Abstracts
OBJECTIVE:
McArdle’s disease is a metabolic myopathy that manifests with varied clinical conditions and is often confounded with other diagnoses. Herein, the authors report a case series and carry out a literature review.
METHODS:
A cross-sectional single-center study evaluating 12 patients with McArdle’s disease was conducted.
RESULTS:
Mean age at onset of symptoms was 28.0±17.4 years, while age at disease diagnosis was 39.0±14.8 years. History of intolerance to physical exercises was observed in 10 cases; muscle weakness in 9, second wind phenomenon in only 1 case. The presence of cramps, fatigue and myalgia was observed in 12, 11 and 9 of the cases respectively. Median creatine phosphokinase level was 5951U/L. Most of the patients (83.3%) were initially diagnosed with another condition (polymyositis, inclusion body myositis, fibromyalgia and/or muscular dystrophy), and approximately half had received glucocorticoids and/or immunosuppressants prior to definitive diagnosis. All patients underwent muscular biopsy, which revealed the presence of subsarcolemmal vacuoles characterized by glycogen deposits, and negative histochemical reaction for the myophosphorylase enzyme.
CONCLUSION:
The present study reinforces the presence of clinical variability among patients and shows that McArdle’s disease should be considered one of the differential diagnoses of inflammatory myopathies and other rheumatic diseases.
KEYWORDS:
Fibromyalgia; glycogen storage disease; myopathies; myophosphorylase; myositis
OBJETIVO:
A doença de McArdle é uma miopatia metabólica que se manifesta com condições clínicas variadas e muitas vezes é confundida com outros diagnósticos. Os autores relatam uma série de casos e realizam uma revisão de literatura.
MÉTODOS:
Estudo transversal de um único centro em que foram avaliados 12 pacientes com doença de McArdle.
RESULTADOS:
A média de idade no início dos sintomas foi de 28,0±17,4 anos, enquanto a idade no diagnóstico da doença foi de 39,0±14,8 anos. História de intolerância ao exercício físico foi observada em 10 dos casos; fraqueza muscular em 9; fenômeno do “second wind” em apenas 1 caso. A presença de câimbras, fadiga e mialgia foi observada, respectivamente, em 12, 11 e 9 dos casos. O nível mediano de creatinafosfoquinase foi de 5951U/L. Oito pacientes foram inicialmente diagnosticados com outra condição (polimiosite, miosite de corpos de inclusão, fibromialgia e/ou distrofia muscular), e aproximadamente metade havia recebido glicocorticoides e/ou imunossupressores antes do diagnóstico definitivo. Todos os pacientes foram submetidos à biópsia muscular, que revelou a presença de vacúolos subsarcolêmicos caracterizados por depósitos de glicogênio e reação histoquímica negativa para a enzima miofosforilase.
CONCLUSÕES:
O presente estudo reforça a presença de variabilidade clínica entre pacientes e mostra que a doença de McArdle deve ser considerada um dos diagnósticos diferenciais de miopatias inflamatórias e outras doenças reumáticas.
PALAVRAS-CHAVE:
Fibromialgia; moléstias de armazenamento de glicogênio; miopatias; monofosforilase; miosite
INTRODUCTION
McArdle’s disease or glycogen storage disease type V is a metabolic myopathy caused by the deficiency of myophosphorylase, an enzyme encoded by the PYGM gene, which catalyzes the degradation of glycogen into glucose in skeletal muscle.11 McArdle B. Myopathy due to a defect in muscle glycogen breakdown. Clin Sci. 1951;10:13-35.
2 Haller RG. Treatment of McArdle disease. Arch Neurol. 2000;57:923-4. DOI:10.1001/archneur.57.7.923
https://doi.org/10.1001/archneur.57.7.92...
3 DiMauro S, Bruno C. Glycogen storage diseases of muscle. Curr Opin Neurol. 1998;11:477-84. DOI:10.1097/00019052-199810000-00010
https://doi.org/10.1097/00019052-1998100...
-44 Kitaoka Y. McArdle disease and exercise physiology. Biology. 2014;3:157-66. DOI:10.3390/biology3010157
https://doi.org/10.3390/biology3010157...
There is scant epidemiological data about McArdle’s disease. The disease has an estimated prevalence of approximately 1 per 100000 - 167000 population,55 Tobon A. Metabolic Myopathies. Continuum (Minneap Minn). 2013;19:1571-97. DOI:10.1212/01.CON.0000440660.41675.06.
https://doi.org/10.1212/01.CON.000044066...
,66 Lucia A, Ruiz JR, Santalla A, Nogales-Gadea G, Rubio JC, García-Consuegra I, et al. Genotypic and phenotypic features of McArdle disease: insights from the Spanish national registry. J Neurol Neurosurg Psychiatry. 2012;83:322-8. DOI:10.1136/jnnp-2011-301593.
https://doi.org/10.1136/jnnp-2011-301593...
and affects individuals of both sexes at a mean age of 44 years.66 Lucia A, Ruiz JR, Santalla A, Nogales-Gadea G, Rubio JC, García-Consuegra I, et al. Genotypic and phenotypic features of McArdle disease: insights from the Spanish national registry. J Neurol Neurosurg Psychiatry. 2012;83:322-8. DOI:10.1136/jnnp-2011-301593.
https://doi.org/10.1136/jnnp-2011-301593...
The symptoms of McArdle’s disease usually commence during adolescence or young adulthood.77 Haller RG, Vissing J. Spontaneous 'second wind' and glucose-induced second 'second wind' in McArdle disease: oxidative mechanisms. Arch Neurol. 2002;59:1395-402. DOI:10.1001/archneur.59.9.1395
https://doi.org/10.1001/archneur.59.9.13...
The disease is characterized by exercise intolerance, myalgias and/or muscle cramps.88 Mauro S Di. Muscle glycogenoses: an overview. Acta Myol. 2007;26:35-41. The “second-wind” phenomenon is very characteristic of the disease, in which muscle pain may dissipate after a brief rest period and allow the patient to resume exercise at the previous or a slightly reduced level.55 Tobon A. Metabolic Myopathies. Continuum (Minneap Minn). 2013;19:1571-97. DOI:10.1212/01.CON.0000440660.41675.06.
https://doi.org/10.1212/01.CON.000044066...
