Abstracts
PURPOSE: To analyze the influence of weight, height and body mass index in the axial tongue force. METHODS: Medical records with data from 44 subjects aged between 20 and 37 years, 11 (25%) males and 33 (75%) female, were analyzed. The investigated information were weight, height, result of clinical evaluation for tongue force (lingual tonus) and instrumental assessment of axial tongue force, which was accomplished by using the FORLING. Data was statistically analyzed. RESULTS: No differences were observed between the force values regarding the variables body mass index classification and clinical classification of tongue force. Body mass index and weight had positive correlation with mean tongue force. There was a strong positive correlation between the variables mean force, maximum force and highest maximum force. CONCLUSION: Although body mass index and weight correlated positively with the mean axial tongue force, there was no association between body mass index classification and the axial tongue forces.
Tongue; Muscle strength; Biomechanics; Speech, language and hearing sciences; Body height; Body weight; Body mass index
OBJETIVO: Analisar a influência de peso, altura e índice de massa corporal na força axial da língua. MÉTODOS: Foram analisados os prontuários referentes a 44 indivíduos com idade entre 20 e 37 anos, sendo 11 (25%) homens e 33 (75%) mulheres. Foram pesquisadas as informações referentes a peso, altura, resultado da avaliação clínica da língua (tônus lingual) e resultado da avaliação instrumental da força axial da língua, sendo esta última realizada por meio do FORLING. Os dados foram analisados estatisticamente. RESULTADOS: Não foram observadas diferenças entre os valores de força em relação às variáveis de classificação do índice de massa corporal e avaliação clínica da língua. O índice de massa corporal e o peso apresentaram correlação positiva com a força média da língua. Verificou-se, ainda, correlação positiva forte entre as variáveis de força média, força máxima e maior força máxima da língua. CONCLUSÃO: Embora o índice de massa corporal e o peso se correlacionem de forma positiva com a força média axial da língua, não há associação entre a classificação do índice de massa corporal e as forças axiais da língua.
Língua; Força muscular; Biomecânica; Fonoaudiologia; Estatura; Peso corporal; Índice de massa corporal
ORIGINAL ARTICLE
IUndergraduate Program in Speech-Language Pathology and Audiology, Universidade Federal de Minas Gerais - UFMG - Belo Horizonte (MG), Brazil
IIGraduate Program (Doctorate degree) in Biomechanical Engineering, Department of Structural Engineering, Universidade Federal de Minas Gerais - UFMG - Belo Horizonte (MG), Brazil
IIIDepartment of Structural Engineering, Universidade Federal de Minas Gerais - UFMG - Belo Horizonte (MG), Brazil
IVDepartment of Speech-Language Pathology and Audiology, Universidade Federal de Minas Gerais - UFMG - Belo Horizonte (MG), Brazil
Correspondence address
ABSTRACT
PURPOSE: To analyze the influence of weight, height and body mass index in the axial tongue force.
METHODS: Medical records with data from 44 subjects aged between 20 and 37 years, 11 (25%) males and 33 (75%) female, were analyzed. The investigated information were weight, height, result of clinical evaluation for tongue force (lingual tonus) and instrumental assessment of axial tongue force, which was accomplished by using the FORLING. Data was statistically analyzed.
RESULTS: No differences were observed between the force values regarding the variables body mass index classification and clinical classification of tongue force. Body mass index and weight had positive correlation with mean tongue force. There was a strong positive correlation between the variables mean force, maximum force and highest maximum force.
CONCLUSION: Although body mass index and weight correlated positively with the mean axial tongue force, there was no association between body mass index classification and the axial tongue forces.
Keywords: Tongue. Muscle strength. Biomechanics. Speech, language and hearing sciences. Body height. Body weight. Body mass index
INTRODUCTION
The human tongue is a muscular organ that plays an important role in several functions of the oral sensorimotor system. This organ is composed of intrinsic and extrinsic muscles, arranged in such a way as to allow necessary multiple configurations for performing the functions of mastication, swallowing, suction and speech articulation(1).
