Abstracts
INTRODUCTION: Transanal endoscopic microsurgery is a technique created in the 1980's for resections of rectal tumors. This technique is a good option for the resections of rectal tumors, with low morbidity and mortality. OBJECTIVE: To report the initial experience of two different services in the Brazilian Northeast, Bahia and Pernambuco. METHODS: Retrospective and descriptive data collected from January 2010 to June 2012 regarding the postoperative outcomes of patients who underwent transanal endoscopic microsurgery for rectal tumor resection in these services. RESULTS: Our initial experience consisted of 52 patients, being 59.6% males; 71.2% were benign diseases, and the mean distance from the anal margin was 5.6 cm. Mean hospital stay was 1.2 days. Complications included bleeding, perforation and entry to the abdominal cavity in three cases, as well as suture dehiscence and neoplasm recurrence in an advanced adenocarcinoma. CONCLUSION: Transanal endoscopic microsurgery is an excellent technical option for the resection of rectum adenomas, which are not feasible for endoscopic resection. The procedure may be used for other indications, as the resection of anal fistulae, being an useful instrument in colorectal surgery.
TEM; adenocarcinoma; rectal neoplasms
INTRODUÇÃO: A microcirurgia endoscópica transanal é uma técnica minimamente invasiva criada nos anos de 1980 para ressecção local de tumores retais. Essa técnica tem se mostrado uma boa opção para as ressecções de tumores retais, com morbidade baixa e mortalidade praticamente nula. OBJETIVO: Relatar a experiência inicial de dois serviços localizados no Pernambuco e na Bahia, Nordeste do Brasil. MÉTODOS: Estudo retrospectivo e descritivo realizado de janeiro de 2010 a junho de 2012 dos resultados pós-operatórios de pacientes submetidos à microcirurgia endoscópica transanal nestes dois serviços. RESULTADOS: Cinquenta e dois pacientes consecutivos submetidos a tratamento cirúrgico por meio de TEM foram revisados, 59,6% dos quais eram do sexo masculino. Em 71,2% dos casos, o procedimento foi realizado para lesões benignas, e a distância média dos tumores da borda anal foi de 5,6 cm. A média do período de internação foi de 1,2 dias. Das complicações encontradas, podemos citar sangramento, perfuração e entrada na cavidade abdominal em três casos, bem como deiscência de sutura e recidiva tumoral em um adenocarcinoma avançado. CONCLUSÃO: A microcirurgia endoscópica transanal é uma excelente alternativa técnica para os casos de ressecção de adenomas de reto que não são possíveis por colonoscopia. O procedimento pode ser utilizado em outras indicações, como a ressecção de fístulas anais, mostrando-se um instrumental útil na cirurgia colorretal.
TEM; adenocarcinoma; neoplasias retais
ORIGINAL ARTICLE
Transanal endoscopic microsurgery (TEM): initial experience
Carlos Ramon Silveira MendesI; Luciano Santana de Miranda FerreiraII; Ricardo Aguiar SapucaiaI; Meyline Andrade LimaI; Sergio Eduardo Alonso AraujoIII; Mauricio Jose de Matos e SilvaIV; Jose Figueiroa FilhoIV; Joaquim Herbenildo Costa CarvalhoIV; Maurilio Toscano de LucenaIV; Orcina Fernandes DuarteIV; Raquel Kelner SilveiraIV; Anna Christina Cordeiro da SilvaIV; Carolina Araujo GuenesV
IDoctor at the Coloproctology Service of Hospital Santa Izabel da Santa Casa de Misericórdia da Bahia Salvador (BA), Brazil; Associate Member of the Brazilian Society of Coloproctology Rio de Janeiro (RJ), Brazil
IIHead of the Coloproctology Service at Hospital Santa Izabel da Santa Casa de Misericórdia da Bahia Salvador (BA), Brazil; Titular at the Brazilian Society of Coloproctology Rio de Janeiro (RJ), Brazil
IIITitular at the Brazilian Society of Coloproctology Rio de Janeiro (RJ), Brazil
IVDoctor at the Coloproctology Service of Hospital Barão de Lucena Recife (PE), Brazil; Titular at the Brazilian Society of Coloproctology Rio de Janeiro (RJ), Brazil
VDoctor of the Coloproctology Service of Hospital Barão de Lucena Recife (PE), Brazil
Correspondence to Correspondence to: Carlos Ramon Silveira Mendes Rua São Domingos Savio, 150 Nazaré CEP: 40050-520 Salvador (BA), Brazil E-mail: proctoramon@hotmail.com
ABSTRACT
INTRODUCTION: Transanal endoscopic microsurgery is a technique created in the 1980's for resections of rectal tumors. This technique is a good option for the resections of rectal tumors, with low morbidity and mortality.
