Abstract
Introduction
The study is aimed to outline the vector of colorectal cancer incidence in the industrial Aktobe province of western Kazakhstan through the first decade of the screening implementation, 2009–2018.
Methods
Rough incidence rates and annual percent changes were estimated for each age group at diagnosis, ethnicities, gender, residences, the disease stages and anatomic subsites (total N 1128) via regression analysis.
Results
Within 2009–2018 colorectal cancer rates increased from 14.74 to 23.19, with annual percent changes of 4.69%. The most significant growth was traced in men compared to women, up to 28.39 by 2018, with annual percent changes 6.64% vs. 2.64% (p = 0.0009). Annual percent changes in Kazakhs reached 8.7%, whereas Slavic groups showed decline in the incidence, annual percent changes −4.3% (p = 0.002). Declining in rates was also observed in urban population compared to rural one, annual percent changes −3.3% vs. 17.6%, respectively. Patients aged 60–69 made 31% of all cases and showed the largest annual percent changes 9.37% (p = 0.002). Patients at Stage II made 61% of all observations, but general trend evidenced sharp growth in the group of Stage I (annual percent changes 28.91%, p < 0.0001).
Conclusion
Overall, during the last decade colorectal cancer incidence increased 1.5 fold with expected further rise. However, the increment of Stage I portion by 2018 vs. advanced stages at diagnosis and the trend to decrease in rates among urban population inspire a definite assurance in potential efficiency of the screening program in long run. The next researches on colorectal cancer should include scenarios to reveal the role of disadvantaged environment in the region and consuming unhealthy ultra-processed food.
Keywords:
Colorectal carcinoma; Kazakhstan; Incidence rates; Prognosis
Resumo
Introdução
O objetivo do estudo é delinear o vetor da incidência do câncer colorretal na província industrial de Aktobe, no oeste do Cazaquistão, durante a primeira década da implementação do rastreamento, 2009‒2018.
Métodos
Taxas de incidência brutas e alterações percentuais anuais foram estimadas para cada faixa etária ao diagnóstico, etnias, sexo, residências, estágios da doença e localizações anatômicas (N total de 1.128) através da análise de regressão.
Resultados
Entre 2009‒2018, as taxas de câncer colorretal aumentaram de 14,74 para 23,19, com alteração percentual anual de 4,69%. O crescimento mais significativo foi evidenciado em homens em comparação com as mulheres, até 28,39 em 2018, com alterações percentuais anuais de 6,64% contra 2,64% (p = 0,0009). Alterações percentuais anuais nos cazaques atingiu 8,7%, enquanto os grupos eslavos mostraram declínio na incidência, alterações percentuais anuais -4,3% (p = 0.002). O declínio nas taxas também foi observado na população urbana em comparação com a rural, alterações percentuais anuais -3,3% vs. 17,6%, respectivamente. Pacientes com idade entre 60‒69 anos eram 31% de todos os casos e apresentaram as maiores alterações percentuais anuais 9,37% (p = 0,002). Os pacientes no Estágio II eram 61% de todas as observações, mas a tendência geral evidenciou crescimento acentuado no grupo do Estágio I (alterações percentuais anuais 28.91%; p < 0,0001).
Conclusão
No geral, durante a última década, a incidência de câncer colorretal aumentou 1,5 vezes com expectativa de maior aumento. No entanto, o incremento da porção do Estágio I em 2018 em comparação com os estágios avançados no momento do diagnóstico e a tendência de diminuição nas taxas entre a população urbana inspira uma garantia definitiva de eficiência potencial do programa de rastreamento em longo prazo. As próximas pesquisas sobre o câncer colorretal devem incluir cenários para revelar o papel do ambiente desfavorecido na região e o consumo de alimentos ultraprocessados não saudáveis.
Palavras-chave:
Carcinoma colorretal; Cazaquistão; Taxas de incidência; Prognóstico
Introduction
According to GLOBOCAN 2018 estimates, Colorectal Cancer (CRC) ranks fourth in worldwide scale in both sexes combined, accounting for 6.1% of all first diagnosed cancer cases.11 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424. There are commonly known risk factors for CRC occurrence: the presence of chronic inflammatory bowel disease, adenomatous polyps; family history; age of men and women over 50, given that more than 90% of patients with CRC are made up of people of this age; consuming unhealthy food and etc.22 Amersi F, Agustin M, Ko CY. Colorectal cancer: epidemiology, risk factors, and health services. Clin Colon Rectal Surg. 2005;18:133-40.–44 Fedewa SA, Sauer AG, Siegel RL, Jemal A. Prevalence of major risk factors and use of screening tests for cancer in the United States. Cancer Epidemiol Biomarkers Prev. 2015;24:637-52.