Half of patients have myoglobinuria and 90% of the cases present a considerable increase in creatine phosphokinase (CPK) during periods of disease exacerbation.88 Mauro S Di. Muscle glycogenoses: an overview. Acta Myol. 2007;26:35-41.,99 Lopez A, Banos I, Garcia-Estan J, Garcia B, Perez J, Salmeron P. Enfermedad de McArdle: descripción de cuatro hermanos con déficit de miofosforilasa. An Med Interna. 2001;18:136-8. Muscle biopsy reveals the presence of subsarcolemmal vacuoles, characterized by deposits of glycogen.1111 Sanjurjo E, Laguno M, Bedini JL, Miró O, Grau JM. Forearm ischemic exercise test. Standardization and diagnostic value in the identification of McArdle disease. Med Clin. 2004;122):761-6. DOI:10.1016/S0025-7753(04)74380-8
https://doi.org/10.1016/S0025-7753(04)74...
12 De Kerviler E, Leroy-Willig A, Duboc D, Eymard B, Syrota A. MR quantification of muscle fatty replacement in McArdle's disease. Magn Reson Imaging. 1996;14):1137-41. DOI:10.1016/S0730-725X(96)00236-6
https://doi.org/10.1016/S0730-725X(96)00...
-1313 Krishnamoorthy N, Santosh V, Yasha TC, Mahadevan A, Shankar SK, Jethwani D, et al. Glycogen storage disease type V (Mc Ardle's disease): a report on three cases. Neurol India. 2011;59:884-6. DOI:10.4103/0028-3886.91370
https://doi.org/10.4103/0028-3886.91370...
In addition, histochemistry shows a deficiency in myophosphorylase enzyme activity.1111 Sanjurjo E, Laguno M, Bedini JL, Miró O, Grau JM. Forearm ischemic exercise test. Standardization and diagnostic value in the identification of McArdle disease. Med Clin. 2004;122):761-6. DOI:10.1016/S0025-7753(04)74380-8
https://doi.org/10.1016/S0025-7753(04)74...
12 De Kerviler E, Leroy-Willig A, Duboc D, Eymard B, Syrota A. MR quantification of muscle fatty replacement in McArdle's disease. Magn Reson Imaging. 1996;14):1137-41. DOI:10.1016/S0730-725X(96)00236-6
https://doi.org/10.1016/S0730-725X(96)00...
-1313 Krishnamoorthy N, Santosh V, Yasha TC, Mahadevan A, Shankar SK, Jethwani D, et al. Glycogen storage disease type V (Mc Ardle's disease): a report on three cases. Neurol India. 2011;59:884-6. DOI:10.4103/0028-3886.91370
https://doi.org/10.4103/0028-3886.91370...
However, the variability of the clinical manifestations and lack of knowledge about the disease can lead to delayed and erroneous diagnosis, such as polymyositis, inclusion myositis, fibromyalgia, among others. Therefore, recognition of McArdle’s disease is of great relevance in rheumatologic practice, especially as one of the differential diagnoses of inflammatory myopathies. Thus, we present a case series of patients with McArdle’s disease, followed by a review of the literature.
MATERIALS AND METHODS
An inception single-center cohort study describing 12 consecutive patients with McArdle’s disease1414 Lucia A, Nogales-Gadea G, Pérez M, Martín MA, Andreu AL, Arenas J. McArdle disease: what do neurologists need to know? Nature Clin Pract Neurol. 2008;4:568-77. DOI:10.1038/ncpneuro0913
https://doi.org/10.1038/ncpneuro0913...
in the period from 2010 to 2017 was carried out. The study was approved by the Local Ethics Committee (case # 0039/10).
Inclusion criteria: patients presenting with objective skeletal muscle weakness, physical exercise intolerance and/or the presence of a “second wind” phenomenon; elevated serum CPK, without apparent cause; muscle biopsy with evidence of subsarcolemmal vacuoles characterized by glycogen deposits, and negative histochemical reaction for the myophosphorylase enzyme.
Definition of variables: demographic, clinical and laboratory data were obtained through a systematic review of medical records. The following parameters were analyzed: sex; ethnicity; age at onset of muscle symptoms; age at diagnosis of the disease; history of intolerance to exercise, myalgias, fatigue, cramps, objective muscular weakness, presence of the second wind phenomenon, acute renal failure, family history, serum CPK level (basal and maximum); electromyography; findings on magnetic resonance imaging of skeletal muscle; initial diagnosis and type of treatment initially received.
The following parameters refer to patient admission to our service: magnetic resonance imaging of the thighs, biopsy of the vastus lateralis muscle or brachial biceps, serum CPK (automated kinetic method), evaluation of muscular strength of the limbs - grade 0: absence of muscular contraction; grade 1: mild contractility deficit, grade 2: normal amplitude movements but does not overcome the action of gravity; grade 3: normal amplitude movements against the action of gravity; grade 4: integral mobility against action of gravity and some degree of resistance; grade 5: complete mobility against severe resistance and against the action of gravity).1515 Medical Research Council. Aids to the examination of the peripheral nervous system, Memorandum no. 45. Her Majesty's Stationery Office, London, 1981.
Statistical analysis: The Kolmogorov-Smirnov test was used to evaluate the distribution of each of the continuous variables. The results were presented as mean, standard deviation for continuous variables, and number (%) for categorical variables. The median (minimum - maximum) values were calculated for continuous variables that did not present a normal distribution. All analyzes were performed using SPSS 15.0 software (Chicago, USA).
RESULTS
The general characteristics of the 12 patients with McArdle’s disease are shown in Table 1. There was a predominance of females and Caucasians. The mean age at the onset of symptoms was 28.0 ± 17.4 years, while the mean age at diagnosis of the disease was 39.0 ± 14.8 years.