OBJECTIVE: To report the initial experience of two different services in the Brazilian Northeast, Bahia and Pernambuco.
METHODS: Retrospective and descriptive data collected from January 2010 to June 2012 regarding the postoperative outcomes of patients who underwent transanal endoscopic microsurgery for rectal tumor resection in these services.
RESULTS: Our initial experience consisted of 52 patients, being 59.6% males; 71.2% were benign diseases, and the mean distance from the anal margin was 5.6 cm. Mean hospital stay was 1.2 days. Complications included bleeding, perforation and entry to the abdominal cavity in three cases, as well as suture dehiscence and neoplasm recurrence in an advanced adenocarcinoma.
CONCLUSION: Transanal endoscopic microsurgery is an excellent technical option for the resection of rectum adenomas, which are not feasible for endoscopic resection. The procedure may be used for other indications, as the resection of anal fistulae, being an useful instrument in colorectal surgery.
Keywords: TEM; adenocarcinoma; rectal neoplasms.
RESUMO
INTRODUÇÃO: A microcirurgia endoscópica transanal é uma técnica minimamente invasiva criada nos anos de 1980 para ressecção local de tumores retais. Essa técnica tem se mostrado uma boa opção para as ressecções de tumores retais, com morbidade baixa e mortalidade praticamente nula.
OBJETIVO: Relatar a experiência inicial de dois serviços localizados no Pernambuco e na Bahia, Nordeste do Brasil.
MÉTODOS: Estudo retrospectivo e descritivo realizado de janeiro de 2010 a junho de 2012 dos resultados pós-operatórios de pacientes submetidos à microcirurgia endoscópica transanal nestes dois serviços.
RESULTADOS: Cinquenta e dois pacientes consecutivos submetidos a tratamento cirúrgico por meio de TEM foram revisados, 59,6% dos quais eram do sexo masculino. Em 71,2% dos casos, o procedimento foi realizado para lesões benignas, e a distância média dos tumores da borda anal foi de 5,6 cm. A média do período de internação foi de 1,2 dias. Das complicações encontradas, podemos citar sangramento, perfuração e entrada na cavidade abdominal em três casos, bem como deiscência de sutura e recidiva tumoral em um adenocarcinoma avançado.
CONCLUSÃO: A microcirurgia endoscópica transanal é uma excelente alternativa técnica para os casos de ressecção de adenomas de reto que não são possíveis por colonoscopia. O procedimento pode ser utilizado em outras indicações, como a ressecção de fístulas anais, mostrando-se um instrumental útil na cirurgia colorretal.
Palavras-chave: TEM; adenocarcinoma; neoplasias retais.
INTRODUCTION
The transanal endoscopic microsurgery (TEM) is a minimally invasive surgical technique introduced in the 1980s by Dr. Gerhard Buess, which enables the excision of rectal neoplasms with excellent exposure of the surgical field and minimum morbidity1-3.
In the lower third of the rectum, the endoanal resection is among the classic surgical techniques employed to treat rectal neoplasm4,5. This technique presents difficulties concerning the control of resection margins, hemostasis, full-thickness resection of the rectal wall, and also regarding the definition of the proximal margin. In the medium third, Mason's transsphincteric-transrectal approach has become obsolete due to its high morbidity and anal incontinence. Kraske procedure enables the access to the upper third of the rectum, but it has also been neglected due to poor results and high morbidity6. The alternative to these techniques for major adenomatous lesions used to be the low anterior resection or abdominoperineal resection, which present with high morbidity and mortality3,7. On the other hand, TEM leads to less complications in comparison to other technoques, also reducing hospital stay1,8.
TEM is performed with a rectoscope (Figure 1) measuring approximately 15 cm in length and 4 cm in diameter. This set is introduced in the anus, after dilation, and placed in the rectum according to the location and height of the lesion. With the rectoscope, it is possible to perform dissection by using curved instruments in its distal portion due to the its broad view9,10. TEM makes it possible to magnify the image of the lesion with endoscopic view, thus improving the visualization of the neoplasm. When performing pneumorectum with the equipment, it is possible to obtain a better definition of the margins of the lesion, which facilitates the use of instruments and manipulation. Therefore, it is possible to remove the whole specimen, which will then be analyzed by the pathologist.
Moore et al.5 demonstrated that the fragmentation of the specimen and compromised surgical margins occurred in 35 and 29% of the cases, respectively, when the conventional endoanal resection was performed. In that same study, it was observed that such values decreased to 6 and 10% with TEM, also showing reduced rates of local recurrence with this technique (24% versus 4%).
TEM has been more and more used for other procedures other than the resection of rectal tumors, as shown by Zoller et al.11, who performed the resection of retrorectal tumor. Another option for using TEM is the correction of stenosis in colorectal anastomoses12.