Among the risk factors for CRC development, environmental pollution with chemical compounds is not mentioned as top-ranked, however the Aktobe province of western Kazakhstan is known by its large chromium producing facilities. To our knowledge, an increased level of the chromosomal aberrations was found in peripheral blood leukocytes in workers exposed to the chromium.55 Mamyrbaev AA, Dzharkenov TA, Imangazina ZA, Satybaldieva UA. Mutagenic and carcinogenic actions of chromium and its compounds. Environ Health Prev Med. 2015;20:159-67.,66 Leonard A, Lauwerys RR. Carcinogenicity and mutagenicity of chromium. Mutat Res. 1980;76:227-39. On assessing the dynamics of cancer morbidity and mortality in the Aktobe province, local researchers had found out almost threefold increase in the rectum cancer incidence in tenths.77 Mamyrbayev A, Djarkenov T, Dosbayev A, Dusembayeva N, Shpakov A, Umarova G, et al. The incidence of malignant tumors in environmentally disadvantaged regions of Kazakhstan. Asian Pac J Cancer Prev. 2016;17:5203-9. Environmental pollution is also related to the fact that the Aktobe province is partially located in the vast Aral Sea ecological disaster region. According to data, long-time average annual levels of cancer morbidity for 2004–2013 in adult population living in the Aral Sea environs was up to 2.6 times higher, comparing to ecologically intact terrains. In particular, long-time average annual levels of cancer morbidity in adult population living in that zone was up to 57.2% higher, and the total cancer morbidity depended on the hazard coefficient (HQ) associated mostly with the inhalation of nickel and the combined cadmium intake (r = 0.8).77 Mamyrbayev A, Djarkenov T, Dosbayev A, Dusembayeva N, Shpakov A, Umarova G, et al. The incidence of malignant tumors in environmentally disadvantaged regions of Kazakhstan. Asian Pac J Cancer Prev. 2016;17:5203-9.
Given the rising rates of CRC, the nationwide screening program launched in Kazakhstan since 2009. Design of the program was developed according to the principles of the “European guidelines for quality assurance in CRC screening and diagnosis” and included iFOBT (immune analysis of fecal occult blood, FIT) and total colonoscopy at positive iFOBT in target groups of both genders 50–70 years aged with 2 year interval.88 von Karsa L, Patnick J, Segnan N, Atkin W, Halloran S, Lansdorp-Vogelaar I, et al. European Colorectal Cancer Screening Guidelines Working Group. European guidelines for quality assurance in colorectal cancer screening and diagnosis: overview and introduction to the full supplement publication. Endoscopy. 2013;45:51-9.
Commonly, the 10 years period of the screening implementation serves as first milestone in evaluation of some key indices of the disease.
Hence, the study is aimed to outline the vector of colorectal cancer incidence in the environmentally disadvantaged Aktobe province of western Kazakhstan through the specifying rates and trends in all age groups, as well as by gender, ethnicities, residences, stages and tumor sites.
Methods
This retrospective database research was approved by the University’s IREC (Protocol nº 21, 24.01.2019). Informed consent was not required because the individually identifiable data of patients were not involved.
Study setting
Territory of the Aktobe province is the largest in western Kazakhstan (Central Asia) and featured by chromium mining, presence of Oil industry and gas condensate works. Indigenous inhabitants are Kazakhs, of turcic ethnic group, followed by Slavs representing about 20% of entire population. Traditional diet of Kazakhs is of nomadic nature and consists mostly of meat and dairy.
Study population
Data on the province’ total population within 2009–2018 (857,711 as of January 2018) were requested from the Aktobe Statistical Committee.
All incident cases of first diagnosed colorectal cancer since 2009 through 2018 in adults aged 20 years and older were obtained from the Cancer registry of the Aktobe regional Oncologic Center. Rough incidence rates (per 100,000) and Annual Percent Changes (APCs), as well as the ratios were estimated for each age group at diagnosis (20–39, 40–49, 50–59, 60–69, 70+ years), by gender, ethinicities, residence (urban or rural area), the disease stages (The 8th edition of the UICC TNM Classification, 2016) and anatomic subsites.
This analysis operated with the ethinicities of patients as it was presented in the Cancer registry (Kazakhs, Slavs and Others). As to the anatomic subsites, the entire CRC was presented as C18.0‒C18.4 (ascending colon), C18.5‒C18.7 (descending colon), C19 (rectosigmoid junction) and C20‒C21 (rectum), respectively (according to International Classification of Diseases, X version, 2016).