A history of intolerance to physical exercise was observed in 10 of the cases, while muscular weakness occurred in 9, and “second wind” phenomenon was described in only 1 case. In addition, the presence of cramps, fatigue and myalgia was observed in 12, 11 and 9 of the cases, respectively. A history of acute renal failure was reported in 2 cases. At admission of the patients to our service, with the exception of 2 patients, all had some degree of muscle weakness of the upper and/or lower limbs. Regarding family history, 2 patients had a history of consanguineous parents.
The mean peak CPK level was 5951 (1162 - 200000) U/L, while the mean baseline CPK serum level was 1341 (110 - 27000) U/L. Only 1 patient had a normal baseline CPK level. Electroneuromyography, performed in half of the cases, revealed a myopathic pattern in about two thirds of the cases. Magnetic resonance imaging of the thigh muscles had been performed in 8 of the 12 patients, four of whom had edema of the muscle compartments.
Ten of the 12 patients were initially treated with the hypothesis of polymyositis, inclusion body myositis, fibromyalgia and/or muscular dystrophy. Half of the patients had received glucocorticoid, immunosuppressants and/or human intravenous immunoglobulin. One patient had a myopathy hypothesis to clarify, and only 1 case was admitted with the initial suspicion of metabolic myopathy.
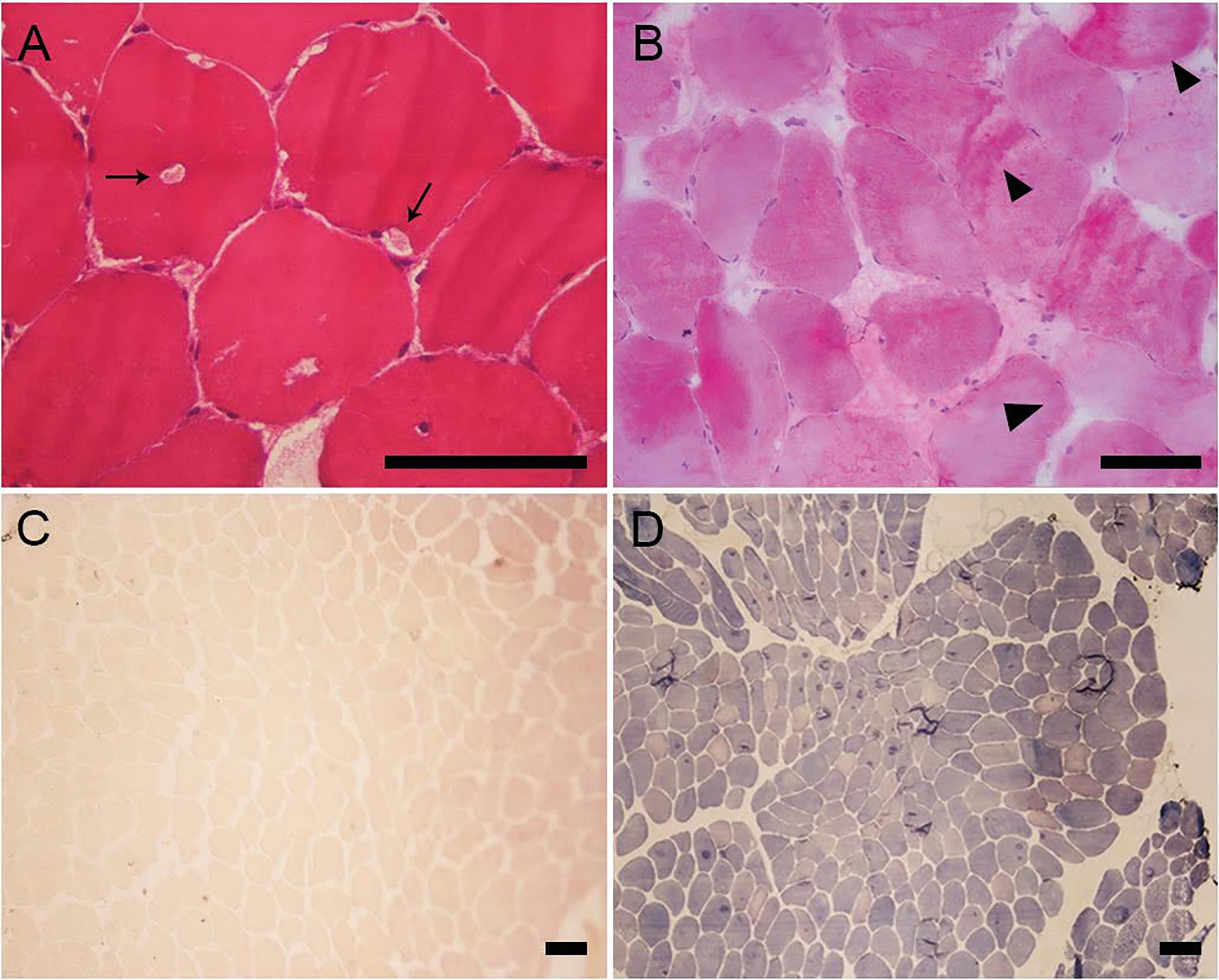
All of these patients underwent muscle biopsy, which showed the presence of subsarcolemmal vacuoles characterized by glycogen deposits (Figure 1).
Muscle biopsy of a patient with McArdle's disease. A) Subsarcolemmal and intracytoplasmic vacuoles in the muscle fiber (Hematoxylin & Eosin) (arrows). B) Schiff's periodic acid (PAS) showing subsarcolemmal accumulation of glycogen (arrow head). C) Absence of reaction staining for myophosphorylase (negative myophosphorylase reaction). D) myophosphorylase normal reaction in a patient without McArdle's disease. Black bar = 100 um.
DISCUSSION
In the present study, the demographic, clinical and laboratory profiles of 12 patients with histologically-confirmed McArdle’s disease were described; most of the cases were initially treated as other rheumatic diseases.