The intrinsic muscles (superior longitudinal, inferior longitudinal, verticalis and transversus) are proper to the tongue and responsible for changes of its shape. The extrinsic muscles (genioglossus, styloglossus, palatoglossus and hyoglossus) are those originated from adjacent structures and are included in the tongue, which allows it to move in all directions. It is due to its extensive innervation and to the complex organization of muscle fibers that the tongue takes many forms and positions in short periods of time(1).
The maximum force of the tongue in normal individuals has been documented by several studies(2-5). In some studies this force is measured by means of the movement of protrusion against resistance(2,6-10). Such movement involves the contraction of the genioglossus and the intrinsic muscles of the tongue, the first being more important for the anteroposterior positioning and the last ones for the generation of protrusive force(11).
Tongue force is related, in most studies, to the age and gender of individuals. Studies have found that the tongue force decreases with the increase in age from 60 years on(12-14). Regarding the gender, the relationship is still controversial. Some studies found greater force in men(2,6,13,15-17). However, in other studies such difference was not observed(12,14,18-22).
The influence of weight, height and body mass index (BMI) on tongue strength has been little studied. Most research on the height and weight as determinants of muscle strength study the muscles of other parts of the body and not specifically the tongue ones(23). Some studies have considered these aspects to basically perform the match between the surveyed groups, assuming therefore to be the responsible parameters for differences between groups(24,25). Others have investigated the existence of correlation between body mass index and tongue force and reached different results(20,24,26). In some studies, it was found a correlation between the maximum tongue force and body mass index(20,24), while others have found no correlation between these variables(26).
Given the scarcity of studies on the influence of some variables on the lingual force, this research aimed to analyze the interference of weight, height and body mass index in the axial tongue force.
METHODS
The study, approved by the Ethics in Research Committee of Universidade Federal de Minas Gerais (UFMG) under number 249/08, was held at the Faculty of Medicine at the same institution. This is a cross-sectional and observational research, performed through analysis of medical records of 44 students and staff of the institution, aged between 20 and 37 years, 33 (75%) women and 11 (25%) men.
The study included medical records that contained age, weight, height, result of clinical evaluation of tongue strength (lingual tonus), result of the instrumental assessment of the axial tongue force and signing of the consent form authorizing the use of the information in the research. The assessment of weight and height was accomplished with participants barefoot. For the weighing it was used a Camry® brand scale and, for the measuring of height, a measuring tape attached to the wall. From these data it was calculated the body mass index of each individual by dividing weight by the square of height. Individuals were classified as underweight (less than 18.5), healthy (from 18.5 to 24.9), overweight (from 25 to 29.9) and obese (above 30)(27).
In the clinical evaluation it was obtained the tongue tonus, which was classified as adequate or decreased. The evaluation was performed by observing the ability of the tongue to achieve and sustain tapering, of the movement and sound produced during a snap and the protrusion test of the structure with counter resistance, i.e., the participant was asked to push the tongue against the examiner's gloved finger and against a wooden spatula. It was considered appropriate tonus when the patient kept with no difficulty the tapering of the tongue, produced a loud snap and symmetrical movement of the tongue, as well as when the muscle was able to perform the protrusion with force against a steady resistance, performed by the spatula and by the finger, keeping this force without trembling and without deformation. The tonus was considered reduced when the participant had difficulty to perform the tapering of the tongue, or produced low snap or asymmetrical movement of the tongue in the task, or when there was the presence of tremors and/or deformation during counter resistance even though the muscle was able to perform protrusion.
In the instrumental assessment of the axial tongue force, data on the mean force and maximum force of this organ were obtained. The evaluation was performed using FORLING, an instrument developed by the Group of Biomechanics Engineering, Universidade Federal de Minas Gerais (7-10,28).
The evaluation was performed with the person seated with supported back and feet, and hands resting on the base of the equipment. After proper fitting of the mouthpiece in the dental arches, an accommodation period of about 20 seconds was awaited. After this time, the individual was asked to push the drive shaft of the piston with the tongue after the beep, with the greatest capable force, and to keep it until hearing another acoustic signal, scheduled to be activated 10 seconds later. This procedure was performed three more times, with one minute intervals between measurements and verbal positive reinforcement in each measurement. The first measurement (training) was disregarded.