Statistical analysis
All calculations were carried out in Statistica.10 (Dell Technologies, Round Rock, Texas, USA), as well as in the software SPSS.v.25. For all tests a two-side type I error of p < 0.05 at 95% Confidence Interval (CI) was assumed statistically significant. Incidence trends and corresponding 95% CIs were determined by the least squares method of regression analysis and expressed as the number of cases per 100,000 individuals. Changes in the incidence rates over time were calculated using the Student’s criterium and expressed as APCs. Ratios for the examined population’s gender, age, stages, CRC anatomic subsites, residences and ethnic groups were presented. The prognostic index of the CRC incidence was obtained by the method of moving averages, based on the smoothing procedure with an interval m = 1.
Results
In the Aktobe Cancer registry, within 2009–2018 a total of 1128 records were found on patients first diagnosed with CRC. General description of the study population is presented in Table 1.
Characteristics of individuals first diagnosed with CRC in the Aktobe province within 2009-2018.
A slight disproportion in favor of men is traced, while the rest items of the profile are featured with substantial differences (Table 1). Affected by CRC are mostly Kazakhs living in urban area, of 60–69 age, registered mostly with Stage II at presentation and having the predominant tumor location either at descending colon, or at rectum (left-sided CRC). Table 2 presents overall crude CRC rates by years, gender, stage (I/II – resectable, III/IV ‒ advanced) and age groups.
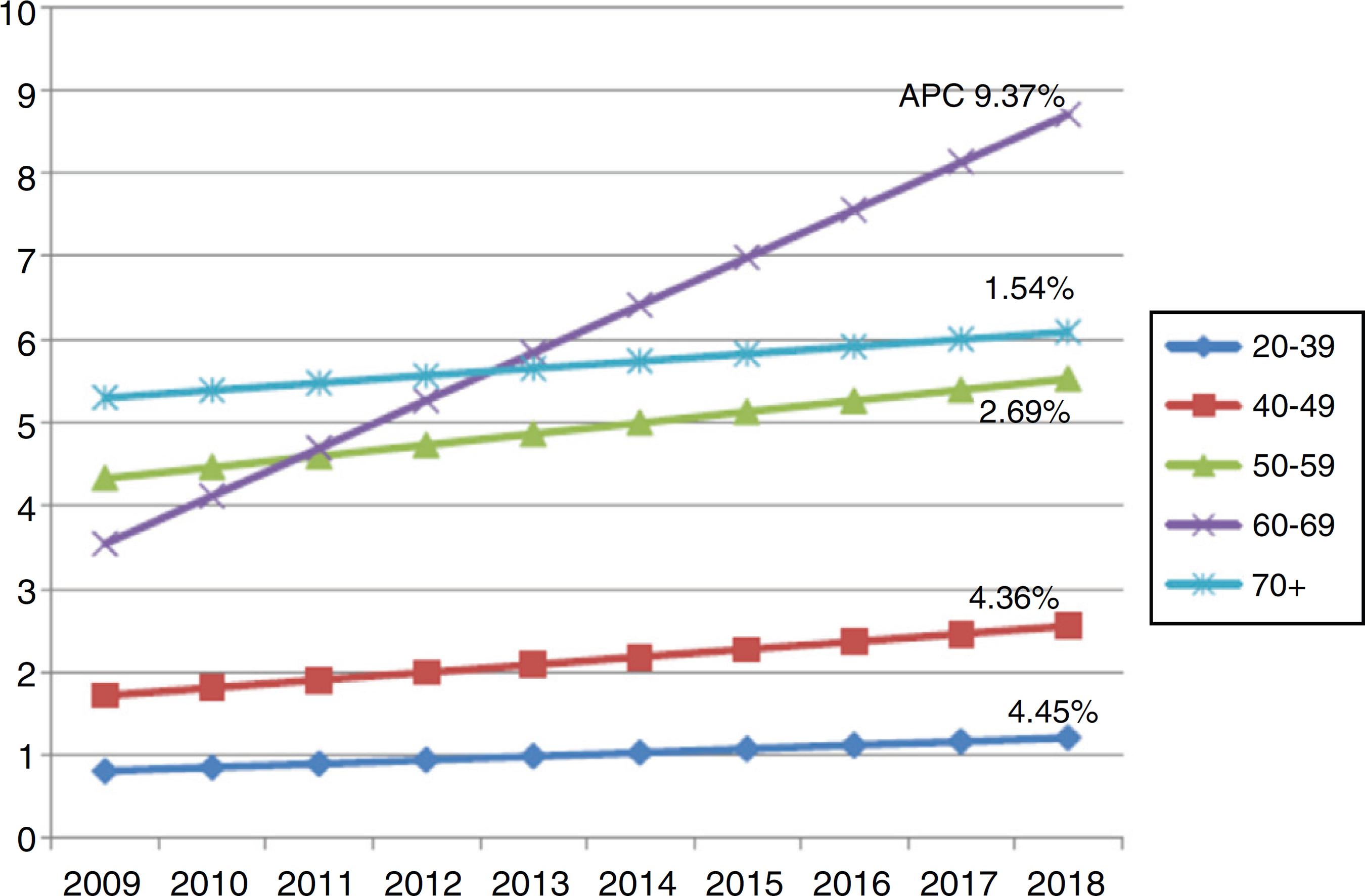
The dynamics by years evidences the boosted growth in incidence in men compared to women, up to 2 times and higher. The incidence rates in young patients (20–39 years old), as well as in 40–49 and 70+ aged have showed insignificant positive dynamics throughout a decade, in patients of 50–59 years slightly have grown up, whereas in 60–69 aged patients the rate soared up to 2.5 times. Age-specific trends with APCs are also presented in Fig. 1.
