuttering; International classification of functioning, disability and health; Quality of life; Speech; Translating
OBJETIVO: Verificar a aplicabilidade do instrumento Overall Assessment of the Speaker's Experience of Stuttering - Adults (OASES-A), traduzido para o Português Brasileiro, em uma amostra de pessoas que gaguejam. MÉTODOS: Foi realizada a aplicação individual do instrumento OASES-A, traduzido para o Português Brasileiro, a 18 pessoas que gaguejam. A classificação da severidade da gagueira foi feita baseada no protocolo Stuttering Severity Instrument for Children and Adults (SSI-3). Os processos de tradução e tradução reversa foram realizados por especialistas, considerando-se as equivalências semântica, conceitual, cultural e idiomática. RESULTADOS: Não houve correlação entre os níveis de severidade da gagueira avaliados por meio do protocolo SSI-3 e os da auto-avaliação mensurados pelo OASES-A. Houve prejuízo relatado quanto à autopercepção da fluência; à habilidade de fala; ao nível de conhecimento da gagueira e opções de tratamento; ao uso de técnicas de enfrentamento; à qualidade de vida. Também foi referida dificuldade em relação aos estados emocionais, como ansiedade e constrangimento, e na comunicação em situações da vida diária. CONCLUSÃO: A aplicação do OASES-A mostrou-se útil para avaliar e tratar pessoas que gaguejam, pois fornece subsídios ao profissional fonoaudiólogo especializado no que se refere à autopercepção destas pessoas sobre as dificuldades na comunicação e o impacto da gagueira sobre a qualidade de vida.
Gagueira; Classificação internacional de funcionalidade, incapacidade e saúde; Qualidade de vida; Fala; Tradução
ORIGINAL ARTICLE
Brazilian version of the Overall Assessment of the Speaker's Experience of Stuttering - Adults protocol (OASES-A)
Eliane Lopes BragattoI; Ellen OsbornI; J. Scott YarussII; Robert QuesalIII; Ana Maria SchieferIV; Brasília Maria ChiariIV
IGraduate Program (Doctorate degree) in Human Communication Disorders, Department of Speech-Language Pathology and Audiology, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil
IIUniversity of Pittsburgh - PITT - Pittsburgh (PA), USA
IIIWestern Illinois University - WIU - Macomb (IL), USA
IVDepartment of Speech-Language Pathology and Audiology, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil
Correspondence address Correspondence address: Eliane Lopes Bragatto R. Botucatu, 802, Vila Clementino São Paulo (SP), Brasil, CEP: 04023-062 E-mail: eliane_bragatto@hotmail.com
ABSTRACT
PURPOSE: To verify the applicability of the protocol Overall Assessment of the Speaker's Experience of Stuttering - Adults (OASES-A), translated into Brazilian Portuguese, in a sample of adults who stutter.
METHODS: The Brazilian Portuguese version of the OASES-A protocol was individually applied to 18 people who stutter. The classification of stuttering severity was based on the Stuttering Severity Instrument for Children and Adults (SSI-3) protocol. Translation and back-translation processes were carried out by specialists, considering semantic, conceptual, cultural, and idiomatic equivalences.
RESULTS: There was no correlation between the severity degrees of stuttering assessed by the SSI-3 protocol and the self-assessment performed using the OASES-A. Subjects reported impairments in perceived fluency; speech ability; level of knowledge about stuttering and treatment options; use of confrontational techniques; quality of life. They also mentioned having difficulty coping with emotional states such as anxiety and embarrassment, and with communication in daily situations.
CONCLUSION: The OASES-A protocol is useful in the assessment and treatment of stutterers, as it provides specialized speech-language pathologists with sutterers' self-perception regarding their communication difficulties and the impact of stuttering on their quality of life.
Keywords: Stuttering; International classification of functioning, disability and health; Quality of life; Speech; Translating.
INTRODUCTION
The World Health Organization (WHO) has proposed a new concept in health which, besides looking at the signs and symptoms of the pathologies, includes greater concern for the social context allied to the efficiency and effectiveness of the evaluative, preventative and interventionist processes. It also seeks for a more critical reflection of the health professional's role in order to improve his capabilities(1,2).