The mean force and maximum force of the tongue of each evaluated participant were analyzed. The mean force refers to the mean of all the forces employed by that individual during the three measurements and the maximum force refers to the mean of the highest values obtained in each measurement. The highest maximum force achieved by the participant was also considered.
Body mass index, height, weight and clinical evaluation of the tongue tonus were correlated with mean force, maximum force and the highest maximum force. Lingual force variables were also correlated among each other. For data analysis it was used measures of central tendency and dispersion, as well as ANOVA test and Pearson correlation coefficient, with a significance level of 5%.
In the literature, some studies have found a relationship between increasing of age and decreasing of tongue force(2,14-16,18). However, the strength reduction only occurs after age 60(12-14) justifying the non stratification of the sample by age.
RESULTS
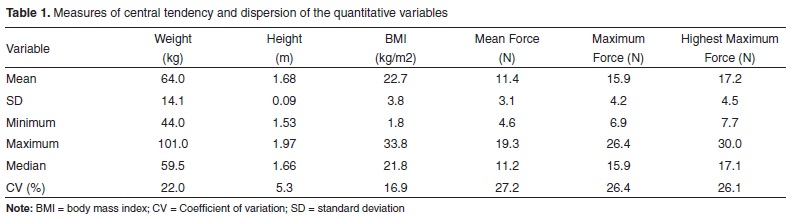
Results of quantitative variables of the study were obtained (Table 1). It is possible to observe that the lowest coefficient of variation was found in the variable height and the highest ones on measures of tongue force. However, in the measurement of weight, high value of coefficient of variation could also be verified.
The force data found in accordance with the classification of body mass index and tongue tonus were also obtained (Table 2). The force values did not show differences between individuals with normal and reduced tongue tonus. There was also no difference in the force values between the different BMI categories.
It was observed the correlation between quantitative variables of the study (Table 3). BMI and weight showed positive correlation with the mean force and the body height did not show correlation with the axial tongue force. All variables of force correlated with each other.
DISCUSSION
The search for studies that scientifically prove what factors can affect tongue strength has been growing in recent years. The knowledge of these factors is of great importance, because changes in the tongue force can cause problems in the performance of the various functions in which this structure is involved.
The instrumental evaluation of tongue force, although uncommon in speech therapy clinical practice, has been gaining ground every day as a means of supplementing the orofacial myofunctional evaluation, since it is sensitive for detecting small increments of the force resulting from the rehabilitation process (which increases the patient adherence to treatment), as well as to detect decreases in strength due to degenerative diseases. However there are only few studies that show values of lingual force for the Brazilian population, and the variables BMI, weight and height are not always considered.
Regarding the tonus of the tongue, which was classified as normal or reduced through clinical evaluation, it was possible to observe that the mean values of the groups showed no differences for all variables of force. The concordance between the findings of the clinical and instrumental evaluations of tongue force has been demonstrated in studies that used FORLING for both mean and maximum forces(21,28), suggesting that the method used in the research would be effective in the clinical application and could be used to complement the diagnosis of alterations of tongue force. However, one study(21) investigated extreme groups: individuals with normal tongue tonus and individuals with serious reduction of tongue tonus. But in another one(28) it was not performed statistical analysis to check this aspect. Further research with larger samples and independent evaluators are needed to verify how the instrumental assessment of tongue strength is able to classify individuals according to the presence of alteration of lingual tonus.
No difference was observed between the force values of individuals with different BMI classifications. However, when analyzing the correlation among the quantitative variables of the study, it was found that BMI showed positive correlation with the variable mean force. Positive correlation was also found between weight and mean force.