Age-specific trend in CRC incidence with APCs*. *Group aged 20–39 labelling in blue; aged 40–49 labelling in red; aged 50–59 labelling in green; aged 60–69 labelling in violet; and aged 70+ in turquoise, respectively.
Though the present profile of patients diagnosed with CRC is featured by prevailing of Kazakhs, mostly men of 60–69 year’s old living in urban area, APCs dynamics allows for supposing the boomed growth in incidence among other population groups in the nearest years. We should expect significant CRC affecting in men representing the ethnic minorities (Coreans, Azerbajanians, Dagestanians, Tatars, Germans), living in overwhelming majority in rural area (APC 17.6%) and having conventional distal location of CRC. Definitely, these individuals should be allocated into a special group at risk, and specialists responsible for population to be screened in countryside, should take this consideration into account.
It is appropriate to assume that impressive dynamics in stages at presentation - positive APC of Stage I (28.91%) and negative annual growth for Stage III (−7.62%) are provided by the launched screening program which significantly impacted the disease revealing.
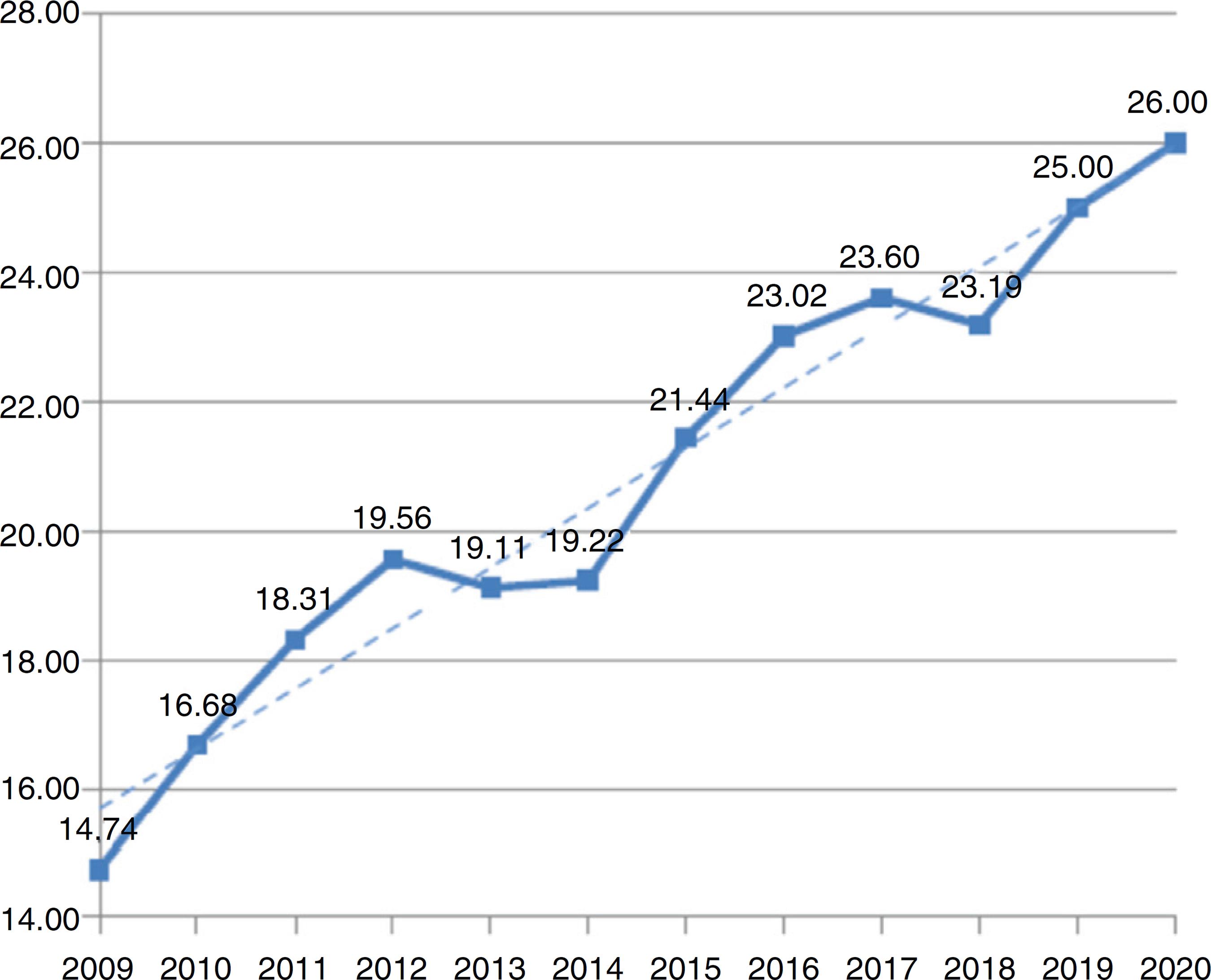
Further prognosis on CRC incidence for 2019–2020 was performed. Prognostic rates evidence its continuing growth to 25.01 by 2019 (95% CI 23.69–26.34) and up to 25.94 by 2020 (95% CI 24.43–27.46), respectively.