Although no molecular analysis was performed to investigate possible mutation in the PYGM gene, the patients included in the study were carefully selected according to the histological findings and with demonstrated deficiency of the myophosphorylase enzyme activity. All had histological analysis of muscle biopsy, the presence of subsarcolemmal vacuoles due to the accumulation of glycogen.
The time of onset of symptoms in McArdle’s disease is variable, ranging from early childhood to adulthood, with disease predominance in females.1313 Krishnamoorthy N, Santosh V, Yasha TC, Mahadevan A, Shankar SK, Jethwani D, et al. Glycogen storage disease type V (Mc Ardle's disease): a report on three cases. Neurol India. 2011;59:884-6. DOI:10.4103/0028-3886.91370
https://doi.org/10.4103/0028-3886.91370...
,1616 Martín MA, Rubio JC, Buchbinder J, Fernández-Hojas R, del Hoyo P, Teijeira S, et al. Molecular heterogeneity of myophosphorylase deficiency (McArdle's disease): a genotype-phenotype correlation study. Ann Neurol. 2001;50:574-81. DOI:10.1002/ana.1225
https://doi.org/10.1002/ana.1225...
17 Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
https://doi.org/10.1136/jnnp.2009.195040...
-1818 Gurgel-Giannetti J, Nogales-Gadea G, van der Linden Jr H, Giannetti AV, de Castro Concentino EL, et al. Clinical and molecular characterization of McArdle's disease in Brazilian patients. Neuromol Med. 2013;15:470-5. DOI:10.1007/s12017-013-8233-2 DOI:10.1007/s12017-013-8233-2
https://doi.org/10.1007/s12017-013-8233-...
In the present study, this characteristic was confirmed, with the majority of patients presenting the first symptoms in adulthood. In addition, although the onset of symptoms is rare after age 50, there was one case (#8) with initial symptoms at the age of 60.
According to the classification of Vieitz et al.1919 Vieitz I, Teijeira S, Fernandez JM, San Millan B, Miranda S, Ortolano S, et al. Molecular and clinical study of McArdle's disease in a cohort of 123 European patients. Identification of 20 novel mutations. Neuromuscul Disord. 2011;21:817-23. DOI:10.1016/j.nmd.2011.07.002
https://doi.org/10.1016/j.nmd.2011.07.00...
there are three clinically distinguishable groups of patients with McArdle’s disease: 1) with exercise intolerance; 2) with permanent muscular weakness and 3) oligo or asymptomatic. Exercise intolerance is the most common clinical form reported in most studies,1616 Martín MA, Rubio JC, Buchbinder J, Fernández-Hojas R, del Hoyo P, Teijeira S, et al. Molecular heterogeneity of myophosphorylase deficiency (McArdle's disease): a genotype-phenotype correlation study. Ann Neurol. 2001;50:574-81. DOI:10.1002/ana.1225
https://doi.org/10.1002/ana.1225...
17 Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
https://doi.org/10.1136/jnnp.2009.195040...
-1818 Gurgel-Giannetti J, Nogales-Gadea G, van der Linden Jr H, Giannetti AV, de Castro Concentino EL, et al. Clinical and molecular characterization of McArdle's disease in Brazilian patients. Neuromol Med. 2013;15:470-5. DOI:10.1007/s12017-013-8233-2 DOI:10.1007/s12017-013-8233-2
https://doi.org/10.1007/s12017-013-8233-...
,2020 Gordon N. Glycogenosis type V or McArdle's disease. Dev Med Child Neurol. 2003;45:640-4. DOI:10.1017/S0012162203001178
https://doi.org/10.1017/S001216220300117...
as observed in our cohort.
In patients with exercise intolerance, the “second wind” phenomenon, described as an improvement in exercise tolerance after a short period of sustained effort (about 12 minutes) is a classic clinical manifestation.2121 Santalla A, Nogales-Gadea G, Ortenblad N, Brull A, de Luna N, Pinós T, et al. McArdle disease: a unique study model in sports medicine. Sports Med. 2014;44:1531-4. DOI:10.1007/s40279-014-0223-5
https://doi.org/10.1007/s40279-014-0223-...
22 Vissing J, Haller RG. A diagnostic cycle test for McArdle's disease. Ann Neurol. 2003;54:539-42. DOI:10.1002/ana.10725
https://doi.org/10.1002/ana.10725...
-2323 Braakhekke JP, de Bruin MI, Stegeman DF, Wevers RA, Binkhorst RA, Joosten EM. The second wind phenomenon in McArdle's disease. Brain. 1986;109:1087-101. DOI:10.1093/brain/109.6.1087
https://doi.org/10.1093/brain/109.6.1087...
However, in our cohort, the “second wind” phenomenon was observed in only one case.
The most common initial symptoms identified in our patients, besides exercise intolerance, were cramps and myalgias, which corroborates previously described information.1616 Martín MA, Rubio JC, Buchbinder J, Fernández-Hojas R, del Hoyo P, Teijeira S, et al. Molecular heterogeneity of myophosphorylase deficiency (McArdle's disease): a genotype-phenotype correlation study. Ann Neurol. 2001;50:574-81. DOI:10.1002/ana.1225
https://doi.org/10.1002/ana.1225...
,1717 Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
https://doi.org/10.1136/jnnp.2009.195040...
Fatigue was also observed in most patients and is usually associated with a hyperkinetic circulation response to exercise.2121 Santalla A, Nogales-Gadea G, Ortenblad N, Brull A, de Luna N, Pinós T, et al. McArdle disease: a unique study model in sports medicine. Sports Med. 2014;44:1531-4. DOI:10.1007/s40279-014-0223-5
https://doi.org/10.1007/s40279-014-0223-...
,2424 Lewis SF, Haller RG. The pathophysiology of McArdle's disease: clues to regulation in exercise and fatigue. J Appl Physiol. 1986;61:391-401. DOI:10.1152/jappl.1986.61.2.391
https://doi.org/10.1152/jappl.1986.61.2....