In some studies it was observed the correlation between the highest maximum force and maximum pressure of the tongue, respectively, and body mass index(20,24). The mean force was not considered in these studies. In one study, the authors measured the maximum pressure held by the tongue of 26 adults between 20 and 49 years (five men and 21 women) and six children, aged 6 to 12 years (four males and two females), and related the values of the highest maximum pressure with the weight of the individuals. The authors found a positive correlation, although weak, between maximum pressure of the tongue and body weight, and the maximum pressure exerted by a child of 25 Kgf did not differ radically from that exerted by an adult of 80 Kgf. Unlike, the hand strength showed a strong positive correlation two times higher than tongue strength(29).
The variable height did not show correlation with the axial tongue force. A study achieved with children found that those with higher age, height and weight (alone or in combination) showed higher strength in six muscle groups of the lower limbs, and the height was the strongest predictor of the strength compared to the age or weight(23). However there is no research on the influence of body height in the tongue force.
It was verified strong correlation between the variables related to the mean force, maximum force and the highest maximum force. This means, for example, that the individuals who showed high values of maximum force also had higher values of mean force and high peak of maximum force. It was possible to think that individuals who produced a high maximum force in one of the tests would not be able to maintain a proper muscle contraction during the 10 seconds of the test due to muscle fatigue. However, this was not observed. The strong correlation between these variables also indicates that it is not necessary the achievement of the three during the evaluation. The quantification of one of them is already sufficient to characterize the axial force of the tongue.
Some limitations could be verified during the development of this work, in particular the reduced sample size and its non-homogeneous distribution in the different groups for analysis by BMI and tongue tonus. It is noteworthy that the distribution of the population of this study in the different BMI categories is compatible with the one of Brazilian population(30).
CONCLUSION
Although BMI and weight correlated positively with the mean axial tongue force, there was no association between BMI classification and the axial tongue forces.
ACKNOWLEDGEMENTS
To the partnership FUNDEP/Santander for scientific initiation scholarship granted to the first author, under case number 165409.
REFERENCES
- 1. Zemlin W. Princípios de anatomia e fisiologia em Fonoaudiologia. 4ªed. Porto Alegre: Artes Médicas; 2000.
- 2. Mortimore IL, Fiddes P, Stephens S, Douglas NJ. Tongue protrusion force and fatigability in male and female subjects. Eur Resp J. 1999;14(1):191-5.
- 3. Sha BF, England SJ, Parisi RA, Strobel RJ. Force production of the genioglossus as a function of muscle length in normal humans. J Appl Physiol. 2000;88(5):1678-84.
- 4. Clark HM, O'brien K, Calleja A, Corrie SN. Effects of directional exercise on lingual strength. J Speech Lang Hear Res. 2009;52(4):1034-47.
- 5. Vitorino, J. Effect of age on tongue strength and endurance scores of healthy Portuguese speakers. Int J Speech Lang Pathol. 2010;12(3):237-43.
- 6. Dworkin JP, Aronson AE, Mulder DW. Tongue force in normals and dysarthric patients with amyotrophic lateral sclerosis. J Speech Hear Res. 1980;23(4):828-37.
- 7. Motta AR, Perim JV, Perilo TV, Las Casas EB, Costa CG, Magalhães FE, et al. Método objetivo para a medição de forças axiais da língua. Rev CEFAC. 2004;6:164-9.
- 8. Barroso MF, Costa CG, Saffar JM, Las Casas EB, Motta AR, et al. Desenvolvimento de um sistema protótipo para medição objetiva das forças linguais em humanos. Sba Controle & Automação. 2009;20(2):156-63.
- 9. Furlan RM, Valentim AF, Perilo TV, Costa CG, Barroso MF, et al. Quantitative evaluation of tongue protrusion force. Int J Orof Myol. 2010;36:33-43.
- 10. Motta AR, César CC, Bommarito S, Chiari BM. Força axial de língua em diferentes faixas etárias. J Soc Bras Fonoaudiol. 2011;23(3):201-5.
- 11. Pittman LJ, Bailey EF. Genioglossus and intrinsic electromyographic activities in impeded and unimpeded protrusion tasks. J Neurophysiol. 2009;101(1):276-82.
- 12. McAuliffe MJ, Ward EC, Murdoch BE, Farrell AM. A nonspeech investigation of tongue function in Parkinson's disease. J Gerontol A Biol Sci Med Sci. 2005;60(5):667-74.