Data on the overall CRC incidence rates by years, including prognostic indices for 2019–2020 are also presented graphically (Fig. 2).
Discussion
This retrospective study provided summarized information on the rates and trends of CRC in the province within first decade of the screening implementation. As it is presented in Table 3, the averaged crude incidence rate between 2009 and 2018 has been found substantially high (19.88 per 100,000), besides, further tendency to rise with positive APC of 4.69% is traced.
While in western Kazakhstan the screening uptake for the time being is accompanied with continuing rise in CRC incidence, the U.S. authors recorded negative APC (−2.7%) at incidence rate of 45.9 within 14 years, 2000‒2014.99 Ansa BE, Coughlin SS, Alema-Mensah E, Smith SA. Evaluation of colorectal cancer incidence trends in the United States (2000–2014). J Clin Med. 2018;7:e22. Reportedly, until the late 1980s colorectal cancer was the second leading cause of cancer-related deaths for both men and women in the United States.1010 Siegel RL, Fedewa SA, Anderson WF, Miller KD, Ma JM, Rosenberg PS, et al. Colorectal cancer incidence patterns in the United States, 1974–2013. J Natl Cancer Inst. 2017;109. At a later date the overall age-adjusted CRC incidence rate decreased steadily between 1975 and 2010 in patients aged 50+ years owing to the screening program introducing since late 1980s.1111 Murphy CC, Sandler RS, Sanoff HK, Yang YC, Lund JL, Baron JA. Decrease in incidence of colorectal cancer among individuals 50 years or older after recommendations for population-based screening. Clin Gastroenterol Hepatol. 2017;15:903-9. The U.S. authors clarified that the overall incidence in whites as being 75.5/100,000 and up to 83.6/100,000 in black persons then decreased since 1980s until 2010–2013, but only among the screening-age population (ages 50 years or older).1212 United States Cancer Statistics. 1999–2014 Incidence and Mortality; 2017. Available from: http://www.cdc.gov/uscs... [Last updated 19 June 2019].
http://www.cdc.gov/uscs...
–1414 Siegel RL, Miller KD, Fedewa SA, Ahnen DJ, Meester RGS, Barzi A, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177-93.
Overall, the role of nationwide screening programs based on iFOBTs (FITs), followed by colonoscopy to reduce the CRC mortality rates currently is proven persuasively. The USPSTF research group reported that the “biennial screening with the guaiac-based FOBT compared to no screening resulted in reduction of CRC-specific mortality at 11–30 years of follow-up, ranging 9%–22% after 2–9 rounds of screening” (based on 5 RCTs, n = 404,396).1515 Ahrq.gov [internet], Lin JS, Piper MA, Perdue LA, Rutter C, Webber EM, et al. Screening for Colorectal Cancer: A Systematic Review for the U.S. Preventive Services Task Force. Evidence Synthesis No. 135. Report No. 14-05203-EF-1. Rockville (MD): Agency for Healthcare Research and Quality; 2016. Available from: https://www.ncbi.nlm.nih.gov/books/NBK43437/. [AccessedJune 2016].
https://www.ncbi.nlm.nih.gov/books/NBK43...
Based on data from 59,389 screenees age 50 to 69 years, researchers from Taiwan found that after a positive FIT-based screening, colonoscopy can reduce by about half the number of deaths from CRC.1616 Lee YC, Li-Sheng Chen S, Ming-Fang Yen A, Yueh-Hsia Chiu S, Ching-Yuan Fann J, Chuang SL, et al. Association between colorectal cancer mortality and gradient fecal hemoglobin concentration in colonoscopy noncompliers. J Natl Cancer Inst. 2017;109.