In the area of Speech-Language Pathology, it is suggested a practice based on structural evidence for the evaluation of clinical significance, in which the real improvement of an individual enrolled in speech-language therapy should be understood in terms of its efficacy (functionality of the treatment), efficiency (comparison between treatments), and effect (how the treatment has altered the individual). Moreover, it takes into consideration the socio-economic/cultural reality, the influence of personality traits (biopsychosocial) on the benefits obtained from the treatment, the personal gains in competence and performance, and personal beliefs and values(3).
Scientific evidence is considered of fundamental importance in any clinical decision. The future of different approaches to evaluation and therapy depends on their effectiveness being demonstrated empirically. Only in this way can better results be achieved and translated into the training and education of the clinician, more cost-effective treatment, better understanding of unusual cases and, perhaps most importantly, treatment specifically designed for each individual(4).
Among communication disorders, stuttering has been the object of many research projects as it has different clinical manifestations which have a strong impact on the social and communication development of the stutterer, such as speech rupture; behavioural traits caused by attempts to minimize or avoid ruptures; feelings and attitudes that reflect emotional reactions to negative experiences of lacking fluency in speech.
Taking into consideration factors other than those of systems like the International Classification of Diseases and Health Related Problems (ICDH)(5) started to be developed by the WHO in 1980, by using another system entitled International Classification of Impairments, Disabilities and Handicaps - ICIDH, which describes the possible consequences of disorders to people's lives. This classification was refined in 2001, and resulted in the International Classification of Functionality, Incapacity and Health (ICF), which is more focused on the identification of what constitutes health than on the impact diseases have on the person(1). In this concept proposed by the ICF, the domains would be based in levels of health and levels related to health, always based on the perspectives of the body, the individual and the society.
Since then, new tools have been developed to respond to the premises of the ICF. In the area of human communication disorders, specifically in the area of speech fluency, the Overall Assessment of the Speaker's Experience of Stuttering - Adults (OASES-A) was developed, describing the stuttering disorders as experienced by the stutterer(6-9).
As stuttering affects an average of 1% of the world population, regardless of race or gender(10,11), the application of the OASES-A protocol could contribute to a more detailed insight into the experience of the individual who stutters.
From this perspective, this study had the aim to verify the applicability of the OASES-A protocol in adults who stutter.
METHODS
This study complied with the ethical principles for research with human beings, was approved by the Ethics Committee of the Universidade Federal de São Paulo (UNIFESP) (protocol number 1531/07), and took place at the Speech-Language Pathology Assessment and Diagnosis Division of the Speech-Language Pathology and Audiology Department of UNIFESP.
Participants were 18 adults who stutter, six female and 12 male, with ages ranging from 18 to 38 years (mean=25.8).
The inclusion criterion was having more than 3% of atypical disfluency, in order to establish the stuttering diagnosis. To this end, a sample of at least 200 syllables of connected speech was recorded using a digital camera, for each individual in the sample. The classification of stuttering severity was based on the Stuttering Severity Instrument for Children and Adults (SSI-3)(12). According to the exclusion criteria, subjects with cognitive, psychological and/or neurological impairment and/or less than six years of basic schooling were not included in the sample.
The Overall Assessment of the Speaker's Experience of Stuttering - Adults (OASES-A) consists of 100 items, each one with a score based on the Likert scale, in the range from one to five, that can be applied to individuals over 18 years of age and has a completion time of approximately 20 minutes(8). The scores provide an indication of the impact stuttering has on many aspects of the speaker's life. The instrument is organized in four sections: (a) General information: 20 items related to the speaker's perception of how natural and fluent his speech is; (b) Reactions to stuttering: 30 items that check the affective, behavioral and cognitive reactions; (c) Communication in every-day situations: 25 items that evaluate the degree of communication difficulties in every-day social, work and domestic situations; (d) Quality of life: 25 items regarding the individual's satisfaction with communicative abilities, personal and professional relationships, and other general judgements about his well-being. After compiling the data, section and overall scores are obtained by combining the scores from the four sections. In interpreting the assessment result, the impact of stuttering is classified as: mild, mild to moderate, moderate to severe, or severe.