OBJECTIVE
The aim of this article was to demonstrate the initial experience with transanal endoscopic microsurgery performed by two teams of the Northeast of Brazil (Bahia and Pernambuco) during two years.
METHOD
All patients who underwent TEM for benign and malignant neoplasms in Salvador (Bahia) and Recife (Pernambuco), from January 2010 to June 2012, were included. These patients were retrospectively reviewed and analyzed regarding demographic data such as age, gender, distance from the anal verge and type of resected lesion. Complications related to the procedure, both during surgery and postoperatively, were evaluated.
The available long-term results of patients were also reported, such as neoplasm recurrence and appropriate treatment.
RESULTS
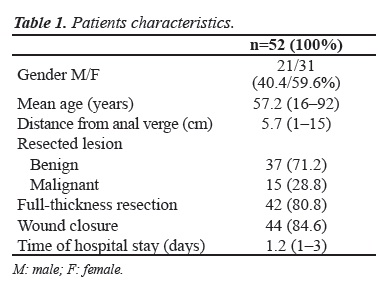
Fifty-two patients who underwent TEM for resection of benign and malignant lesions were included. Most procedures were performed to treat benign disease (71.2%). General characteristics of the patients included are demonstrated in Table 1. The preoperative pathology submitted to surgical resection was benign in 71.2% of the cases, and 28.8% accounted for malignant lesions. The full-thickness resection was performed in 80.8% of the procedures, and partial-thickness resection or mucosectomy, in 19.2%. The closure of the rectal wall was performed in 84.6% of the lesions, not being carried out in eight cases due to the difficulty caused by the proximity to the anal verge, aiming not to cause tissue tension, and in cases of mucosectomy of small diameter lesions.
Nine cases (17.3%) presented with intraoperative and postoperative complications, Two patients had bleeding (3.8%), solved during surgery, and three patients (5.8%) had perforation and entry into the abdominal cavity. In two of the latter we performed transanal primary closure. In the other one, the patient was already diverted with a colostomy and a laparoscopic approach was performed to assess the defect. Perineal sepsis was reported in one case (1.9%), and it was treated with antibiotics. Wound dehiscence was observed postoperatively in three patients (5.8%). No other complications were reported during the surgical procedure and at the initial follow-up (Table 2).
Recurrence of benign lesions was demonstrated in two cases, which were submitted to new resection by TEM. In one patient with rectal adenocarcinoma who refused undergoing radical surgery, local resection by TEM was performed, and she presented with local recurrence eight months after surgery, not accepting other treatments.
DISCUSSION
The studied population does not differ much from the literature. As to gender, it has been observed that mostly females undergo TEM, ranging from 51 to 65%5,8,10,13,14. In our population, the prevalence was of 59.6% (Figure 2), and this correlation was not associated with any specific characteristic of patients who underwent this treatment. We observed that the mean age (57.1 years old) was apparently lower than of the age seen in the literature (Figure 3). Regarding the distance of the lesion from the anal verge, our mean distance was 5.7 cm, similar to the population studied by Barendse et al.10, which presented with an average of 6 cm. Gonzalez et al.14 reported a mean distance of 9.1 cm (Figure 4). The distance of the lesion to the anal verge is probably related to the rates of peritoneal invasion. However, this was not the objective of this study.
TEM proved to be a safe technique with low rates of severe complications. In our study, the total complication rate was 17.3%, regardless of the etiology of the resected lesion. It is a known fact that patients with malignant neoplasm submitted to neoadjuvant chemotherapy and radiotherapy, followed by TEM, present with higher complication rates than those with no previous treatment15. The indication of TEM for malignant neoplasm should be highly selective, since there is no lymph node resection, which might compromise the final oncologic result.
In the study by Gonzalez et al.14, the percentage of patients with benign lesion submitted to TEM was 72.8%, which is very similar to our results (71.2%). This same study reported the complication rate after TEM including rectovaginal fistula in 3% and perforation associated with entry into the abdominal cavity in 6.1%, which is similar to our study, especially in lesions located 10 cm above the anal verge. The recurrence of a rectal lesion previously resected by TEM does not contraindicate the recommendation of the same method to treat the recurrence, as observed in this sample, apparently without increasing the complication rate. Due to the restricted number of patients in this sample who were submitted to re-resection by TEM, the evaluation of complications could not be objectively assessed.
Guerrieri et al.8 reported a median time of hospital stay of 3.5 days, more than our median hospital stay of 1.2 days (1 to 3 days). This study8, with 590 patients, also reported two rectovaginal fistula requiring diversion ostomy, complication not seen in our sample.