There is an accompanying effective measure to prevent growing incidence of CRC through increasing of public awareness on the disease which could arise a willingness to undergo a screening. According to mentioned US authors, not only the screening uptake, but arranging of nation-scale public health campaigns such as “Screen for Life”, allowed for significant decline in the CRC incidence rates.99 Ansa BE, Coughlin SS, Alema-Mensah E, Smith SA. Evaluation of colorectal cancer incidence trends in the United States (2000–2014). J Clin Med. 2018;7:e22. The findings of Saudi authors (Zubaidi et al.) who have explored the level of public awareness and possible ways to raise a willingness to undergo CRC screening, are of great interest as being universal in respect to population of any countries.1717 Zubaidi AM, AlSubaie NM, AlHumaid AA, Shaik SA, AlKhayal KA, AlObeed OA. Public awareness of colorectal cancer in Saudi Arabia: a survey of 1070 participants in Riyadh. Saudi J Gastroenterol. 2015;21:78-83. Almadi et al. upon studying the effect of public knowledge concluded that “neither gender, level of education, occupation, income, marital status, nor general knowledge about CRC was found to be associated with the willingness to undergo CRC screening”.1818 Almadi MA, Mosli MH, Bohlega MS, Al Essa MA, AlDohan MS, Alabdallatif TA, et al. Effect of public knowledge, attitudes, and behavior on willingness to undergo colorectal cancer screening using the health belief model. Saudi J Gastroenterol. 2015;21:71-7. As much as a majority of people are mostly negative about CRC screening, likely, only nationwide media campaigns may run as quite an effective tool to change their perception.
According to our data, although the highest proportion and annual growth were recorded in patients aged 60–69 (31.0%, APC 9.37%), the younger groups of age 20–39 and 40–49 (5.3% and 7.3%, respectively) also demonstrated quite sizable annual growth (APCs within 4.5%). Analysts from the USA noted that “the lifestyle behaviors, such as consuming unhealthy diets and physical inactivity, with the resultant increase in the prevalence of overweight and obesity were possible factors contributing to the increased rates of CRC among people younger than 50 years”.1111 Murphy CC, Sandler RS, Sanoff HK, Yang YC, Lund JL, Baron JA. Decrease in incidence of colorectal cancer among individuals 50 years or older after recommendations for population-based screening. Clin Gastroenterol Hepatol. 2017;15:903-9. Such environmental factors as cultural and economic relations play in this context considerable role, as low- and middle income countries have adopted diet and lifestyle practices similar to high-income countries. In regard to CRC, across Sub-Saharan Africa (SSA), reportedly, the significant affecting of younger patients under 40 years has been observed, compared to 3%–7% in high-income countries, which is related mostly to nutrition transition made by native Africans in favor of western food.1919 Irabor DO. Emergence of colorectal cancer in West Africa: accepting the inevitable. Niger Med J. 2017;58:87-91. The issues of consuming unhealthy, particularly processed food leading to obesity have widely been studying the latest years.2020 Bouvard V, Loomis D, Guyton KZ, Grosse Y, Ghissassi FE, Benbrahim-Tallaa L, et al. International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015;16:1599-600.,2121 Murphy N, Cross AJ, Abubakar M, Jenab M, Aleksandrova K, Boutron-Ruault MC, et al. A nested case-control study of metabolically defined body size phenotypes and risk of colorectal cancer in the European prospective investigation into cancer and nutrition (EPIC). PLoS Med. 2016;13:e1001988. Recently presented data on associations between ultra-processed food consumption and risk of cancer statistically proved a global trend: a 10% increase in the proportion of such a food is linked to a more than 10% in the risks of overall cancer.2222 Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Alles B, Mejean C, et al. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ. 2018;360:k322.,2323 GBD Diet Collaborators. Health effects of dietary risks in 195 countries, 1990‒2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019;393:1958-72.
Based on our Registry, data on rates and APCs by CRC tumor subsites (Table 3) partly vary from the USA’s indices within 2000–2014,99 Ansa BE, Coughlin SS, Alema-Mensah E, Smith SA. Evaluation of colorectal cancer incidence trends in the United States (2000–2014). J Clin Med. 2018;7:e22., as the ascending colon (20.0 per 100,000 in the USA, 42.9%) is not a predominant location of the neoplasm in western Kazakhstan, unlike the descending part (28.7%) and, particularly, rectum (35.3%), though the most sharp growth (APC 6.26%) is recorded in C19, recto sigmoid junction. Saudi authors, who also marked the growing CRC incidence in the country last years, reported almost similar data on the tumor sites distribution: rectum 28.1% and sigmoid 37.7% with a negligible proportion of the ascending colon.2424 Hassanain M, Al-alem F, Simoneau E, Traiki TA, Alsaif F, Alsharabi A, et al. Colorectal cancer liver metastasis trends in the Kingdom of Saudi Arabia. Saudi J Gastroenterol. 2016;22:370-4.