- 13. Stierwalt JA, Youmans SR. Tongue measures in individuals with normal and impaired swallowing. Am J Speech Lang Pathol. 2007;16(2):148-56.
- 14. Youmans SR, Youmans GL, Stierwalt JAG. Differences in tongue strength across age and gender: is there a diminished strength reserve? Dysphagia. 2009;24(1):57-65.
- 15. Crow HC, Ship JA. Tongue strength and endurance in different aged individuals. J Gerontol A Biol Sci Med Sci. 1996;51(5):247-50.
- 16. Utanohara Y, Hayashi R, Yoshikawa M, Yoshida M, Tsuga K, Akagawa Y. Standard values of maximum tongue pressure taken using newly developed disposable tongue pressure measurement device. Dysphagia. 2008;23(3):286-90.
- 17. Trawitzki LV, Borges CG, Giglio LD, Silva JB. Tongue strength of healthy young adults. J Oral Rehabil. 2011;38(7):482-6.
- 18. Hayashi R, Tsuga K, Hosokawa R, Yoshida M, Sato Y, Akagawa Y. A novel handy probe for tongue pressure measurement. Int J Prosthodont. 2002;15(4):385-8.
- 19. Clark HM, Henson PA, Barber WD, Stierwalt JA, Sherrill M. Relationships among subjective and objective measures of the tongue strength and oral phase swallowing impairments. Am J Speech Lang Pathol. 2003;12(1):40-50.
- 20. Yoshida M, Kikutani T, Tsuga K, Utanohara Y, Hayashi R, Akagawa Y. Decreased tongue pressure reflects symptom of dysphagia. Dysphagia. 2006;21(1):61-5.
- 21. Furlan RM, Avaliação quantitativa da força axial da língua em indivíduos com grave diminuição da força lingual [trabalho de conclusão de curso de graduação]. Belo Horizonte: Faculdade de Medicina da Universidade Federal de Minas Gerais; 2008.
- 22. Lambrechts H, De Baets E, Fieuws S, Willems G. Lip and tongue pressure in orthodontic patients. Eur J Orthod. 2010;32(4):466-71.
- 23. Macfarlane TS, Larson CA, Stiller C. Lower extremity muscle strength in 6- to 8-year-old children using hand-held dynamometry. Pediatr Phys Ther. 2008;20(2):128-36.
- 24. Mortimore IL, Bennett SP, Douglas NJ. Tongue protrusion strength and fatiguability: relationship to apnoea/hypopnoea index and age. J Sleep Res. 2000;9(4):389-93.
- 25. Potter NL, Short R. Maximal tongue strength in typically developing children and adolescents. Dysphagia. 2009;24(4):391-7.
- 26. Blumen MB, Perez de La Sota A, Quera-Salva MA, Frachet B, Chabolle F, Lofaso F. Genioglossal electromyogram during mantained contraction in normal humans. Eur J Appl Physiol. 2002;88(1-2):170-7.
-
27WHO. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation on obesity. Geneva, 1998.
- 28. Perilo TV, Motta AR, Las Casas EB, Saffar JM, Costa CG. Avaliação objetiva das forças axiais produzidas pela língua de crianças respiradoras orais. Rev Soc Bras Fonoaudiol. 2007;12(3):184-90.
- 29. Robin DG, Somodi LB, Luschei ES. Measurement of tongue strength, endurance in normal and articulation disordered subjects.In: Moore CA, Yorkston KM, Beukelman DR (org). Dysarthria and apraxia of speech: perspectives on management. Baltimore: Brookes; 1991. p. 173-84.
- 30. Acuña K, Cruz T. Avaliação do estado nutricional de adultos e idosos e situação nutricional da população brasileira. Arq Bras Endocrinol Metabol. 2004;48(3):345-61.
Influence of height, weight and body mass index in the axial tongue force
Publication Dates
-
Publication in this collection
07 Jan 2013 -
Date of issue
2012
History
-
Received
15 Mar 2012 -
Accepted
13 Aug 2012