Although McArdle’s disease is not a potentially fatal condition, rhabdomyolysis can occur and lead to acute renal failure, described in up to 50% of cases.1717 Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
https://doi.org/10.1136/jnnp.2009.195040...
,2121 Santalla A, Nogales-Gadea G, Ortenblad N, Brull A, de Luna N, Pinós T, et al. McArdle disease: a unique study model in sports medicine. Sports Med. 2014;44:1531-4. DOI:10.1007/s40279-014-0223-5
https://doi.org/10.1007/s40279-014-0223-...
,2525 Pillarisetti J, Ahmed A. McArdle disease presenting as acute renal failure. South Med J. 2007;100:313-6. DOI:10.1097/01.smj.0000242355.27078.f3
https://doi.org/10.1097/01.smj.000024235...
In our series, about one-fifth of cases evolved with rhabdomyolysis without the need for hemodialysis.
The presence of muscle weakness ranges from 16 to 33%1414 Lucia A, Nogales-Gadea G, Pérez M, Martín MA, Andreu AL, Arenas J. McArdle disease: what do neurologists need to know? Nature Clin Pract Neurol. 2008;4:568-77. DOI:10.1038/ncpneuro0913
https://doi.org/10.1038/ncpneuro0913...
,1717 Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
https://doi.org/10.1136/jnnp.2009.195040...
and is generally of proximal predominance. In the present study, the complaint of muscle weakness was observed in 10 of the 12 patients, affecting both upper and lower limbs. Serum levels of muscle enzymes are also variable between the rest period and physical activity.1616 Martín MA, Rubio JC, Buchbinder J, Fernández-Hojas R, del Hoyo P, Teijeira S, et al. Molecular heterogeneity of myophosphorylase deficiency (McArdle's disease): a genotype-phenotype correlation study. Ann Neurol. 2001;50:574-81. DOI:10.1002/ana.1225
https://doi.org/10.1002/ana.1225...
,1717 Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
https://doi.org/10.1136/jnnp.2009.195040...
,2121 Santalla A, Nogales-Gadea G, Ortenblad N, Brull A, de Luna N, Pinós T, et al. McArdle disease: a unique study model in sports medicine. Sports Med. 2014;44:1531-4. DOI:10.1007/s40279-014-0223-5
https://doi.org/10.1007/s40279-014-0223-...
Even during rest periods, our patients had elevated levels of CPK.
With regard to electroneuromyography findings these can be normal, nonspecific, neuropathic or, in most cases, myopathic findings.1818 Gurgel-Giannetti J, Nogales-Gadea G, van der Linden Jr H, Giannetti AV, de Castro Concentino EL, et al. Clinical and molecular characterization of McArdle's disease in Brazilian patients. Neuromol Med. 2013;15:470-5. DOI:10.1007/s12017-013-8233-2 DOI:10.1007/s12017-013-8233-2
https://doi.org/10.1007/s12017-013-8233-...
,2626 Andreu AL, Nogales-Gadea G, Cassandrini D, Arenas J, Bruno C. McArdle disease: molecular genetic update. Acta Myol. 2007;26:53-7. In our series, two thirds of the patients tested had evidence of a pure myopathic pattern.
Ischemic exercise testing is used in the evaluation of patients with suspected McArdle´s Disease. A lack of increase in blood lactate concentration during exercise is indicative of a defect in conversion of glycogen (or glucose) to lactate, consistent with the deficiency of skeletal muscle phosphorylase in this disease. However, this test is unspecific in metabolic myopathies, whereby other glycogen storage diseases, such as phosphofructokinase deficiency and debranching enzyme, also yield an abnormal ischemic exercise response.2727 Coleman RA, Stajich JM, Pact VW, Pericak-Vance MA. The ischemic exercise test in normal adults and in patients with weakness and cramps. Muscle Nerve. 1986;9:216-21. DOI:10.1002/mus.880090305
https://doi.org/10.1002/mus.880090305...
The confirmatory diagnosis of McArdle’s disease can be established by evidence of mutation in the PYGM gene or by muscle biopsy disclosing a deficiency of myophosphorylase activity.1414 Lucia A, Nogales-Gadea G, Pérez M, Martín MA, Andreu AL, Arenas J. McArdle disease: what do neurologists need to know? Nature Clin Pract Neurol. 2008;4:568-77. DOI:10.1038/ncpneuro0913
https://doi.org/10.1038/ncpneuro0913...
Over 100 types of mutations in the PYGM gene have been described to date, the most common being the p.R50X variant (previously known as p.R49X).1818 Gurgel-Giannetti J, Nogales-Gadea G, van der Linden Jr H, Giannetti AV, de Castro Concentino EL, et al. Clinical and molecular characterization of McArdle's disease in Brazilian patients. Neuromol Med. 2013;15:470-5. DOI:10.1007/s12017-013-8233-2 DOI:10.1007/s12017-013-8233-2
https://doi.org/10.1007/s12017-013-8233-...
,2828 Tsujino S, Shankse S, Di Mauro S. Molecular genetic heterogeneity of myophosphorylase deficiency (McArdle's disease). N Engl J Med. 1993;329:241-5. DOI:10.1056/NEJM199307223290404
https://doi.org/10.1056/NEJM199307223290...
However, access to genetic testing in Brazil is limited and therefore the diagnosis is typically confirmed by muscle biopsy, usually indicated before the suspicion of myopathy under investigation.
The diagnosis of McArdle’s disease can pose a challenge in clinical practice, since its clinical manifestations can be extremely variable, as shown in the present study, and depends on a high level of suspicion. Patients are often initially diagnosed as having depression, Parkinson’s, chronic fatigue syndrome, fibromyalgia, muscular dystrophy or inflammatory myopathies.1616 Martín MA, Rubio JC, Buchbinder J, Fernández-Hojas R, del Hoyo P, Teijeira S, et al. Molecular heterogeneity of myophosphorylase deficiency (McArdle's disease): a genotype-phenotype correlation study. Ann Neurol. 2001;50:574-81. DOI:10.1002/ana.1225
https://doi.org/10.1002/ana.1225...