In order to get an overall idea on our current situation with CRC incidence rates, the same indices throughout other countries from different world regions were being compared. Reportedly, as of 2016 across the European high-income countries, CRC incidence rates were 38.9 in Norway and 29.2 in Sweden, whereas in Finland, where a national organized program was available, they were 23.5, respectively.2525 Altobelli E, D’Aloisio F, Angeletti PM. Colorectal cancer screening in countries of European Council outside of the EU-28. World J Gastroenterol. 2016;22:4946-57. The most populated country of Latin America, Brazil, has also faced high incidence and mortality from CRC, and both indices imminently tended to grow. Until the year 2025, mortality rates are expected at the level of 75.8% in men and 67.5% in women in Brazil.2626 Souza DL, Jerez-Roig J, Cabral FJ, de Lima JR, Rutalira MK, Costa JA. Colorectal cancer mortality in Brazil: predictions until the year 2025 and cancer control implications. Dis Colon Rectum. 2014;57:1082-9. From the other hand, in Mediterranean countries, adhered to a Mediterranean dietary pattern, noticeably low incidence of cancers linked to dietary factors, including CRC has been observed comparing to Scandinavian countries, the United Kingdom, and the United States.2727 Donovan MG, Selmin OI, Doetschman TC, Romagnolo DF. Mediterranean diet: prevention of colorectal cancer. Front Nutr. 2017;4:59.
Thus, our region with the actual incidence rate of 19.88 per 100,000 currently takes the mid position among the listed countries, but overall trends in incidence predict further worsening that can be prevented through the national screening program.
Strengths and limitations of the study
Overall, the incidence rates analysis among various population groups may be referred to strengths of this epidemiological study. In fact, identifying the group at risk on CRC development in the region was the most important value of the research performed. Meanwhile, data on the trends in CRC precancerous conditions diagnosis were not analyzed and discussed in frames of this study, as well as other key indices, such as mortality and survival rates. This shortness may be considered undoubtful limitation.
Conclusions
The overall vector of CRC incidence through the first decade of the screening implementation in western Kazakhstan evidenced its 1.5 fold growth with further expected rise. However, the increment of stage I portion vs. advanced stages at diagnosis by 2018, as well as the trend to decrease in rates among urban population inspires, to a definite extent, assurance in unconditional efficiency of the screening programmed in long run.
Data obtained must contribute to changing a current state of things, such as fast growing CRC rates among rural people, for whom timely medical examination is far less available. Public awareness to prevent CRC diagnosis at advanced stages should be straightened through the nationwide media campaigns.
The next researches on CRC should include scenarios to highlight and differentiate as much as possible the role of disadvantaged environment in the region and consuming unhealthy, in particular ultra-processed food.
-
Source of supportThis analysis is performed in frameworks of the scientific project on Colorectal cancer “Comparative analysis and clinical evaluation of predictive value of Serum Biomarkers CEA, CA19-9 used for the disease course monitoring in patients with Colorectal Carcinoma”, funded by the West Kazakhstan Medical University.
Acknowledgements
The authors thank Mrs. Gulmira Yerimbetova for her work in statistical processing of the results.
References
-
1Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424.
-
2Amersi F, Agustin M, Ko CY. Colorectal cancer: epidemiology, risk factors, and health services. Clin Colon Rectal Surg. 2005;18:133-40.
-
3Colorectal Cancer Facts & Figures 2017–2019. Atlanta: American Cancer Society, Inc; 2017. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics
» https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics -
4Fedewa SA, Sauer AG, Siegel RL, Jemal A. Prevalence of major risk factors and use of screening tests for cancer in the United States. Cancer Epidemiol Biomarkers Prev. 2015;24:637-52.
-
5Mamyrbaev AA, Dzharkenov TA, Imangazina ZA, Satybaldieva UA. Mutagenic and carcinogenic actions of chromium and its compounds. Environ Health Prev Med. 2015;20:159-67.
-
6Leonard A, Lauwerys RR. Carcinogenicity and mutagenicity of chromium. Mutat Res. 1980;76:227-39.
-
7Mamyrbayev A, Djarkenov T, Dosbayev A, Dusembayeva N, Shpakov A, Umarova G, et al. The incidence of malignant tumors in environmentally disadvantaged regions of Kazakhstan. Asian Pac J Cancer Prev. 2016;17:5203-9.
-
8von Karsa L, Patnick J, Segnan N, Atkin W, Halloran S, Lansdorp-Vogelaar I, et al. European Colorectal Cancer Screening Guidelines Working Group. European guidelines for quality assurance in colorectal cancer screening and diagnosis: overview and introduction to the full supplement publication. Endoscopy. 2013;45:51-9.