The translation and adaptation of the OASES-A protocol were carried out based on the recommended methodology for translating questionnaires into other languages(13,14), which was carried out in two phases. The first phase was the translation and adaptation of the content of the OASES-A into Brazilian Portuguese. In the second phase, its concordance after translation was checked.
The translated and adapted version of the OASES-A instrument into Brazilian Portuguese was then applied to the individuals in the sample. The results of the tests were analyzed based on descriptive and inferential statistics.
It is important to emphasize that, originally, the OASES-A protocol is self-administered(8). In the present study, the protocol was also self-administered, but we excluded individuals with less than six years of basic schooling to avoid possible difficulties reading and answering the questionnaire. Further studies may show whether an interview format would be more appropriate for the Brazilian version.
RESULTS
Most of the participants completed the OASES-A protocol in 20 minutes and the mean total time spent with each individual was 35 minutes, including the time taken to explain the instrument and clarify eventual doubts.
There was no correlation between the stuttering severity levels measured by the SSI-3 protocol and the self-assessment measured by the OASES-A in the studied individuals (Table 1).
The findings showed that there was no gender- (Table 2) and/or schooling-related (Table 3) differences in the studied variables: General information, Reactions to stuttering, Communication in every-day life, Quality of life, and Total impact, measured by the OASES-A protocol.
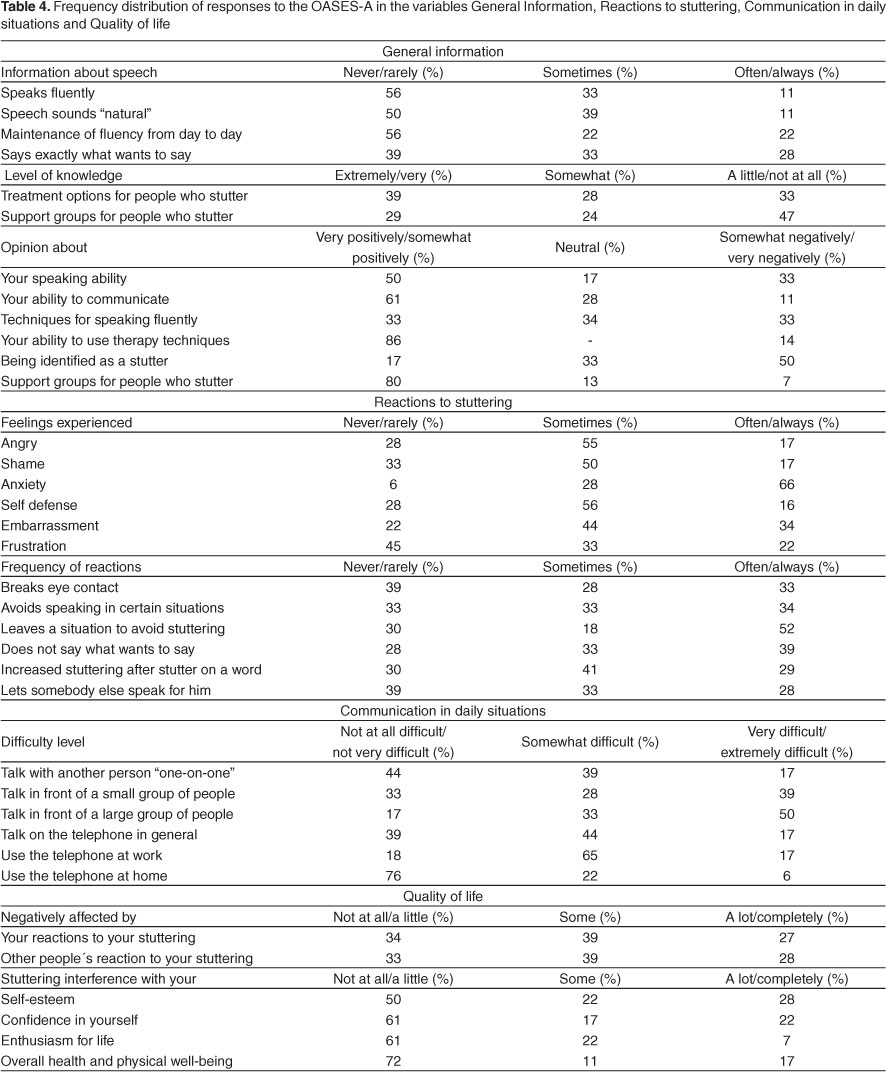
The frequency distribution of the OASES-A responses for the variables: General information, Reactions to stuttering, Communication in every-day life, and Quality of life is shown in Table 4.