17 Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
https://doi.org/10.1136/jnnp.2009.195040...
-1818 Gurgel-Giannetti J, Nogales-Gadea G, van der Linden Jr H, Giannetti AV, de Castro Concentino EL, et al. Clinical and molecular characterization of McArdle's disease in Brazilian patients. Neuromol Med. 2013;15:470-5. DOI:10.1007/s12017-013-8233-2 DOI:10.1007/s12017-013-8233-2
https://doi.org/10.1007/s12017-013-8233-...
Currently, there is no curative treatment for McArdle’s disease, with no evidence of significant benefit from any specific nutritional or pharmacological treatment, such as ramipril, verapamil, oral ribose, branched chain amino acids, or dantrolene.2929 Quinlivan R, Martinuzzi A, Schoser B. Pharmacological and nutritional treatment for McArdle disease (Glycogen Storage Disease type V). Cochrane Database Syst Rev. 2014;12:CD003458. DOI:10.1002/14651858.CD003458.pub5.
https://doi.org/10.1002/14651858.CD00345...
30 Martinuzzi A, Sartori E, Fanin M, Nascimbeni A, Valente L, Angelini C, et al. Phenotype modulators in myophosphorylase deficiency. Ann Neurol. 2003;53:497-502. DOI:10.1002/ana.10499
https://doi.org/10.1002/ana.10499...
31 Lane RJ, Turnbull DM, Welch JL, Walton J. A double-blind, placebo-controlled, crossover study of verapamil in exertional muscle pain. Muscle Nerve. 1986;9:635-41. DOI:10.1002/mus.880090710
https://doi.org/10.1002/mus.880090710...
32 Steele IC, Patterson VH, Nicholls DP. A double blind, placebo controlled, crossover trial of D-ribose in McArdle's disease. J Neurol Sci. 1996;136:174-7. DOI:10.1016/0022-510X(95)00320-2
https://doi.org/10.1016/0022-510X(95)003...
33 MacLean D, Vissing J, Vissing SF, Vissing SF, Haller RG. Oral branched-chain amino acids do not improve exercise capacity in McArdle disease. Neurology. 1998;51:1456-9. DOI:10.1212/WNL.51.5.1456
https://doi.org/10.1212/WNL.51.5.1456...
34 Poels PJ, Braakhekke JP, Joosten EM, Stegeman DF. Dantrolene sodium does influence the second-wind phenomenon in McArdle's disease. Electrophysiological evidence during exercise in a double-blind placebo-controlled, cross-over study in 5 patients. J Neurol Sci. 1990;100:108-12. DOI:10.1016/0022-510X(90)90020-N
https://doi.org/10.1016/0022-510X(90)900...
-3535 Day TJ, Mastaglia FL. Depot-glucagon in the treatment of McArdle's disease. Aust N Z J Med. 1985;15:748-50. Similarly, there was no benefit from treatment of the disease with pyridoxine over placebo, except in one study in which one patient was supplemented with vitamin B6 and showed enhanced myophosphorylase activity.3636 Phoenix J, Hopkins P, Bartram C, Beynon RJ, Quinlivan RC, Edwards RH. Effect of vitamin B6 supplementation in McArdle's disease: a strategic case study. Neuromuscul Disord. 1998;8:210-2. DOI:10.1016/S0960-8966(98)00004-2
https://doi.org/10.1016/S0960-8966(98)00...
,3737 Sato S, Ohi T, Nishino I, Sugie H. Confirmation of the efficacy of vitamin B6 supplementation for McArdle disease by follow-up muscle biopsy. Muscle Nerve. 2012;45:436-40. DOI:10.1002/mus.22290.
https://doi.org/10.1002/mus.22290...
Use of low dose creatine produced a slight benefit,3838 Vorgerd M, Grehl T, Jager M, Muller K, Freitag G, Patzold T, et al. Creatine therapy in myophosphorylase deficiency (McArdle disease): a placebo-controlled crossover trial. Arch Neurol. 2000;57:956-63. DOI:10.1001/archneur.57.7.956
https://doi.org/10.1001/archneur.57.7.95...
but a high dose of creatine caused myalgia3939 Vorgerd M, Zange J, Kley R, Grehl T, Husing A, Jager M, et al. Effect of high-dose creatine therapy on symptoms of exercise intolerance in McArdle disease: double-blind, placebo-controlled crossover study. Arch Neurol. 2002;59:97-101. DOI:10.1001/archneur.59.1.97
https://doi.org/10.1001/archneur.59.1.97...
in patients with McArdle’s disease.
In general, recommendation for patients with exercise intolerance is primarily the indication of a diet high in carbohydrates (65%) and low in fat (20%), which has been shown to be a beneficial intervention that relieves intolerance and protects against rhabdomyolysis.4040 Andersen ST, Vissing J. Carbohydrate- and protein-rich diets in McArdle disease: effects on exercise capacity [published erratum appears in J Neurol Neurosurg Psychiatry. 2010;81:1414. J Neurol Neurosurg Psychiatry. 2008;79:1359-63. DOI:10.1136/adc.2008.146548
https://doi.org/10.1136/adc.2008.146548...
In addition, supervised aerobic training and self-awareness about the “second wind” phenomenon are considered fundamental in the treatment of McArdle’s disease. Patients may learn to recognize the point at which exercise becomes better tolerated, when glycolytic pathway deviation to lipid beta-oxidation occurs metabolically. This approach has an impact on quality of life and promotes improvement in exercise intolerance.
The limitations of this study were the small number of patients and the lack of genetic analysis, not routinely performed in Brazil.
SUMMARY
McArdle’s disease has broad clinical variability, often being misdiagnosed as other diseases, leading to costly and unnecessary treatments. Knowing the characteristics of this condition and assuming a high level of suspicion in clinical practice can help establish a faster and more accurate diagnosis.
ACKNOWLEDGEMENTS
This work was supported by: Federico Foundation, Faculdade de Medicina and Fundação Faculdade de Medicina to S.K.S.