CONCLUSION
The transanal endoscopic microsurgery is a safe procedure with low morbidity and pratically null mortality. This technique can be an excellent alternative to resect benign rectal adenomas and neuroendocrine tumors placed in the rectum. For the adenocarcinoma, new studies should be analyzed in order to better define it indication instead of performing a total mesorectal excision, and also the role of neoadjuvant and adjuvant treatment associated with the resection of malignant rectal tumors. Nonetheless, TEM is a very powerful tool whose indications may include other anorectal pathologies, besides benign and malignant rectal tumors.
Submitted on: 01/09/2012
Approved on: 01/02/2013
Study carried out at the Hospital Santa Izabel of Santa Casa de Misericórdia da Bahia Salvador (BA), Brazil, and at Hospital Barão de Lucena Recife (PE), Brazil.
Financing source: none.
Conflict of interest: nothing to declare.
- 1. Buess G, Mentges B, Manncke K, Starlinger M, Becker HD. Technique and results of transanal endoscopic microsurgery in early rectal cancer. Am J Surg 1992;163:63-9; discussion 9-70.
- 2. Cataldo PA, O'Brien S, Osler T. Transanal endoscopic microsurgery: a prospective evaluation of functional results. Dis Colon Rectum 2005;48:1366-71.
- 3. Atallah S, Albert M, Larach S. Transanal minimally invasive surgery: a giant leap forward. Surg Endosc 2010;24:2200-5.
- 4. Endreseth BH, Wibe A, Svinsas M, Marvik R, Myrvold HE. Postoperative morbidity and recurrence after local excision of rectal adenomas and rectal cancer by transanal endoscopic microsurgery. Colorectal Dis 2005;7:133-7.
- 5. Moore JS, Cataldo PA, Osler T, Hyman NH. Transanal endoscopic microsurgery is more effective than traditional transanal excision for resection of rectal masses. Dis Colon Rectum 2008;51:1026-30; discussion 30-1.
- 6. Nahas SC, Nahas CSR, Marques CFS, Dias AR, Pollara WM, Cecconello I. Transanal endoscopic microsurgery (TEM): A minimally invasive procedure for treatment of selected rectal neoplasms. Arq Bras Cir Dig 2010;23:35-9.
- 7. Lezoche G, Baldarelli M, Guerrieri M, Paganini AM, De Sanctis A, Bartolacci S, et al. A prospective randomized study with a 5-year minimum follow-up evaluation of transanal endoscopic microsurgery versus laparoscopic total mesorectal excision after neoadjuvant therapy. Surg Endosc 2008;22:352-8.
- 8. Guerrieri M, Baldarelli M, Morino M, Trompetto M, Da Rold A, Selmi I, et al. Transanal endoscopic microsurgery in rectal adenomas: experience of six Italian centres. Dig Liver Dis 2006;38:202-7.
- 9. Middleton PF, Sutherland LM, Maddern GJ. Transanal endoscopic microsurgery: a systematic review. Dis Colon Rectum 2005;48:270-84.
- 10. Barendse RM, Doornebosch PG, Bemelman WA, Fockens P, Dekker E, de Graaf EJ. Transanal employment of single access ports is feasible for rectal surgery. Ann Surg 2012;256:1030-3.
- 11. Zoller S, Joos A, Dinter D, Back W, Horisberger K, Post S, et al. Retrorectal tumors: excision by transanal endoscopic microsurgery. Rev Esp Enferm Dig 2007;99:547-50.
- 12. Moraes RS, Buess G, Lima JHF, Morgenstern AG, Campos ACL, Coelho JCU, et al. Transanal endoscopic microsurgery (TEM) in the treatment of postoperative colorectal stenosis. Arq Bras Cir Dig 2008;21:147-9.
- 13. de Graaf EJ, Doornebosch PG, Tetteroo GW, Geldof H, Hop WC. Transanal endoscopic microsurgery is feasible for adenomas throughout the entire rectum: a prospective study. Dis Colon Rectum 2009;52:1107-13.
- 14. Gonzalez JEB, Zulueta AF, Alfonso MAM, Díaz OFC, Faife BF, Hernández JMG, et al. Cuban experience and the future perspectives of transanal endoscopic microsurgery. Rev Cubana Cir 2009;48.
- 15. Perez RO, Habr-Gama A, Sao Juliao GP, Proscurshim I, Scanavini Neto A, Gama-Rodrigues J. Transanal endoscopic microsurgery for residual rectal cancer after neoadjuvant chemoradiation therapy is associated with significant immediate pain and hospital readmission rates. Dis Colon Rectum 2011;54:545-51.
Correspondence to:
Publication Dates
-
Publication in this collection
02 July 2013 -
Date of issue
Dec 2012
History
-
Received
01 Sept 2012 -
Accepted
01 Feb 2013