Regarding the variable General information, in the questions regarding self-perception of the ability to speak fluently, producing a speech that sounds natural, and in maintaining speech fluency from one day to the next, half of the participants reported that they always/many times achieved this. This was noted even for participants classified as having moderate or severe stuttering according to the SSI-3 protocol. Only one third of the participants reported that they rarely/never say exactly what they want when they feel they may stutter. Still on this subject, higher scores were attributed to the negative impression about the ability to speak, when compared to the scores attributed to the negative impression about the ability to communicate.
In the questions regarding the level of knowledge about stuttering, a large number of participants reported to have low or no knowledge about treatment options for stutterers, especially regarding self-help or support groups. However, most of those who knew the subject well considered self-help or support groups for stutterers very positive/positive, and more than half of the participants felt negatively about being a stutterer or being identified by others as a stutterer.
A large number of participants indicated a negative impression about the techniques used to speak fluently; however, when asked about the ability to apply the techniques learned in therapy, most of them had a positive/very positive impression.
As for the variable Reactions to stuttering, more than half of the participants reported having anxiety always/very often, concomitant with situations of disfluent speech. Embarrassment was the second most mentioned emotional state. Other relevant aspects regarding the reactions to stuttering were: avoiding eye contact, looking at the interlocutor, answering questions and speaking in certain situations or to certain people, letting others speak for them, the increase in stuttering after stuttering over a word, leaving a situation for fear of stuttering, and asking for something not needed.
Regarding the variable Every-day communication, few participants referred a lot/extreme difficulty in talking "face-to-face" to the interlocutor, but when asked about talking in front of a small group of people, the percentage increased, reaching half of the participants regarding dealing with speaking in front of a large group of people. When the questions were related to the degree of relationship with the interlocutor(s), more than half reported some degree of difficulty in talking to people they vaguely knew, but no difficulty in talking to people they knew well. The questions related to situations in familiar surroundings, such as when talking to their spouse or to other members of the family or taking part in family discussions, were the ones with less difficulty. Speaking on the phone at work and in other everyday situations presented some degree of difficulty for most subjects, but this index fell dramatically when speaking on the phone was done within a familiar environment.
As for the variable Quality of life, it was observed that most participants felt some loss. However, when asked about their own reactions and those of other people to stuttering, the indices are high. Stuttering was also cited by the participants as a factor that interfers a lot/completely in self-esteem, self-confidence, enthusiasm for life, and general and physical well-being.
DISCUSSION
It is generally felt that the translation and adaptation process frequently prioritizes the adaption to the culture in detriment to the semantic equivalence(15). In the translation of OASES- adaptations of the cultural equivalence were not checked as it was assumed that the translation is less susceptible to generating doubts when applied to people who stutter.
The average time spent completing the instument was similar to that of the participants in the English version As the instrument is made up of a total of 100 items, it is possible to surmise that the time spent is comparatively short and, therefore its application in the health service is feasible.