REFERENCES
-
1McArdle B. Myopathy due to a defect in muscle glycogen breakdown. Clin Sci. 1951;10:13-35.
-
2Haller RG. Treatment of McArdle disease. Arch Neurol. 2000;57:923-4. DOI:10.1001/archneur.57.7.923
» https://doi.org/10.1001/archneur.57.7.923 -
3DiMauro S, Bruno C. Glycogen storage diseases of muscle. Curr Opin Neurol. 1998;11:477-84. DOI:10.1097/00019052-199810000-00010
» https://doi.org/10.1097/00019052-199810000-00010 -
4Kitaoka Y. McArdle disease and exercise physiology. Biology. 2014;3:157-66. DOI:10.3390/biology3010157
» https://doi.org/10.3390/biology3010157 -
5Tobon A. Metabolic Myopathies. Continuum (Minneap Minn). 2013;19:1571-97. DOI:10.1212/01.CON.0000440660.41675.06.
» https://doi.org/10.1212/01.CON.0000440660.41675.06 -
6Lucia A, Ruiz JR, Santalla A, Nogales-Gadea G, Rubio JC, García-Consuegra I, et al. Genotypic and phenotypic features of McArdle disease: insights from the Spanish national registry. J Neurol Neurosurg Psychiatry. 2012;83:322-8. DOI:10.1136/jnnp-2011-301593.
» https://doi.org/10.1136/jnnp-2011-301593 -
7Haller RG, Vissing J. Spontaneous 'second wind' and glucose-induced second 'second wind' in McArdle disease: oxidative mechanisms. Arch Neurol. 2002;59:1395-402. DOI:10.1001/archneur.59.9.1395
» https://doi.org/10.1001/archneur.59.9.1395 -
8Mauro S Di. Muscle glycogenoses: an overview. Acta Myol. 2007;26:35-41.
-
9Lopez A, Banos I, Garcia-Estan J, Garcia B, Perez J, Salmeron P. Enfermedad de McArdle: descripción de cuatro hermanos con déficit de miofosforilasa. An Med Interna. 2001;18:136-8.
-
10Morrondo CD, Zarza LP, Tejadob BSM. McArdle Disease: 2 Case Reports. Reumatol Clin. 2016;12:161-3. DOI:10.1016/j.reumae.2015.06.004
» https://doi.org/10.1016/j.reumae.2015.06.004 -
11Sanjurjo E, Laguno M, Bedini JL, Miró O, Grau JM. Forearm ischemic exercise test. Standardization and diagnostic value in the identification of McArdle disease. Med Clin. 2004;122):761-6. DOI:10.1016/S0025-7753(04)74380-8
» https://doi.org/10.1016/S0025-7753(04)74380-8 -
12De Kerviler E, Leroy-Willig A, Duboc D, Eymard B, Syrota A. MR quantification of muscle fatty replacement in McArdle's disease. Magn Reson Imaging. 1996;14):1137-41. DOI:10.1016/S0730-725X(96)00236-6
» https://doi.org/10.1016/S0730-725X(96)00236-6 -
13Krishnamoorthy N, Santosh V, Yasha TC, Mahadevan A, Shankar SK, Jethwani D, et al. Glycogen storage disease type V (Mc Ardle's disease): a report on three cases. Neurol India. 2011;59:884-6. DOI:10.4103/0028-3886.91370
» https://doi.org/10.4103/0028-3886.91370 -
14Lucia A, Nogales-Gadea G, Pérez M, Martín MA, Andreu AL, Arenas J. McArdle disease: what do neurologists need to know? Nature Clin Pract Neurol. 2008;4:568-77. DOI:10.1038/ncpneuro0913
» https://doi.org/10.1038/ncpneuro0913 -
15Medical Research Council. Aids to the examination of the peripheral nervous system, Memorandum no. 45. Her Majesty's Stationery Office, London, 1981.
-
16Martín MA, Rubio JC, Buchbinder J, Fernández-Hojas R, del Hoyo P, Teijeira S, et al. Molecular heterogeneity of myophosphorylase deficiency (McArdle's disease): a genotype-phenotype correlation study. Ann Neurol. 2001;50:574-81. DOI:10.1002/ana.1225
» https://doi.org/10.1002/ana.1225 -
17Quinlivan R, Buckley J, James M, Twist A, Ball S, Duno M, et al. McArdle disease: a clinical review. J Neurol Neurosurg Psychiatry. 2010;81:1182-8. DOI:10.1136/jnnp.2009.195040
» https://doi.org/10.1136/jnnp.2009.195040 -
18Gurgel-Giannetti J, Nogales-Gadea G, van der Linden Jr H, Giannetti AV, de Castro Concentino EL, et al. Clinical and molecular characterization of McArdle's disease in Brazilian patients. Neuromol Med. 2013;15:470-5. DOI:10.1007/s12017-013-8233-2 DOI:10.1007/s12017-013-8233-2
» https://doi.org/10.1007/s12017-013-8233-2 -
19Vieitz I, Teijeira S, Fernandez JM, San Millan B, Miranda S, Ortolano S, et al. Molecular and clinical study of McArdle's disease in a cohort of 123 European patients. Identification of 20 novel mutations. Neuromuscul Disord. 2011;21:817-23. DOI:10.1016/j.nmd.2011.07.002
» https://doi.org/10.1016/j.nmd.2011.07.002 -
20Gordon N. Glycogenosis type V or McArdle's disease. Dev Med Child Neurol. 2003;45:640-4. DOI:10.1017/S0012162203001178
» https://doi.org/10.1017/S0012162203001178 -
21Santalla A, Nogales-Gadea G, Ortenblad N, Brull A, de Luna N, Pinós T, et al. McArdle disease: a unique study model in sports medicine. Sports Med. 2014;44:1531-4. DOI:10.1007/s40279-014-0223-5
» https://doi.org/10.1007/s40279-014-0223-5 -
22Vissing J, Haller RG. A diagnostic cycle test for McArdle's disease. Ann Neurol. 2003;54:539-42. DOI:10.1002/ana.10725
» https://doi.org/10.1002/ana.10725 -
23Braakhekke JP, de Bruin MI, Stegeman DF, Wevers RA, Binkhorst RA, Joosten EM. The second wind phenomenon in McArdle's disease. Brain. 1986;109:1087-101. DOI:10.1093/brain/109.6.1087
» https://doi.org/10.1093/brain/109.6.1087 -
24Lewis SF, Haller RG. The pathophysiology of McArdle's disease: clues to regulation in exercise and fatigue. J Appl Physiol. 1986;61:391-401. DOI:10.1152/jappl.1986.61.2.391
» https://doi.org/10.1152/jappl.1986.61.2.391 -
25Pillarisetti J, Ahmed A. McArdle disease presenting as acute renal failure. South Med J. 2007;100:313-6. DOI:10.1097/01.smj.0000242355.27078.f3
» https://doi.org/10.1097/01.smj.0000242355.27078.f3 -
26Andreu AL, Nogales-Gadea G, Cassandrini D, Arenas J, Bruno C. McArdle disease: molecular genetic update. Acta Myol. 2007;26:53-7.