-
9Ansa BE, Coughlin SS, Alema-Mensah E, Smith SA. Evaluation of colorectal cancer incidence trends in the United States (2000–2014). J Clin Med. 2018;7:e22.
-
10Siegel RL, Fedewa SA, Anderson WF, Miller KD, Ma JM, Rosenberg PS, et al. Colorectal cancer incidence patterns in the United States, 1974–2013. J Natl Cancer Inst. 2017;109.
-
11Murphy CC, Sandler RS, Sanoff HK, Yang YC, Lund JL, Baron JA. Decrease in incidence of colorectal cancer among individuals 50 years or older after recommendations for population-based screening. Clin Gastroenterol Hepatol. 2017;15:903-9.
-
12United States Cancer Statistics. 1999–2014 Incidence and Mortality; 2017. Available from: http://www.cdc.gov/uscs.. [Last updated 19 June 2019].
» http://www.cdc.gov/uscs -
13Bailey CE, Hu CY, You YN, Bednarski BK, Rodriguez-Bigas MA, Skibber JM, et al. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975-2010. JAMA Surg. 2015;150:17-22.
-
14Siegel RL, Miller KD, Fedewa SA, Ahnen DJ, Meester RGS, Barzi A, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177-93.
-
15Ahrq.gov [internet], Lin JS, Piper MA, Perdue LA, Rutter C, Webber EM, et al. Screening for Colorectal Cancer: A Systematic Review for the U.S. Preventive Services Task Force. Evidence Synthesis No. 135. Report No. 14-05203-EF-1. Rockville (MD): Agency for Healthcare Research and Quality; 2016. Available from: https://www.ncbi.nlm.nih.gov/books/NBK43437/ [AccessedJune 2016].
» https://www.ncbi.nlm.nih.gov/books/NBK43437/ -
16Lee YC, Li-Sheng Chen S, Ming-Fang Yen A, Yueh-Hsia Chiu S, Ching-Yuan Fann J, Chuang SL, et al. Association between colorectal cancer mortality and gradient fecal hemoglobin concentration in colonoscopy noncompliers. J Natl Cancer Inst. 2017;109.
-
17Zubaidi AM, AlSubaie NM, AlHumaid AA, Shaik SA, AlKhayal KA, AlObeed OA. Public awareness of colorectal cancer in Saudi Arabia: a survey of 1070 participants in Riyadh. Saudi J Gastroenterol. 2015;21:78-83.
-
18Almadi MA, Mosli MH, Bohlega MS, Al Essa MA, AlDohan MS, Alabdallatif TA, et al. Effect of public knowledge, attitudes, and behavior on willingness to undergo colorectal cancer screening using the health belief model. Saudi J Gastroenterol. 2015;21:71-7.
-
19Irabor DO. Emergence of colorectal cancer in West Africa: accepting the inevitable. Niger Med J. 2017;58:87-91.
-
20Bouvard V, Loomis D, Guyton KZ, Grosse Y, Ghissassi FE, Benbrahim-Tallaa L, et al. International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015;16:1599-600.
-
21Murphy N, Cross AJ, Abubakar M, Jenab M, Aleksandrova K, Boutron-Ruault MC, et al. A nested case-control study of metabolically defined body size phenotypes and risk of colorectal cancer in the European prospective investigation into cancer and nutrition (EPIC). PLoS Med. 2016;13:e1001988.
-
22Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Alles B, Mejean C, et al. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ. 2018;360:k322.
-
23GBD Diet Collaborators. Health effects of dietary risks in 195 countries, 1990‒2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019;393:1958-72.
-
24Hassanain M, Al-alem F, Simoneau E, Traiki TA, Alsaif F, Alsharabi A, et al. Colorectal cancer liver metastasis trends in the Kingdom of Saudi Arabia. Saudi J Gastroenterol. 2016;22:370-4.
-
25Altobelli E, D’Aloisio F, Angeletti PM. Colorectal cancer screening in countries of European Council outside of the EU-28. World J Gastroenterol. 2016;22:4946-57.
-
26Souza DL, Jerez-Roig J, Cabral FJ, de Lima JR, Rutalira MK, Costa JA. Colorectal cancer mortality in Brazil: predictions until the year 2025 and cancer control implications. Dis Colon Rectum. 2014;57:1082-9.
-
27Donovan MG, Selmin OI, Doetschman TC, Romagnolo DF. Mediterranean diet: prevention of colorectal cancer. Front Nutr. 2017;4:59.
Publication Dates
-
Publication in this collection
23 Mar 2020 -
Date of issue
Jan-Mar 2020
History
-
Received
7 Sept 2019 -
Accepted
9 Oct 2019 -
Published
1 Nov 2019