One of the things that could make completing OASES-A easier, despite the high number of items,is that it is compartmentalised in four distinct sections and these , in turn , are divided into specific areas such as, in situations: general,work,social and family environments. This disposition of the items leads the participant to answer, in sequence, questions about the same subject thereby helping the concentration and avoiding dispersions and/or doubts. A typical example is the situation of speaking on the phone, identified as being one of the most difficult for stutterers, in which the same question is put in three distinct ways in section lll: How difficult is it for you to communicate in these situations? Speaking on the phone in general/Using the phone at work/ Using the phone at home.
Most studies do not show any significant differences in the self-evaluation of stuttering for male and female stutterers (16-23), however, when more precise themes are studied differences can be identified.
A study done to determine the handicap caused by stuttering when seeking placement in the work environment, showed that men and ethnic and racial minorities were more susceptible to the disadvantage caused by stuttering than women and caucasians(24).
Despite it not being possible to establish an equivalence between the levels of severity attributed in the SSI-3 and in the self-evaluation proposed by OASES-A it is possible to determine a tendency of the individual classified under SSI-3 with severe and very severe degree of stuttering to show a less severe self-evaluation under OASES-A. In contrast, there is a tendency of those classified as having a mild degree under SSI-3 to show a more moderate degree in the OASES-A. There is nothing in any reference works which is conclusive about these findings.
It was noted that, within the health components, internal and/or external factors such as negative affective reactions, behavioral and cognitive, limitations in the participation in everyday activities and negative impact on the quality of life may be relevant for the stutterer. OASES-A allows visualisation of elements which may be integrated into the therapy for the stutterer , such as self-monitoring speech activities which enable the individual to make a more realistic analysis of his/her fluency at different points of the process, comparing it to that of fluent and nonfluent speakers along the whole programme.
It was also noted that it may be difficult for stutterers to say exactly what they want when they think they may stutter, and it is not uncommon for them to report that when they fear this might happen, they use a synonym or omit the word . This behaviour, however, is qualified by the speaker as being extremely unsettling, as if there had been na interruption in the thought process and the message frequently appears to be broken or inexact. This can be one of the reasons for the importance of the use of the confrontational techniques learned and/or developed by the person who stutters. It is generally believed that various procedures may be helpful allowing more time for the language planning and the motor execution, such as slowing down; a smooth beginning to the words; the production of consonants with relaxed articulators and a constant flow of air with the use of fricatives and slightly distorted stops; a phonoarticulatory sensorial feedback of the muscles of the tongue, lips and jaw which are crucial to the control of speech.(10,11)
The difference encountered in the present study between the perception of the capabilities of speaking and communicating may signify that the stutterer feels less at ease in a speaking situation than in a communication one in which other means such as gestures can be used to transmit the message. The high negative impression level related to being identified as someone who stutters and the variations in fluency in different situations are consistent with the difference. There may be a preference to use means of communication other than speech in an attempt to avoid being identified as a stutterer.
When dealing with the level of knowledge of stuttering, there are studies which point to a lack of knowledge of those individuals who attend(ed) self-help groups and benefit they may have gained from that (16,17). The implementation of programmes which favour the clarification and awareness about stuttering and its treatment is relevant, as are those which are held by official organisations and under the clinical auspices of a speech and language specialist.
In the question which deals specifically with the techniques of speech therapy there was a high level of satisfaction. It is not uncommon for a stutterer to receive the most diverse suggestions as to how to stop stuttering, many of them without any basis in clinical-theory, others extremely uncomfortable and sometimes, even bizarre.In a study about those elements judged relevant in overcoming and coping with disfluency, from the stutterer's point of view the conclusion was that the satisfaction generated by the therapy was one of the six themes mostly associated with the ability to manage and improve the stuttering.In the cases of dissatisfaction with the therapeutic process, inadequate therapy was one of the recurring themes of the stutterers(19). It is relevant that speech and language treatment supplies the stutterer with the techniques which will enable him/her to monitor speech thereby reducing the fear of speech and increasing self-confidence.