-
27Coleman RA, Stajich JM, Pact VW, Pericak-Vance MA. The ischemic exercise test in normal adults and in patients with weakness and cramps. Muscle Nerve. 1986;9:216-21. DOI:10.1002/mus.880090305
» https://doi.org/10.1002/mus.880090305 -
28Tsujino S, Shankse S, Di Mauro S. Molecular genetic heterogeneity of myophosphorylase deficiency (McArdle's disease). N Engl J Med. 1993;329:241-5. DOI:10.1056/NEJM199307223290404
» https://doi.org/10.1056/NEJM199307223290404 -
29Quinlivan R, Martinuzzi A, Schoser B. Pharmacological and nutritional treatment for McArdle disease (Glycogen Storage Disease type V). Cochrane Database Syst Rev. 2014;12:CD003458. DOI:10.1002/14651858.CD003458.pub5.
» https://doi.org/10.1002/14651858.CD003458.pub5 -
30Martinuzzi A, Sartori E, Fanin M, Nascimbeni A, Valente L, Angelini C, et al. Phenotype modulators in myophosphorylase deficiency. Ann Neurol. 2003;53:497-502. DOI:10.1002/ana.10499
» https://doi.org/10.1002/ana.10499 -
31Lane RJ, Turnbull DM, Welch JL, Walton J. A double-blind, placebo-controlled, crossover study of verapamil in exertional muscle pain. Muscle Nerve. 1986;9:635-41. DOI:10.1002/mus.880090710
» https://doi.org/10.1002/mus.880090710 -
32Steele IC, Patterson VH, Nicholls DP. A double blind, placebo controlled, crossover trial of D-ribose in McArdle's disease. J Neurol Sci. 1996;136:174-7. DOI:10.1016/0022-510X(95)00320-2
» https://doi.org/10.1016/0022-510X(95)00320-2 -
33MacLean D, Vissing J, Vissing SF, Vissing SF, Haller RG. Oral branched-chain amino acids do not improve exercise capacity in McArdle disease. Neurology. 1998;51:1456-9. DOI:10.1212/WNL.51.5.1456
» https://doi.org/10.1212/WNL.51.5.1456 -
34Poels PJ, Braakhekke JP, Joosten EM, Stegeman DF. Dantrolene sodium does influence the second-wind phenomenon in McArdle's disease. Electrophysiological evidence during exercise in a double-blind placebo-controlled, cross-over study in 5 patients. J Neurol Sci. 1990;100:108-12. DOI:10.1016/0022-510X(90)90020-N
» https://doi.org/10.1016/0022-510X(90)90020-N -
35Day TJ, Mastaglia FL. Depot-glucagon in the treatment of McArdle's disease. Aust N Z J Med. 1985;15:748-50.
-
36Phoenix J, Hopkins P, Bartram C, Beynon RJ, Quinlivan RC, Edwards RH. Effect of vitamin B6 supplementation in McArdle's disease: a strategic case study. Neuromuscul Disord. 1998;8:210-2. DOI:10.1016/S0960-8966(98)00004-2
» https://doi.org/10.1016/S0960-8966(98)00004-2 -
37Sato S, Ohi T, Nishino I, Sugie H. Confirmation of the efficacy of vitamin B6 supplementation for McArdle disease by follow-up muscle biopsy. Muscle Nerve. 2012;45:436-40. DOI:10.1002/mus.22290.
» https://doi.org/10.1002/mus.22290 -
38Vorgerd M, Grehl T, Jager M, Muller K, Freitag G, Patzold T, et al. Creatine therapy in myophosphorylase deficiency (McArdle disease): a placebo-controlled crossover trial. Arch Neurol. 2000;57:956-63. DOI:10.1001/archneur.57.7.956
» https://doi.org/10.1001/archneur.57.7.956 -
39Vorgerd M, Zange J, Kley R, Grehl T, Husing A, Jager M, et al. Effect of high-dose creatine therapy on symptoms of exercise intolerance in McArdle disease: double-blind, placebo-controlled crossover study. Arch Neurol. 2002;59:97-101. DOI:10.1001/archneur.59.1.97
» https://doi.org/10.1001/archneur.59.1.97 -
40Andersen ST, Vissing J. Carbohydrate- and protein-rich diets in McArdle disease: effects on exercise capacity [published erratum appears in J Neurol Neurosurg Psychiatry. 2010;81:1414. J Neurol Neurosurg Psychiatry. 2008;79:1359-63. DOI:10.1136/adc.2008.146548
» https://doi.org/10.1136/adc.2008.146548
Publication Dates
-
Publication in this collection
22 Oct 2018 -
Date of issue
2018
History
-
Received
17 Apr 2018 -
Reviewed
18 May 2018 -
Accepted
10 June 2018 -
Published
20 Aug 2018