The reactions of stutterers to stuttering are the object of many studies.The fact that in this study, anxiety was the most cited emotional state is in line with the literature and clinical findings in which it appears as one of the mostly identified problems by stutterers.(10,11,25,26)
One of the factors related to the increase in anxiety and embarrassment referred to by stutterers is bullying(27,28). It means the use of power or force to persecute, humiliate, be dismissive of others, making victims of them. This is a phenomenon which is growing in the school and work environments and is causing concern amongst the educational and health authorities. Studies have been developed recently to analyse a possible relationship between the emotional states of anxiety and/or embarrassment, mentioned by stutterers ,and their vulnerability to bullying. Studies show that repeated negative experiences associated to stuttering provoke new attitudes in stutterers, including those which might be harmful to their social relationships(10,11,29) .
Communication in Daily Situations which demand a satisfactory communicative competence causes different levels of difficulty for the stutterer depending on the situation. In conversations in general situations, it can be seen that the degree of difficulty increases with the number of people involved. However the level of familiarity interferes directly, which shows that, for the stutterer,even in arguments, one of the most influential factors is the closeness of the bond with the other parties.
Besides, speaking on the telephone is one of the biggest complaints of the stutterer(10,11) and OASES-A permits a more detailed evaluation of this subject. Talking on the phone at work and in day-to-day situations is shown to be much more difficult than in the family environment. Normally in the working environment we deal with heirarchically superior individuals, clients and suppliers - situations which stutterers describe as being uncomfortable.
The factors described above ratify the importance of speech therapy strategies which simulate daily activities beginning in internal environment in the therapy room, and, subsequently moving to outside environment, generalizing new behavioural patterns and attitudes to situations which the stutterer used to identify as being the most difficult to cope with.
This study also showed handicap felt by the stutterers in questions intimately linked to the quality of life, such as self-esteem, self-confidence, enthusiasm for life and health in general as well as physical well-being. This finding agrees with the proposition that stuttering can affect more than just the ability of the person to produce the necessary fluency, as the qualiy of life is an important factor to be considered for its multidimensional characteristics(7-9,18,20-23,30).
Yet again on the subject of Quality of Life, the stutterer's own reactions and the reactions of the listener confronted with the discourse of the stutterer reveal one of the handicaps which directly affect the quality of life of the stutterer. Besides which, it reinforces the importance of making society aware of stuttering, which is being done through awareness and counselling campaigns run by various organizations related to Speech and Language.
CONCLUSION
The application of the translated and adapted to Brazilian Portuguese OASES-A to a population of adult stutterers enabled the verification of the instrument's capability of providing different and important focusses which go beyond the diseases and injuries, based on the body, the individual and the society, as proposed by the ICF. It can also be an auxiliary tool in the designing and follow-up of the therapeutic process of the stutterer, as it is possible to re-apply it periodically and compare the behaviour with that identified by other protocols.
The collection of data which includes the results of the treatment from the perspective of the stutterer can provide the necessary information in the evidence based practice in the field of speech fluency disorders.
Received: 5/17/2011
Accepted: 2/13/2012
Study conducted at the Department of Speech-Language Pathology and Audiology, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil
Conflict of interests: None
- 1. World Health Organization. International classification of functioning, disability and health. Geneva: World Health Organization; 2001.
- 2. Di Nubila HB, Buchalla CM. O papel das Classificações da OMS - CID e CIF nas definições de deficiência e incapacidade. Rev Bras Epidemiol. 2008;11(2):324-35.
- 3. de Andrade CR. A fonoaudiologia baseada em evidências. Einstein (São Paulo). 2004;2(1):59-60.
- 4. Kully D, Langeven M. Evidence-based practice in fluency disorders. ASHA Lead. 2005;18(23):10-1
-
5Organização Mundial da Saúde. Classificação estatística internacional de doenças e problemas relacionados à saúde, 10a rev. São Paulo: Centro Colaborador da OMS para a Classificação de Doenças em Português; 2008.
- 6. Yaruss JS. Describing the consequences of disorders: Stuttering and the International Classification of Impairments, Disabilities, and Handicaps. J Speech Lang Hear Res. 1998;41(2):249-57.
- 7. Yaruss JS, Quesal RW. Stuttering and the International Classification of Functioning, Disability, and Health: an update. J Commun Disord. 2004;37(1):35-52.
- 8. Yaruss JS, Quesal RW. Overall Assessment of the Speaker's Experience of Stuttering (OASES): documenting multiple outcomes in stuttering treatment J Fluency Disord. 2006;31(2):90-115.
- 9. Yaruss JS. Application of the ICF in fluency disorders. Semin Speech Lang. 2007;28(4):312-22.
- 10. Guitar B. Stuttering: an integrated approach to Its nature and treatment. 3Ş ed. Baltimore (MD): Lippincott Williams Wilkins; 2006.
- 11. Bloodstein O, Ratner BN. A handbook of stuttering. 6a ed. New York: Thomson Delmar Learning; 2008.
- 12. Riley GD. Stuttering severity instrument for children and adults. 3rd ed. Austin (TX): Pro-Ed; 1994.
- 13. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417-32.
- 14. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186-91.
- 15. da Mota Falcão D, Ciconelli RM, Ferraz MB. Translation and cultural adaptation of quality of life questionnaires: an evaluation of methodology. J Rheumatol. 2003;30(2):379-85.
- 16. Yaruss JS, Quesal RW, Reeves L, Molt LF, Kluetz B, Caruso AJ, et al. Speech treatment and support group experiences of people who participate in the National Stuttering Association. J Fluency Disord. 2002;27(2):115-33.
- 17. Yaruss JS, Quesal RW, Murphy B. National Stuttering Association members' opinions about stuttering treatment. J Fluency Disord. 2002;27(3):227-41.
- 18. Klompas M, Ross E. Life experiences of people who stutter, and the perceived impact of stuttering on quality of life: personal accounts of South African individuals. J Fluency Disord. 2004;29(4):275-305.
- 19. Plexico L, Manning WH, Dilollo A. A phenomenological understanding of successful stuttering management. J Fluency Disord. 2005;30(1):1-22.
- 20. de Andrade CR, Sassi FC, Juste FS, Ercolin B. Qualidade de vida em indivíduos com gagueira desenvolvimental persistente. Pró-Fono. 2008;20(4):219-24.
- 21. Craig A, Blumgart E, Tran Y. The impact of stuttering on the quality of life in adults who stutter. J Fluency Disord. 2009;34(2):61-71.
- 22. Bricker-Katz G, Lincoln M, McCabe P. A life-time of stuttering: how emotional reactions to stuttering impact activities and participation in older people. Disabil Rehabil. 2009;31(21):1742-52.
- 23. Yaruss JS. Assessing quality of life in stuttering treatment outcomes research: J Fluency Disord. 2010;35(3):190-202.
- 24. Klein JF, Hood SB. The impact of stuttering on employment opportunities and job performance J Fluency Disord. 2004;29(4):255-73.
- 25. Craig A, Hancock K, Tran Y, Craig M. Anxiety levels in people who stutter: a randomized population study. J Speech Lang Hear Res. 2003;46(5):1197-206.
- 26. Blumgart E, Tran Y, Craig A. Social anxiety disorder in adults who stutter. Depress Anxiety. 2010;7;27(7):687-92.
- 27. Furnham A, Davis S. Involvement of social factors in stuttering: a review and assessment of current methodology. Stammering Res. 2004;1(2):112-22.
- 28. Blood GW, Blood IM. Preliminary study of self-reported experience of physical aggression and bullying of boys who stutter: relation to increased anxiety. Percept Mot Skills. 2007;104(3 Pt 2):1060-6.
- 29. Iverach L, O'Brian S, Jones M, Block S, Lincoln M, Harrison E, et al. The five factor model of personality applied to adults who stutter. J Commun Disord. 2010;43(2):120-32.
- 30. Cummins RA. Fluency disorders and life quality: subjective wellbeing vs. health- related quality of life. J Fluency Disord. 2010;35(3):161-72.
Publication Dates
-
Publication in this collection
20 July 2012 -
Date of issue
2012
History
-
Received
17 May 2011 -
Accepted
13 Feb 2012